
Abstract
Objectives
To compare the efficacy of C2 dorsal root ganglion high-dose pulsed radiofrequency and nerve block in managing cervicogenic headache with ocular symptoms.
Methods
This retrospective study analyzed 55 cervicogenic headache patients with ocular symptoms (blurred vision, eye pain, or photophobia) treated at the Second Hospital of Dalian Medical University from January 2022 to December 2024. Patients who received either high-dose pulsed radiofrequency (Group A, n = 29) or nerve block therapy (Group B, n = 26), both targeting the C2 dorsal root ganglion, were consecutively enrolled at our center. Pain intensity and ocular symptom severity were assessed using the numeric rating scale and Ocular Surface Disease Index, respectively, before treatment and at 1 day, 1 week, and 1 month after treatment.
Results
The primary outcome was the change in pain intensity (as assessed using the numeric rating scale). Numeric rating scale scores at all postoperative time points in both groups were significantly reduced compared with preoperative values (all p < 0.05), with the reduction in the numeric rating scale score at 1 month postoperatively in group A (Δ = 4.45 ± 1.23) being significantly greater than that in group B (Δ = 3.11 ± 1.18; between-group comparison: p < 0.05). Secondary outcomes included ocular symptoms (assessed using the Ocular Surface Disease Index) and overall clinical response rate; the Ocular Surface Disease Index value in group A decreased more significantly than that in group B (p < 0.05); the overall clinical response rate in group A (93%) was significantly higher than that in group B (39%) (p < 0.01).
Conclusions
Both high-dose pulsed radiofrequency and nerve block therapy effectively reduce pain associated with cervicogenic headache. High-dose pulsed radiofrequency therapy was superior to nerve block therapy in terms of superior pain relief, improved ocular symptoms, and higher overall clinical response rate.
Introduction
Headache disorders constitute a major global health burden, ranking among the most prevalent neurological conditions, with an estimated lifetime prevalence of >48% among adults. Epidemiological studies have demonstrated a consistent female predominance across headache subtypes, particularly in secondary headaches of cervical spine origin. 1 Cervicogenic headache (CEH), formally classified under the International Classification of Headache Disorders, 3rd edition (ICHD-3) as headache attributed to cervical spine disorders, has shown a progressive rise in incidence over the past decade, paralleling global trends in cervical degenerative disease.
The pain associated with CEH typically originates in the cervical region and radiates to the ipsilateral eye, forehead, and temporal area, usually as a unilateral dull, aching, and non-pulsating headache.2–5 Some studies have shown that anatomical variations in the cervical intervertebral disc, segmental dysfunction, and other common cervical spine lesions (e.g. uncovertebral arthropathy, osteophyte formation, disc herniation, cervical muscle fat infiltration, reduced cross-sectional area of cervical muscles, subarachnoid space stenosis, and ventral dura mater compression) can lead to CEH. 6
The cardinal clinical features of CEH include headache, reduced cervical range of motion, and visual disturbances. The severity of pain and associated ocular symptoms substantially diminish the quality of life. At present, the pathogenesis of CEH remains unclear. The manifestation of ocular symptoms in CEH implicates multisystem interactions. The cervical spine and its related structures are neuroanatomically linked to CEH via the trigeminocervical complex (TCC). Cervical sensorimotor control involves the central integration and processing of all afferent information, including visual, vestibular, and cervical proprioceptive inputs, which then execute motor programs via the neck muscles, resulting in the misinterpretation of neck pain signals as head or ocular discomfort.7,8 This neural crosstalk can trigger referred pain, manifesting as periorbital pain, blurred vision, or photophobia.
Therapeutic interventions for CEH include pharmacological treatment, physical therapy, nerve blocks, minimally invasive procedures, and surgical interventions targeting the cervical spine. Although nerve blocks offer both diagnostic utility and pain relief, their long-term efficacy is constrained, with a notable recurrence rate. 9 Minimally invasive techniques, such as pulsed radiofrequency (PRF), represent innovative therapeutic strategies for refractory pain conditions, including neuropathic pain, spinal-origin pain, and joint pain. PRF has garnered increasing interest in CEH management. PRF therapy modulates nerve function and inhibits pain signal transmission by applying specific pulsed currents to the cervical nerves, minimizing nerve damage, and preserving nerve function while enhancing local blood circulation. Research has suggested that high-voltage PRF exhibits superior analgesic effects compared with standard-voltage (45 V) PRF in a spared nerve injury (SNI) model of the dorsal root ganglion in rats. 10 However, the SNI rat model of sciatic nerve injury is inherently different from human CEH in terms of pathological mechanisms, pain signaling, and neuroplasticity. Voltage parameters obtained from rat dorsal root ganglia cannot be directly extrapolated to determine safe and effective therapeutic doses for the human cervical nerve plexus. Furthermore, animal studies typically exclude confounding factors such as underlying comorbidities, prior medications, and anatomical variations. Thus, despite evidence from animal studies supporting the analgesic potential of high-voltage PRF, its clinical efficacy, optimal parameters, and safety in CEH patients, particularly those with ocular symptoms, needs to be validated in well-designed human trials. Therefore, we hypothesized that high-dose pulsed radiofrequency (HDRF) (pulse dose = pulse width × voltage) is more effective in alleviating the ocular symptoms associated with CEH by modulating signal transmission within the TCC through a more potent field effect.
Given the propensity for misdiagnosis and suboptimal therapeutic outcomes in CEH with concomitant ocular symptoms, 3 this study aimed to evaluate the clinical utility of HDRF for managing CEH accompanied with ocular manifestations to inform clinical practice.
Materials and methods
General information
This study retrospectively analyzed the clinical data of 55 patients with CEH treated at the Pain Department of the Second Hospital of Dalian Medical University between January 2022 and December 2024. The inclusion criteria were as follows: (a) CEH diagnosis per ICHD-3 criteria 11 ; (b) age, 40–70 years; (c) no prior regular CEH treatment; (d) presence of ≥2 ocular symptoms (blurred vision, eye pain, or photophobia) with other ocular pathologies excluded through ophthalmological examination; (e) symptom duration or recurrent episodes >3 months; (f) numeric rating scale (NRS) score ≥4; and (g) no history of chronic analgesic use, substance abuse, tobacco, or alcohol dependence. Exclusion criteria comprised the following: (a) puncture site infection/tumor; (b) severe cervical pathology (disc herniation with prolapse/free fragment, spondylolisthesis, or spinal instability); (c) spinal canal or intracranial space-occupying lesions; (d) severe cardiopulmonary, hepatic, or renal dysfunction; (e) coagulation disorders; and (f) severe, uncontrolled psychiatric or neurological disorders (e.g. major depression with suicidal ideation, bipolar disorder, schizophrenia, and dementia). The choice of treatment regimen was made by the attending physician based on a comprehensive assessment of the patient's specific condition, prior treatment response, financial status, and patient preference. After retrospective data collection, patients were divided into the HDRF group (Group A, n = 29) and nerve block group (Group B, n = 26) according to the treatment they actually received. Baseline characteristics showed no statistically significant intergroup differences (p > 0.05), confirming comparability (Table 1). The study protocol was approved by the Institutional Ethics Committee (Approval No. KY2025–163–01).
General data of the two groups of patients.

Treatment methods
Group A (HDRF): Patients were positioned in the prone position in the operating room under routine monitoring of blood oxygen, blood pressure, and heart rate. Following standard skin disinfection and sterile draping, a low-frequency ultrasound probe (Philips Sparq) was prepared with coupling gel and covered with a sterile sheath. The probe was advanced caudally from the skull base until identification of the first spinous process bifurcation (C2). With the probe spanning the C2 spinous process and C1 transverse process, the “small boat sign” (representing the inferior oblique muscle) was visualized. Deep to this muscle layer, the vertebral artery, atlantoaxial joint, and C2 dorsal root ganglion (DRG) were identified in a lateral-to-medial orientation. Under local anesthesia (1% lidocaine), an ultrasound-guided radiofrequency needle was advanced to target the C2 DRG (Figure 1). Following ultrasound-confirmed needle positioning, the radiofrequency generator was activated. Sensory stimulation (50 Hz, 0.4 V) reproduced preoperative pain distribution paresthesia. Motor stimulation (2 Hz, 0.5 V) confirmed muscle contraction. PRF parameters included pulse width, 20 ms; frequency, 2 Hz; temperature, 55°C; and duration, 12 min. Output voltage was titrated from 45 V to the patient's maximum tolerance (45–99 V). After treatment, the needle was withdrawn, and sterile dressing applied. No adverse events occurred.
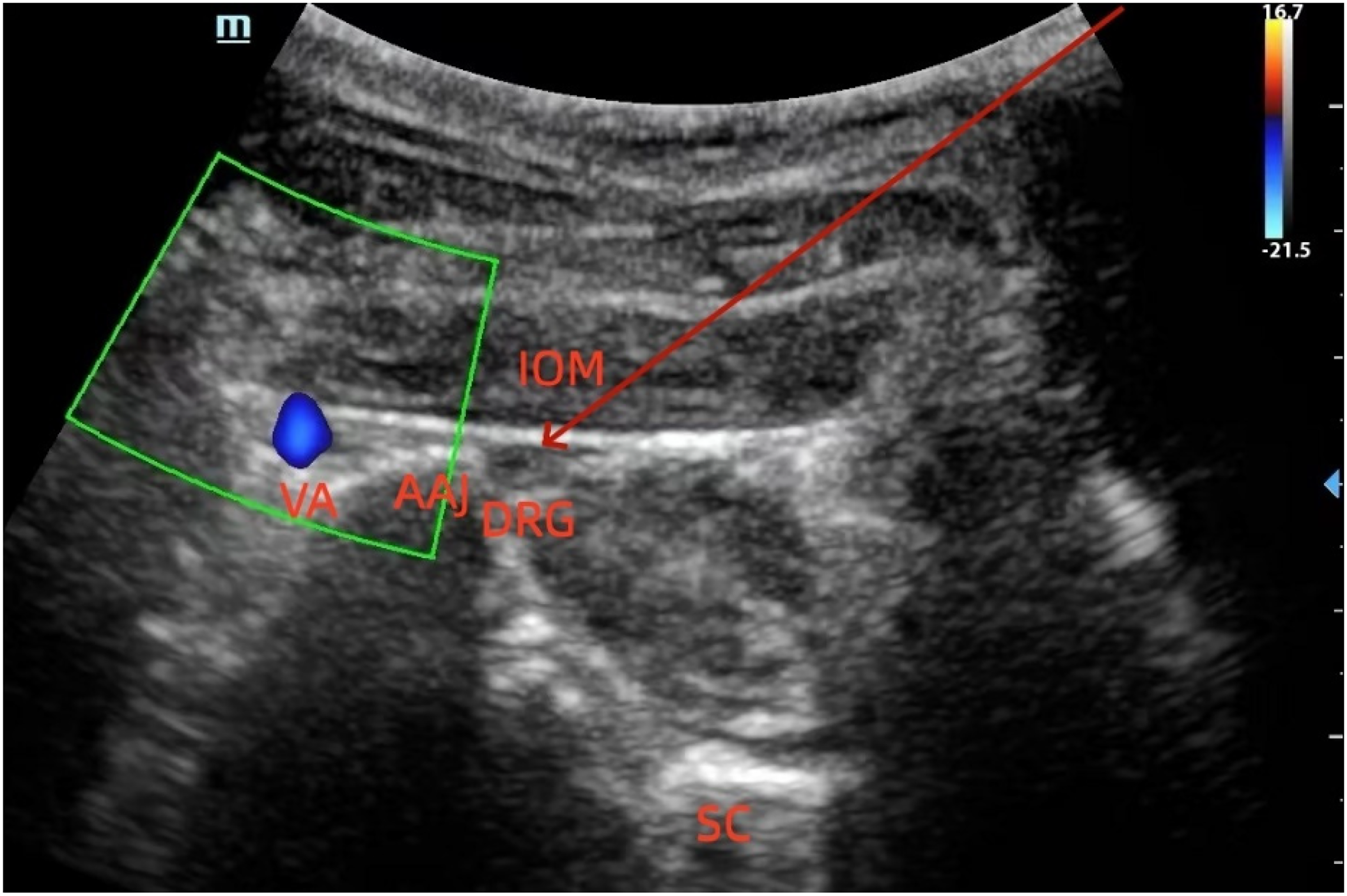
Ultrasound guided C2 dorsal root ganglion puncture.
Group B (Nerve Block): A 5 mL solution containing: 1% ropivacaine (0.5 mL), Betamethasone (5 mg), Vitamin B12 (0.5 mg), Vitamin B1 (200 mg) and 0.9% sodium chloride (qs to 5 mL) was prepared. Under ultrasound guidance, the needle was advanced to the C2 DRG (Figure 1). Following position verification, 5 mL of the solution was administered. The needle was then removed with sterile dressing application. No adverse reactions were observed.
Observational indicators and evaluation criteria
Pain assessment
Pain intensity was evaluated using the NRS at four timepoints, including pre-treatment (T0) as well as 1 day (T1), 1 week (T2), and 1 month (T3) post-treatment. Scores ranged from 0 (no pain) to 10 (worst imaginable pain), with scores ≥4 defining moderate-to-severe pain.
Ocular symptom evaluation
Ocular symptoms were quantified using the Ocular Surface Disease Index (OSDI). The 100-point scale categorized severity as follows: ≤20, mild symptoms; 21–45, moderate symptoms; and ≥46, severe symptoms.
Therapeutic efficacy evaluation
Treatment outcomes were assessed according to the modified MacNab criteria at the timepoint of T3. Complete symptom resolution, unrestricted mobility, and return to normal occupation were considered excellent outcome. Meaningful symptom relief enabling light occupational duties was indicative of good outcome. Insufficient improvement or symptom exacerbation was classified as poor outcome. Total efficacy rate was calculated as: (Number of excellent + good cases)/Total cases × 100%.
Statistical analyses
All analyses were performed using the Statistical Package for Social Sciences (SPSS) software (version 29.0; IBM Corp.). Continuous variables were assessed for normality using Shapiro–Wilk test. Normally distributed data are presented as mean (x) ± SD and were compared between groups using independent samples t-tests. Non-normally distributed data are expressed as median (interquartile range (IQR)) and analyzed using the Mann–Whitney U test. Categorical variables were compared using Pearson's chi-square (χ2) as appropriate. Statistical significance was defined as p <0.05. To control for potential confounding, multivariable regression analyses were performed. For the primary outcome (change in NRS score at 1 month), a multiple linear regression model was constructed, adjusting for age, sex, disease duration, and baseline NRS score. For the secondary binary outcome (clinical effective rate), a multivariable logistic regression model was used with the same covariates. Model assumptions were checked (linearity, normality of residuals, absence of multicollinearity). Adjusted mean differences (linear regression) or adjusted odds ratios (ORs) (logistic regression) with 95% confidence intervals (CIs) and p-values are reported.
Results
The registered trial enrolled 55 patients from January 2022 to December 2024. All follow-up data were complete and met the inclusion criteria. We summarized the baseline demographic and clinical characteristics of the patients, including their age, sex, and disease duration. There were no statistically significant differences between the two groups in terms of age, sex, disease duration, preoperative NRS scores, and preoperative OSDI scores. Therefore, the demographic characteristics of the two groups were comparable (Table 1).
Pain assessment
No statistically significant difference was observed in the NRS scores between the two groups before treatment (T0) or 1 day after treatment (T1) (p > 0.05). However, the NRS scores at all post-treatment time points were significantly reduced compared with those at baseline (T0) in both groups, with statistically significant reductions observed at 1 week (T2) and 1 month (T3) post-treatment (p < 0.05). Furthermore, the NRS scores in Group A were significantly lower than those in Group B at both T2 and T3 (p < 0.05) (Figure 2).
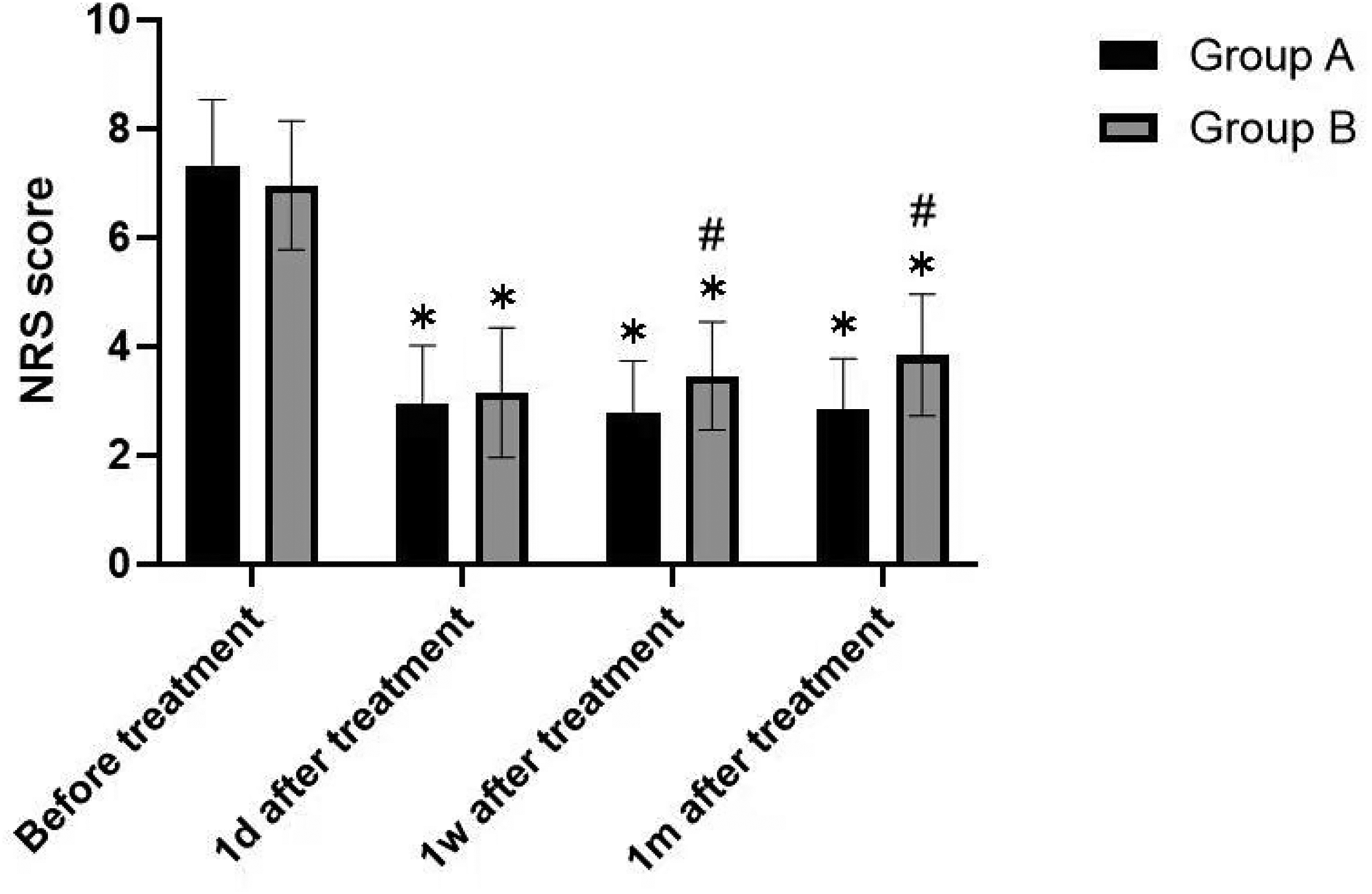
Comparison of the NRS scores between the two groups before and after treatment.
Comparison of ocular symptom relief
Before treatment (T0), the OSDI values did not differ significantly between the groups (p > 0.05). Post-treatment, both groups exhibited significant reductions in the OSDI values compared with those at baseline (p < 0.05). Importantly, the magnitude of reduction in the OSDI values was significantly greater in Group A than in Group B (p < 0.05, Figure 3).
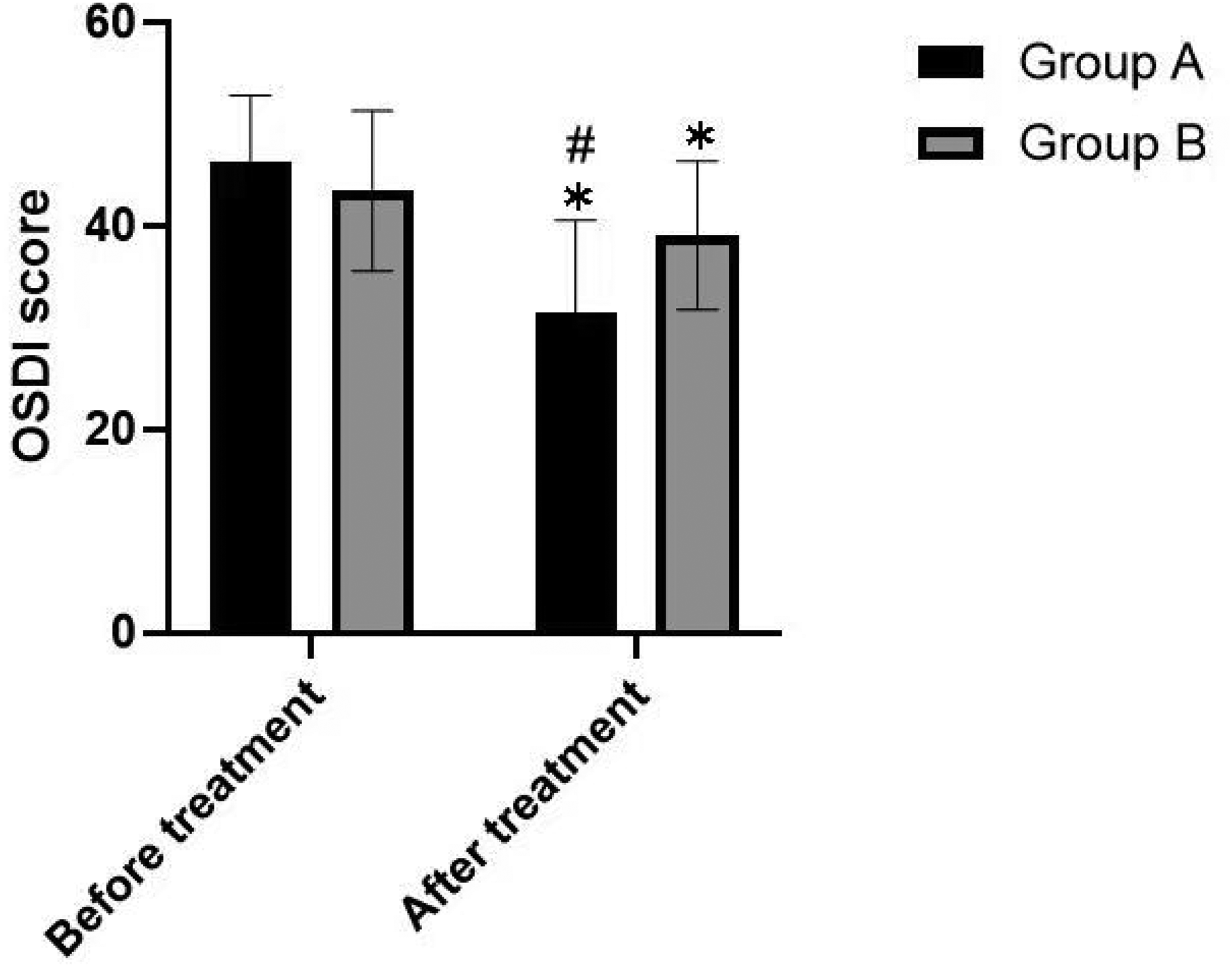
Comparison of the OSDI values before and after treatment in the two groups of patients.
Comparison of clinical efficacy
Post-treatment assessment using established efficacy criteria revealed significant intergroup differences. Group A demonstrated superior outcomes; 11 patients (37.9%) achieved significant improvement, 16 (55.2%) showed moderate improvement, and only 2 (6.9%) were non-responsive, yielding a 93% total effective rate. Conversely, Group B exhibited limited efficacy; 1 patient (3.8%) showed significant improvement, 9 (34.6%) demonstrated moderate improvement, and 16 (61.5%) were non-responsive, resulting in a 39% total effective rate.
Chi-square analysis confirmed significantly superior clinical efficacy in Group A than in Group B (χ2 = 18.59, p < 0.01, Table 2).
Comparison of the effective rate at different time points in the two groups of patients.

After adjusting for age, sex, disease duration, and baseline NRS score, multiple linear regression showed that Group A exhibited a significantly greater reduction in the NRS score at 1 month compared with Group B (adjusted mean difference = 1.28, 95% CI: 0.52–2.04, p = 0.001). Multivariable logistic regression demonstrated that Group A had a significantly higher clinical effective rate than Group B (adjusted OR = 18.6, 95% CI: 4.1–84.3, p < 0.001).
Discussion
CEH is defined as pain originating from the cervical spine, with complex and incompletely understood etiology and pathogenesis. Physiologically, CEH pain mirrors spinal-origin pain referred to the shoulder, chest wall, hip, and lower extremities. Anatomically, the C2 spinal nerve and its DRG lie proximate to the lateral capsule of the atlantoaxial (C1–2) facet joint, with branches innervating both C1–2 and C2–3 facet joints. Consequently, pathological, inflammatory, or traumatic changes affecting these joints may contribute to headache pain. 12
Concurrent headache and neck pain arise from shared nociceptive innervation of the head and neck within the TCC. The TCC extends from the medulla to the C1 and C2 spinal segments. Within its caudal portion, the TCC receives first-order nociceptive Aδ and C afferents from both ophthalmic nerve (V1) and, primarily, the C2 dorsal root. These primary afferents connect directly or indirectly via wide dynamic range neurons to secondary neurons. Specifically, the ophthalmic nerve (V1) transmits nociceptive input via Aδ and C fibers to superficial and deep secondary nociceptive neurons in the C1 and C2 dorsal horns of the TCC. C2 nerve root conveys Aδ and C nociceptive afferent information from the posterior fossa vasculature, dura mater, and upper cervical myofascial structures. Crucially, nociceptive terminals from the ophthalmic nerve and the C2 nerve root exhibit structural overlap within the C1 and C2 dorsal horns of the TCC. 13 This neuroanatomical convergence of ophthalmic and cervical nociceptive afferents onto second-order neurons in the caudal TCC is therefore critical for the manifestation of concurrent headache and neck pain.
The caudal portion of the trigeminocervical nucleus (TNC) exhibits longitudinal continuity with the lateral lamina of the dorsal horn at the C3–4 spinal segments. This anatomical continuity facilitates functional convergence of cervical and trigeminal sensory pathways, enabling bidirectional transmission of pain signals between the cervical region and trigeminal sensory receptive fields of the face and head. 12 Consequently, afferent fibers from the trigeminal nerve and the upper cervical spinal nerves (C1-C4) converge onto second-order neurons within the TNC. These neurons integrate nociceptive input not only from the trigeminal spinal tract (carrying afferents from the ophthalmic branch and parietal, frontal, and orbital regions), but also from the C1, C2, and C3 spinal nerves and adjacent cervical nerves. 4 This convergence mechanism underlies various patterns of referred pain and explains the recurrent headaches induced by repeated activation of cervico-occipital structures. 14 Therefore, we hypothesize that HDRF reduces the projection of nociceptive signals to the ocular region by modulating the convergence pathway between the C2 DRG and the trigeminal spinal nucleus within the TNC.
Consistent with the above mechanism, the case report on ophthalmic trigeminal neuralgia by González-González et al. directly confirmed that pain associated with the first branch of the trigeminal nerve (ophthalmic nerve) can manifest as periorbital discomfort, blurred vision, and other symptoms, which are highly consistent with the chief complaints of CEH patients in our study. 15 That study highlighted the anatomical–clinical overlap between the cervical and trigeminal systems and provides strong indirect evidence supporting our mechanistic hypothesis that targeting the C2 DRG with HDRF alleviates ocular symptoms.
Research indicates a significantly reduced suboccipital pressure pain threshold in the CEH group compared with that in controls, characteristic of TNC sensitization. Central sensitization, involving diffusion along the anterior neural axis to the trigeminal spinal nucleus, plays a primary role in CEH development. 16 Furthermore, the case report by Martínez-Lozano et al. indicated that individual differences in pain perception and response are influenced by both psychological and neurobiological factors, which may partly account for the variability in treatment efficacy observed within the HDRF group in our study. 17 Baseline central sensitization status was not assessed in this study; therefore, we could not adjust for these potential central modulatory factors. Future studies should incorporate central sensitization indicators and psychosocial assessments to more accurately explain the variability in treatment response.
The primary nerves conducting CEH are the greater and lesser occipital nerves, formed by the medial branch of the second cervical nerve (C2) and fibers from the third cervical nerve (C3). A prospective case series by Kuhn et al. involving 12 patients with occipital neuralgia symptoms reported common associated symptoms including tinnitus, scalp paresthesia, nausea, dizziness, and visual disturbances. 18 Although vertebral artery dissection can also present with headache and neck pain, the warning signs warranting further medical evaluation include progressively worsening headache, thunderclap headache onset, headache accompanied with high fever/neck stiffness/rash, post-traumatic headache onset, and visual problems or severe dizziness. 19 Among the CEH patients in this study, the primary ocular symptoms were blurred vision, eye pain, and photophobia. However, ocular examinations revealed no specific manifestations and varied considerably across patients.
The greater occipital nerve (GON), a primary site of CEH, originates from the medial branch of the C2 dorsal ramus. 20 It innervates the posterior scalp region extending from the external occipital protuberance to the vertex. Given this anatomical significance, the C2 DRG represents a key therapeutic target for CEH. Studies have demonstrated successful ultrasound-guided blockade of the GON at the C2 level for treating occipital neuralgia and CEH, with significant reductions in pain scores observed over 4-week periods. 21 C2 neuralgia itself can manifest as occipital tenderness, often resulting from compressive or inflammatory lesions affecting the C2 nerve root. Compared with isolated GON neuralgia, C2 neuralgia may additionally involve ocular symptoms such as excessive tearing (lacrimation) or conjunctival injection (ciliary congestion). 20 The anatomical rationale for selecting the C2 DRG as the therapeutic target in this study is directly supported by the cadaveric study by Alvarez et al. 22 That study demonstrated that cervical nerves exhibit segmental-specific tension patterns during physiological movements, particularly involving the C1–C3 nerve roots, and that this dynamic tension may induce or exacerbate CEH-related nociceptive input. This finding further explains why PRF or nerve block targeting the C2 DRG can effectively relieve referred pain originating from the upper cervical spine and provides a solid kinesiological basis for our choice of interventional target.
A comprehensive patient history and physical examination constitute the most reliable approach for diagnosing CEH. Diagnostic facet joint injections and cervical nerve or medial branch blocks can further confirm the diagnosis and predict therapeutic outcomes. Persistent head and neck pain encompass conditions, including chronic migraine, chronic tension-type headache, new daily persistent headache, and CEH. Compression of the greater and lesser occipital nerves by posterior cervical muscles and their fascial attachments at the occipital ridge, leading to local perineural inflammation, may underlie certain persistent head and neck pain syndromes. The resulting pain typically originates in the suboccipital and occipital regions and radiates anteriorly into trigeminal nerve-innervated areas of the head via anatomical connections between extracranial and intracranial nerves. Radiation to frontal regions can induce migraine-like symptoms such as photophobia and nausea. Treatments targeting extracranial structures—notably occipital nerve blocks and cervical trigger point injections—often provide significant relief for persistent head and neck pain. 23 When conservative measures fail, interventional pain management strategies may be employed, including GON and lesser occipital nerve (LON) blocks, cervical medial branch blocks (C1-C3), C3 medial branch and C4 dorsal ramus blocks, intra-articular facet joint injections (C2-C3, C3-C4), atlantoaxial joint injections, cervical epidural steroid injections, radiofrequency ablation, and occipital nerve stimulation. 24
Minimally invasive percutaneous treatments deliver alternating current at radiofrequency wavelengths to eliminate or modulate pain signals originating from target sites. PRF is a neuromodulation technique that applies short bursts of radiofrequency current separated by extended pauses. This pulsed delivery prevents significant temperature elevation, avoiding permanent neural tissue damage while providing pain relief. Pulsed Dose Radio Frequency (PDRF) is a specific PRF modality that generates pulses of consistent amplitude and width. A key distinction lies in thermal management; PRF systems modulate the amplitude or width of subsequent pulses if the tissue temperature exceeds a threshold, whereas PDRF systems pause until the temperature decreases before delivering the next pulse with identical parameters. PDRF aims to precisely modulate field effect intensity for neuromodulation. 25 The precise mechanism of PRF action remains incompletely understood. Unlike continuous radiofrequency (which relies on thermal neurolysis to block pain pathways), PRF utilizes pulsed current to generate an electric field around neural tissue. Evidence suggests this field mediates temperature-independent neuromodulation, potentially exerting analgesic effects. 26 The rapidly changing electric field—rather than heat—may modulate pain signal transmission through pathways involving the immediate early gene c-Fos, potentially including pain-inhibitory mechanisms such as long-term depression and inhibition of excitatory C-fibers. 27 Consequently, field effect intensity, defined by pulse dose (pulse dose = pulse width × voltage), is critical for therapeutic neuromodulation.
We hypothesize that HDRF produces analgesic effects by modulating signal transmission in the TCC through a high field effect. 25 The case report by Sillevis et al. showed that external vagus nerve stimulation can effectively relieve CEH, suggesting that autonomic regulation and central pain networks may be involved. 28 This finding resonates with our mechanistic hypothesis: the effect of HDRF may not be limited to peripheral modulation of the local C2 DRG, but may also influence the trigeminal nucleus caudalis and upstream pain matrices via central projections. Therefore, future studies could combine functional imaging or electroencephalography to explore the modulatory effects of HDRF on central neural pathways.
PRF technology has been widely applied in both domestic and international settings for treating CEH, either as monotherapy or in combination regimens. In one case series, PRF applied to the C2 DRG achieved complete pain resolution lasting 6 months (parameters: 42°C, 4 min; voltage unspecified). 29 However, another retrospective cohort study has reported shorter efficacy durations for isolated C2 DRG PRF in CEH. 30 Given this limitation, our study employed HDRF therapy. The HDRF parameters included a fixed pulse width of 20 ms, while voltage was titrated intraoperatively to the patient's maximum tolerable sensation level. This approach aimed to maintain a higher field effect intensity (pulse dose). The enhanced neuromodulatory capacity of HDRF may improve therapeutic outcomes, particularly in CEH patients with concomitant ocular symptoms. To our knowledge, this represents the first reported application of HDRF for CEH with concurrent ocular manifestations.
Although the results of this study showed a statistically significant difference in the reduction in the NRS scores in the HDRF group compared with that in the nerve block group, statistical significance does not equate to clinical importance. Currently, there is no established minimal clinically important difference (MCID) for NRS scores specifically in CEH. Referring to commonly used thresholds in the chronic pain field (e.g. a reduction of 2 points or 30%), the decrease in the NRS score at 1 month postoperatively in the HDRF group (Δ = 4.45 ± 1.23) reached the accepted standard for clinically significant improvement. However, due to the lack of blinding and standardized outcome assessment, patient or assessor expectations may have amplified the subjective scores; therefore, the true magnitude of this clinical benefit should be interpreted cautiously.
More notably, the overall clinical response rate reported in this study was as high as 93% in the HDRF group and 39% in the nerve block group. This finding suggests that certain biases exist. Potential reasons include the following: (a) the definition of response may be overly liberal—in this study, response was defined as a reduction in NRS ≥50% or a reduction in OSDI ≥30%, a cutoff lacking CEH-specific validation; (b) lack of blinding—both patients and assessors were aware of group assignment, and HDRF, as a minimally invasive intervention, may have produced stronger placebo effects or expectation bias; (c) selection bias—in this retrospective design, patients with more severe disease or higher treatment expectations may have been preferentially assigned to the HDRF group, while the nerve block group may have included more patients who responded poorly to minimally invasive therapy; and (d) small sample size—with <30 patients per group, the outcome of a single patient could substantially alter the response rate percentage. Therefore, this response rate should not be directly interpreted as “true efficacy” but as an exploratory, preliminary signal requiring validation. In future prospective studies, blinded designs should be adopted, along with more conservative definitions of response (e.g. reduction of ≥2 in the NRS score and reduction of ≥30% in the OSDI value), to test the robustness of the findings.
Notably, as a chronic pain disorder, CEH is also modulated by psychosocial factors. The observational study by Viñals Narváez et al. has indicated that anxiety, depression, and maladaptive coping strategies are significantly associated with pain conditions involving the trigeminal pathway. 31 Although patients with severe anxiety, depression, or other psychiatric disorders were excluded from this study, mild-to-moderate emotional distress may still affect patients’ tolerance to treatment and the evaluation of therapeutic outcomes. Future studies should incorporate psychological assessment scales and employ structural equation modeling or mediation analysis to explore whether psychological factors partially mediate the difference in efficacy between HDRF and nerve block therapy. Integrating a biopsychosocial framework will facilitate more individualized pain management.
The OSDI is one of the most commonly used standardized questionnaires for assessing ocular symptoms and their impact on quality of life. Although it was originally designed for ocular surface diseases such as dry eye, the ocular symptoms in patients with CEH—including periorbital pain, blurred vision, photophobia, and a sensation of dryness—arise essentially from referred pain via the TCC and aberrant sensory integration, rather than from primary corneal or conjunctival lesions. Nevertheless, these symptoms overlap considerably with those of ocular surface diseases in terms of subjective experience, manifesting as visual disturbance, discomfort, and limitations in daily activities. The OSDI covers three domains (ocular symptoms, vision-related function, and environmental triggers) and can comprehensively capture patients’ subjective ocular complaints. Moreover, it has been used in previous studies to evaluate ocular symptoms associated with neuropathic pain conditions such as migraine and trigeminal neuralgia.32,33 Therefore, although the OSDI is not a CEH-specific instrument, its use as an exploratory outcome measure in this study can reflect patients’ overall ocular symptom response to treatment.
To our knowledge, this study is the first to demonstrate that both C2 DRG nerve blocks and HDRF effectively alleviate CEH pain. Additionally, the preliminary results of this study suggest that HDRF is superior to conventional nerve block therapy in the degree and durability of relief for concomitant ocular symptoms. However, it must be emphasized that this study is retrospective in design and has numerous inherent limitations, which make the findings exploratory rather than confirmatory. Therefore, although HDRF exhibited a favorable efficacy trend in this study population, it is currently not recommended as a first-line interventional therapy for CEH with ocular symptoms. Based on the current level of evidence, we only suggest that HDRF is considered a promising alternative or second-line treatment option for CEH patients with ocular symptoms who have responded poorly to or are intolerant of conventional therapies (e.g. nerve block) and that it should be used on an individual basis after full discussion of the potential benefits and risks. Future prospective, randomized controlled, double-blind, large-sample trials with fixed voltage or dose-stratified designs, using validated specific ocular symptom assessment tools and combined with functional imaging to explore neuromodulatory mechanisms, are needed to determine the true efficacy, optimal parameters, and clinical role of HDRF.
Limitations
This study has certain major limitations that should be considered when interpreting the results. First, there was an absence of true randomization. This was a retrospective cohort study in which treatment allocation was determined by the attending physician based on patients’ clinical characteristics, prior treatment response, financial status, and preferences, rather than random assignment. This inevitably introduced selection bias. Second, there was insufficient adjustment for confounding factors. Although we reported baseline demographic and clinical characteristics, the relatively small sample size (HDRF, n = 29; nerve block, n = 26) precluded robust multivariable regression to adjust for all potential confounders (e.g. disease duration, baseline pain intensity, and concomitant medications), leading to possible bias in effect estimation. Third, there was considerable variability in the HDRF intervention. Voltage was titrated according to patient tolerance across a range of 45–99 V, and individual voltage values were not recorded in this retrospective study. Consequently, we could not perform a quantitative dose–response analysis, which directly limits the testing of the dose-dependent neuromodulation hypothesis. Fourth, the validity of a key outcome measure is uncertain. The OSDI is a widely used questionnaire but was originally designed for ocular surface diseases; its formal validation for CEH-related ocular symptoms (arising from referred pain via the TCC) is lacking. Therefore, the OSDI may not fully capture patients’ visual complaints due to neuropathic referred pain, and its validity and reliability in the CEH population require further assessment. Fifth, the study involved a relatively small sample size and a short follow-up period (only up to 3 months postoperatively). These factors may have introduced measurement bias and reduced the statistical power, limiting the evaluation of long-term efficacy and safety. Taken together, these limitations suggest that the results of this study should be considered exploratory rather than confirmatory. The long-term efficacy of HDRF for CEH patients with ocular symptoms needs to be validated with further research. Future studies should adopt prospective, randomized, double-blind, controlled designs with fixed-voltage or stratified dose-comparison arms (e.g., 45 V, 70 V, and 95 V groups), strictly record individual treatment parameters, and perform multivariable regression or analysis of covariance to adjust for baseline confounders. Moreover, follow-up should be extended to at least 6 months, and functional imaging (e.g., functional magnetic resonance imaging (fMRI)) could be incorporated to assess neuromodulatory changes in the TCC and pain matrix, thereby testing the dose–response relationship at a mechanistic level. Finally, CEH-specific instruments for ocular symptoms should be developed or validated, or existing scales such as the OSDI should undergo psychometric testing in the CEH population. Only through such rigorous designs can the optimal parameters, true efficacy, and clinical value of HDRF for CEH with ocular symptoms be determined.
Conclusions
Both HDRF and nerve block interventions targeting the C2 DRG effectively alleviated pain symptoms in patients with CEH. However, HDRF demonstrated superior and more sustained efficacy in relieving associated ocular symptoms compared with traditional nerve blocks, resulting in improved short-term prognosis. Therefore, HDRF should be considered as a first-line treatment for CEH patients presenting with ocular symptoms.
Footnotes
Ethical approval
This study was approved by the Ethics Committee of the Second Hospital of Dalian Medical University (No. KY2025–163–01). This study adhered to the principles of the Declaration of Helsinki (1964) and its later amendments. All participants provided written informed consent.
Author contributions
Mingxi Dong conducted literature search, drafted the manuscript, and created tables/figures. Dongbai Li performed proofreading and language editing. Lingchao Li contributed to manuscript editing, study design, data analysis / interpretation, project supervision, and critical revisions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Datasets generated and/or analyzed in this study are available from the corresponding author upon reasonable request.