
Abstract
Background:
Thoracic paravertebral block is a technique for perioperative analgesia in patients undergoing thoracic, chest wall, or breast surgery, or for pain management with rib fractures, which can be performed with or without ultrasound guidance. The ultrasound guidance technique can be used to identify the thoracic paravertebral space, guide needle placement, monitor the spread of local anesthetic (LA) solution, and reduce complications such as pleural puncture and pneumothorax. The possibility of assessing anesthetic spread in real time using ultrasound guidance during paravertebral block offers numerous advantages, including the immediate and accurate identification of the extent of nervous block, with a consequent reduction of LA dose. The real-time visualization of spread may be used to achieve good anesthetic cover by administering the block at a single level, thus reducing complications normally associated with the technique.
Case summary:
This case report describes the use of ultrasound-guided thoracic paravertebral block, at thoracic (T) 4 and 5 levels, in a patient undergoing breast surgery for perioperative analgesia. The authors were able to witness cranial diffusion of LA at T3-T4 in real time, and measure the increase in space between the costotransverse ligament and pleura, as an indication of anesthetic spread, at T2-T3 and T6-T7 levels.
Conclusions:
This is the first known case in the literature of direct viewing of LA diffusion in a paravertebral space other than the one in which the block is administered and may open important scenarios for the improvement of anesthesia technique.
Introduction
Thoracic paravertebral block (TPVB) is a technique for perioperative analgesia in patients undergoing thoracic, chest wall, or breast surgery or for pain management with rib fractures. The paravertebral space contains thoracic spinal nerves with their branches and the sympathetic trunk: local anesthetic (LA) is administered in this space.1,2 TPVB can be performed with or without ultrasound guidance. The ultrasound guidance technique can be used to identify the thoracic paravertebral space, guide needle placement, monitor the spread of LA solution, 3 and could also reduce complications such as pleural puncture and pneumothorax. 4
With this study, we aim to highlight how ultrasound guidance enables the real-time visualization of LA spread so that TPVB can be carried out at a single level, resulting in a reduction of LA dose, according to diffusion, and a consequent reduction of the potential toxic effects of the anesthetic itself.
Case Description
We describe the use of ultrasound-guided thoracic paravertebral block in one patient undergoing breast surgery for perioperative analgesia. 5 The patient gave her consent for report publication. The patient was a 50-year-old 65-kg 160-cm woman (body mass index 25.39 kg m−2) with American Society of Anesthesiologists physical status II, scheduled for a right modified radical mastectomy for infiltrating ductal carcinoma. No contraindications to the TPVB block were present. The patient received standard heart rate monitoring, noninvasive blood pressure, and oxygen saturation. A single injection into the paravertebral space was administered before general anesthesia, under direct ultrasound guidance, using an ultrasound system (SonoSite M-Turbo; Sonosite Inc., Bothell, WA), with a 50 mm, 5-10 MHz linear ultrasound transducer. The patient was placed in the lateral position with the site of surgical interest uppermost. The transverse process was visualized as a hyperechoic structure, with acoustic shadowing below it. The costotransverse ligament and the pleura were visualized as hyperechoic structures, and the paravertebral space was like a wedge-shaped hypoechoic layer between these structures. The puncture area and the ultrasound probe were prepared in a sterile manner and the puncture was performed with a 22-G × 50-mm needle using the out-of-plane technique. A total volume of 10 mL 0.7% ropivacaine was administered at thoracic (T) level T4-T5. The video and the images (video 1 and Figures 1 to 3) show needle penetration within the paravertebral space, with the diffusion of LA at T4-T5 level and, upon injection of the fourth mL of LA, the start of cranial diffusion to T3-T4 level, resulting in a downward movement of the pleura until the end of LA injection. The distance between the costotransverse ligament and pleura was measured using ultrasound imaging, at T2-T3 and T6-T7 levels, before and after the execution of thoracic paravertebral block at T4-T5 level. An increase in distance between costotransverse ligament and pleura at T2-T3 and T6-T7 levels was observed after block administration, indicating the caudal spread of LA. Forty minutes after the administration of TPVB, sensory blockage was assessed by cold sensation to an alcohol-soaked sponge and by pinprick testing with a 22-G short bevel needle. The blocked area was tested from the T4 dermatome at the anterior axillary line in a cranial and caudal direction, and each dermatome on the blocked side was compared to the contralateral one. The test confirmed cranial diffusion of LA up to T2 level and caudal diffusion up to T7 level. Anesthesia was induced by means of intravenous (IV) propofol 2 mg kg−1; an I-Gel size 3 was inserted according to manufacturer’s instruction. Anesthesia was maintained by continuous IV propofol infusion (6-9 mg kg−1h−1). The sedation level was monitored using Bispectral Index System. Fentanyl 2 μg kg−1 in bolus doses was administered intravenously if mean blood pressure or heart rate exceeded 20% of the preoperative value. Surgery was completed in 80 minutes, no fentanyl bolus was required, and there was no reduction in patient heart rate or blood pressure associated with sympathetic blockade. Acetaminophen 1 g IV was administered 30 minutes before the end of surgery and then every 8 hours. The patient was monitored for pain intensity using the numeric rating scale (NRS) at time 0 and 6, 12, and 24 hours after surgery. Pain never exceeded 3 on the NRS pain score. No postoperative nausea and vomiting or symptoms or signs of LA toxicity were reported.
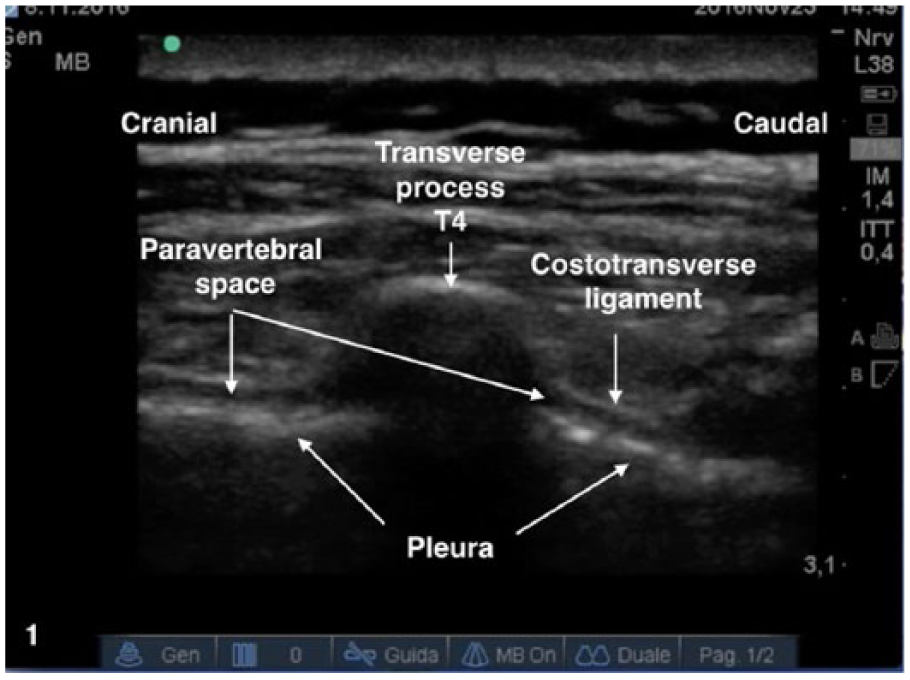
Thoracic paravertebral space.
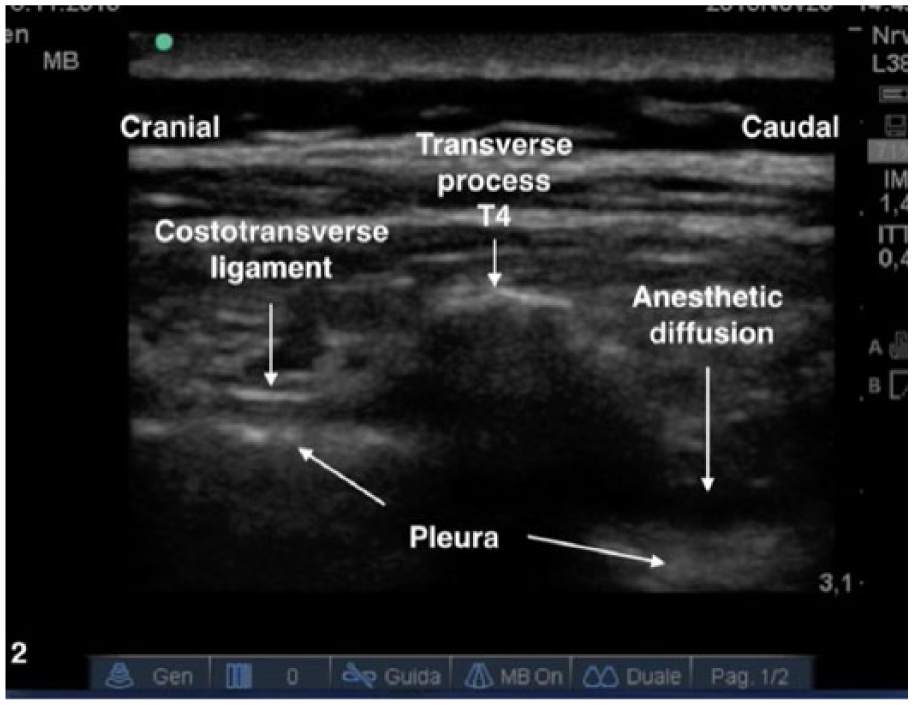
Injection of local anesthetic.
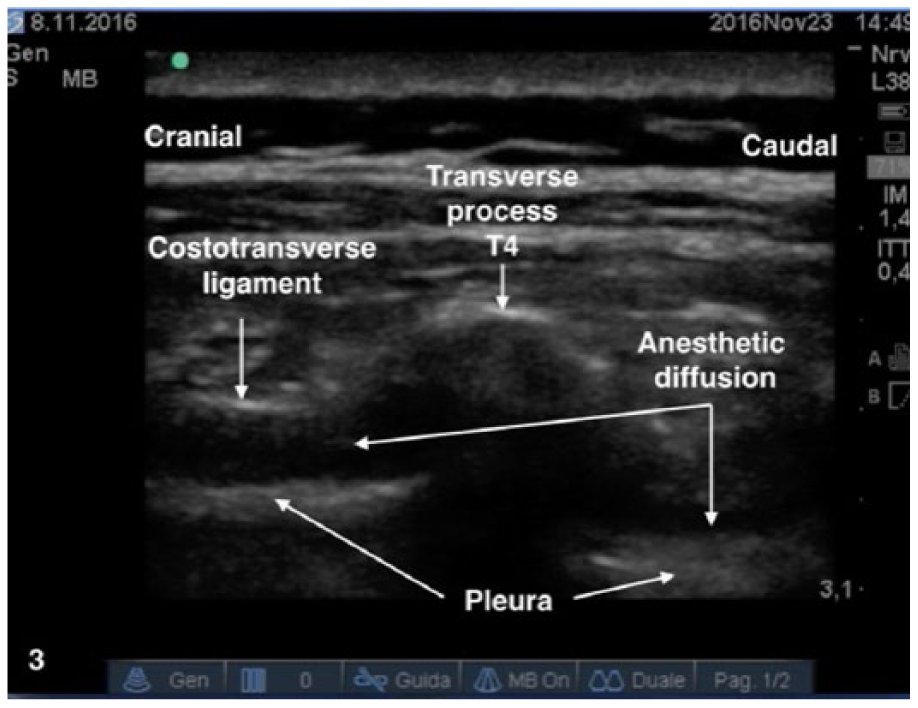
Cranial spread.
Conclusions
Some studies have investigated LA longitudinal spread into the thoracic paravertebral space through the assessment of methylene blue diffusion, checked by means of the insertion of a thoracoscopy camera into the chest, magnetic resonance imaging, or cadaveric study.6-8 These authors evaluated LA spread after block administration, but not at the same time. In the case we describe, the use of an ultrasound guide to carry out the block enabled us to witness cranial diffusion of LA at T3-T4 in real time and to measure the increase in space between the costotransverse ligament and pleura, as an indication of anesthetic spread, also caudally, at T5-T6 and T6-T7 levels. The possibility of assessing anesthetic spread in real time using ultrasound guidance during paravertebral block offers numerous advantages, such as the immediate and accurate identification of the extent of nervous block, with a consequent reduction of LA dose, according to diffusion, and a reduction of the potential toxic effects of the anesthetic itself. The real-time visualization of spread could be used to achieve good anesthetic cover by administering the block at a single level, thus perhaps reducing complications of the technique, such as vascular puncture, pleural puncture, and pneumothorax. 4
Longitudinal spread is an established fact, as demonstrated by copious literature. We have further confirmed this by using ultrasound guidance to cranially and caudally measure the increase in the space between the costotransverse ligament and pleura for block administration.
It is also important to highlight that it was not always possible to view the cranial diffusion of LA so clearly.
In conclusion, this is the first case in the literature known to us of direct viewing of LA diffusion in a paravertebral space other than the one in which the block is administered. If confirmed by further studies involving broader patient cohorts, the possibility of assessing LA diffusion when carrying out a paravertebral block immediately and in real time may open up important scenarios for the improvement of anesthesia technique.
Footnotes
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.