
Abstract
Purpose:
To report long-term effects on anorectal function and bowel disorders and late toxicity rate of preoperative chemoradiotherapy in patients with locally advanced rectal cancer.
Methods:
Between 2000 and 2016, 201 patients treated with different neoadjuvant schedules of chemotherapy and radiotherapy doses were retrospectively analyzed. The Memorial Sloan–Kettering Cancer Center score was used for the evaluation of anal sphincter function.
Results:
The median follow-up time was 68 months (interquartile range 35–113 months). Radical resection was performed in 188 (93.5%) patients with a pathologic complete response rate of 26.4%. Overall sphincter function resulted excellent in 105 (52.2%) patients, good in 13 (6.5%), fair in 10 (5.0%), and poor (incontinence) in 40 (19.9%), with a persistent stoma rate of 16.4%. A further evaluation on 194 patients showed an improvement of sphincter function after 2 years in 11.9% of them. Seventy-three patients presenting stoma or poor sphincter function were re-evaluated for quality of life (QoL) indexes. Twenty-one (29%), 19 (26%), and 24 (33%) of them declared some variations concerning well-being, fatigue, and ability to perform daily activities. The 5-year overall survival, disease-free survival, and local recurrence rates were 88.0% ± 2.6%, 86.3% ± 2.5%, and 94.6% ± 1.9%, respectively.
Conclusions:
In our study, neoadjuvant chemoradiotherapy was associated with good results in terms of sphincter function, late toxicities, and QoL indexes. A routine use of assessment scales could contribute to a better selection of patients with increased risk of developing functional disorders who could benefit from neoadjuvant therapy.
Introduction
Currently, multimodality treatment for locally advanced rectal cancer patients, such as neoadjuvant long-course chemoradiotherapy (CRT) or short-course radiotherapy (RT) followed by total mesorectal excision (TME), has become the standard of care. This approach results in an improvement of oncologic outcomes, including local control and long-term survival, but also in an increased number of low anterior resection (LAR) with sphincter preservation surgery, due to tumor size reduction and downstaging.1–3
On the other hand, complications related to both surgery and RT, mostly represented by bowel dysfunction, fecal urgency and/or incontinence, and urinary and sexual disorders,4,5 could adversely affect social relationships and quality of life (QoL), and need to be taken into account, especially in long-term surviving patients, as evaluated in some studies.6,7 Health-related QoL is an important issue when evaluating the efficacy of treatment.
The aim of this study was to evaluate long-term effects of preoperative long-course CRT on anorectal function and late toxicity in patients with locally advanced rectal cancer treated in our institution.
Methods
From 2000 to 2016, 289 patients with locally advanced rectal cancer were treated with preoperative CRT at our RT department. Patients who underwent abdominoperineal resection were excluded from the analysis. A total of 201 patients were then retrospectively analyzed for bowel and sphincter function. Their clinical and pathologic data were collected.
RT was always performed by 3D conformal technique, with a total dose of 4500 cGy, 180 cGy/d, on the pelvic nodes, followed by a sequential boost of 540 cGy (180 cGy/d; total dose 5040 cGy) or a concomitant boost of 1000 cGy (100 cGy/d, 2 times/wk; total dose 5500 cGy).
Three-field (postero-anterior and lateral fields) and 4-field (postero-anterior and lateral fields) techniques were performed, following standard techniques. During the simulation process, patients were immobilized in prone position on a belly board, a device aimed at reducing small bowel irradiation. The clinical target volume (CTV) included the primary tumor as well as mesorectal, presacral, and pelvic nodes up to the S1/S2 junction. The anal sphincter was included in the CTV, in case any abdominoperineal resection had been planned, resulting in an upper border at the level of the promontory and lateral borders 1.5 cm over the pelvic inlet. In lateral fields, the entire sacrum was included, and the anterior border included the posterior part of the prostate or vagina. Subsequently, CTV was delineated according to the available guidelines in 2006, including the primary tumor, mesorectal, and pelvic subsites. 8
5-Fluorouracil and leucovorin or capecitabine, alone or in association with cisplatin (Plafur) or oxaliplatin (Xelox), were administered as concomitant chemotherapy.
Radical surgery, including TME, and abdominoperineal resection (APR) or LAR, with colorectal or colon-anal anastomosis, was performed according to surgical evaluation.
The pathologic response was evaluated according to TNM pathologic classification and tumor regression grade (TRG), according to the Mandard score. 9 The absence of residual cancer in resected specimen (TRG 1) was defined as pathologic complete response (pCR).
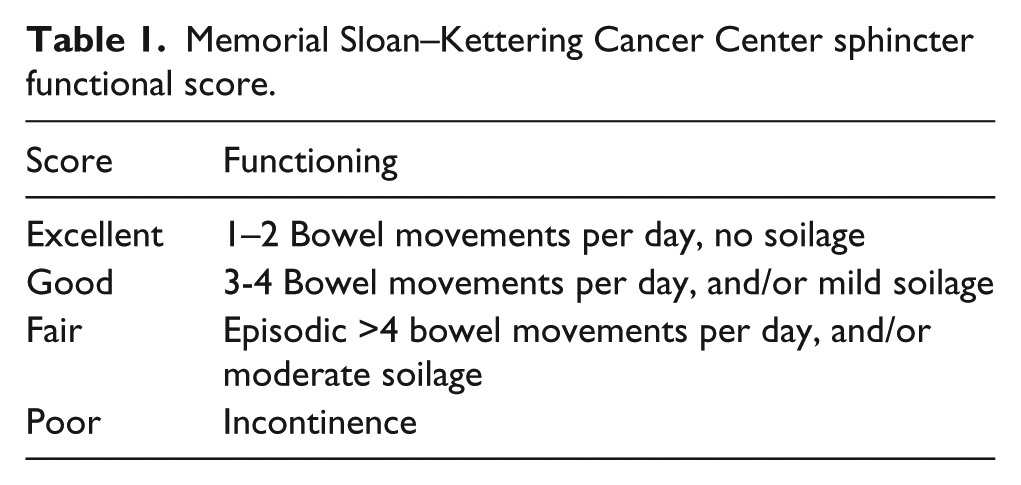
Acute toxicities were assessed using the Radiation Therapy Oncology Group (RTOG) scale. 10 Postoperative routine follow-up examinations were performed every 6 months from surgery during the first 5 years from surgery, then annually. Gastrointestinal symptoms and anorectal function of patients were evaluated at baseline and at every follow-up examination. Late toxicities were reported according to the RTOG/European Organization for Research and Treatment of Cancer (EORTC) late radiation scoring system. 11 The Memorial Sloan–Kettering Cancer Center (MSKCC) score was used to evaluate anal sphincter continence, evaluating the number of evacuations per day including incontinence episodes12,13 (Table 1). Patients presenting stoma or poor sphincter function were reevaluated to assess the impact of bowel function on QoL, using indexes by cancer linear analog scales (CLAS). 14 Impact on well-being (CLAS1), fatigue (CLAS2), and ability to perform daily activities (CLAS3) were considered mild, moderate, or severe when the registered score was 1–4, 5–7, or 8–10, respectively.
Memorial Sloan–Kettering Cancer Center sphincter functional score.
All qualitative variables were summarized in terms of frequency and percentage, whereas all quantitative variables were summarized in terms of mean and SD or median and interquartile range (IQR) according to their distribution, following the Shapiro-Wilk test. The statistical significance of differences between MSKCC score subgroups with respect to qualitative variables was assessed using the chi-square test. t Test was used for unpaired data and one-way analysis of variance was applied for comparing quantitative variables between subgroups. The Kaplan-Meier method was used to calculate the 5-year and 10-year overall survival (OS), local control (LC), and disease-free survival (DFS) rates. The follow-up was defined as the time interval between surgery and death for OS curve, the time interval between surgery and the first verified event for the DFS curve, and as the time between surgery and the local recurrence for the LC curve. As regards patients who were not affected by any of these events, the observation time interval was defined as the period from surgery to the last follow-up examination. A p value of 0.05 or less was considered statistically significant. All statistical analyses were performed using SPSS software 13.0 (SPSS, Chicago, IL).
Results
Detailed data of the population included in the study (201 patients), as well as the tumor and treatment characteristics, are shown in Table 2. The mean patient age was 62.2 years (range 32–88 years); 122 (60.7%) patients were male and 79 (39.3%) female. Mean length tumor was 49.3 mm (SD 17.7 mm), sited at a distance from the anorectal ring shorter than 30 mm, between 31 and 50 mm, and longer than 50 mm in 43 (21.4%), 66 (32.8%), and 77 (38.3%) patients, respectively. The majority of patients (82.5%) had cT3 tumors.
Tumor and patient characteristics (n = 201).
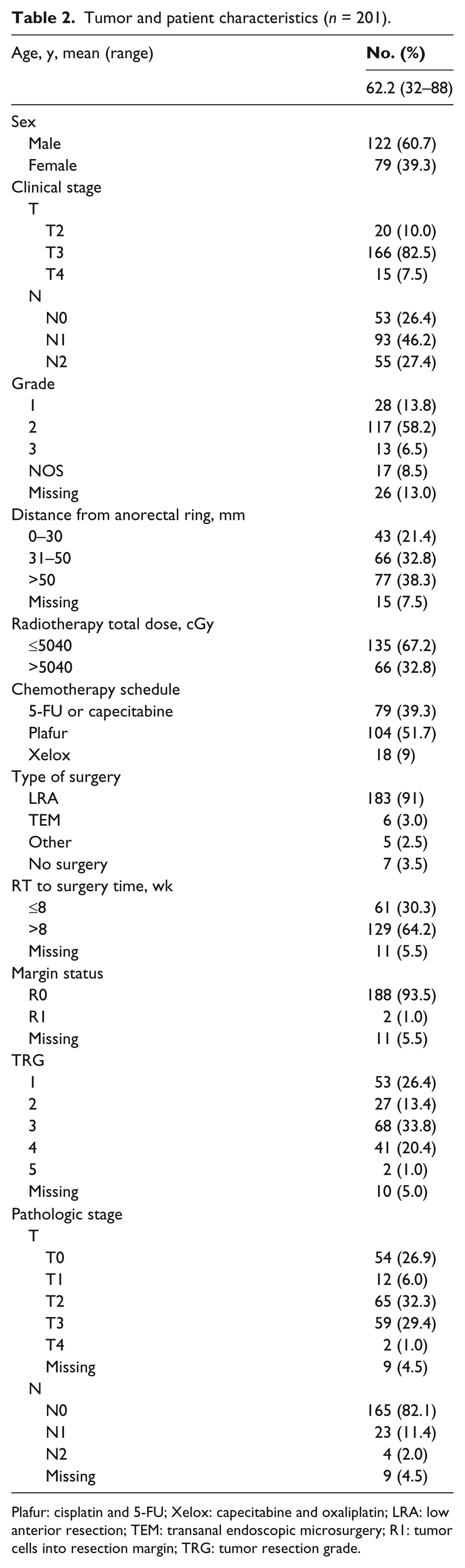
Plafur: cisplatin and 5-FU; Xelox: capecitabine and oxaliplatin; LRA: low anterior resection; TEM: transanal endoscopic microsurgery; R1: tumor cells into resection margin; TRG: tumor resection grade.
Sixty-six patients (32.8%) received a RT schedule using concomitant boost with a total dose of 5500 cGy. Concomitant chemotherapy based on 5-FU or capecitabine was administrated to 79 patients (39.3%). An intensification with the addition of cisplatin or oxaliplatin was given to 104 (51.7%) and 18 (9%), respectively.
Acute toxicities higher than G2 according to the RTOG scale were reported in 23 (11.4%) patients: skin (humid exfoliation) in 9 (4.5%) patients, gastrointestinal (rectal bleeding and/or severe diarrhea) in 9 (4.5%), genitourinary (hematuria) in 6 (3%). Three (1.5%) patients reported a hematologic G3 (anemia) toxicity, requiring blood transfusions (Table 3).
Acute toxicity of 201 patients, n (%).

Seven patients (3.5%) refused surgery. A total of 194 patients underwent surgical resection with a median interval of 9 weeks from the end of RT (IQR 8–11 weeks). Radical resection was performed in 188 patients, with a pCR rate of 26.4%. Overall, postoperative complications were reported in 31 (15.4%) patients and the major ones, mostly represented by anastomotic leakage, abscess, and fistula, occurred in 7 (3.5%), 3 (1.5%), and 6 (3%), respectively.
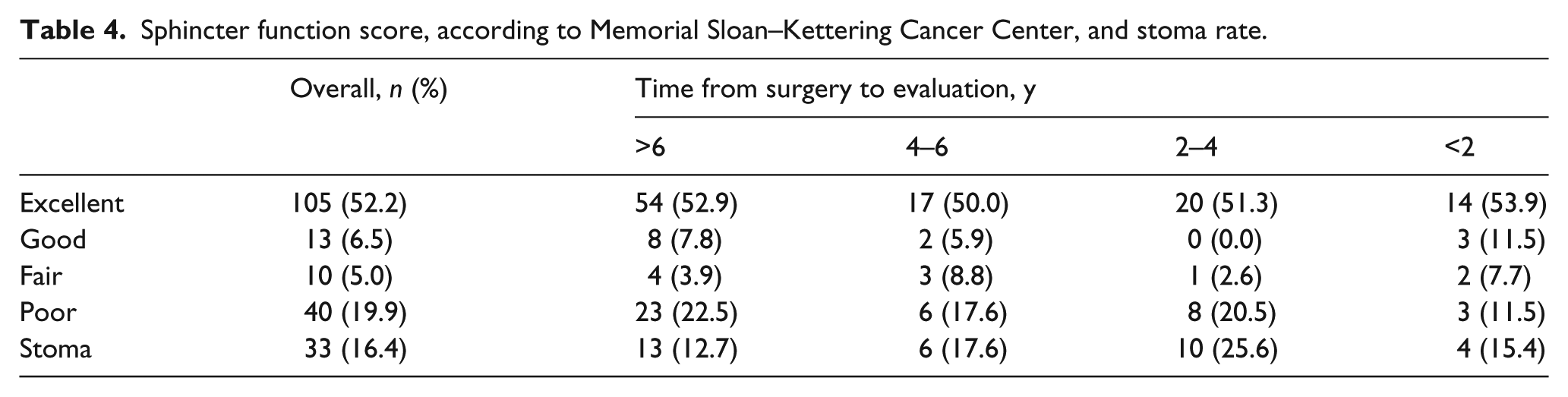
At a median follow-up of 68 months (IQR 35–113 months), the overall sphincter function evaluated according to the MSKCC score was excellent in 105 (52.2%) patients, good in 13 (6.5%), fair in 10 (5.0%), and poor (incontinence) in 40 (19.9%). Thirty-three patients (16.4%) had persistent stoma, one of them due to sphincter incontinence. In addition, as detailed in Table 4, considering the last follow-up, MSKCC score was reported at different intervals, showing excellent and good score in 62 (60.7%) patients, evaluated after more than 6 years.
Sphincter function score, according to Memorial Sloan–Kettering Cancer Center, and stoma rate.
In 117 patients, comparison with a previous evaluation was performed. A total of 11.9% of patients had improved sphincter function after 2 years from previous evaluation.
No statistically significant correlation between sphincter function and patients’ age (≤ or >65 years; p = .804), tumor location (≤30 mm, 31–50 mm, >50 mm; p = .202) or size (p = .487), or RT schedules (≤ or >5040 cGy; p = .639) was found.
Seventy-three patients presenting stoma or poor sphincter function were then retrospectively evaluated using QoL indexes by CLAS. Thirty-three (45 %), 10 (14%), and 9 (12%) patients reported a mild, moderate, or severe impact of bowel function on well-being (CLAS1). Regarding CLAS2, 40 (55%), 8 (11%), and 6 (8%) patients reported mild, moderate, or severe fatigue, respectively. Finally, 34 (47%), 6 (8%), and 9 (12%) patients declared a mild, moderate, or severe impact of bowel function on the ability to perform daily activities (CLAS3), respectively. Twenty-one (29%), 19 (26%), and 24 (33%) patients declared any variation concerning well-being, fatigue, and ability to perform daily activities.
Grade 3 late bowel dysfunction in terms of bleeding (RTOG/EORTC scale) requiring surgery was reported in 3 patients (1.5%). Mild (5 daily bowel movements) and moderate (more than 5 daily bowel movements) diarrhea was reported in 53 (26.4%) and 24 (11.9%) patients, respectively. No other severe late toxicities were recorded, except for 1 (.5%) case with gross telangiectasia and 2 (1%) patients with severe dysuria.
The 5-year OS, DFS, and LC rates were 88.0% ± 2.6%, 86.3% ± 2.5%, and 94.6% ± 1.9%, respectively. Long-term results were also evaluated showing a 10-year OS, DFS, and LC of 72.1% ± 4.4%, 62.9% ± 4.4%, and 92.2% ± 2.5%, respectively.
Discussion
Since a multimodal approach for rectal cancer treatment, including neoadjuvant short course RT and/or CRT, followed by anal sphincter preserving surgery, has led to improved oncologic outcomes, the possibility of offering lower toxicities with good QoL, especially in long-survival and young rectal cancer patients, is currently a relevant end point investigated in different trials (Table 5).
Major phase II and III studies evaluating bowel movement frequency and sphincter functionality in preoperative radio-chemotherapy.
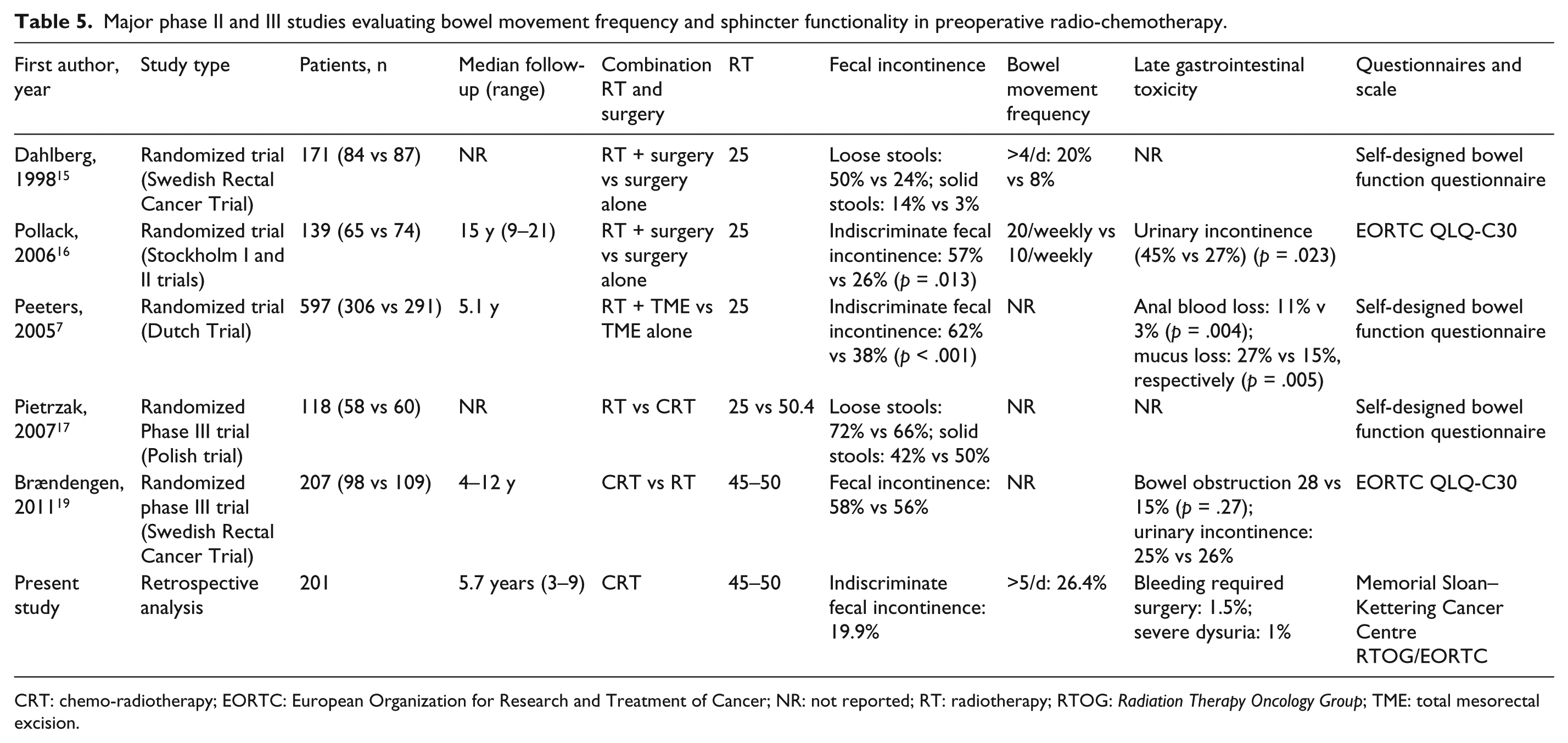
CRT: chemo-radiotherapy; EORTC: European Organization for Research and Treatment of Cancer; NR: not reported; RT: radiotherapy; RTOG: Radiation Therapy Oncology Group; TME: total mesorectal excision.
Knowledge of late adverse effects of RT on bowel and sphincter function for rectal cancer comes mostly from randomized trials on 5×5 Gy RT or postoperative RT.3,7,15–17 Data regarding their impact on QoL are not always concordant.
In the Swedish Rectal Cancer Trial, 171 patients treated with preoperative RT and anterior resection were evaluated for bowel function, showing an increase of bowel dysfunction with loose stools incontinence, urgency, and emptying difficulties compromising social life in the irradiated group. 12
However, long-term analysis (mean follow-up 15 years) on 139 patients treated with surgery and with or without preoperative RT included in the Stockholm Radiotherapy Trials showed that patients in the RT group experienced a higher number of late complications, represented by fecal incontinence (57% vs 26% patients having undergone anterior resection) and urinary incontinence (45% vs 27%). 16 Moreover, in a subanalysis on 64 patients (mean follow-up 14 years), the group with anal incontinence had significantly lower QoL scores compared to continent patients, showing that anal incontinence was the most important factor impairing QoL, without any significant difference in QoL scores between irradiated and nonirradiated patients. 3
The 5-year follow-up of the Dutch TME trial 7 showed an increased rate of bowel dysfunction in terms of fecal incontinence (62% vs 38%), pad wearing for incontinence (56% vs 33%), anal blood loss (11% vs 3%), and mucus loss (27% vs 15%) in irradiated compared to nonirradiated patients, with a negative impact on daily activities. Also, the fecal incontinence frequency (more than once a week) was higher after RT compared to surgery alone (25% vs 11%). The risk factors for fecal incontinence reported in the Dutch TME trial were then evaluated 3, 6, 12, 18, and 24 months after surgical treatment, in the same median follow-up of 5 years, on 339 patients treated with LAR, with or without short-course preoperative RT. 18 Fecal incontinence occurred especially in patients treated with RT, in particular in cases of perineum irradiation. Moreover, in patients treated with preoperative RT, excessive blood loss was the main risk factor related to and predicting incontinence at both 2 and 5 years. An anastomosis level closer to more than 40 mm from the anal verge and a low tumor site were significantly associated with bowel impairment at 2 or 5 years as well.
Some randomized and nonrandomized trials are also been conducted to evaluate the effects of preoperative long-course radiation plus chemotherapy on anorectal function.
A Polish randomized trial compared short-course preoperative RT (5 × 5 Gy) with CRT (50 Gy, 5-fluorouracil/leucovorin), reporting no significant differences in the proportion of patients having anorectal function and sexual impairment. However, mean follow-up time from surgery was only 1 year and probably too short to be conclusive concerning late RT toxicities . 17
Late side effects of RT alone compared to integrated (5-fluorouracil/leucovorin) CRT have been reported in a phase III randomized Swedish trial. 19 Fecal incontinence, erectile dysfunction, and urinary complications were found to be the most frequent late sequelae in both groups, with a more significant trend in patients treated with CRT. No statistically significant differences related to the rate of permanent stoma were reported (73% vs 52%, p = .09). The only difference in the RT alone group was in the number of patients without permanent stoma and with good anal functionality (11% vs 30%, p = .046).
Considering the relevant issue, we retrospectively analyzed patients with rectal cancer treated with long-course preoperative CRT in our center, in order to assess long-term effects on anorectal function (median follow-up 68 months).
Despite the retrospective analysis, our results were in good agreement with literature data (Table 5). Sphincter incontinence was shown in 19.9% of patients, whereas an overall excellent and good sphincter functional score was reported in 60.7% of patients over a follow-up period of more than 6 years (Table 4). Moderate (more than 5 daily bowel movements) diarrhea was reported in 11.9% of patients, and severe bowel dysfunction in terms of bleeding requiring surgery in 3 patients (1%).
In particular, our study confirmed data from previous studies using the MSKCC score.20,21 In a retrospective study on 100 patients treated between 1996 and 2003 with neoadjuvant CRT and TME, sphincter function resulted excellent in 53 patients, good in 22, fair in 20, and poor in 5, and only 14% of the patients were not satisfied because they had to use a pad, whereas 81% were content. 20 In 193 rectal cancer patients receiving preoperative CRT or only surgery, increased defecation problems with reduced social activities were found in patients receiving CRT, with persistent problems of leakage of stool, limiting daily activities due to their bowel function. Defecatory dysfunctions were reported in 102 patients and stoma-related issues in 32 patients. 21
Considering that, as reported in many studies, 5 bowel movement frequency tends to increase immediately after resection, decrease progressively and slightly during the first year, then become stable after the second year. An evaluation of the MSKCC score was performed in our patients at 2-year follow-up: 11.9% of the patients who had undergone previous evaluation (117 patients) presented an improvement in sphincter function.
Due to its retrospective design, one of the limits of our analysis was the absence of pretreatment anal sphincter function evaluation. Although at baseline most of the patients had not experienced sphincter dysfunction or fecal leakage, the major issue was rectal bleeding. Furthermore, although QoL questionnaires were not used, a retrospective analysis of patients presenting stoma or poor sphincter function was carried out to assess the impact of bowel function on QoL. About 30% of the patients declared no variations in well-being (CLAS1), fatigue (CLAS2), or ability to perform daily activities (CLAS3). 14
A prospective study for sexual dysfunction evaluation with more detailed QoL questionnaires is in progress in our department.
Conclusion
Our analysis showed good results in terms of sphincter functionality and late toxicities and 5-year OS, DFS, and LC rates, in agreement with the available literature. Since CRT and radical surgery, mostly represented by TME, could adversely affect anorectal function, patient stratification could improve functional outcomes by better identifying the patients who could benefit from neoadjuvant therapy for the treatment of rectal cancer. Routine use of scales evaluating late toxicities, bowel and sphincter dysfunction, and their impact on QoL could contribute to a more thorough selection of patients at high risk of developing functional issues.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.