
Abstract
This review examines the development of organoid technology and its recent advances in the study of pituitary neuroendocrine tumors. As three-dimensional in vitro culture models, organoids can recapitulate the structural and functional characteristics of native organs, providing an innovative platform for investigating disease mechanisms, conducting drug screening, and developing personalized treatment strategies for pituitary neuroendocrine tumors. The article begins with an overview of the historical progression of organoid technology and then focuses on its specific applications in pituitary neuroendocrine tumor research, including disease modeling, drug testing, and potential uses in regenerative medicine. Finally, it addresses current challenges in the field and outlines future research directions and potential clinical applications.
Keywords
Background
Organoid technology has emerged as a transformative innovation in biomedical research, especially in the study of complex diseases such as pituitary neuroendocrine tumors (PitNETs). This approach involves cultivating stem cells or tissue-derived cells to generate three-dimensional (3D) structures that faithfully recapitulate the architecture and function of native organs. By replicating both physiological and pathological tissue states, organoids offer substantial advantages over traditional two-dimensional (2D) cell cultures and animal models, which often lack the complexity and specificity of human diseases. In PitNET research, organoid models provide a highly representative platform for studying tumorigenesis and evaluating therapeutic interventions in a controlled, human-relevant environment (Figure 1).1–7
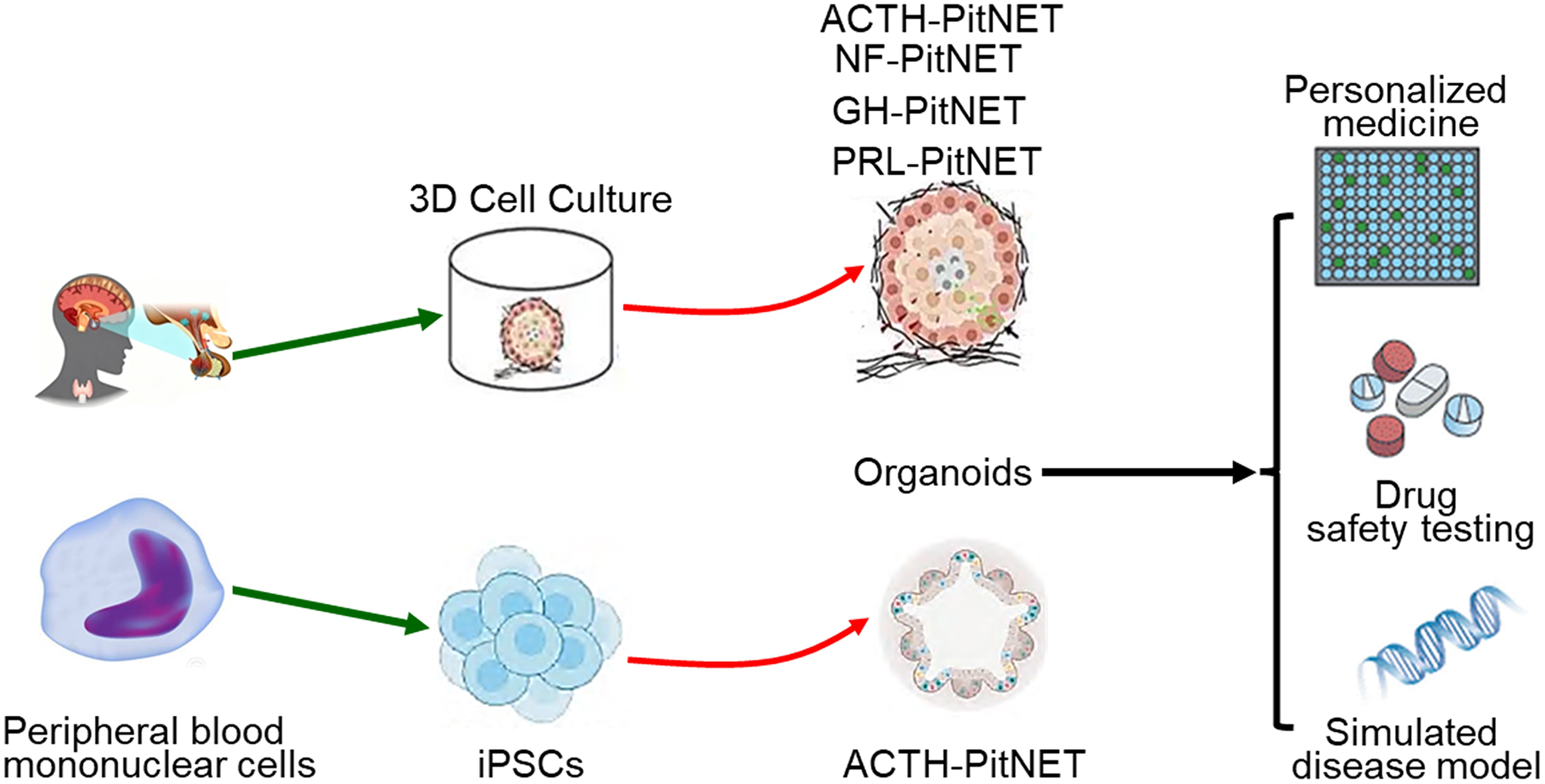
Construction and applications of pituitary neuroendocrine tumor (PitNET) organoid models. Adrenocorticotropic hormone–secreting PitNET (ACTH-PitNET), growth hormone–secreting type PitNET (GH-PitNET), prolactin hormone–secreting PitNET (PRL-PitNET), nonfunctioning PitNET (NF-PitNET), three-dimensional cell culture (3D cell culture), and induced pluripotent stem cells (iPSCs).
PitNETs are one of the most common intracranial tumors, and research in this field has long been constrained by the limitations of existing methodologies. Traditional 2D cell cultures often fail to recapitulate the spatial architecture and cellular diversity of the tumor microenvironment, thereby limiting comprehensive understanding. Although animal models remain valuable, they frequently do not translate accurately to human disease because of interspecies differences in tumor biology and treatment responses. The advent of organoid technology has introduced a paradigm shift in the study of PitNETs. This platform not only retains the genetic and phenotypic features of the original tumors but also enables the examination of their interactions within the surrounding microenvironment. 8 The establishment of organoid models for PitNETs carries substantial implications for both basic and clinical research. 4 For example, patient-derived organoids can be used for drug screening,4,6 offering valuable insights into personalized treatment strategies for individuals with refractory tumors. This method has demonstrated potential in predicting therapeutic efficacy and in identifying biomarkers for targeted therapies, thereby supporting the development of more individualized treatment approaches. 9 Furthermore, organoid technology provides a robust tool for investigating the mechanisms driving tumor growth and progression. It enables researchers to explore the genetic and epigenetic factors underlying the pathogenesis of PitNETs.1,2
Despite significant progress, organoid technology still faces several challenges. Standardization of culture protocols is critical for ensuring reproducibility and reliability across different studies. Additionally, ethical issues related to the use of human tissues, particularly concerning informed consent and the potential implications for patients and donors, must be carefully addressed. 10 As the technology evolves, it is imperative to establish clear guidelines that balance scientific innovation with ethical responsibility in organoid research.
In conclusion, organoid technology holds great promise for advancing the study and treatment of PitNETs. By offering a more physiologically relevant model, organoids help bridge the gap between basic research and clinical application, paving the way for more effective patient therapies. To fully realize this potential, ongoing refinement of organoid models, along with strengthened interdisciplinary collaboration, will be essential to overcome existing limitations and harness the full capabilities of this innovative technology in the study of PitNETs.1,4
Pathobiological features of PitNETs and clinical needs
PitNETs are among the most prevalent benign intracranial tumors, accounting for approximately 17.1% of all intracranial neoplasms. 11 They are typically classified according to their hormonal secretion profiles into functional tumors (e.g. prolactin-secreting PitNETs (PRL-PitNETs) and growth hormone–secreting PitNETs (GH-PitNETs)) and nonfunctional PitNETs. 12 Currently, the primary therapeutic approaches for patients with PitNETs are surgery and medication. Although the majority of patients achieve favorable outcomes, some face challenges because of incomplete surgical resection or poor responses to pharmacological treatment. Previous research has shown that the pathogenesis of PitNETs involves a complex interplay of genetic mutations, particularly in genes such as guanine nucleotide-binding protein G(s) subunit alpha (GNAS) and multiple endocrine neoplasia type 1 (MEN1) and epigenetic alterations, which collectively contribute to tumor initiation and progression.13,14 Previous studies have shown that the frequency of GNAS gene mutations in tumor tissues from patients with GH-PitNET reaches 40%. These patients have smaller tumors and respond better to treatment with somatostatin analogs. 15 The most common functional subtype associated with MEN1 gene mutations is PRL-PitNETs, accounting for approximately 42% of cases. Most are microadenomas (approximately 60%) and typically exhibit indolent behavior rather than invasive growth. Their treatment mainly involves dopamine agonists, with only a few patients requiring surgery. 16 The current in vitro models used for PitNETs include rat-derived cell lines and clinically isolated primary cells, whereas in vivo models mainly involve subcutaneous tumor xenografts in nude mice or estrogen-induced in situ PRL-PitNET in rats. Conventional cell culture methods are insufficient for elucidating the pathogenesis and tumor heterogeneity of PitNETs. In addition, in vivo models are largely limited to rat-derived cell transplantation. Therefore, the development of novel research tools is essential to advance the study of PitNETs.
Basic principles and developmental history of organoid technology
Traditional 2D cell culture systems are limited in their ability to recapitulate the 3D architecture and microenvironment of tumors, features essential for a comprehensive understanding of tumor biology. 17 Similarly, animal models such as murine xenografts face constraints because of species-specific differences and ethical considerations, which complicate the in-depth study of the pathogenesis of PitNETs. These limitations highlight the need for more physiologically relevant model systems. Organoids mark a major advance in personalized medicine, as they can be derived directly from patient samples to create individualized models of PitNETs. 3 The criteria for the successful construction of PitNET organoids are as follows: (a) stable passaging for more than three passages and maintaining good viability after recovery; (b) suitability for genetic-level analysis (whole-exome sequencing); (c) suitability for cellular-level analysis (hematoxylin and eosin (HE) staining and immunohistochemistry); and (d) suitability for functional-level analysis (hormone detection and drug response). This makes them particularly valuable for predicting drug responses and screening targeted therapies, bringing us closer to precision medicine for treatment of PitNETs. For example, testing dopamine agonist efficacy using organoids can help guide treatment choices tailored to each patient's specific tumor profile. 6 In addition, Mallick et al. constructed adrenocorticotropic hormone–secreting PitNET (ACTH-PitNET) organoids and used clustered regularly interspaced short palindromic repeats (CRISPR)/CRISPR-associated protein 9 (Cas9) to introduce common somatic mutations (such as USP8) to screen for therapeutic drug responses. 3 Beyond improving our understanding of tumor biology, this approach holds strong potential to enhance clinical outcomes through more effective and personalized therapeutic strategies.
Construction methods of organoids and key technological breakthroughs
The inception of organoid technology dates back to 2009, marked by the successful generation of intestinal organoids. 18 This breakthrough established a foundation for deriving organoids from diverse tissues such as the liver, kidney, and brain. Key advancements in the field include the standardization of 3D culture protocols, enabling the consistent production of organoids with well-defined characteristics. Organoids are 3D structures generated through the self-organization of stem cells or tissue-specific progenitor cells in vitro, which recapitulate the architectural and functional features of their corresponding organs.18,19 The construction of organoids typically relies on extracellular matrix (ECM)–derived materials, such as Matrigel or synthetic hydrogels, to provide a supportive scaffold for cellular growth. 20 The core component of Matrigel is laminin, which directly regulates cell adhesion, migration, and growth hormone (GH) secretion by binding to integrins on the cell surface. Second, the ECM includes collagen, which provides structural support and participates in cell signaling, and heparan sulfate proteoglycans, which form local activity gradients in the ECM by binding and stabilizing growth factors. Key growth factors, including epidermal growth factor (EGF),21,22 fibroblast growth factor (FGF), and activators of the Wnt signaling pathway, 23 are supplemented into the culture medium to guide cellular proliferation and differentiation. The cultivation of PitNET organoids requires supplementation with common cytokines, including EGF, the core driver of cell proliferation; FGFs (e.g. FGF-2, FGF-8b, and FGF-10), which provide essential signals for pituitary development and promote cell growth and specific subtype differentiation; and the Wnt signaling pathway activators WNT-3a and R-spondin 1, which maintain the long-term self-renewal of organoids. The incorporation of CRISPR/Cas9 gene editing has further empowered researchers to introduce disease-associated mutations into organoids, significantly improving their applicability for modeling pathogenesis. 24 Recent progress in microfluidic systems and 3D bioprinting has considerably enhanced the reproducibility and structural complexity of organoid models, enabling the generation of more physiologically accurate and high-fidelity systems for disease modeling and drug screening. 25
These technological advances are instrumental in enabling the precise manipulation of the organoid microenvironment. Such precision is paramount for elucidating intricate cellular interactions and responses to diverse stimuli, processes that are vital for advancing our understanding of organogenesis and disease mechanisms.26,27 These developments have established organoids as indispensable tools in cancer research by providing unprecedented insights into tumor biology and mechanisms of therapeutic response.4,27,28
Current challenges and limitations
Despite the rapid progress in organoid technology, several challenges and limitations remain. The high cost of culture materials, prolonged generation time, and substantial batch-to-batch variation present significant barriers to the broad adoption of organoids in both research and clinical applications.29–31 Moreover, current organoid models often do not fully recapitulate the in vivo microenvironment, particularly because they lack vascularization and interactions with immune cells, which are essential for modeling complex diseases such as PitNETs. 5 These limitations may be overcome by enabling endothelial cells to form a microvascular network, introducing immune cells during perfusion, and embedding organoids near the vascular network to simulate the recruitment and infiltration of immune cells within the tumor microenvironment. 32 In addition, during the cultivation of PitNET organoids, stem/progenitor cells are preferentially preserved and expanded, enabling multiple passages, the establishment of biobanks, and support for large-scale drug screening and mechanism research. However, the loss of tumor heterogeneity (e.g. drug resistance or tumor cell invasion) during organoid culture may affect the evaluation of drugs and disease progression. During long-term culture, the growth-promoting effects of high-level hormone secretion may diminish, thereby affecting the evaluation of endocrine therapy. Even when drug responses are positive in vitro, equivalent therapeutic effects may not be achieved in vivo. Furthermore, in glioma research, recent studies have incorporated immune components into the construction and application of organoid models. Baisiwala et al. developed an immune-human brain organoid tumor transplantation (iHOTT) model, in which tumor cells derived from patients with glioblastoma and autologous peripheral blood mononuclear cells (PBMCs) were co-implanted into human brain cortical organoids to establish an autologous co-culture platform. 33 This model preserves the composition of immune cells, immune signaling pathways, and intercellular interactions within the patient's tumor. The changes in cell type and cell–cell interactions observed after treatment with pembrolizumab are highly consistent with those observed in patients. Salvato et al. delivered the major histocompatibility complex (MHC)-II transactivator (CIITA) gene into glioblastoma organoids using an adenoviral vector. 34 After co-culturing these treated organoids with PBMCs or isolated T cells, significant organoid disintegration and tumor cell death were observed. This cytotoxic effect depended on the participation of cluster of differentiation (CD) 8 (CD8)+ and CD4+ T cells as well as direct contact between T cells and tumor cells. The future construction and application of PitNET organoids may focus on the following aspects: (a) establishing a PitNET-autologous PBMC co-culture module to investigate interactions between T cells and tumor organoids and evaluate the sensitivity to immune checkpoint inhibitors or cell therapy; (b) integrating induced pluripotent stem cell (iPSC)–derived pituitary-specific endothelial cells and macrophages to build a pituitary tumor organoid–immune–vascular assembly that more closely resembles the in vivo 3D structure; and (c) using CRISPR or viral vectors to engineer the tumor–immune interface (e.g. MHC-II/CIITA and programmed cell death-ligand 1 (PD-L1)) in PitNET organoids to actively regulate immune recognition ability. Overcoming these limitations is crucial to enhancing the reliability and translational potential of organoids in biomedical research, especially in the fields of personalized medicine and targeted tumor therapy.27,35
Application of organoids in modeling PitNETs
Methods for establishing PitNET organoid models
The development of organoid models derived from PitNET tissue represents a major advance in endocrine tumor research. These models are typically generated by isolating stem cells from surgically resected PitNET specimens or by differentiating iPSCs into pituitary lineages.3,5,7 The process involves optimizing culture conditions through the precise selection of growth factors and ECM components that support pituitary cell survival and expansion. 3 Zou et al. digested fresh surgical tumor specimens (clinically diagnosed as GH-PitNETs) and cultured them in defined medium supplemented with Matrigel, generating GH-PitNET organoids that recapitulated the structure and function of the primary tumors. 2 Validation of these organoids demonstrated that FB23-2 (an FTO inhibitor) combined with octreotide (a somatostatin analog) significantly enhanced the sensitivity of the organoids to octreotide and inhibited GH secretion. Mallick et al. established two types of organoid models for PitNETs associated with Cushing disease: (a) genetically engineered iPSC-derived organoids, in which CRISPR/Cas9 was used to edit healthy human iPSCs by introducing the somatic mutations USP48 and USP8, which are commonly found in Cushing disease, followed by successful differentiation into organoids exhibiting the characteristics of corticotroph tumors, including high ACTH secretion; and (b) patient-derived organoids, generated directly from fresh surgical tumor tissue obtained from patients with Cushing disease, which retained the pathological features and hormone secretion function of the primary tumors.3,7 Research has shown that relacorilant can induce cell death and increase sensitivity to pasireotide, providing a mechanistic basis and preclinical evidence for the combined treatment of Cushing's disease with relacorilant and pasireotide. Nys et al. successfully established and optimized an organoid culture system derived from pituitary tumor tissue of Drd2−/− mice. 5 These organoids, originating from SRY-box transcription factor 2 (SOX2)+ stem cells, expressed key stem cell markers, including SOX2, SOX9, and tumor-associated calcium signal transducer 2 (TACSTD2), and faithfully recapitulated the activated tumor stem cell phenotype of the original tumors. 5 Mouse tumor organoids can faithfully reproduce this activated phenotype, including increased proliferative activity and elevated expression of cytokines- and chemokine-related genes, and depend on interleukin-6 (IL-6) signaling. Human pituitary tumor organoids can be established efficiently and preserve patient-specific features; however, their expansion capacity is severely limited, which may be related to regression of cytokine signaling pathways, aging, and apoptosis. Cheng et al. established a patient-derived organoid model from dopamine agonist-resistant prolactinomas using a 3D culture method, which was subsequently applied to investigate drug resistance mechanisms and conduct high-throughput drug screening. 6 For the first time, a dopamine agonist-resistant PRL-PitNET organoid model was established and used for large-scale drug screening. Genistein was identified as a potentially effective drug that exerts antitumor effects by inhibiting the focal adhesion signaling pathway, providing a new treatment strategy for refractory PRL-PitNETs. The construction and application of organoids in current research on PitNETs are shown in Table 1.2–7
Research on organoids in PitNETs.
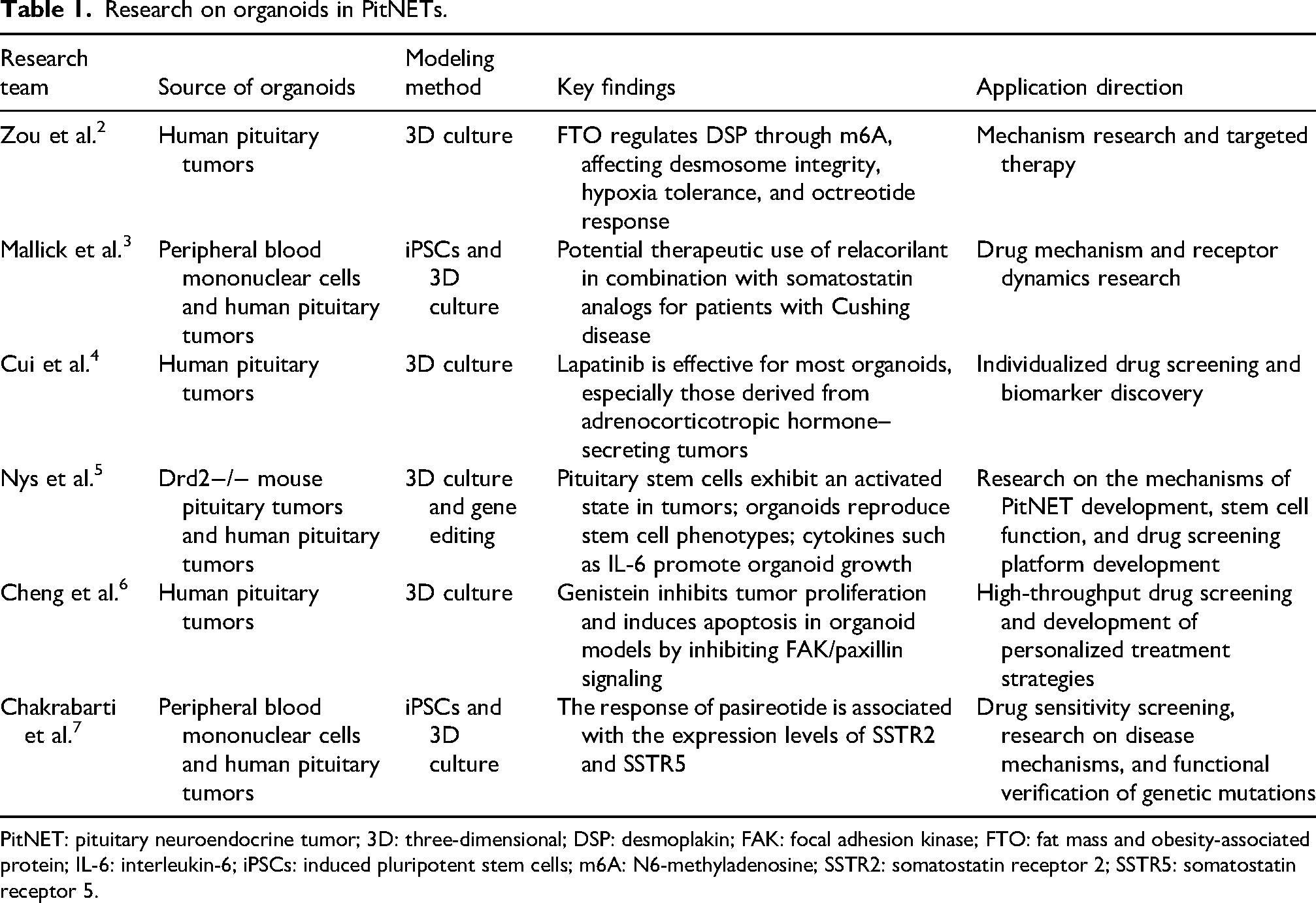
PitNET: pituitary neuroendocrine tumor; 3D: three-dimensional; DSP: desmoplakin; FAK: focal adhesion kinase; FTO: fat mass and obesity-associated protein; IL-6: interleukin-6; iPSCs: induced pluripotent stem cells; m6A: N6-methyladenosine; SSTR2: somatostatin receptor 2; SSTR5: somatostatin receptor 5.
This rigorous methodological framework enables the establishment of highly representative models that mimic the in vivo microenvironment of PitNETs, thereby offering a powerful platform for investigating tumor biology and evaluating novel therapeutic approaches.36,37
High-throughput drug screening platforms
Organoids have become pivotal tools for drug screening, particularly in high-throughput applications. Their capacity to recapitulate the architectural and microenvironmental complexity of tumors enables the development of miniaturized screening platforms capable of efficiently testing large libraries of pharmacological compounds.38–40 Using a 3D organoid culture model, Cui et al. screened a panel of 10 drugs, including temozolomide, lapatinib, and cabergoline, and observed substantial heterogeneity in drug responses among organoids derived from different subtypes and treatment backgrounds of PitNETs. 4 These findings provide a valuable foundation for developing personalized therapeutic strategies for patients with PitNETs. However, the study suggests that some organoids may not maintain the molecular characteristics or drug response consistency of the primary tumor after passaging. In addition, some patients may have received treatments such as radiotherapy and bromocriptine before surgery, which may alter the biological characteristics of the tumors and affect the results of drug screening based on postoperative organoids.
Cheng et al. established 3D organoid cultures from drug-resistant PRL-PitNETs in 18 of 22 patients. Using 8 of these organoid lines for high-throughput screening of 180 small-molecule antitumor compounds, they found that genistein produced an inhibition rate exceeding 30% in 5 of the 8 samples, highlighting its potential as a promising therapeutic agent. 6 Although organoids were successfully established from 22 cases of drug-resistant tumors, only 8 organoid lines were used for high-throughput drug screening because of limited tissue availability, which may not fully represent the heterogeneity of dopamine agonist-resistant PRL-PitNETs. Chakrabarti et al. used 3D culture and iPSC-derived organoids for high-throughput drug screening. They found that organoids from different patients exhibited individual variability in their responses to drugs, such as pasireotide and cabergoline, mirroring the heterogeneous treatment responses observed clinically. 7 A total of 35 patients, including 12 with functional ACTH-secreting tumors, were included; however, the number of organoids used for drug screening was not fixed. Significant differences in drug responses were observed among different tumor subtypes (e.g. sparse granule and Crooke cell types) and among individuals, but the limited sample size precluded statistically robust subgroup analyses. Although PitNET organoids currently have limitations in drug screening research, including tumor heterogeneity, limited tissue availability, and single-point drug testing, this approach not only improves the accuracy of drug screening but also substantially enhances throughput, enabling the simultaneous assessment of thousands of compounds. By leveraging organoid technology, researchers can improve the prediction of patient-specific therapeutic responses, thereby advancing the development of treatment strategies tailored to individual tumor characteristics.8,27,41
Strategies for achieving personalized medicine
The emergence of organoid technology has transformed the landscape of personalized medicine, especially in oncology. By creating patient-derived organoids, clinicians can effectively conduct “drug trials in a dish” that simulate an individual's tumor microenvironment, enabling the prediction of therapeutic responses to agents such as octreotide or temozolomide. 3 In this approach, patient-derived PitNET organoids are used as a personalized drug screening platform to predict individual responses to candidate therapeutic agents. Organoids established from surgically resected tumor tissue from individual patients can be used to predict responses to specific drugs, guide postoperative adjuvant therapy or drug selection after recurrence, and retrospectively compare in vitro half-maximal inhibitory concentration (IC50) values with subsequent clinical treatment responses. This approach markedly reduces the reliance on trial-and-error treatment selection, which is particularly valuable for patients with resistant PitNETs. Organoid models facilitate the design of tailored combination therapies based on the unique biology of each tumor, thereby improving the likelihood of successful treatment. Furthermore, drug sensitivity testing using these organoids provides critical information to guide clinical decision making by helping to prioritize the most effective therapeutic options for each patient. By aligning treatment with individual tumor profiles, this personalized strategy not only enhances therapeutic efficacy but also spares patients from ineffective treatments, ultimately leading to more refined and optimized clinical care.42–44
Challenges and optimization directions
Despite the considerable promise of organoids in drug screening and personalized medicine, several challenges impede their widespread adoption. A major obstacle is the lack of standardization and scalability in organoid culture protocols, as variations in growth conditions often compromise reproducibility. 45 Furthermore, current organoid models frequently lack critical microenvironmental components, such as vascularization and immune interactions, which are essential for accurately predicting drug responses. 46 Future efforts should prioritize the development of advanced co-culture systems that integrate stromal and immune cells to enhance the biological fidelity of organoids. Additionally, emerging technologies such as 3D bioprinting and microfluidics offer promising avenues for constructing more physiologically relevant organoid models that better mimic the in vivo tumor niche. 47 Addressing these limitations will be crucial to accelerating the translation of organoid technology from bench to bedside, ultimately improving the efficiency of drug discovery and the implementation of personalized treatment strategies.44,48,49
Ethical and regulatory considerations
The integration of organoid technology into regenerative medicine and gene therapy presents complex ethical and regulatory challenges that must be carefully addressed to ensure its responsible development. A major ethical concern involves the possibility that highly developed organoids, particularly those modeling complex organs, may exhibit features associated with consciousness or sentience. 50 This underscores the need for rigorous ethical frameworks governing informed consent and the use of human-derived tissues. Regulatory obstacles, such as securing approval from the US Food and Drug Administration (FDA) for clinical applications, further complicate the translation of organoid-based therapies from research to practice. In the context of PitNETs, it is imperative to balance innovation with ethical integrity, ensuring that patient safety and welfare remain paramount. Sustained collaboration among researchers, ethicists, and regulatory agencies is essential to establish clear guidelines that promote the safe and ethically sound application of organoid technology in clinical environments.51,52
Future directions and comprehensive challenges
Standardization and clinical translation pathways
To ensure the reliability and reproducibility of organoid research, it is essential to establish standardized, internationally harmonized protocols for organoid culture and characterization. Such standardization will improve the comparability of data across laboratories and strengthen the credibility of organoid-based findings for clinical applications. To support clinical translation, large-scale prospective clinical studies are needed to validate the accuracy of organoids in predicting patient-specific treatment responses. These studies will be critical for incorporating organoid technology into mainstream clinical practice and developing evidence-based guidelines. Furthermore, overcoming challenges related to scalability and consistency in organoid production is necessary to enable widespread clinical adoption. By systematically demonstrating the predictive value of organoids in therapeutic contexts, researchers can pave the way for their routine use in clinical settings, ultimately improving patient outcomes through more personalized and effective treatment strategies.49,53
Addressing global health challenges
Organoid technology offers considerable potential for mitigating the global health burden posed by PitNETs, especially in resource-limited settings.4,5 By advancing low-cost culture techniques and incorporating telemedicine platforms, researchers can make organoid-based diagnostics and treatments more accessible in underserved regions. Promoting equitable access to these innovations is critical. To this end, educational programs designed to train local healthcare workers in organoid methodologies will play a vital role. Additionally, establishing partnerships among academic institutions, healthcare providers, and policymakers can improve the dissemination of expertise and resources. Through focused efforts in these areas, organoid technology may help foster a more inclusive global health landscape, ensuring that advances in PitNET research benefit all patients, irrespective of geographic or socioeconomic barriers.54,55
Conclusion
The emergence of organoid technology has marked a transformative shift in the study of PitNETs, substantially advancing our understanding of the biological mechanisms underlying these tumors. By enabling the development of highly sophisticated in vitro models that closely recapitulate the in vivo microenvironment, organoids have unlocked new research opportunities beyond the reach of traditional experimental systems. This innovative methodology not only enhances our understanding of tumor pathophysiology but also expedites the discovery of novel therapeutics and the development of personalized treatment approaches tailored to individual patients.
From an expert perspective, integrating organoid technology into PitNET research requires a balanced synthesis of diverse scientific perspectives and findings. A key strength of organoids lies in their capacity to emulate the intricate architecture and cellular heterogeneity of pituitary tissue, thereby providing more faithful models of tumor behavior and drug sensitivity. This capability carries significant implications for drug development, as organoid platforms enable high-throughput screening of compound libraries, improving the efficiency of identifying promising treatment candidates.
Nevertheless, several challenges must be overcome to fully realize the potential of organoid models. Standardization of culture protocols remains a major obstacle, as current variability may compromise reproducibility and comparability across studies. Ethical considerations regarding the use of human-derived tissues also warrant careful attention to ensure compliance with ethical standards without hindering scientific progress. Additionally, technical challenges such as scaling production and establishing sustainable biobanking infrastructures are critical for the broader clinical integration of organoid technology.
Looking forward, the role of organoids in the management of PitNETs will depend on multidisciplinary collaboration and successful clinical translation. Partnerships among researchers, clinicians, and industry are essential to foster innovation and continuously refine organoid models. Such collaboration will improve the robustness and clinical relevance of organoid-based research, helping to bridge the gap between laboratory findings and patient care.
The integration of cutting-edge technologies, such as CRISPR-based gene editing, single-cell sequencing, and artificial intelligence, promises to further elucidate the molecular landscape of PitNETs. These tools can uncover genetic and epigenetic alterations at unprecedented resolution, revealing new therapeutic targets and biomarkers for personalized treatment.
In conclusion, organoid technology constitutes a landmark innovation in PitNET research, providing an unprecedented platform for investigating tumor biology and advancing precision medicine. Although challenges remain, a coordinated effort across the scientific community will be essential to address these limitations and fully realize the potential of organoids. As organoid models continue to improve and clinical adoption increases, a new paradigm in the management of PitNETs is emerging, with the potential to substantially improve patient prognosis and quality of life. Sustained collaboration and technological innovation will be integral to establishing organoid technology as a cornerstone of future research and clinical practice in this field.
Footnotes
Ethics approval
Not applicable.
Author contributions
All authors contributed to the study conception and design. Data collection, analysis, and revision were performed by Shaolin Zhang, Yonghong Zhu, Jun Shen, Zeyu Lin, Zhang Xiong, and Xiaochun Jiang. The first draft of the manuscript was written by Qing Rao, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Natural Science Foundation of China (82470816), the Natural Science Research Project in Higher Education of Anhui Province (2024AH051948), the Special Research Start-up Foundation for Introduced Talents (YR20230138), and the Anhui Provincial Health Research Project (AHWJ2024Ab0097).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
No datasets were generated or analyzed during the current study.