
Abstract
Background and objective
Developmental dysplasia of the hip is a common musculoskeletal condition in children. Although surgery is often required, the use of general anesthesia can lead to complications that may delay recovery. Regional anesthesia offers a means of reducing these risks; however, its use in children is often limited by challenges in patient cooperation. At our institution, regional anesthesia has been routinely employed for these procedures. This study retrospectively reviewed data from children who underwent surgery for developmental dysplasia of the hip under regional anesthesia over the past 6 years, stratified by age group. The aim was to provide evidence regarding the optimal anesthetic approach for these procedures.
Methods
A comprehensive database was established comprising 1254 pediatric patients who underwent surgery for developmental dysplasia of the hip between 1 January 2018 and 31 December 2023. The study included children classified as American Society of Anesthesiologists physical status I–II, who were categorized into three age-based groups: (a) low age (Group L, 0–36 months); (b) middle age (Group M, 36–96 months); and (c) high age (Group H, 96–156 months). The primary outcome was the use of regional anesthesia across the three groups, including the overall utilization rate and the distribution of specific regional anesthesia techniques. Secondary outcomes included anesthetic and surgical characteristics, including anesthesia methods, anesthesia duration, postanesthesia recovery time, surgical procedures, operative duration, intraoperative blood transfusion rates, and hemoglobin levels before and after surgery.
Results
We analyzed 1254 pediatric patients with developmental dysplasia of the hip and found that 99.8% received general anesthesia, 64.4% received regional anesthesia, and 64.2% underwent combined general and regional anesthesia. Group M included the largest number of patients, whereas Group H had the highest rate of regional anesthesia utilization (P < 0.05). Regarding regional anesthesia techniques, caudal anesthesia was the most commonly used in Group L, whereas the fascia iliaca compartment block was increasingly used in Groups M and H (P < 0.05). Combined intravenous–inhalational anesthesia with mechanical ventilation was predominantly used in Groups L and M (P < 0.05). The use of sevoflurane for general anesthesia was highest in Group L and gradually decreased in Groups M and H (P < 0.05). Although surgical complexity increased with age, as reflected by more complex procedures, higher intraoperative blood transfusion rates, and longer anesthesia, and operative durations (P < 0.05), Group H had a shorter postanesthesia recovery time than Groups L and M (P < 0.05). The high utilization of regional anesthesia in Group H was associated with improved postoperative recovery in children undergoing surgery for developmental dysplasia of the hip and was consistent with the principles of Enhanced Recovery after Surgery.
Conclusion
Regional anesthesia is widely used in pediatric orthopedic hip surgery. However, the choice of regional anesthesia technique varies considerably with patient age, reflecting differences in anesthetic requirements and surgical characteristics. Younger children most commonly receive caudal anesthesia, whereas older children are more frequently managed with alternative regional techniques, including the fascia iliaca compartment block, lumbar plexus block, and quadratus lumborum block.
Keywords
Introduction
Developmental dysplasia of the hip (DDH) represents the most common clinical form of hip disorders in children. 1 As a spectrum of musculoskeletal conditions affecting healthy hip development, DDH has an overall incidence of 1–3 per 1000 live births. Genetic and environmental factors both contribute to its etiology. Given China's large population, with 15.23 million births reported in 2018, and the notably higher incidence observed in some remote regions, DDH represents a substantial clinical burden in pediatric practice. 2 Orthopedic surgery remains the definitive treatment for DDH. These procedures are often complex, involve extensive surgical exposure, and typically require general anesthesia (GA) in pediatric patients. 3
Regional anesthesia (RA) is well established in adult hip surgery because of its clinical benefits. However, certain RA techniques pose challenges and risks in children because of limited cooperation, which has restricted their broader application in clinical practice.4,5 Within the Enhanced Recovery After Surgery (ERAS) framework, RA is strongly recommended as a core strategy to complement GA in pediatric surgery. 6 When effectively implemented, RA can significantly reduce opioid consumption, improve hemodynamic stability, provide better postoperative pain control, and decrease the incidence of postoperative adverse events.7,8 Although ERAS protocols have gained increasing adoption in China since 2018, the optimal use of RA in pediatric hip surgery remains uncertain, and standardized recommendations are still lacking. 6
At our institution, RA has long been an integral part of routine practice across the full spectrum of pediatric surgical procedures. This study retrospectively analyzed RA practices in DDH surgery over a 6-year period, with particular focus on anesthetic and surgical characteristics across different age groups. Our objective was to generate robust clinical evidence to support anesthesia selection for DDH, thereby facilitating the implementation of ERAS protocols in pediatric hip surgery and ultimately improving postoperative outcomes.
Patients and methods
Study design
The study protocol was approved by the Ethics Committee of Beijing Jishuitan Hospital, Capital Medical University (Approval Number: K2024-475–00; date: 29 October 2024). Written informed consent forms were signed by the guardians of the children. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki, as revised in subsequent amendments.
This retrospective observational study utilized data from the hospital's electronic medical record system (EMRS), which contains comprehensive patient information, including detailed preoperative, intraoperative, and postoperative records from hospitalization.
Participants
We reviewed the records of all pediatric patients who underwent orthopedic surgery for DDH at Beijing Jishuitan Hospital between 1 January 2018 and 31 December 2023. The study included children diagnosed with DDH who underwent unilateral hip open reduction, acetabular osteotomy, or pelvic osteotomy. Exclusion criteria were as follows: (a) age ≥13 years; (b) American Society of Anesthesiologists (ASA) physical status III–IV; (c) mental or psychological disorders; (d) coexisting neurological or motor system conditions, including cerebral palsy, multiple joint contractures, or congenital meningocele; (e) severe spinal deformity; (f) coagulopathy; (g) minimally invasive procedures, such as hip arthroscopy or bilateral or multisite surgery; and (f) direct postoperative transfer to the intensive care unit (ICU). Eligible participants were stratified into three age-based groups: low age (Group L, 0–36 months), middle age (Group M, 36–96 months), and high age (Group H, 96–156 months).
Data collection
We extracted the following data for analysis: (a) general patient information from admission and discharge records (e.g. name, hospitalization identification code, sex, age, date of birth, height and weight, principal and secondary diagnoses, past medical history and systemic diseases, admission and discharge date, length of stay, and discharge status); (b) surgical details from progress notes and surgery records (e.g. DDH severity based on the Crowe classification, surgical date, surgical approach, operative duration, intraoperative blood transfusion requirements, hemoglobin (Hb) levels before surgery and on the first postoperative day, and preoperative albumin (Alb) levels); (c) anesthesia-related information from anesthesia records and postoperative visit sheets (e.g. ASA physical status, anesthesia method and airway management, anesthesia duration, anesthetic and analgesic agents, postanesthesia recovery time, and, most importantly, the use of RA.
Observation indicators
The primary outcome was the utilization of RA across the three age groups. This included both the overall rate of RA use and the distribution of specific RA techniques: caudal anesthesia (CA), spinal anesthesia (SA) or epidural anesthesia (EA), lumbar plexus block (LPB), fascia iliaca compartment block (FICB), and quadratus lumborum block (QLB). For each age group, the overall RA utilization rate was calculated as follows: R (%) = (number of RA cases/total cases in the group) × 100%. The proportion of each specific RA technique was calculated as follows: P (%) = (number of cases using the specific RA technique/total RA cases in the group) × 100%.
One secondary objective focused on characterizing anesthesia practices. We analyzed GA utilization rates, mechanical ventilation use, anesthesia duration, and postanesthesia recovery time across the three age groups. GA was administered as either combined intravenous–inhalational anesthesia (CIVIA) or total intravenous anesthesia. Standard anesthetic agents in our department included sevoflurane, propofol, etomidate, and esketamine, typically combined with opioids such as fentanyl, sufentanil, or remifentanil. Airway management involved either endotracheal intubation or a laryngeal mask airway (LMA). The GA utilization rate and mechanical ventilation rate were calculated as follows: R (%) = (number of cases using the technique/total cases in the group) × 100%. The utilization proportion of specific drugs or airway devices was calculated as follows: P (%) = (number of cases using a specific drug or device/total cases in the group) × 100%. Postanesthesia recovery time was defined as the interval from discontinuation of anesthetic agents to discharge from the postanesthesia care unit. Recovery was assessed using the Steward score, with a score of ≥4 considered suitable for discharge to the ward.
Surgical characteristics were another secondary objective. We analyzed specific surgical approaches, operative duration, intraoperative blood transfusion rates, and Hb levels before and after surgery. The surgical procedure consists of several steps. The osteotomy around the acetabulum, involving all or part of ilium, ischium, and pubis, could be performed as triple osteotomy, Salter osteotomy, Ganz osteotomy, Pemberton osteotomy, Dega osteotomy, or Chiari osteotomy. Proximal femoral osteotomy and adductor-iliopsoas tenotomy, although not performed in all patients, were crucial procedures for children with severe dislocation and difficult reduction. The proportion of each surgical approach was calculated as follows: P (%) = (number of cases undergoing the specific procedure/total cases in the group) × 100%. Intraoperative blood transfusions included red blood cell (RBC) suspensions, fresh frozen plasma (FFP), or intraoperative cell salvage (IOCS). Transfusion rates and the distribution of transfusion types were calculated as follows: R (%) = (number of transfused cases/total cases in the group) × 100%; P (%) = (number of uses of a specific blood product/total transfused cases in the group) × 100%.
Statistical analysis
All cases that met the predefined eligibility criteria within the specified study period were included in the database. Statistical Package for the Social Sciences (SPSS) 20.0 (Chicago, IL, USA) was used for data analysis. Continuous data were assessed for normality using the Shapiro–Wilk test. Data that conformed to a normal distribution were expressed as the mean ± SD and analyzed using one-way analysis of variance (ANOVA), followed by the least significant difference (LSD) test for pairwise comparisons among the three groups. Data that did not follow a normal distribution were presented as the median (M) with interquartile ranges (IQR) and analyzed using the Mann–Whitney U test. Categorical data were expressed as counts (n) and percentages (%). These data were analyzed using the chi-squared test or Fisher's exact test, as appropriate. A P-value of <0.05 was considered statistically significant.
Results
Demographics
Based on the predefined criteria, we initially identified 1498 eligible cases. After applying the exclusion criteria—157 patients aged ≥13 years, 45 with cerebral palsy, 5 with meningocele, 12 with severe spinal deformity, and 25 who underwent minimally invasive, bilateral, or multisite surgery—a total of 1254 cases were included in the final analysis (Figure 1).
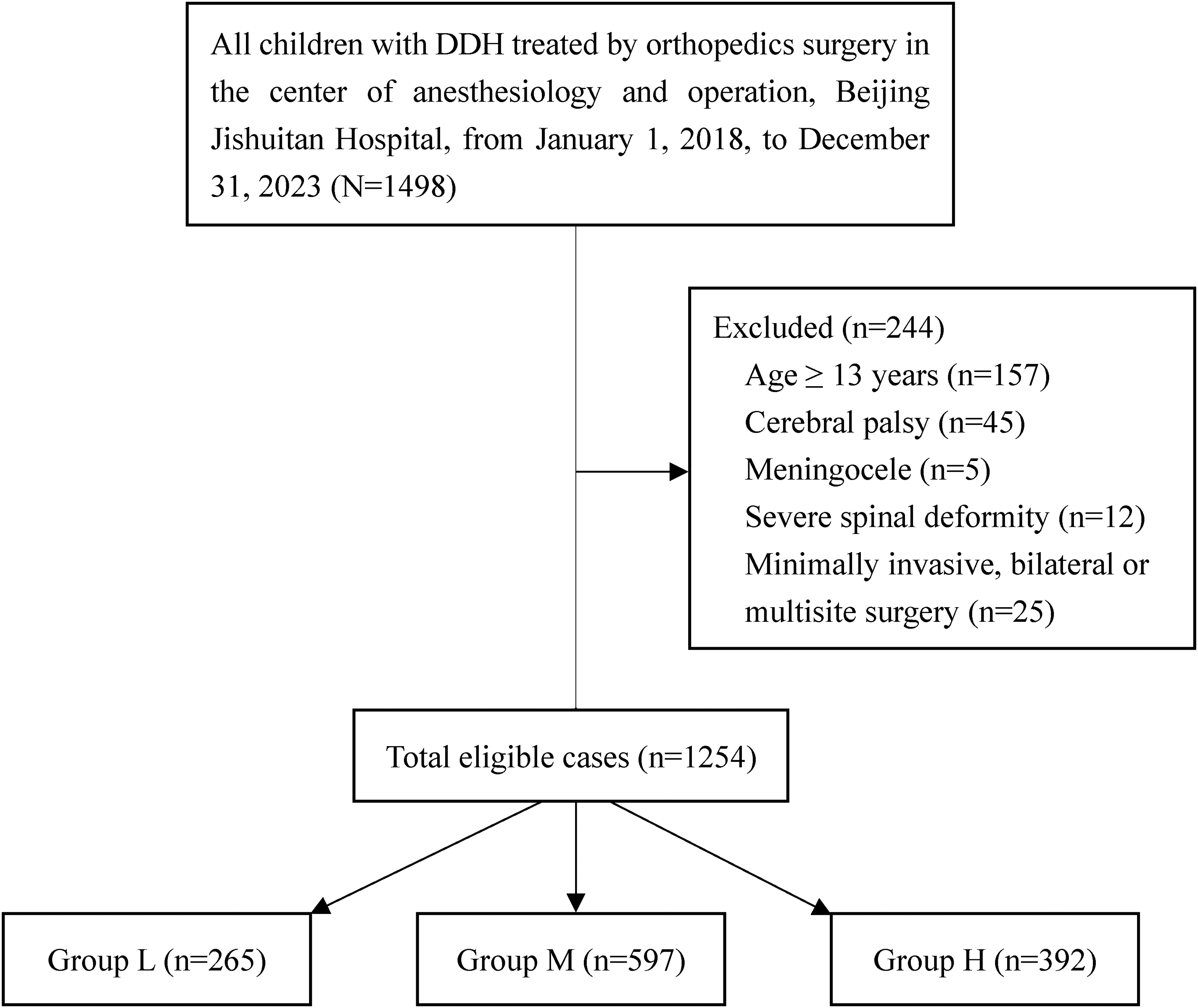
Flowchart showing children’s selection according to our study inclusion and exclusion criteria.
The cohort consisted of 426 males and 828 females, with a mean age of (75.1 ± 37.7) months and a mean body mass index (BMI) of (17.0 ± 2.1) kg/m2. All children were classified as ASA physical status I–II. The youngest child in the study was 19 months old. No significant differences were observed in BMI, ASA physical status, or preoperative Alb levels among the three age groups. However, Group L showed a significantly higher proportion of female patients than Groups M and H (P < 0.05), whereas no significant difference in sex distribution was observed between Groups M and H (Table 1).
Baseline characteristics across the three age groups.
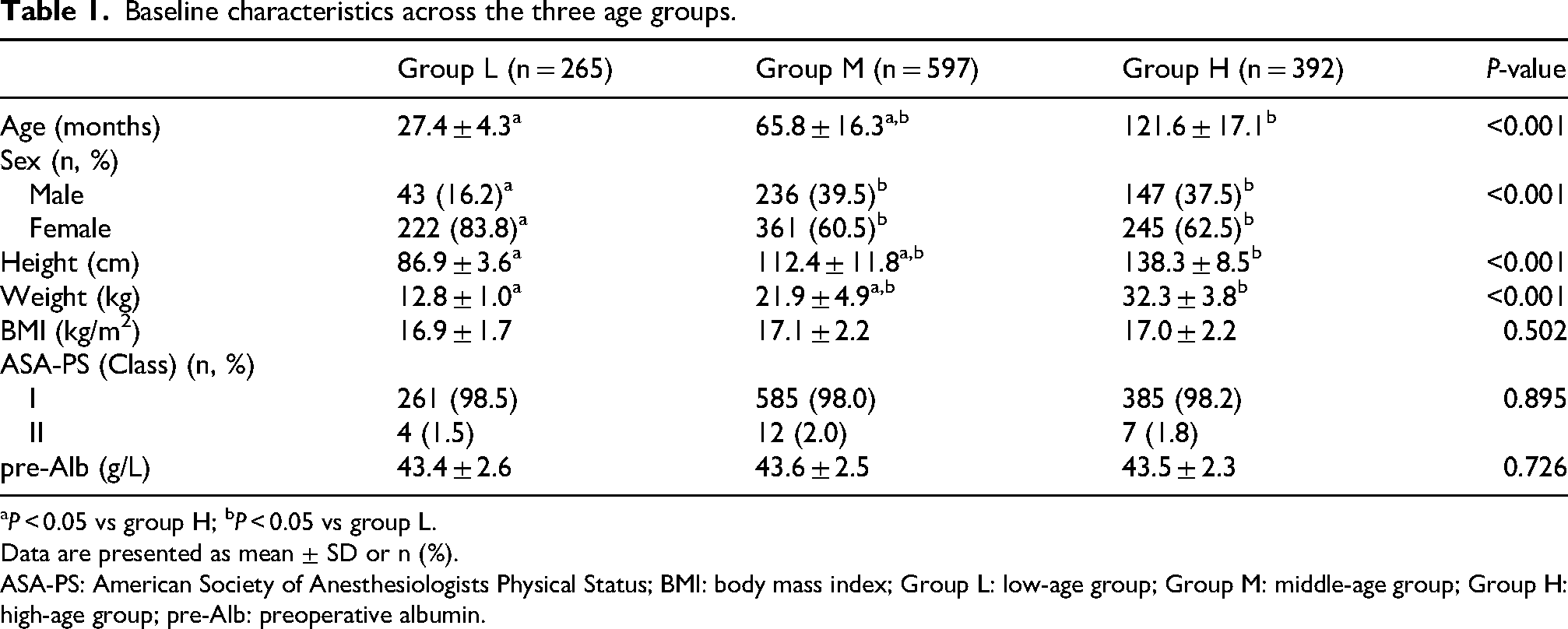
P < 0.05 vs group H; bP < 0.05 vs group L.
Data are presented as mean ± SD or n (%).
ASA-PS: American Society of Anesthesiologists Physical Status; BMI: body mass index; Group L: low-age group; Group M: middle-age group; Group H: high-age group; pre-Alb: preoperative albumin.
The study population comprised 265 children (21.1%) in Group L, 597 (47.6%) in Group M, and 392 (31.3%) in Group H, with significant differences in group distribution (P < 0.05). From 2018 to 2023, Group M consistently had the highest annual number of cases. This pattern persisted throughout the coronavirus disease 2019 (COVID-19) pandemic (2020–2022), as shown in Figure 2. Furthermore, Group H exhibited a significant increase in the number of cases in 2023 compared with both 2018 and 2019 (P < 0.05), whereas Group M did not demonstrate similar growth. This increase in Group H may reflect the progression of children who were previously in Group M during the pandemic and subsequently underwent surgical treatment at an older age.
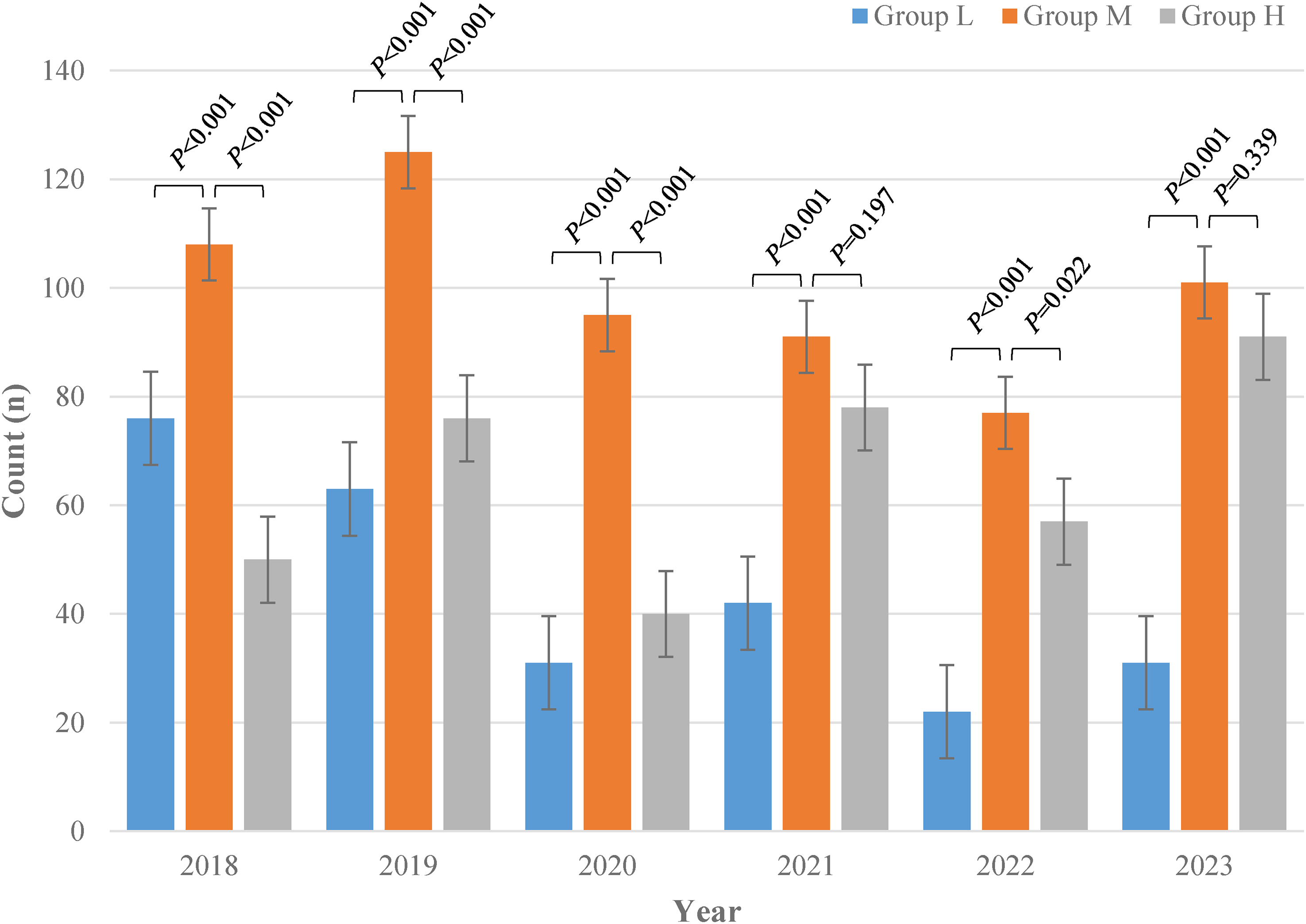
Bar chart showing the number of children in three groups from 1 January 2018 to 31 December 2023 (including the 3 years of COVID-19 pandemic: 2020, 2021, and 2022).
Application of RA
We observed 1251 cases involving GA, accounting for 99.8% of the total; 808 cases involving RA, accounting for 64.4%; and 805 cases in which GA was combined with RA, accounting for 64.2%. Group H exhibited the highest rate of RA utilization (P < 0.05).
In Group L, the most commonly used RA technique was CA, accounting for a significantly higher proportion than in Groups M and H. Conversely, SA or EA was more commonly used in Group H (P < 0.05). Children in Groups M and H showed a significantly higher proportion of FICB than those in Group L (P < 0.05). Additionally, LPB and QLB were used in a limited number of cases and were not used in Group L (Table 2).
Application of RA across the three age groups.
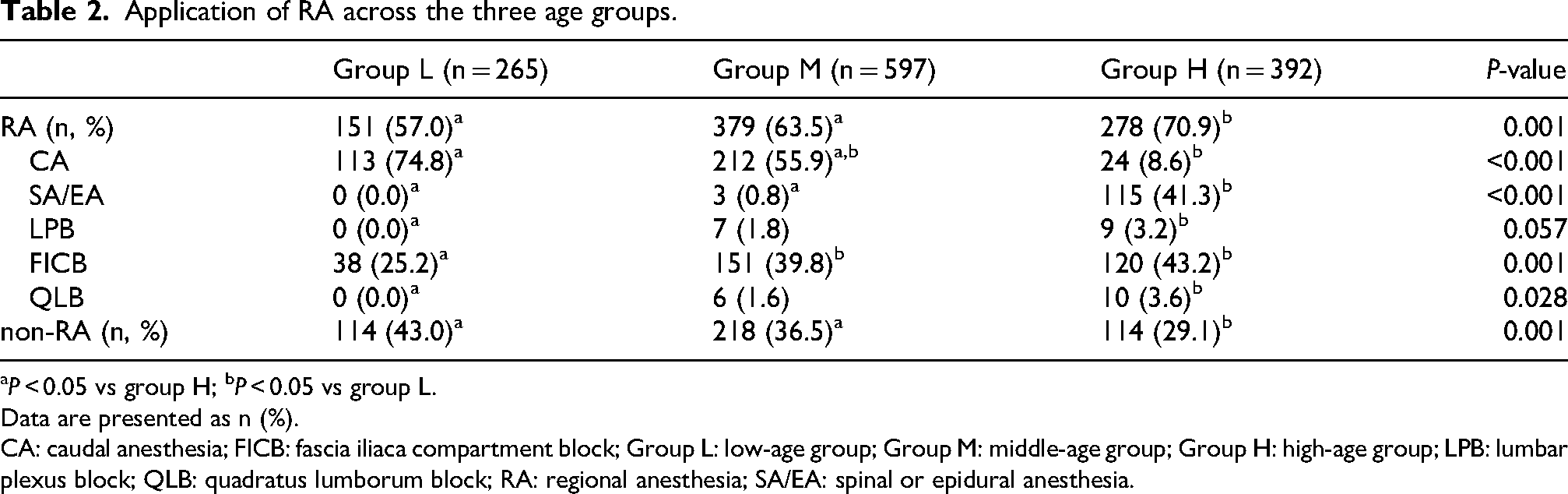
P < 0.05 vs group H; bP < 0.05 vs group L.
Data are presented as n (%).
CA: caudal anesthesia; FICB: fascia iliaca compartment block; Group L: low-age group; Group M: middle-age group; Group H: high-age group; LPB: lumbar plexus block; QLB: quadratus lumborum block; RA: regional anesthesia; SA/EA: spinal or epidural anesthesia.
GA characteristics
The utilization rate of GA in both Group L and Group M was 100%, significantly higher than that in Group H (P < 0.05). CIVIA with mechanical ventilation was more commonly used in Groups L and M (P < 0.05). Group L exhibited the highest proportion of sevoflurane use for GA, with a gradual decline from Group L to Group M and from Group M to Group H (P < 0.05). The utilization proportion of remifentanil was highest in Group H (P < 0.05). The mechanical ventilation rate in Group L was 100% and did not differ significantly from that in Group H (P < 0.05). Endotracheal intubation was the most commonly used airway device in all groups, with a significantly higher utilization proportion in Group L than in Groups M and H (P < 0.05). However, the utilization proportion of LMA was significantly higher in Groups M and H than in Group L (P < 0.05).
The anesthesia duration was similar between Groups M and H, and both were significantly longer than that in Group L (P < 0.05). However, Group H demonstrated a significantly shorter postanesthesia recovery time than Groups L and M (P < 0.05) (Table 3).
GA characteristics across the three age groups.
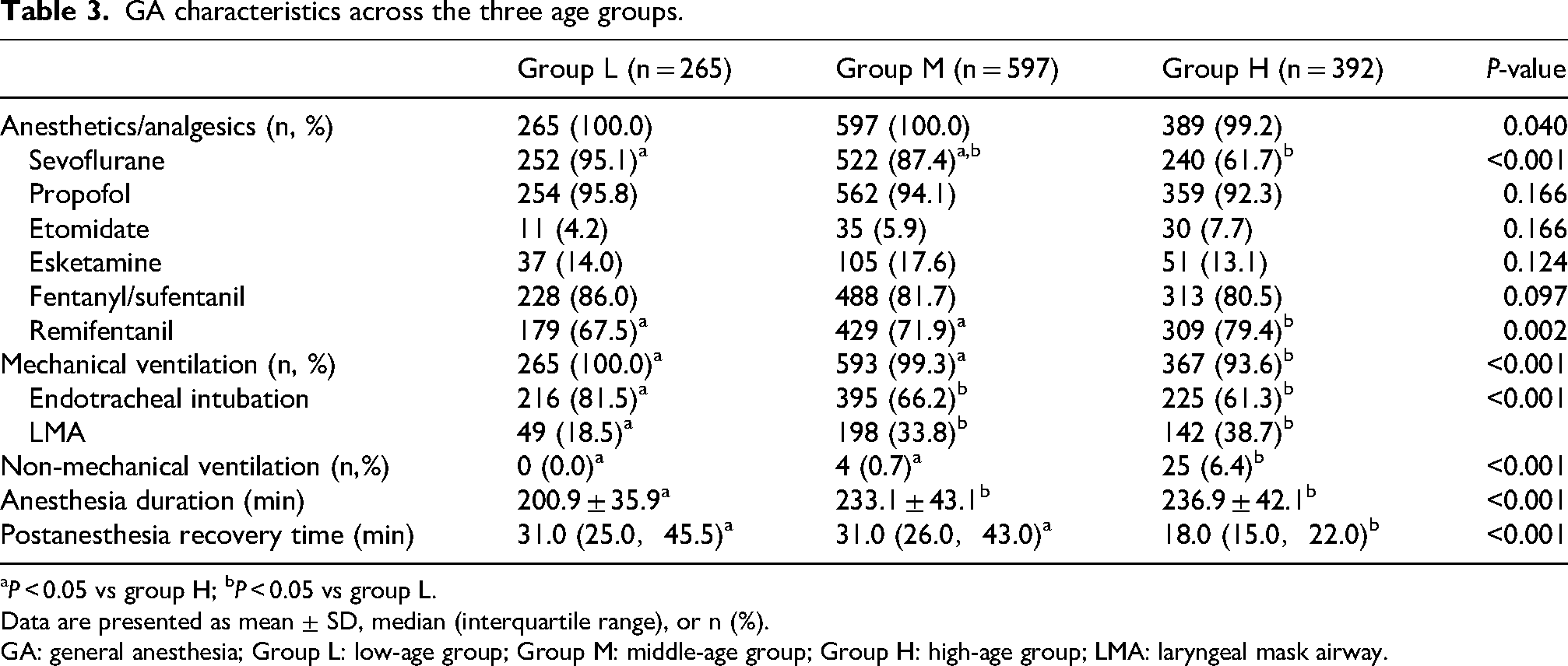
P < 0.05 vs group H; bP < 0.05 vs group L.
Data are presented as mean ± SD, median (interquartile range), or n (%).
GA: general anesthesia; Group L: low-age group; Group M: middle-age group; Group H: high-age group; LMA: laryngeal mask airway.
Surgery characteristics
In the context of acetabular or pelvic osteotomy, triple osteotomy and Salter osteotomy were the predominant surgical approaches. With increasing patient age, there was a notable trend toward a higher prevalence of triple osteotomy, whereas the proportion of Salter osteotomy decreased accordingly. Notably, Group L exhibited the highest proportion of Salter osteotomy, whereas Group H had the highest proportion of triple osteotomy (P < 0.05). Furthermore, a substantial proportion of children in Group H underwent Ganz osteotomy, a procedure that was rarely performed in the other two groups (P < 0.05). Pemberton osteotomy, Dega osteotomy, and Chiari osteotomy were performed infrequently, with no significant differences in their utilization among the three groups (P > 0.05).
Although not all children underwent proximal femoral osteotomy, the majority of children in each group did. The proportion in Group H was significantly lower than those in Groups L and M (P < 0.05). More than half of the children in each group underwent adductor-iliopsoas tenotomy, with no significant differences in the proportion among the three groups (P > 0.05).
Compared with Group L, Groups M and H had longer operative durations and higher intraoperative blood transfusion rates, particularly in the use of IOCS (P < 0.05). All groups showed a significant decrease in Hb levels on the first postoperative day compared with preoperative values, with the reduction being more pronounced in Groups M and H than in Group L (P < 0.05) (Table 4).
Surgery characteristics across the three age groups.
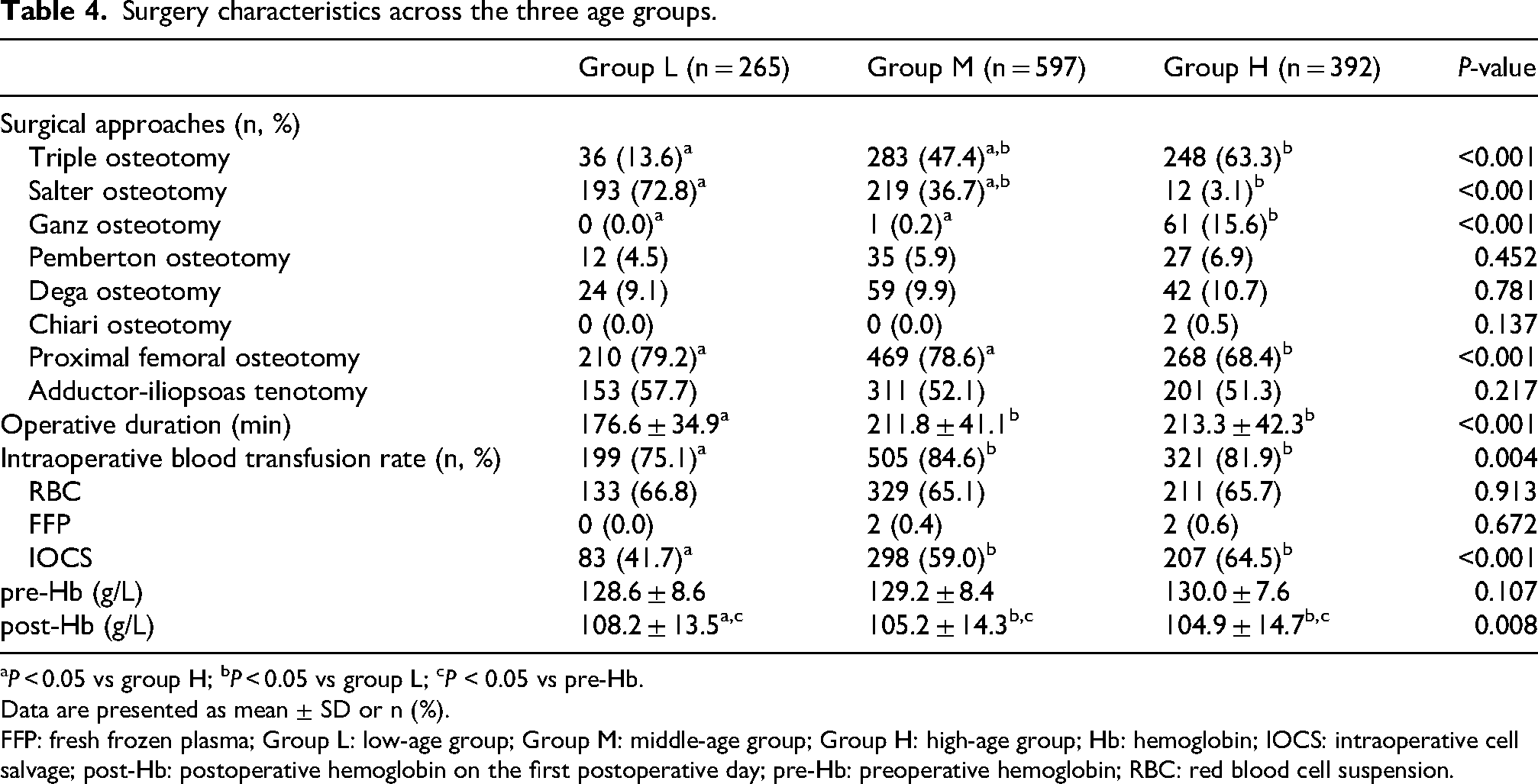
P < 0.05 vs group H; bP < 0.05 vs group L; cP < 0.05 vs pre-Hb.
Data are presented as mean ± SD or n (%).
FFP: fresh frozen plasma; Group L: low-age group; Group M: middle-age group; Group H: high-age group; Hb: hemoglobin; IOCS: intraoperative cell salvage; post-Hb: postoperative hemoglobin on the first postoperative day; pre-Hb: preoperative hemoglobin; RBC: red blood cell suspension.
Discussion
Although GA provides safety and convenience for pediatric surgery, adverse reactions associated with GA are not uncommon, including respiratory depression, delayed recovery, postoperative nausea and vomiting, and constipation. 3 A recent study indicated that sevoflurane may be a triggering factor for postoperative delirium (POD) in children. 9 To minimize postoperative complications, the pediatric ERAS guidelines recommend the use of RA as a complement to GA. 6 Our study demonstrated an RA utilization rate of 64.4%, which substantially exceeds the rates reported in previous European studies. 10 This higher adoption can be attributed to two main factors: our institution's long-standing expertise in RA techniques dating back to the 1980s and the recent integration of ultrasound guidance, which has significantly improved the precision and safety of these procedures in pediatric patients.11,12
Pediatric hip surgery presents unique challenges for RA because of the complex dual innervation of the hip joint by both the lumbar plexus and the sciatic nerve. 4 Our data confirm that multiple RA techniques are currently used in DDH surgery, including CA, FICB, LPB, and QLB. Each of these techniques offers distinct advantages but have specific limitations, requiring careful consideration by anesthesiologists to optimize outcomes. 5
CA remains one of the most frequently used RA techniques for younger children undergoing DDH surgery. Ultrasound guidance has significantly improved the precision of locating the sacral hiatus and advancing the needle within the sacral canal. Although CA can provide reliable anesthesia, its duration of action is typically limited to 4–6 h,13,14 which is insufficient for postoperative analgesia. Our findings suggest that CA may be less suitable for older children, who often require larger volumes of local anesthetics (LA) to achieve adequate blockade. This increases the risk of local anesthetic systemic toxicity (LAST), a serious concern in pediatric anesthesia. 11 In these cases, SA or EA presents a valuable alternative, as demonstrated by our results.
FICB is valued for its technical simplicity and safety profile, as the injection site is distant from major neurovascular structures, thereby minimizing the potential for injury. LA remains in the tissue plane longer, resulting in slower systemic absorption and prolonged analgesic duration.4,15 Studies have shown that FICB in DDH surgery can reduce intraoperative anesthetic requirements and lower Face, Legs, Activity, Cry, and Consolability (FLACC) pain scores for up to 48 h postoperatively. 16 However, even with ultrasound guidance, FICB retains an element of uncertainty. The success of the blockade is largely dependent on the direction and extent of LA diffusion. Increasing the dosage of LA can optimize the blocking effect of FICB by facilitating the cephalad spread of LA toward the fascial plane of the lumbar muscles, lumbar plexus, and even the lumbar paravertebral space. 17 The safe dosage of LA for children should not be overlooked. Evidence supports the use of 0.2% ropivacaine or 0.25% levobupivacaine or bupivacaine at 0.5–1.5 mL/kg as safe and effective for pediatric RA. 11 In our study, FICB use increased significantly with children’s age. This trend reflects both the ability of older children to tolerate larger volumes of LA and anesthesiologists’ preference for techniques that balance efficacy with safety.
Previous research on the use of LPB in adult hip surgery has been quite comprehensive. 4 However, there is a scarcity of reports on its application in pediatric patients, and it remains infrequently used in clinical practice for children. The nerve fibers in children are often too small to be accurately identified on ultrasound images, and the lumbar plexus is closely adjacent to several critical anatomical structures, such as the abdominal aorta and kidney. 18 Consequently, most anesthesiologists consider the risks of LPB in children to outweigh its potential benefits. This cautious approach is also reflected at our center, where LPB is seldom selected as the primary RA technique for DDH surgery.
QLB has emerged as another RA option for hip surgery. Recent studies have shown that QLB provides analgesic efficacy comparable to that of FICB.19,20,21 Further evidence has shown that QLB is not only feasible but also potentially safer for pediatric patients than LPB. 22 Despite these promising findings, QLB has not gained widespread clinical adoption, as reflected in our data. Since 2022, only a limited number of cases at our institution have involved this technique. This restrained uptake may be attributed to its relative novelty and the specialized training required for its consistent use.
Based on etiology and pathogenesis, pediatric DDH is categorized into three types: idiopathic, teratogenic, and neuromuscular. The latter two forms are frequently associated with complex conditions and present distinct therapeutic challenges compared with the idiopathic DDH cases included in our study, 2 which led to their exclusion. Recent reports have revealed that the incidence of DDH in childhood varies among different countries and ethnic groups. Nonetheless, a consistent trend is that female children are more frequently affected. This sex disparity is hypothesized to be associated with the influence of estrogen on fetal development during pregnancy.1,2
DDH progressively compromises hip function from infancy through adulthood, leading to pain, gait impairment, and functional limitations. 1 Early diagnosis and timely intervention are crucial to prevent disease progression. During the initial stages, nonsurgical approaches or minimally invasive procedures are preferred. The Pavlik harness for infants younger than 6 months and hip arthroscopy for children younger than 18 months have demonstrated effectiveness. However, the efficacy of these treatments tends to diminish as children grow older. This is because the lower limbs bear greater weight once children begin standing and walking. The increased weight can cause irreversible changes in the bony structures of the hip and stiffening of the soft tissues around the joint, which are likely the main factors contributing to the failure of reduction. At this stage, typically before the age of 8 years, open reduction becomes necessary; otherwise, DDH may progress to osteonecrosis of the femoral head and hip osteoarthritis, conditions that are difficult to prevent in adulthood.1,23 Studies indicate that the rate of clinical improvement in hip function can exceed 80%–90% when children with DDH undergo surgery before the age of 7 years.23–25 This established treatment paradigm not only informed the age-stratified design of our study but also explains the predominance of middle-age children (Group M) in our cohort, as this period represents the primary window for surgical correction.
Despite the plethora of surgical approaches available in clinical practice, no single method is universally applicable to all cases.2,26 The optimal surgical approach is determined by a comprehensive set of factors. The severity of DDH increases with age.26–28 Consequently, it is reasonable to deduce that the age at which surgery is performed is among the most important factors influencing the choice of surgical approach. In our study, the majority of younger children underwent Salter osteotomy, whereas the proportions of triple osteotomy and Ganz osteotomy increased markedly among older children. We observed a trend toward increasing surgical complexity with age, which was also reflected in operative duration, intraoperative blood transfusion rates, and changes in Hb levels before and after surgery. Our findings suggest that the older the child at the time of surgery, the more severe the hip condition and the more complex the surgical intervention required.
Given the retrospective observational nature of this study, certain limitations inherent to clinical data collection constrained our analysis. Although we identified a correlation between the use of RA and postanesthesia recovery time in pediatric patients, we were unable to determine whether this association was attributable to postoperative pain or other complications. Teratogenic and neuromuscular subtypes of DDH were excluded; although uncommon, their exclusion may modestly limit the external validity of our findings. Similarly, surgeon-specific preferences for operative technique and the anesthesiologist's prior experience with RA were not captured, introducing potential unmeasured confounding. Finally, the modest sample size and single-institution design limit the generalizability of our findings. Multicenter prospective studies with standardized data collection are needed to validate these preliminary observations and to clarify the mechanisms underlying the apparent benefit of RA in pediatric hip surgery.
In summary, RA is extensively utilized in pediatric orthopedic hip surgery. However, the selection of RA techniques is influenced by patient age, reflecting differences in anesthetic and surgical considerations. Younger children are more likely to receive CA, whereas older children are more frequently managed with alternative RA techniques, such as the FICB, LPB, and QLB.
Footnotes
Acknowledgments
The authors acknowledge the contributions of the doctors in the Department of Pediatric Orthopedics, Beijing Jishuitan Hospital, Capital Medical University, Beijing, China. They provided valuable suggestions regarding orthopedic expertise and study design.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Beijing Jishuitan Hospital, Capital Medical University (approval no. K2024–475–00; approval date: 29 October 2024). Informed consent forms were signed by the guardians of the children. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki, as revised in subsequent amendments.
Consent for publication
Written informed consent for publication of the children's clinical details was obtained from their legal guardian. A copy of the consent form is available for review by the Editor of this journal.
Authors’ contributions
Yi Zhang contributed to clinical data collection. Yi Yuan contributed to verifying the data and establishing a database. Ke Sun contributed to designing the study, analyzing the data, and drafting the manuscript. All authors collaborated in analyzing the data and revising the manuscript. All authors have reviewed and endorsed the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are not publicly available because of data sensitivity but are available from the corresponding author upon reasonable request. The data are stored in controlled-access Electronic Medical Record System (EMRS) of Beijing Jishuitan Hospital, Capital Medical University.