
Abstract
Background:
Radium-223 (223Ra) chloride, an alpha emitter, has been shown to improve overall survival (OS) and pain control, and to delay skeletal-related events, in patients with castration-resistant prostate cancer (CRPC) and bone metastases. Our retrospective observational study presents the first Italian experience on the efficacy and safety of 223Ra therapy in routine clinical practice.
Methods:
A total of 83 patients with metastatic CRPC were treated with 223Ra at 3 Italian centers between August 2013 and August 2016. 223Ra-chloride (55 kBq/kg) was administered every 4 weeks for a total of 6 cycles. Primary endpoints were OS and progression-free survival (PFS). Secondary endpoints included toxicity, pain evaluation using numeric rating scale (NRS), symptomatic skeletal-related events and biomarkers response.
Results:
Patients had a median age of 75 (range 53–89) years. The majority of men showed a Gleason score of 7, 8, or 9. Forty-one patients completed 6 treatment cycles; 33 stopped treatment before completing 6 cycles. Nine were still receiving therapy at the time of data collection. At the end of therapy, NRS pain scores significantly improved (p < .000001). OS was a mean of 10.1 months, while median OS had not been attained. According to Kaplan-Meier estimation, OS and PFS were 17.5 and 7.7 months, respectively. There was a significant correlation between OS and PFS with the number of 223Ra cycles; patients receiving all 6 cycles experienced the major benefit from the therapy. 223Ra was well-tolerated.
Conclusions:
223Ra alpha therapy is an important therapeutic option for men with CRPC and symptomatic skeletal metastases.
Introduction
Prostate cancer is the most common male cancer worldwide, and a leading cause of cancer-related morbidity and death. 1 Castration-resistant prostate cancer (CRPC) develops in 10%–20% of patients and has a poor prognosis, with a median survival duration of approximately 2 years.2,3 More than 90% of men with CRPC present with bone metastases, which are a key cause of decreased quality of life, morbidity, mortality, and treatment costs. 4
Several new therapeutic agents aimed at improving survival and quality of life (QoL) in metastatic CRPC (mCRPC) have been developed and clinically tested in recent years. In this context, radium-223 (223Ra) chloride is the first radiopharmaceutical approved for treatment of skeletal mCRPC that has been shown to improve overall survival (OS) and delay skeletal-related events, in addition to providing better pain control.5, 6 223Ra is an alpha-emitting radiopharmaceutical agent with a half-life of 11.4 days that selectively binds to areas of increased bone turnover, producing nonrepairable double-stranded DNA breaks and cytotoxic activity.7,8 223Ra is associated with a relatively good hematologic toxicity profile because of the shorter range of alpha particles (100 μm) in comparison with beta particles of previous radioisotopes used only in bone palliation.9,10
The survival benefit and safety profile of 223Ra were documented in the ALSYMPCA trial, a randomized, double-blind, placebo-controlled, multinational phase III study that compared 223Ra plus best standard of care with placebo plus best standard of care in a total of 921 patients with symptomatic bone metastases of CRPC. There was a 30% reduction in the risk of death and a longer median time to first symptomatic skeletal-related event with 223Ra treatment versus placebo. 6 These results led to increased clinical use of 223Ra-chloride in skeletal mCRPC. 11
Although the efficacy and safety of 223Ra-chloride have been assessed in study protocols, they have not been completely established in routine clinical practice. Furthermore, candidate patients for this therapy in the daily practice setting may differ from those enrolled in clinical trials due to less restrictive case selection in clinical practice, greater heterogeneity in previous treatments and diagnostic assessment, and varied presentation of clinical features among uro-oncologic centers. Also, routine practice may differ between centers, both in terms of patient enrollment modalities and response assessment during and after 223Ra-chloride administration.
In the ALSYMPCA trial, radiologic evaluation of response was not scheduled; the primary study endpoint was OS, with secondary efficacy endpoints based on clinically evaluated symptomatic skeletal events (SSEs; ie, spinal cord compression, external beam radiation therapy to alleviate bone symptoms, new symptomatic pathologic skeletal fractures, and tumor-related orthopedic surgery) and pain score evaluation, progression-free survival (PFS), time to first skeletal event, and biochemical evaluation. In clinical practice, we routinely use these endpoints rather than imaging evaluation, but without a precise timing schedule and standardization. Therefore, this Italian, multicenter, retrospective, observational analysis reports our experience with 223Ra-chloride therapy in daily medical practice.
Methods
Data from patients with mCRPC who underwent 223Ra-chloride treatment over the period from August 2013 to August 2016 at 3 Italian centers (Sant’Orsola-Malpighi University Hospital in Bologna, University Hospital in Pisa, and the Cancer Centre in Aviano) were collected retrospectively. This study met national and international regulatory guidelines (Declaration of Helsinki, European Medical Association) for clinical trial research and was approved by the local ethics committees. Informed consent was obtained from all individual participants included in the study.
Eligible patients had a histologic diagnosis of prostate cancer, surgically resected or radiotreated, which had become castration-resistant according to Prostate Cancer Working Group (PCWG2) criteria, 12 and were candidates for 223Ra-chloride treatment. Irrespective of prior chemotherapeutic treatment with a taxane-based regimen, all included patients had been treated with 223Ra-chloride alone without any concomitant pharmacologic treatment, apart from zoledronic acid, denosumab, or local radiotherapy (but not coincident with a SSE as previously defined). Exclusion criteria were hormonal-sensitive disease, visceral metastases or lymph-nodal metastases larger than 3 cm, asymptomatic skeletal disease, or previous treatment with 223Ra-chloride.
Data were collected from all 3 centers using a standardized case report form (CRF) that included patient age, weight and height, comorbidities, and concomitant therapies, cancer history, and lines of therapy before 223Ra. CRF data were entered into a unique database for aggregation and analysis.
223Ra-chloride (55 kBq/kg) was administered every 4 weeks for up to 6 cycles of therapy, as per recommendations. The primary endpoint was OS. Secondary endpoints included PFS, evaluation of pain score using a numeric rating scale (NRS), hematologic parameters, number of SSEs, response evaluation based on biomarkers (prostate serum antigen [PSA] and alkaline phosphatase [ALP]), and imaging assessment. Specifically, the following data were collected: concomitant bone target therapy, diagnostic imaging for response evaluation, therapeutic cycle, NRS score, 13 analgesic treatment, PSA level, ALP level (patients were divided into 2 groups: <220 vs ≥220 U/L), lactate dehydrogenase (LDH) level, calcium level, hemoglobin (Hb) concentration, platelet count, white blood cell (WBC) count, neutrophil count, hematologic and gastrointestinal toxicity, transfusions during treatment, and SSEs. The following parameters were assessed 2 months after the end of treatment: NRS pain score, diagnostic imaging, biochemical markers, time to first disease progression, site of progressive disease during or after treatment, and time and type of skeletal event.
Statistical analysis
Patient characteristics and clinical measures of interest were described using descriptive statistics. Data were analyzed on an intention-to-treat basis. Associations between 223Ra cycles and all available variables for each cycle were evaluated using one-way analysis of variance (ANOVA) and its nonparametric equivalent, the Kruskal-Wallis test. Variables included scintigraphy levels, NRS scores, PSA, ALP, LDH, calcium, Hb, platelet, WBC, and neutrophil levels. OS and PFS times were calculated using the Kaplan-Meier estimation. Associations between OS, PFS, and clinical measures of interest were evaluated by univariate and multivariable Cox proportional hazards regression models, including hazard ratio (HR), R2, and p value. Variables were included in the Cox models as time-dependent covariates. The PSA doubling time (PSADT) was computed in 2 ways: (1) for each consecutive PSA value and (2) for the first and last PSA values. The following formula was used to compute PSADT 14 :
All statistical analyses were performed using R, the R Project for Statistical Computing software package, version 3.3.0, with a significance level of 5%.
Results
A total of 83 patients with mCRPC were treated with 223Ra in 3 Italian radiotherapy/nuclear medicine departments (Table 1). Median age was 75 years (range 53–89 years). Mean follow-up was 176±195 days (range 0–928 days). The majority of patients had received previous lines of therapy for CRPC; only 24 were chemotherapy-naive. The median number of previous lines of treatment was 2 (range 0–5). Regarding analgesic requirements, 36 patients used opioids; 36 had mild pain treated chronically or occasionally with nonopioid painkillers (data were not available for 11 patients). Fifteen patients received other allowed pharmacologic treatment, such as zoledronic acid or denosumab. The majority of patients had a Gleason score of 7 (n = 25), 8 (n = 16), or 9 (n = 21). Eighty-three patients completed a total of 386 cycles of treatment with 223Ra.
Clinical characteristics of the 83 patients who underwent 223Ra therapy.
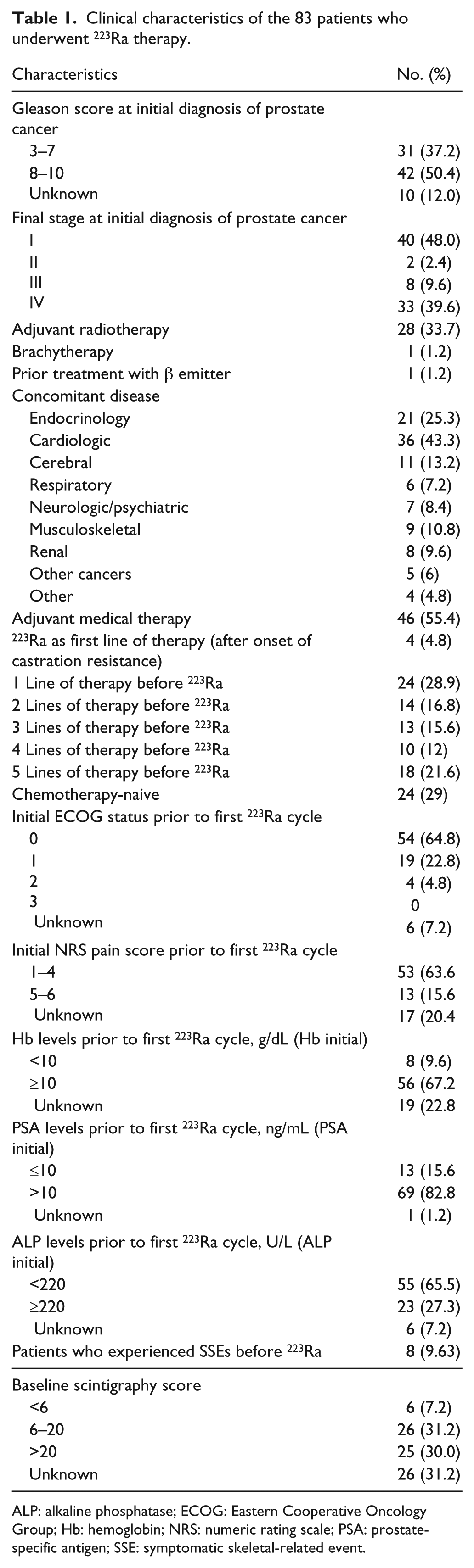
ALP: alkaline phosphatase; ECOG: Eastern Cooperative Oncology Group; Hb: hemoglobin; NRS: numeric rating scale; PSA: prostate-specific antigen; SSE: symptomatic skeletal-related event.
Nine of 83 patients were under treatment at the time of data collection. Thirty-three patients stopped treatment: 12 due to toxicity, 10 due to disease progression, and 11 for other reasons (eg, clinical deterioration, withdrawal of consent). Seven patients stopped treatment after 1 cycle, 5 after 2 cycles, 7 after 3 cycles, 5 after 4 cycles, and 9 after 5 cycles. Forty-one patients completed the recommended 6 cycles. No patient experienced a SSE during treatment. After treatment, 9 patients had a SSE. The mean time to a SSE was 247.6 days (median 240.5 days).
Pain
Thirty-seven patients had a reduction in bone pain, 15 had worsening pain due to disease progression or a decline in physical condition, and 41 remained stable (threshold 10%).15,16 During 6 cycles of treatment, there was a significant improvement in NRS pain scores (Kruskal test; p < .000001) (Figure 1a). At 1st cycle, the mean value of NRS pain score was 3.061 (median 2.0), while at the 6th cycle the mean was 1.361 (median 0.5); a significant difference between NRS pain score value at 1st versus 6th cycle of p < .002 (Mann-Whitney test) was noted.
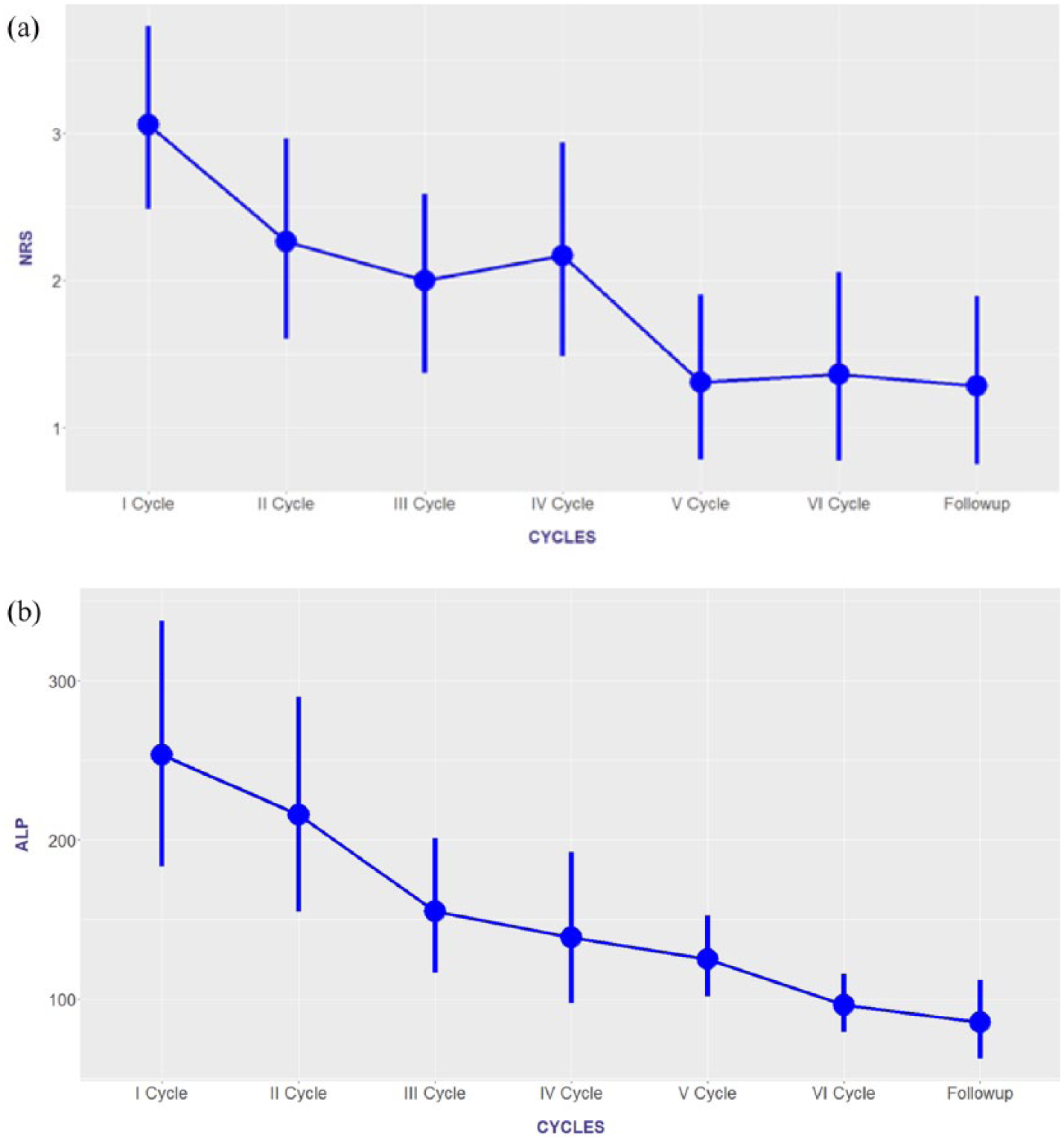
Change in numeric rating scale (NRS) pain scores (a) and alkaline phosphatase (ALP) levels (U/L) (b) during treatment with 223Ra-chloride. Median values with 95% confidence intervals.
Tolerability
Nonhematologic toxicities were asthenia (7 events), nausea (5 events), anorexia (3 events), and diarrhea (3 events); of these, all anorexia and 1 diarrhea event were of grade 3 severity. The most common hematologic toxicity was anemia (149 events; 8 grade 3). All other hematologic events were grade 2 in severity (4 thrombocytopenia, 13 leukopenia, and 3 neutropenia). Patients with grade 2/3 anemia were treated with blood transfusions. Bone marrow failure (defined as development of World Health Organization grade 3 or 4 hematologic toxicity with no recovery after 6 weeks, or death due to bone marrow failure after the last 223Ra dose) occurred in 2 patients. No significant correlations were found between toxicity and number of cycles, toxicity and patients’ age, and toxicity and burden of bone disease.
Biomarkers
PSA levels were reduced in 13% of patients and increased in 87%. In general, there was a trend towards increasing PSA during treatment, probably due to flare phenomena, as reported in the literature17,18; median 77 ng/mL in cycle 1 versus 126 ng/mL in cycle 3.
The median decline from baseline in ALP was 29%, and 59 patients experienced an ALP decline >10%. ALP levels varied significantly across the 6 cycles (Kruskal test; p < .00004) (Figure 1b). However, there was no significant correlation between ALP levels and OS or PFS.
Ten patients had a ≥10% decrease in LDH, while the median LDH trend was not significantly different from the baseline median value.
Survival
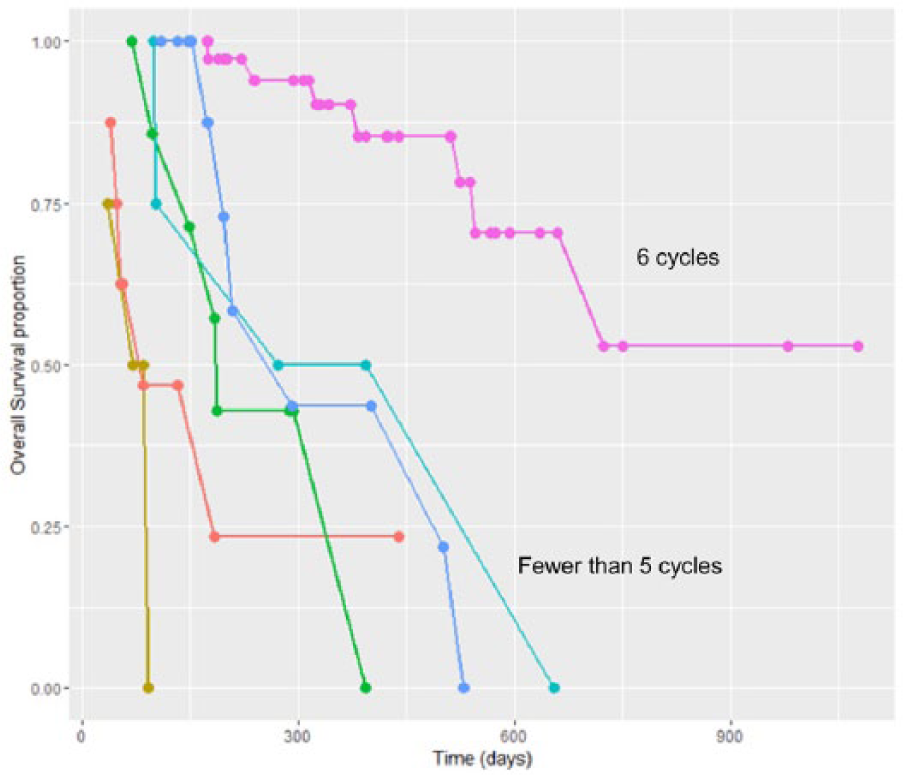
The mean OS was 10.1 months, while the median had not yet been attained at the time of reporting (49 alive, 29 dead, 5 data not available). The Kaplan-Meier estimate for the survival curve showed a median OS of 17.5 months (Figure 2a). OS was significantly associated with the number of 223Ra cycles in a Cox proportional hazards regression model (p < .00002; HR 0.71, 95% confidence interval [CI] 0.61–0.82; Table 2). On univariate analysis, OS was also significantly associated with the number of 223Ra cycles, Gleason score, and baseline levels of Hb, LDH, and ALP (Table 2). On multivariate analysis, only the number of 223Ra cycles and baseline ALP level remained as statistically significant predictors of OS (Figure 3).
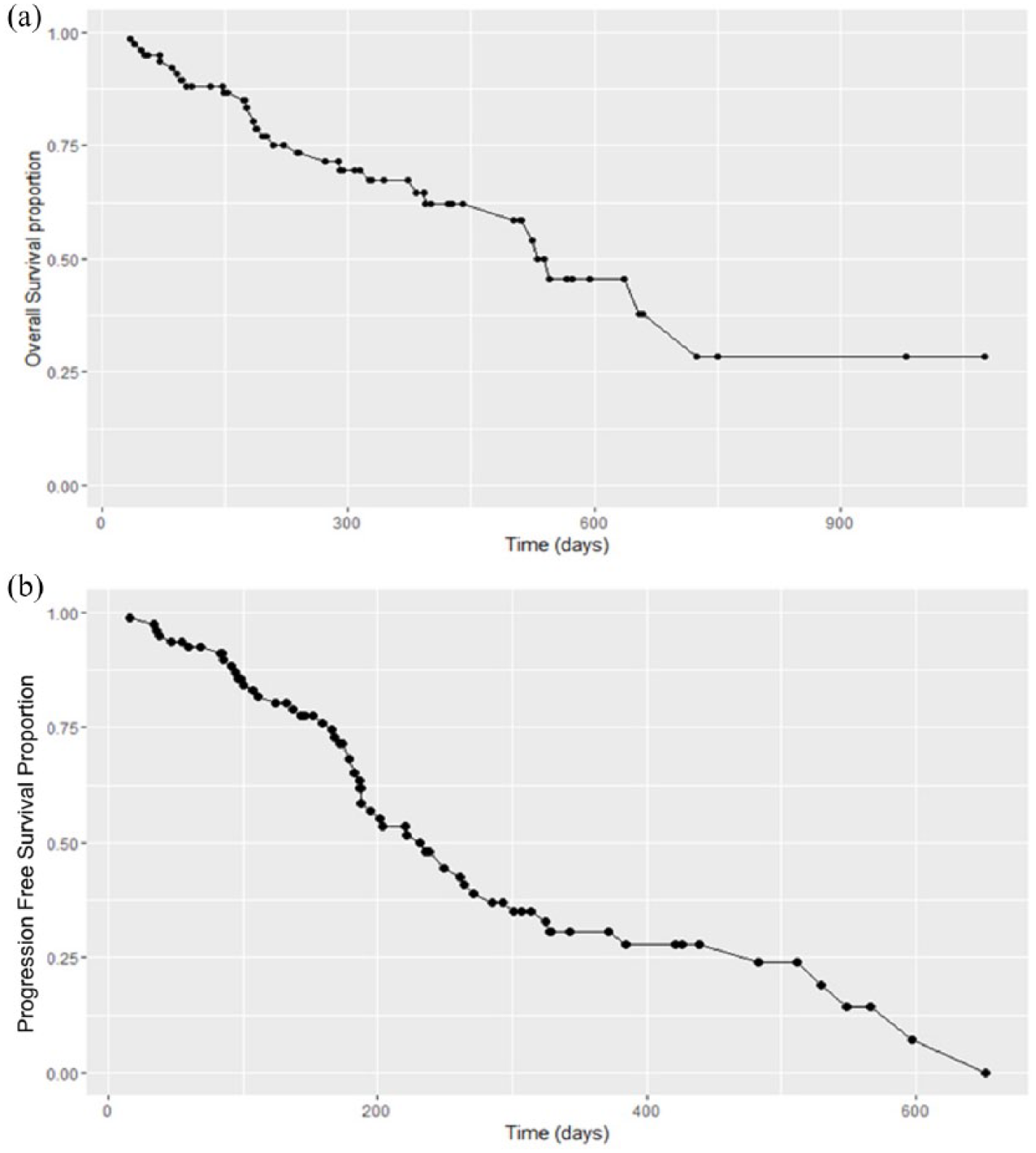
Kaplan-Meier survival estimates for overall survival (a) and progression-free survival (b).
Univariate and multivariate models of overall survival and progression-free survival in relation to clinical and laboratory parameters.
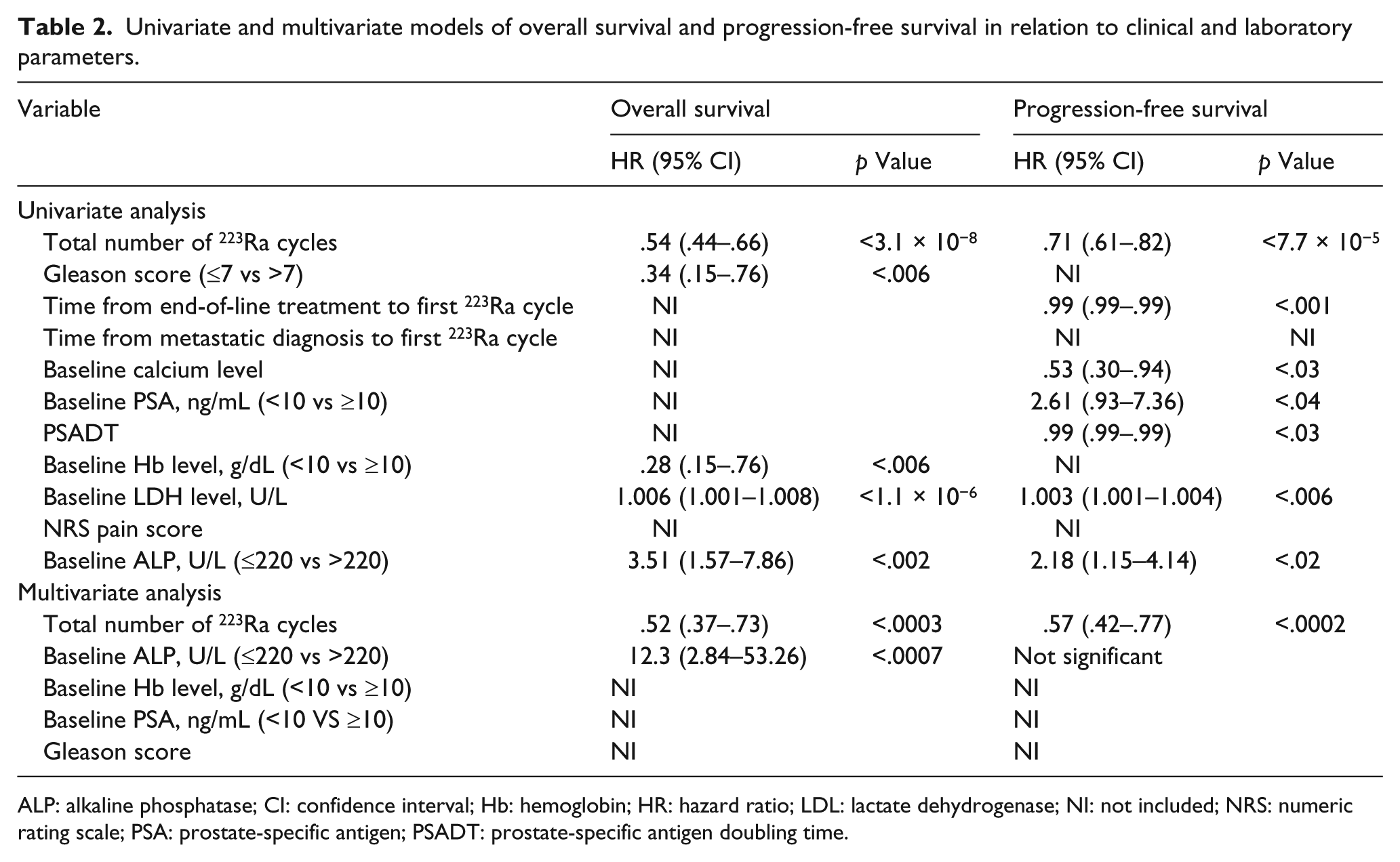
ALP: alkaline phosphatase; CI: confidence interval; Hb: hemoglobin; HR: hazard ratio; LDL: lactate dehydrogenase; NI: not included; NRS: numeric rating scale; PSA: prostate-specific antigen; PSADT: prostate-specific antigen doubling time.
Cox proportional hazards regression estimate of overall survival (OS).
Median PFS was 6.2 (range 16–652) months (50 progression or death, 29 with no progression, 4 data not available). The Kaplan-Meier estimate for the PFS curve had a median of 7.7 months (Figure 2b). Univariate Cox proportional hazards regression model analysis showed that PFS was significantly associated with time from end-of-line treatments to the first 223Ra cycle (p < .002; HR 0.99, 95% CI 0.99–0.99) and the number of 223Ra cycles (p < .00002; HR 0.71, 95% CI 0.61–0.82) (Table 2). On univariate analysis, PFS was also significantly associated with the total number of 223Ra cycles, Gleason score, time from end-of-line treatment to first 223Ra cycle, baseline calcium level, PSA levels, PSADT, ALP levels, and LDH levels. However, on multivariate analysis, the only significant factor remaining was the number of 223Ra cycles.
Patients with ALP ≥220 U/L had significantly worse prognosis in terms of both OS and PFS compared to those with ALP <220 U/L (OS 655 vs 208 days, respectively, p = .00116; and PFS 264 vs 169 days, respectively, p = .0139) (Figure 4 [a] and [b]).
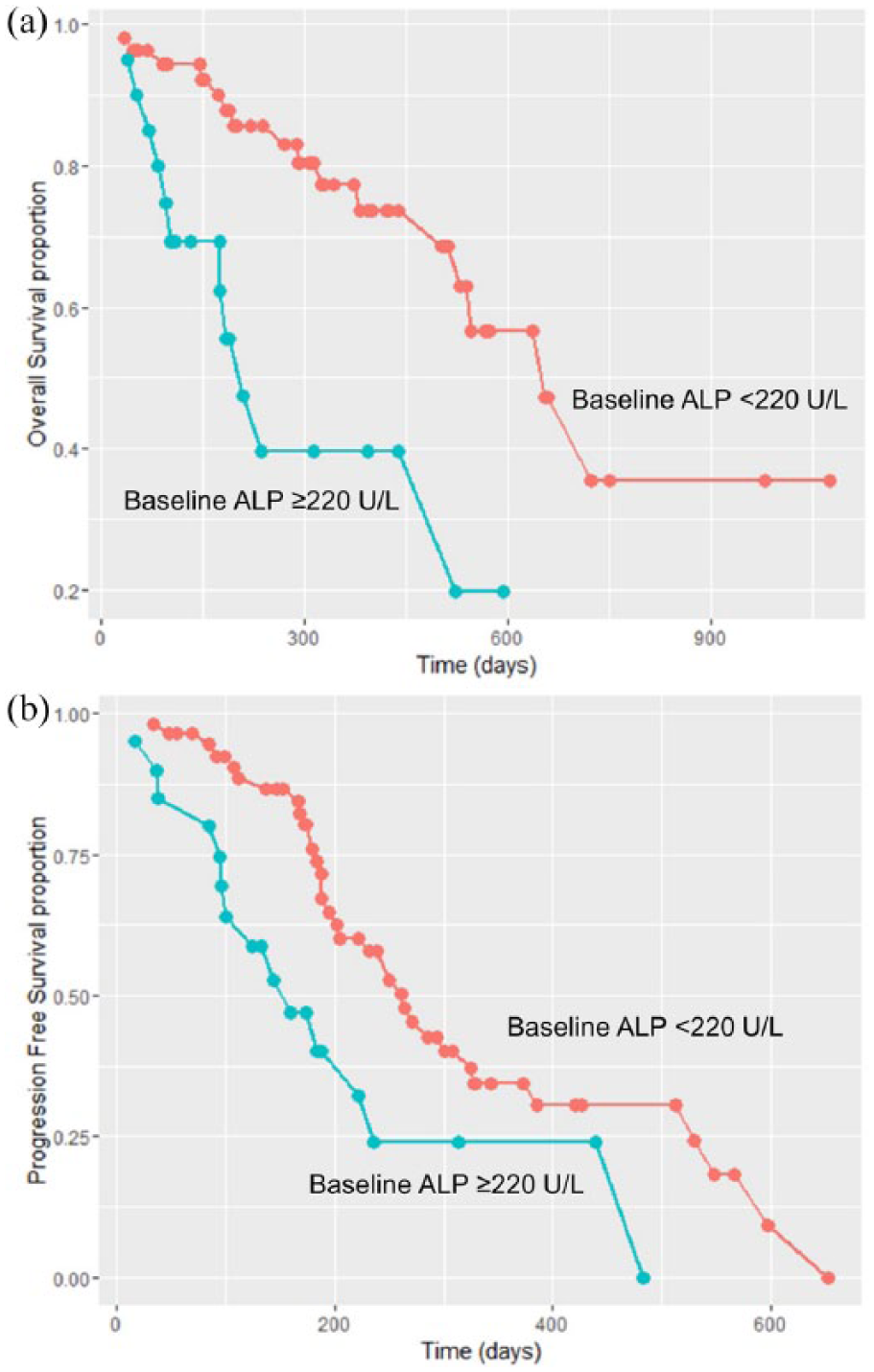
Kaplan-Meier survival estimates for overall survival (a) and progression-free survival (b) in patients stratified according to baseline alkaline phosphatase (ALP) level (<220 U/L, ≥220 U/L).
Discussion
Data from this retrospective analysis show that patients diagnosed with mCRPC and symptomatic bone metastases treated with 223Ra had a slightly longer median OS than in the ALSYMPCA study 6 (by 2.6 months, median OS of 17.5 vs 14.9 months, respectively). The reason for this difference is not immediately clear, but could be related to differences in baseline characteristics between the 2 populations. For instance, some of our patients may have had a lower burden of disease when they started the treatment, resulting in a longer life expectancy at baseline compared with ALSYMPCA patients. Our results showed that patients with lower ALP levels (<220 vs ≥220 U/L) had better OS and PFS. That suggests that starting 223Ra therapy as early as possible, based on ALP levels, could improve patient outcomes.
Multivariate analysis demonstrated that OS significantly increased with the number of 223Ra cycles received. This confirms data from the literature reporting a higher OS in patients undergoing a complete course of therapy. 19 Analyzing pain reduction and NRS score, our data confirm the ability of 223Ra to reduce bone pain, cycle after cycle of 223Ra. OS was also associated with NRS score throughout the 6 cycles, suggesting that patients with a low baseline pain intensity (lower NRS score) show a better improvement in OS after completing 6 cycles of 223Ra therapy. This is consistent with a previous analysis of 696 patients enrolled in an international expanded access program. 20 In that study, median OS was not reached in patients with no reported pain at baseline, compared with an OS of 14 months for those with mild pain and 11 months for those with moderate to severe pain. In addition, median OS was longer for patients with baseline ALP concentrations less than the upper limit of normal, in those with baseline Hb ≥10 g/dL, and for patients with a baseline Eastern Cooperative Oncology Group (ECOG) performance status of 0 versus those with a poorer performance status. 20
Similarly, our study suggests that patients in the best clinical condition (high Hb or low LDH and ALP) seem to achieve a better result at the end of 223Ra therapy, in terms of OS and PFS, in the univariate analysis. Completion of the full 6 cycles of 223Ra was also associated with a significantly better PFS.
The safety profile of 223Ra therapy in our analysis of real-world use was favorable in terms of both hematologic and nonhematologic toxicities. Diarrhea was a rare adverse event, and no serious adverse events occurred during the treatment period.
To ensure proper resource management and to maximize the effectiveness of therapy, it is important to properly select patients to undergo 223Ra treatment. Appropriately selected patients also have the best chance of completing the full treatment course, thus maximizing the effectiveness of 223Ra. Clinicians play an important role in the early identification of patients with castration-resistant disease, and in the evaluation of all approved therapies, including alpha emitters such as 223Ra, which probably should be used early after a diagnosis of castration resistance in cases with symptomatic bone metastases.
Currently, there is a lack of scientific studies concerning the role of imaging in the evaluation of response to treatment. Possible diagnostic options are bone scan, choline single photon emission tomography/computed tomography (PET/CT), or 18 F-fluorodeoxyglucose PET/CT.21,22 In our study, imaging data from bone scans before and after therapy were used to monitor response in patients treated with 223Ra. However, no statistically significant differences were found in scans before and after therapy in terms of numbers of lesions.
Regarding blood markers, we observed a significant reduction of ALP levels in this study. ALP is a key marker of bone turnover associated with bone metastases and useful for evaluating the clinical course during therapy. However, we found no significant correlation between ALP levels and OS or PFS. Further research is needed to explore the role of ALP as a biomarker in 223Ra therapy. No other markers, such as baseline calcium level, PSA levels, PSADT, ALP levels, and LDH levels, were significant predictors of response to treatment in our study; the only significant factor on multivariate analysis was the number of 223Ra cycles. In most patients (87%), PSA values increased from baseline value during 223Ra therapy. There were no significant correlations between PSA levels and OS, and therefore this does not appear to be a useful parameter in guiding patient management during 223Ra therapy or as a predictor of outcome. SSEs were rare events in our study, experienced by only 9 patients after therapy (10.8%), consistent with other reports in the literature. 23
In our study, 223Ra therapy was manageable and easy to administer. It was well-tolerated with a low toxicity profile. The main side effects were hematologic, particularly anemia and thrombocytopenia. Patients with anemia were treated using iron therapy or blood transfusions. These treatments provided effective management, thus side effects did not compromise therapeutic process, as reported in the literature. 24
However, results from the ongoing randomized trials are essential before positioning 223Ra in different therapeutic strategies or settings.
Conclusion
223Ra is an important treatment option for patients with CRPC and symptomatic bone metastases, since it is proven to prolong OS and delay the time to the first skeletal event, in the face of an acceptable hematologic and nonhematologic toxicity.23,24 Full 6-cycle 223Ra therapy should be completed to obtain the maximum survival benefit. 223Ra therapy is also associated with a beneficial effect on pain. The safety profile is favorable, with a low incidence of myelosuppression, which is managed effectively without compromising the therapeutic process.
Regarding the selection of patients, available data support the use of 223Ra in patients with CRPC and symptomatic bone metastases without visceral disease, both before and after chemotherapy.23,24
Currently, there is no consensus about the optimal sequence position for 223Ra. However, despite this, there is agreement that early 223Ra therapy in patients with predominant bone disease (without visceral metastases), progressing on first-line treatment (new hormone treatment), may be considered. Nevertheless, similarly, administration of 223Ra in later lines of therapy may be an appropriate and advantageous option for some patients (before the onset of visceral metastases), unfitted to chemotherapy or hormone therapy, after a careful evaluation of clinical and hematologic conditions. Additional randomized trials are needed to establish the optimal sequences and combination strategies for the use of 223Ra in patients with mCRPC.
Footnotes
Acknowledgements
We thank Ray Hill, an independent medical writer, who provided English-language editing and journal styling prior to submission on behalf of Health Publishing & Services Srl.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
Giuseppe Boni, Sara Mazzarri, Claudia Cianci, Luca Galli, Azzurra Farnesi, Eugenio Borsatti, Roberto Bortolus, Lucia Fratino, Carlo Gobitti, Elda Lamaj, Pietro Ghedini, Elisa Lodi Rizzini, Francesco Massari, Valeria Dionisi, Stefano Fanti, Duccio Volterrani, and Fabio Monari: conception/design. Giuseppe Boni, Sara Mazzarri, Claudia Cianci, Luca Galli, Azzurra Farnesi, Eugenio Borsatti, Roberto Bortolus, Lucia Fratino, Carlo Gobitti, Elda Lamaj, Pietro Ghedini, Elisa Lodi Rizzini, Francesco Massari, Valeria Dionisi, Stefano Fanti, Duccio Volterrani and Fabio Monari: provision of study material or patients. Giuseppe Boni, Sara Mazzarri, Claudia Cianci, Luca Galli, Azzurra Farnesi, Eugenio Borsatti, Roberto Bortolus, Lucia Fratino, Carlo Gobitti, Elda Lamaj, Pietro Ghedini, Elisa Lodi Rizzini, Francesco Massari, Valeria Dionisi, Stefano Fanti, Duccio Volterrani and Fabio Monari: collection and/or assembly of data. Giuseppe Boni, Sara Mazzarri, Claudia Cianci, Luca Galli, Azzurra Farnesi, Eugenio Borsatti, Roberto Bortolus, Lucia Fratino, Carlo Gobitti, Elda Lamaj, Pietro Ghedini, Elisa Lodi Rizzini, Francesco Massari, Valeria Dionisi, Stefano Fanti, Duccio Volterrani and Fabio Monari: data analysis and interpretation.
Giuseppe Boni, Eugenio Borsatti, Roberto Bortolus, Lucia Fratino, Carlo Gobitti and Elda Lamaj: manuscript writing. Giuseppe Boni, Sara Mazzarri, Claudia Cianci, Luca Galli, Azzurra Farnesi, Eugenio Borsatti, Roberto Bortolus, Lucia Fratino, Carlo Gobitti, Elda Lamaj, Pietro Ghedini, Elisa Lodi Rizzini, Francesco Massari, Valeria Dionisi, Stefano Fanti, Duccio Volterrani and Fabio Monari: final approval of manuscript.