
Abstract
A woman in her 30s was administered linezolid treatment for pneumonia. Without continuous medical prescriptions, the patient self-administered linezolid for a total of 9 months, which subsequently led to symptoms of bilateral visual impairment and central scotomas. Fundus examination revealed blurred disc margins, accompanied with mild edema, flame-shaped hemorrhages around the optic disc, and mild tortuosity and dilation of retinal veins in both eyes. Visual field testing indicated the presence of central scotomas in both eyes. Visual evoked potentials testing showed reduced amplitudes in both eyes. After excluding other causes of optic neuropathy, the patient was tentatively diagnosed with bilateral toxic optic neuropathy (linezolid-associated optic neuropathy) based on these findings. After discontinuing linezolid, the patient's visual function gradually improved. This case suggests that close monitoring of visual function and neurological symptoms in patients receiving linezolid treatment is crucial, and early identification of relevant abnormalities and timely discontinuation of the drug can effectively improve patient prognosis.
Case presentation
A female patient aged approximately 30 years presented to the Department of Ophthalmology at the Second Hospital of Jilin University with a 2-month history of progressive bilateral visual impairment, accompanied with photophobia and ocular dryness. Nine months prior, she had been prescribed oral linezolid (600 mg twice daily) for the treatment of pneumonia. Ophthalmic examination revealed a best-corrected visual acuity of 0.04 in the right eye and 0.02 in the left eye. Intraocular pressure was 20 mmHg in the right eye and 21 mmHg in the left eye. Pupils were sluggish, with no afferent pupillary defect. Fundus examination showed blurred disc margins, mild disc edema, peripapillary flame-shaped hemorrhages, and mild retinal venous tortuosity and dilation in both eyes (Figure 1). Optical coherence tomography (OCT) of the macula and optic disc revealed thickening of the nasal retina in both maculae. Magnetic resonance imaging (MRI) of the optic nerves with and without contrast showed no significant abnormalities. Cranial computed tomography (CT) was also normal. Visual field testing revealed central scotomas in both eyes (Figure 2). Visual evoked potential (VEP) testing showed normal P100 latencies but reduced amplitudes bilaterally.
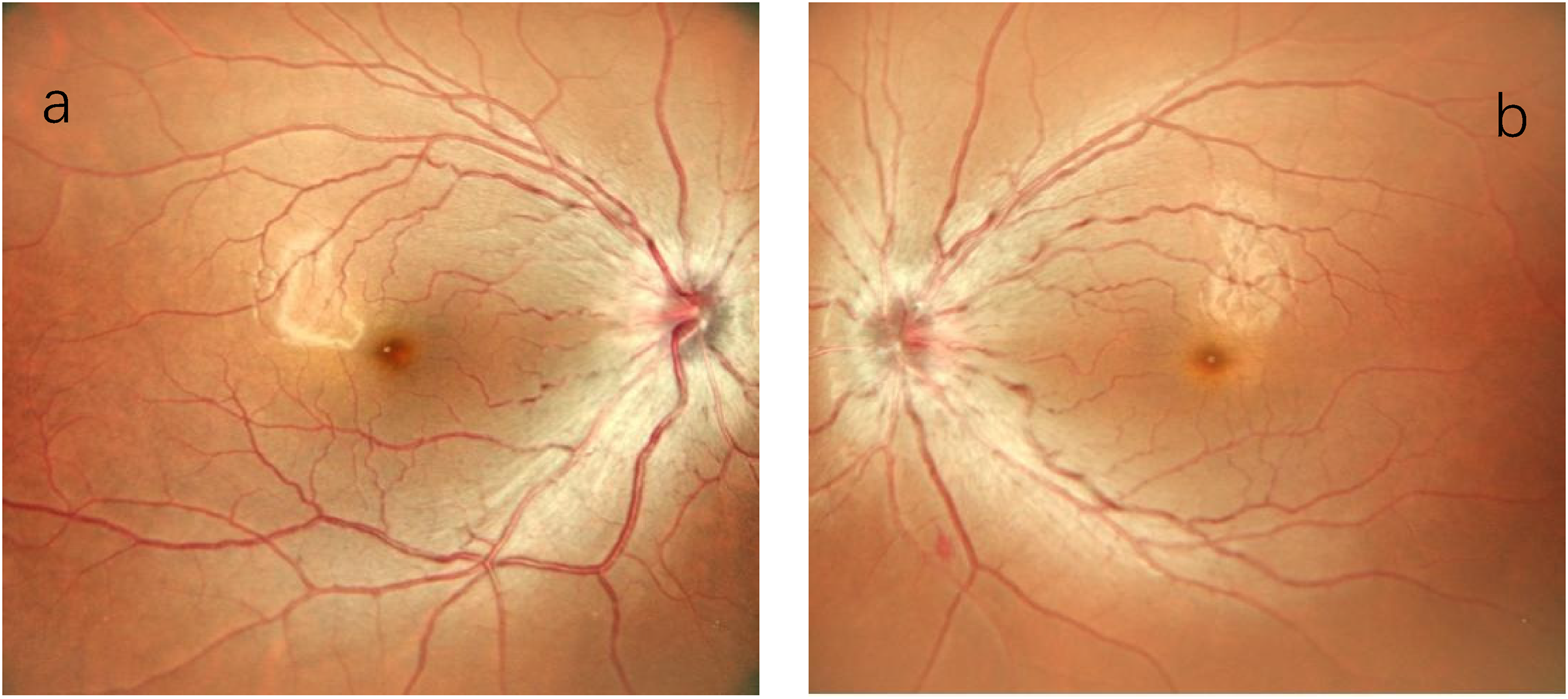
Fundus photographs showing bilateral optic disc edema and hyperemia with blurred margins and superficial peripapillary retinal hemorrhages.
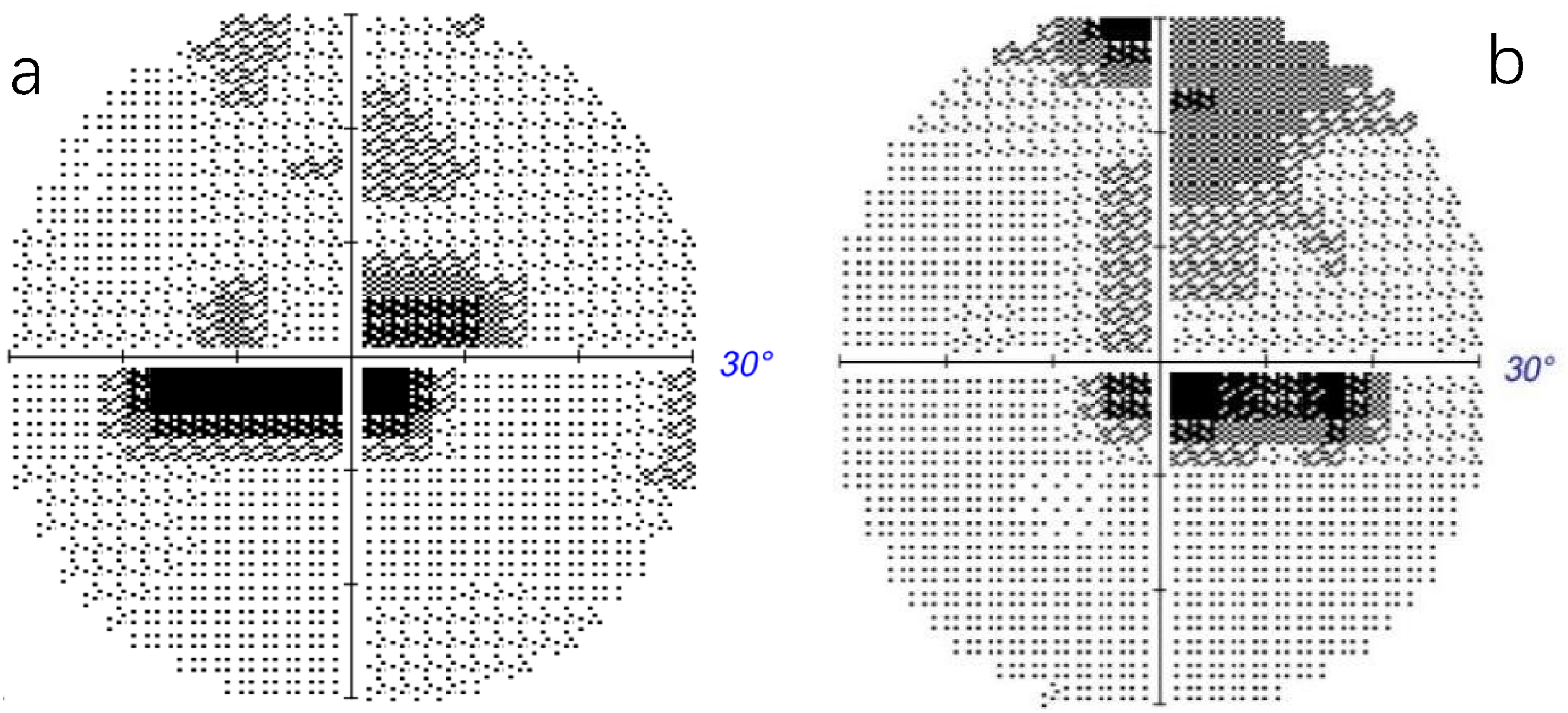
Visual field testing demonstrating bilateral central scotomas.
Considering the patient's history of long-term linezolid use and the onset of ocular symptoms accompanied with numbness in the extremities, a diagnosis of bilateral toxic optic neuropathy was tentatively established. The patient was advised to discontinue linezolid and receive sodium hyaluronate eye drops to relieve ocular dryness. Unfortunately, the patient did not return for follow-up due to the long distance from her residence to the hospital, and telephone follow-up was therefore performed after 1 month. Follow-up revealed that she had discontinued linezolid and reported subjective improvement of her symptoms. Written informed consent was obtained from the patient for study participation.
Discussion
Linezolid is an oxazolidinone-class antibiotic that is increasingly being used to treat infections caused by drug-resistant Gram-positive bacteria. It acts by inhibiting bacterial protein synthesis. However, its metabolites may impair mitochondrial function, which can cause several adverse effects. The most frequently reported adverse effects of linezolid include gastrointestinal disturbances, thrombocytopenia, and anemia.1,2 Furthermore, an increasing number of reports have described cases of optic and peripheral neuropathies as well as lactic acidosis.3–6 Although linezolid is generally well tolerated and early reports considered its adverse effects relatively uncommon, its broader clinical use has raised concerns regarding its potential toxicity. The spectrum of reported adverse effects includes diarrhea, vomiting, headache, anemia, thrombocytopenia, lactic acidosis, and both peripheral and optic neuropathies. 7 Because of its high penetration into the central nervous system and intraocular tissues, linezolid may cause optic nerve toxicity.8,9
Toxic optic neuropathy has been linked to various toxic agents, such as ethylene glycol, methanol, isoniazid, ethambutol, and fluoroquinolones as well as to deficiencies of vitamin B12, folate, and thiamine. 10 It is typically characterized by progressive, painless, bilateral visual loss, often accompanied with central scotomas and impaired color perception. In the early phase, the optic nerve may appear normal; however, optic disc edema and hyperemia often develop subsequently. In later stages, optic atrophy may develop in some patients. 11
This patient had received oral linezolid therapy for 9 months, which far exceeded the maximum recommended duration of 28 days specified in the product labeling. 3 In phase III clinical trials limited to 28 days, only mild adverse events were observed. Although the recommended maximum treatment duration is 28 days, linezolid is frequently administered for extended periods in clinical practice to treat infections caused by high-risk or drug-resistant pathogens. Consequently, adverse effects associated with prolonged linezolid therapy have been reported with increasing frequency. 12 Bone marrow suppression, peripheral and optic neuropathies, and lactic acidosis occur predominantly in patients treated beyond the recommended 28-day duration.1,4 In this case, the patient, a young woman with a 9-month history of linezolid therapy, presented with a 2-month history of painless, symmetrical bilateral visual decline. Fundus examination revealed optic disc changes resembling those observed in patients with optic neuritis. Visual field testing demonstrated symmetrical bilateral central scotomas. VEP testing showed normal P100 latencies but reduced amplitudes in both eyes. MRI did not suggest optic neuritis or compressive pathology. Based on the clinical presentation and history, linezolid-induced toxic optic neuropathy was the most likely diagnosis. The patient discontinued linezolid, after which her visual function improved markedly. This outcome supports the diagnosis of drug-induced optic neuropathy and indicates that the condition was reversible in this case. For patients suspected of optic neuropathy, immediate discontinuation of linezolid is essential. Neurotrophic agents, such as mecobalamin tablets, may be used as potential supportive therapy. Most patients with optic nerve damage show improvement after medication discontinuation, likely because the offending agent is withdrawn before the onset of irreversible axonal loss and apoptosis. 13 However, unlike optic neuropathy, linezolid-induced peripheral neuropathy has been reported to be largely irreversible. 12 We have summarized the reported clinical cases of linezolid-induced optic neuropathy in recent years in Table 1.4,14–16
Summary of reported clinical cases of linezolid-induced optic neuropathy in recent years.
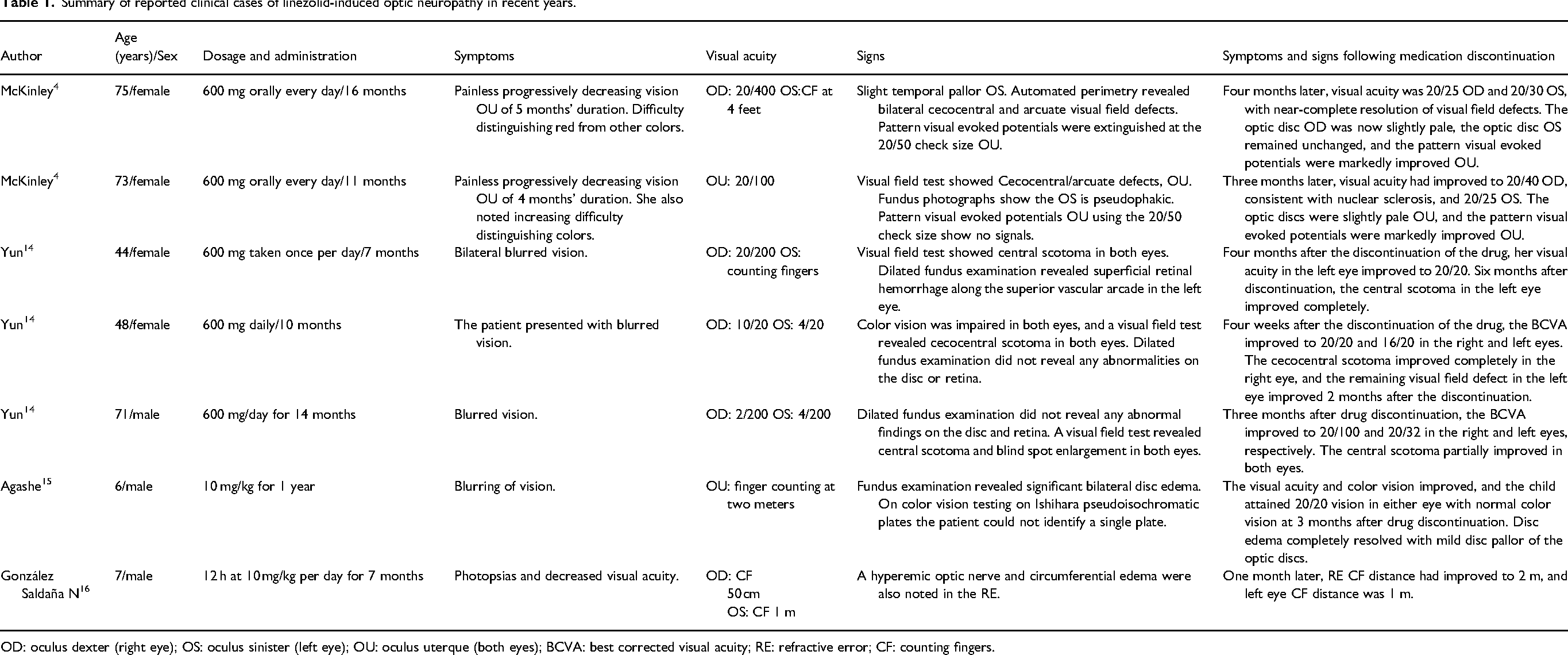
OD: oculus dexter (right eye); OS: oculus sinister (left eye); OU: oculus uterque (both eyes); BCVA: best corrected visual acuity; RE: refractive error; CF: counting fingers.
Linezolid can induce optic nerve toxicity, manifested as visual impairment, dyschromatopsia, and other symptoms. Most patients exhibit symptom improvement after drug discontinuation; however, some (including pediatric patients) do not experience full recovery. Children are prone to missed diagnosis due to limited expressive ability, requiring close monitoring of ocular and neurotoxicity. Linezolid-induced toxicities are dose- and duration-dependent. Gou et al. investigated the relationship between hepatic and renal function and serum exposure levels of linezolid and its metabolites. They found that the serum levels of linezolid and its major metabolites significantly increased with worsening hepatic and renal impairment. Hepatic and renal dysfunction can lead to drug accumulation and an increased risk of toxicity, predisposing patients to adverse reactions such as thrombocytopenia and anemia. Therefore, dosage reduction is recommended for these patients in clinical practice. 17 In addition, Liu et al. found that the in vitro hepatic clearance of linezolid in hepatocytes from rats with hepatic impairment decreased by 61.3%, indicating a marked reduction in hepatic metabolic capacity. In hepatocytes of rats with renal failure, the in vitro hepatic clearance of linezolid dropped by 44.1%. Meanwhile, both renal and total clearance of linezolid as well as its two metabolites was decreased. 18 We advise close monitoring for signs of both peripheral and optic neuropathies in patients receiving linezolid treatment for >28 days. For the evaluation of peripheral neuropathy, patients should be carefully questioned about typical symptoms such as numbness, paresthesia, weakness in the extremities, and decreased or absent tendon reflexes. Neuroelectrophysiological studies may be performed for definitive diagnosis if necessary. For optic neuropathy, visual acuity and fundus examination should be performed routinely, and visual field testing may be additionally performed when clinically indicated. Additionally, strategies such as reducing the total cumulative dose or implementing intermittent dosing schedules may help mitigate neurotoxicity. The reporting of this study conforms to the Case Report (CARE) guidelines. 19
Conclusion
Although linezolid remains an effective antimicrobial agent, its potential to induce optic neurotoxicity warrants high clinical attention. This case supplements clinical evidence for the neurotoxicity profile of linezolid. This case reinforces awareness of optic neuropathy associated with prolonged linezolid use. Strict control of the treatment duration and close monitoring of visual function and peripheral neuropathic signs are essential to minimize the risks associated with long-term administration. Once any suspicious visual or neurological symptoms occur, immediate discontinuation of linezolid and early ophthalmologic evaluation are crucial for improving visual prognosis.
This study has certain limitations. As a single case report, it cannot reflect the overall incidence and risk factors of linezolid-related optic neurotoxicity. In addition, the absence of objective ophthalmic re-examinations is a major limitation of this case report, and the long-term visual outcome of the patient requires further follow-up. The lack of systematic clinical examination and electrophysiological assessment for the patient's extremity numbness is also a limitation of this case report. Future multicenter and large-sample studies are needed to verify the risk characteristics, early warning indicators, and intervention strategies of linezolid-induced neurotoxicity.
Footnotes
Acknowledgments
The authors would like to thank all clinicians involved in the diagnosis and management of this patient. We also appreciate the patient's cooperation and consent for publication. In addition, we acknowledge the use of AI tools for language improvement.
Authors’ contributions
Si-Yu Chang collected and analyzed the data as well as wrote and revised the manuscript. Chun-Xia Zhang and Yue-Cong collected data and provided comments for the Discussion section. Xu Li designed this research, participated in the interpretation and discussion of the results, and revised the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used during the case report are available from the corresponding author, upon reasonable request.