
Abstract

PROGRAMME OF OECI 2019 ONCOLOGY DAYS
Editorial Board:
Giovanni Apolone (Milan)
Gennaro Ciliberto (Rome)
Ruggero De Maria (Rome)
Paolo De Paoli (Rome)
Antonio Delvino (Bari)
Claudio Lombardo (Brussels)
Thierry Philip (Paris)
Nicola Silvestris (Bari)
Scientific Secretariat:
Antonella Argentiero (Bari)
Section 1: welcomes
Thierry Philip
Matti Aapro, Giovanni Apolone, Angelika Eggert, Alexandru Eniu, Xosé M. Fernández, Thierry Philip, Otmar D. Wiestler, Manfred Weber
Giovanni Apolone, Gennaro Ciliberto, Ruggero De Maria, Paolo De Paoli, Claudio Lombardo, Thierry Philip, Nicola Silvestris
Giovanni Leonardi
Michele Emiliano
Antonio Felice Uricchio, Giovanni Migliore, Antonio Delvino
Section 2: Scientific papers
Pathology Day
Giorgio Stanta
Olli Carpén
Reinhard Buettner
Dominique Figarella-Branger
Luciana Neamţiu
Angelo Virgilio Paradiso, Mariagrazia Daidone, Barbara Parodi, Anna Sapino, Gerardo Botti
Marco G. Paggi, Rita Falcioni, Ruggero De Maria, Pier Giuseppe Pelicci, Gennaro Ciliberto
Eliseo Mattioli, Anna Altavilla, Leonardo Resta, Ettore Attolini, Lucia Bisceglie, Antonella Caroli, Francesco Alfredo Zito
Antonio Federici, Claudio D’Amario
Patient Day
Patrick Miqueu and Dominique de Valeriola
Mervi Siekkinen, Ritva Kosklin, Hanna Ilus, Teija Kemppainen, Sirkku Jyrkkiö, Pia Vihinen
Sara Paltrinieri
Chiara Ariotti
Martine Bouyssie
Laura Del Campo, Olga Sapoznikov, Francesca Traclò, Nicola Di Flora, Francesco De Lorenzo, Silvia Carelli, Alessandro Sproviero and INTENT group
Camilla Havsteen and Anne Skov Villadsen
Anne Grethe Ryen Hammerstad
Bernd Kremer
Francesca Romito
Véronique Gillon
Patrick Miqueu
Scientific Conference
Sabino Ciavarella, Maria Carmela Vegliante, Marco Fabbri, Simona De Summa, Federica Melle, Giovanna Motta, Anna Enjuanes, Alessandro Gulino, Stefania Tommasi, Anna Scattone, Alfredo Francesco Zito, Claudio Agostinelli, Umberto Vitolo, Annalisa Chiappella, Elias Campo, Claudio Tripodo, Attilio Guarini, Stefano A. Pileri
Caterina Aversa, Johann S. de Bono
Paolo De Paoli, Silvia Careccia, Gennaro Ciliberto, Anna Sapino, Pier Giuseppe Pelicci, Ruggero De Maria
Antonio Delvino, Giovanni Battista Bochicchio, Nicola Silvestris, Alessandro Sgambato, Gerardo Botti, Elio Borgonovi, Angelo Rosa, Rosa Martino, Pietro Milella, Antonio Colasurdo, Carmine Mariano, Massimo Mancini, Cristiana Mecca, Attilio Bianchi
Thierry Philip
Philip Poortmans, Richard Price
Francesco de Lorenzo, Antonella Cardone, Alex Filicevas
Denis Lacombe
Joanna Kazmierska, Núria Jornet Sala, Michelle Leech, Chiara Gasparotto, Barbara Alicja Jereczek-Fossa, Yolande Lievens, Umberto Ricardi, John Yarnold
Carolina Espina, Linda Bauld, Bernardo Bonanni, Hermann Brenner, Karen Brown, Joakim Dillner, Ellen Kampman, Mef Nilbert, Paolo Vineis, Matty P. Weijenberg, Alison Cox, Theo M. de Kok, Daniela Fecht, Giota Mitrou, David C. Muller, Davide Serrano, Karen Steindorf, Hans Storm, Mangesh A. Thorat, Fränzel van Duijnhoven, Elisabete Weiderpass, Joachim Schüz
A&D Session
Simon Oberst
EDITORIAL: INTRODUCING A EUROPEAN MASTER PLAN 2027 TO FIGHT CANCER
Thierry Philip
OECI President
Europe has been often criticised for its reduced capacity to find a common ground and, cancer-wise, for the absence of a project which may unify the 28 Member Countries and build a common vision of the actions to be undertaken so as to reduce incidence, provide our patients with the best treatments and promote innovation.
Over the past two years, the European Cancer Organisations, and several stakeholders, debated on a possible Cancer Mission without managing to agree on a common objective concerning “what can we do”. The debate is still open.
On the other hand, in a document entitled “A European Cancer Plan for Children and Adolescents” and in the 2019 Manifesto “Cure more and cure better, towards zero deaths and zero late effects”, the European pediatric cancer community has already demonstrated a common vision on the feasibility of a Pediatric Cancer Mission. As a result, the European Commission, the Parliament and the Research Council strongly supported a “moon-shot” vision on pediatric cancer to ensure “90% survival and reduce toxicity by half”.
The European pediatricians are members of SIOPE, the International Society of Pediatric Oncology Europe, and they have already adopted common protocols to disseminate innovation throughout Europe, including Eastern and Southern European Countries. At the same time, SIOPE has established practical connections with the USA, China, South America, it is linked to industries and to the best fundamental research Institutes in Europe. What’s more, the pediatricians work in close relationship with patient organisations and are active promoters of innovation in cancer care in Africa.
Since 2018, in my quality of President of the Organisation of European Cancer Institutes, regrouping about 100 among the most prominent European Comprehensive Cancer Centres/Institutes and Comprehensive Cancer Centres within a university hospital, I was called to find a bottom-up approach to agree on a common vision for a European Cancer Mission in adults, similarly to the proposal put forward by the pediatricians. The approach, discussed during a Meeting organised in Brussels, where representatives of the most important cancer organisations of professionals partecipated, has been endorsed by the patient organisations.
In fact, the European Cancer Patients Coalition and the European Cancer Leagues should play a major role and I am sure that they will enthusiastically take their roles as part of a European Mission to join our forces in the fight against cancer.
Unfortunately, we were not able to reach a consensus with all the actors interested to launch and participate to such a major breakthrough.
Eng. Manfred Weber, Member of the European Parliament, and candidate to the Presidency of the European Commission, recently proposed a Master Plan to fight Cancer, a Vision that has been endorsed by several top cancer scientists and representatives of European cancer organisations, including the OECI.
The Weber’s proposal, to be realised as part of Horizon Europe, will give the European dream a new breath of life: as President of OECI and of the Institut Curie, I strongly support this approach confirming the Marie Curie’s belief that “Science is international”.
Despite winning two Nobel Prizes, she never patented her discoveries because she maintained that innovation was a humanity heritage and should be shared for free. Marie Curie, one of the World Founder of the Comprehensive Cancer Centres concept, would certainly support a European Master Plan to join our forces in the fight against cancer.
I firmly believe that the cancer fight cannot be seen from left or right, because patients have not political appurtenance and ask us to receive the best available treatments and to provide innovation in cancer. A Mission is a new chapter of the European dream and as an individual with my whole background, as OECI President and as heir of Marie Curie’s human values, I strongly support this Master Plan proposal. Therefore, I will fully engage to achieve its ultimate goal: equality of chances when a European citizen is diagnosed with cancer in the north, west, east or south, in rich or less rich countries.
Big data, artificial intelligence and machine learning will be at the heart of the means to achieve these objectives and Weber’s proposed Plan of Action is at the core of what could become a Cancer Mission.
24 of the 28 European Countries currently have a National Cancer Plan or a major chapter on cancer in a global public health plan. Therefore, one of the main challenges to be undertaken is making a real joint venture among the European research and innovation ambitions and the health and care responsibilities assigned to the Member States.
We also need a better connection among the European Commission Directorates that should be working in synergy and not as independent pillars, each one bearing its own responsibility on a specific policy. Amore transversal view connecting Research, Public Health, Industry…. and a stronger cooperation among Member States and Europe is what currently is needed.
Prof. Thierry Philip
Curie Foundation President
OECI President
A EUROPEAN MASTER PLAN TO JOIN OUR FORCES IN THE FIGHT AGAINST CANCER
Matti Aapro, MD1, Giovanni Apolone2, Angelika Eggert3, Alexandru Eniu4, MD, PhD, Xosé M. Fernández5, Thierry Philip6, Otmar D. Wiestler7, Manfred Weber8
1Genolier Cancer Center Board of Directors member, Clinique de Genolier, Switzerland, 2Scientific Director Fondazione Istituto Nazionale dei Tumori – Milan – Italy – Germany, 3Director of the Department of Paediatrics m.S. Oncology and hematology from the Charité in Berlin - Germany, 4Cancer Institute “Ion Chiricuta” Cluj-Napoca Romania & European School of Oncology Deputy Scientific Director, Bellinzona/Milano –Switzerland/Italy, 5Chief Data Officer, Institut Curie, France, 6President of OECI & President, Institut Curie, France, 7President of Helmholtz Association of German Research Centres, 8EPP Lead Candidate - Germany
I.The decisive fight of the 21st century: the war against cancer
When divisions and egoism seem to endanger our European unity, it is time to remember what Europeans are capable of achieving when they work together. We must start from what really matters to the citizens, from what makes a difference in their lives. While Europe is threatened both internally and externally, we must not forget our most insidious enemy that we are not able to defeat. We have not won the war against cancer yet.
Cancer represents the first cause of death in an increasing number of European countries1 and 40% of us will face cancer in our lives.2 This is an enemy in continuous evolution, that quickly mutates and that takes over 100 different forms. So many people courageously go through this struggle every day, in the quiet of their homes, facing the feeling of being powerless, the difficulty of the loved ones to go on in the everyday life, the grief.
Today, only 1 out of 2 cancer patients survive: this is not enough. If we truly pool all our knowledge and resources together, we can pursue ambitious goals so that, by combining prevention, early diagnosis and screening with personalized medicine, we could double the survival rate of bad prognosis tumours. In paediatrics, 80% of children are cured. Although this is a remarkable result, we can do much more and make sure at least 90% are cured by 2030. By reaching this goal, 30.000 more children around the world could be saved each year.3 It is our lives and the lives of our loved ones that are at stake. That is why Europe must join forces and take up arms: the fight against cancer has to be an absolute priority of the next European Commission.
II.Seizing the digital wave: one key to the solution
While medicine is becoming increasingly digital, key technological advancements will shape innovation in the health sector all over the world: finding a cure for cancer will be one of the crucial research questions of the future. If we want to succeed, Europe must seize the great opportunities that are being created by revolutionary advancements in biomedicine, bioinformatics, Big Data and artificial intelligence to put patients at the centre and support them to go through this difficult path in the least painful way possible.
What makes cancer so dangerous is that it is such a complex disease. Tumours that come under the same umbrella term will often be quite different: for example, there are many types of breast cancer, but they are still collectively called breast cancer. In addition to this, tumours go through an evolutionary process due to their genetic instability, which means they can quickly become different and so become resistant to treatments that were previously working. In the last two decades, revolutionary progress has been made to deal with these issues. Immunotherapy, a treatment that involves taking medicines that encourage the immune system to fight cancer, has shown promising results alongside smart drug combinations, which use two or more already known drugs taken together to fight cancers. Advancements in genomic research and the reduction of cost for DNA sequencing is allowing research on tumour cell mutations to progress much faster. Further studies in epigenetics, will enable researchers to look deeper, beyond DNA and combine it with information about external factors.
From these remarkable developments in medicine and technology, a massive amount of data is being generated that holds great potential for new discoveries. However, such an amount of data cannot be collected and analysed traditionally. That is why it is crucial for Europe to combine the potential of biomedicine and Big Data to take the next step in cancer research and treatment. As medicine is ultimately based on previous knowledge and experiences, harnessing the opportunities provided by Big Data and artificial intelligence allows researchers and doctors to directly query the past to predict the future more accurately and more quickly. This can lead to breakthrough advancements in cancer prevention and early-detection, it can mean quicker diagnosis, improved testing capabilities of drugs as well as to allow for more tailored, personalized and quicker treatment of patients so that no precious time would be wasted.
Despite the impressive progress, a number of obstacles remain that prevent the full European potential in cancer research, treatment and patient support to be unleashed.
Data and information are not always sufficiently shared and easily accessible, especially to remote and rural areas.
Even when results are available thanks to open access initiatives, the amount of data is so vast that finding the desired piece of information may be like looking for a needle in a haystack.
Access to appropriate technological infrastructure to analyse the data is often an issue and Europe excessively relies on foreign technology, especially from the USA and China, which raises dependency as well as security concerns.
It still makes too much of a difference to get sick in the East rather than in the West of Europe: in fact, depending on the type of cancer a patient in the East will have 30% less chance to heal, a dramatic and unacceptable reality.4 Similarly, there are fewer clinical trials currently taking place in the East compared to the West, which can make advancements more difficult to achieve: in EU-13 there are currently just under 5.000 clinical trials taking place, while in EU-15 there are over 26.000.5
There is an increasing burden of cancer in Europe as more people are diagnosed each year, many of them having other diseases related to their age. Cancer could become more difficult to deal with due to the high volume of cases. In addition, there is currently insufficient focus on prevention and early detection strategies, which could be used to reduce this growing burden.
Patients, their families, and all those who care for them not only need support during the difficult times of the treatment, but they need as much support after care as well. Cancer survivors often find it hard to go on with their lives as they face prejudice due to their medical history. For example, banks not giving them a mortgage to buy a new house, insurance companies turning them away or new employers refusing to hire them, all because of their past disease. Despite being completely healed, they are forced to live with a stigma.
That is why we need to remind everyone of what Europe is all about: Europe is about making sure each and every one of its people enjoys a good life and has access to the same chances. Europe is about making the world a better place.
III.Together, we can fight back: launching a European Master Plan to fight cancer
In Europe, we already have everything it takes to achieve ambitious goals: brilliant minds, strong drive, resources, innovative spirit, and solid values that embrace diversity. This is the source of our greatest strength; what makes Europe unique. Our continent has historically been at the forefront of revolutionary discoveries. Now, we have to look ahead and take up our responsibility to face the great challenge of our time. We only need to renew our efforts once more and come together as the community we are to spread and consolidate the achievements of the past while seizing the opportunities of the future.
As cancer is not just one disease but, for each type, many other subtypes exist, Europe must rely on the specialisation and expertise of each centre. That is why it is crucial for the European Union to harness the network potential. By establishing a
We want to employ research and innovation purposefully, by bringing biomedicine and Big Data together and empowering the new generation of data scientists. To handle the huge volume of research data, we must invest in artificial intelligence that would be available to all researchers and can assist in quickly identifying the most pertinent research for a given case. In this way, research would spread much faster, it would not be limited only to the most well-funded centres, but also extend to experts throughout Europe and results would reach patients much earlier.
Our efforts must go towards bridging the gaps in the continuum of cancer basic and clinical research and care with supportive and palliative aspects. There have been huge successes in survival rates for some cancer types. For paediatrics, for example, 80% of all cases are cured, 83% of breast cancer sufferers survive8, as do over 85% of those with HPV throat cancer.9 With some cancers so close to reaching 100% survival rates and the possibility of reducing the increasing incidences of cancer, if we are even more ambitious with focused and joint efforts, they could be eradicated completely.
All centres and hospitals in Europe, all health care providers in their speciality, must be able to reach the highest standard of care and benefit from the scale of European-wide action in their research, for instance by pooling knowledge for clinical trials on a particular cancer sub-type. By launching a
There should be no differences in cancer care across European regions: patients in remote areas and small villages have to be able to benefit from the same quality care of patients in central areas and Europe must strive to achieve the same survival rates for good prognosis patients in every European country. That is why Europe must harness the revolutionary potential of technology to break down distance barriers across Europe by creating
Most of us have a dear friend or family member who has battled cancer. It is a very intimate matter for a family and, yet, it concerns us all. We found a vaccination against smallpox. We found penicillin against pneumonia. Together we have already eradicated these devastating diseases. Why should we not also manage to eradicate cancer? Let’s make it a common project. Europe has the minds, the capacity and the energy: it has only to unleash its potential to take the lead in this fight. Together we, Europeans, can join our forces and strive to find a cure. Let us launch a European master plan to cure cancer.
Acknowledgements
This paper has also greatly benefitted from the contribution of the following experts and it was written with deep thanks for their insights and expertise.
European Commission, Research and Innovation, Cancer, https://ec.europa.eu/research/health/index.cfm?pg=area&areaname=cancer
Zentrum für Krebsregisterdaten, https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebsgeschehen/Krebsgeschehen_node.html
WHO, Cancer in Children, https://www.who.int/news-room/fact-sheets/detail/cancer-in-children
Euronews, “Cancer survival rates ‘improving across Europe’”, https://www.euronews.com/2018/02/04/cancer-survival-rates-improving-across-europe-
ClinicalTrials.gov, https://clinicaltrials.gov/ct2/results/map?cond=Cancer&map=EU
Berns et al, “A mission-oriented approach to cancer in Europe: Boosting the social impact of innovative cancer research”, European Academy of Cancer Sciences and the Pontifical Academy of Sciences, The Vatican, November 16-17, 2018.
D. Forman et al, “Time for a European initiative for research to prevent cancer: A manifesto for Cancer Prevention Europe (CPE)”, Journal of Cancer Policy, Volume 17, pp. 15-23, 2018.
Euronews, op. cit.
Mountsinai, Head and Neck Institute, Cancer, https://www.mountsinai.org/locations/head-neck-institute/cancer/oral/hpv-faqs
THE 41st OECI ANNIVERSARY: WELCOME TO BARI
Giovanni Apolone1, Gennaro Ciliberto2, Ruggero De Maria3, Paolo De Paoli4, Claudio Lombardo5, Thierry Philip6, Nicola Silvestris7
1Scientific Directorate–Fondazione IRCCS National Cancer Institute, Milan, 2Scientific Directorate–IRCCS Regina Elena National Cancer Institute, Rome, 3Institute of General Pathology, Catholic University of the Sacred Heart, Rome, 4Alliance Against Cancer, Rome, 5OECI, Brussels, 6OECI President–Fondation Universitaire–11, Brussels, Belgium, 7Scientific Directorate–National Cancer Institute “Giovanni Paolo II,” Bari, Italy
The year 2019 marks the 41st anniversary of the founding of the Organization of European Cancer Institutes (OECI). After 13 years, Italy has been elected as the host country for the OECI Oncology Days Meeting, where the city of Bari has been awarded the privilege of hosting this prestigious event. Everything that has been accomplished up to now has been made possible thanks to the support of all the Scientific Directors of the Cancer Centres in Italy and the Italian Cancer Network “Alliance Against Cancer” (Alleanza Contro il Cancro [ACC]).
The 41st Anniversary of OECI takes place in Bari, Italy, from the 19th until the 21st of June. It has been organized in collaboration with the National Cancer Institute “Giovanni Paolo II.”
The “2019 OECI Oncology Days” meeting covers a range of topical issues in the field of oncology. The aim of the Scientific Conference OECI 2019 is to provide ground for joint actions that will be focused both on highlighting tumour heterogeneity among research institutes in Europe and on emphasizing the pivotal role of ACC in carrying out translational research dedicated to precision medicine. The aim is to exchange data and ideas concerning the difficulties and opportunities which may emerge from a thorough understanding of the impact of tumour heterogeneity in cancer treatments. We envision that this approach may provide ground for working towards the next generation of cancer therapies, in which dynamic clinical practice, along with the active collaboration of patients, can provide timely adjustments of antineoplastic strategies.
THE 2019 OECI ONCOLOGY DAYS PROGRAMME
First day: June 19
The Organization of European Cancer Institutes (OECI) Pathology Day focuses on molecular pathology in aggressive types of tumours. The speakers go in depth on various types of tumours, such as ovarian cancer, breast cancer, and paediatric tumours. Methods of diagnosis of cancer diseases, such as neuroblastoma, will be explained by using blood samples. The speakers will discuss in detail the plan to implement in order to reach uniform European quality standards and to create specific tumour-related OECI networks. Pathology Day ends with a description of the activities of the Alleanza Contro il Cancro (ACC) Working Group.
The OECI Patient Day focuses on the patient’s key role in decision-making processes to drive better innovation and process efficiency and quality. The OECI is supporting all actions that bring the patient to the table and take into account our aims to reduce inequalities between patients throughout Europe, restrain cancer costs, and integrate palliative and supportive care needs.
Second day: June 20
The Scientific Conference “Tackling tumour heterogeneity: Biological, laboratory, clinical and regulatory implications” aims to discuss tumour heterogeneity and gain deeper insight on its relationship with the following issues:
(a) Biological and laboratory implications: Intratumour heterogeneity among different types of cancers in terms of tumour genomics and characteristics of the tumour microenvironment, through pathologic, molecular, and complex bioinformatics approaches, is explored. The main topics, which are the heterogeneity of cancer, its integration with the tumour microenvironment, and how to translate current knowledge into therapeutic modalities, could be explored only by investigating and disseminating evidence on the capacity of cells to change continuously and adapt to their local and systemic environment (in order to evade death, proliferate, and form metastasis), and by unravelling the routes through which cancer cells circumvent therapeutic targeting.
(b) Clinical and regulatory implications: To bridge the gap between biomedical research and clinical practice, the winning strategy is to establish translational research and clinical networks through interdisciplinary collaboration, funding support and infrastructure.
(c) Introduction to the ACC structure and the Southern Italy Cancer Network: The networks explore opportunities to maximize the skills of each partner in order to reach exploitable results.
All the presentations of the speakers are reported in the first section of this special issue of Tumori Journal, which is already online. The second section of this issue is devoted to introducing the visions of several European Cancer Organisations on a European Cancer Mission to be launched as part of Horizon Europe 2021–2027.
After the Oncology Days 2019 Conference, the participants will have time to enjoy the surroundings. Bari is a charming city, with its origins going back 3500 years, before the Bronze Age.
On behalf of the OECI, the Italian Cancer Network, and the Cancer Institute of Bari “Giovanni Paolo II,” we are looking forward to welcoming you to Bari.
Acknowledgements
The authors thank Tania Merlino for proofreading for English language.
WELCOME ADDRESS: DIRECTOR GENERAL FOR RESEARCH AND INNOVATION IN HEALTHCARE OF THE MINISTRY OF HEALTH: ITALY
Giovanni Leonardi
Direttore Generale della Ricerca e dell’Innovazione in Sanità, Rome, Italy
One of the main tasks of The Ministry of Health is fostering research in healthcare, since we strongly believe that carrying out research within the National Health Service (NHS) helps improve the standards of care of our citizens. The Ministry is endowed with an annual budget of €250 million, part of which is distributed through a national call open to all NHS researchers and in part allocated through the assessment of the activities performed by a selected group of research hospitals, the so-called Istituti di Ricovero e Cura a Carattere Scientifico (IRCCS).
IRCCS are public or private hospitals certified by the Ministry of Health for the high standard of research and clinical care based on a careful assessment of an independent committee, which verifies that the applicant fulfils the requirements set by law.
IRCCS carry out translational research in different disciplines both individually and in networks. Currently, IRCCS networks are set up in oncology, neuroscience and rehabilitation, cardiovascular diseases, paediatrics, and aging.
Alleanza Contro il Cancro (ACC), the network of the oncologic IRCCS, was founded in 2002 by initiative of the Minister of Health and is the largest Italian organization for cancer research.
The vision behind ACC and the other networks is that institutes cooperate on all the research issues critical for healthcare, so that citizens may benefit throughout the country of the best cures and procedures. This allows the NHS to keep up with innovation and helps provide health services at sustainable costs.
Several working groups are active within ACC, coping with lung, breast, and colon cancer, as well as melanoma, glioblastoma, and sarcoma. Other groups deal with immunotherapy, pathology and biobanking, and genomics. As for the latter, a flagship project has been launched, supported by the Ministry of Health, ACC Genomics, a research project that aims at identifying the best therapy for each patient through the clinical validation of large panels for routine sequencing of the actionable tumor genome.
Fostering international cooperation, especially at the EU level, is also a major purpose for ACC. It is actively involved in several EU programs and, in particular, is partner in the ERAnet Transcan, where it acted as Joint Secretariat in the last call. Moreover, ACC was selected to become an MD Anderson Sister Institution.
The relationship between the Ministry of Health and ACC is not confined to research activities only, but also looks at improving the quality of the institutes. To this aim, the Ministry sponsored the accreditation by Organization of European Cancer Institutes (OECI) of all the IRCCS belonging to the network, an initiative launched in 2012 by Angelo Paradiso, who was at that time the Scientific Director of the Bari Institute. For this reason, celebrating the Oncology Days in Bari acknowledges the role of the Istituto Oncologico “Giovanni Paolo II” in strengthening the partnership between OECI and ACC.
We thank OECI for the conscious and professional job performed. We also confirm our availability to support the accreditation process in the future, as we believe that undergoing independent international review is the best way to sustain the quality of our IRCCS.
WELCOME ADDRESS: PRESIDENT OF THE APULIA REGION
Michele Emiliano
President of the Apulia Region
The month of June will be a very exciting month for the region of Apulia and the city of Bari. After 13 years, Italy will welcome once again the Organization of European Cancer Institutes Oncology Days and Bari has been chosen as the host city for this prestigious event. Owing to the untiring efforts of all the clinicians and researchers, coordinated by doctors Antonio Delvino and Nicola Silvestris, the first General Director and the second Scientific Director of the institute, who synchronized all the activities related to the organization of this event, we will have the privilege of being part of this experience.
The Apulia region acknowledges the hard work and the dedicated efforts that the Cancer Institute has put forth in the recent past.
The year 2018 has seen the birth of the Apulian Cancer Network (Rete Oncologica Pugliese). This network gathers all the regional cancer-related operative units with the aim to guarantee the best possible cure and assistance for each Apulian patient. The ongoing development of clinical and research activities of the Institute have led it to play the role of coordinator of this network.
The efforts of clinicians and researchers of the Cancer Institute have not only been recognized in our region, but also at national and international levels as well.
The region of Apulia is honoured to host this event and welcomes all the international guests who will participate in this congress. I am sure that this will result in a twofold benefit: Bari will have the opportunity to give its best and the guests will have a chance to experience the famous Apulian hospitality. The region will have the chance to proudly show off its historical, archaeologic, and cultural treasures. Along with this, the guests will have the pleasure of tasting our exquisite foods and stupendous wines.
Though over the last few years we have witnessed an increment of tourist arrivals from abroad, we are still pleased with the idea that our region can attract new guests. We hope the guests of our region will find it so enticing that they will want to come back again and again.
All the attractions of the region, all the beauties of the sea, all the goodness of the food, must not lead us to forget the main object of this congress, which is the never-ending efforts that clinicians and researchers put forth to alleviate human suffering.
The welcome mat is ready for you.
INTEGRATION FOR INNOVATION: A NETWORK MODEL AT THE UNIVERSITY OF BARI “ALDO MORO,” THE UNIVERSITY HOSPITAL CONSORTIUM “POLYCLINIC OF BARI” AND THE NATIONAL CANCER INSTITUTE OF BARI–IRCCS “GIOVANNI PAOLO II”
Antonio Felice Uricchio1, Giovanni Migliore2, Antonio Delvino3
1Rector, University “Aldo Moro”, Bari, 2General Director, University Hospital Consortium, Bari, 3General Director, Cancer Institute “Giovanni Paolo II”, Bari, Italy
In recent years, the university has been hit by a series of growing expectations regarding both the ability to influence innovation processes and the ability to generate knowledge as well as the ability to disseminate it. The university is an institution that besides being the depository of knowledge, represents the main tool through which innovations and changes can be made available to all sectors. The current historical phase is characterized by processes of permanent innovation that require not only higher levels of training, but also adaptability, flexibility, and capacity for integration. Thus, universities “integrate” various forms of knowledge, transfer this knowledge through trainers, and act as agents of social and cultural development through research. In other words, they (the universities) can be defined as “knowledge hubs” that represent the terminals on which global networks deposit skills and know-how that can influence development paths. From the point of view of a network, the Italian university and the research environment represent an integrated system of absolute importance for our country. In particular, there appears to be an increase in strategies aimed at increasing university involvement in regional development programmes focused on health research. In fact, the Memorandum of Understanding among the Apulia Region, the University of Bari, and the University of Foggia lays the foundations for a strengthening of the processes of collaboration and integration between the university and the regional health system. The achievement of these goals requires the development of methods and tools of collaboration between the health system and the training system to pursue together, with quality, efficiency, and competitiveness, the aims related to health needs, the training of medical and health personnel, and the strengthening of biomedical and clinical research. Another aim is to ensure the inseparability and coherence between care activity and the needs of training and research. In this perspective of “regional development” and integration programmes, an agreement among the University of Bari “Aldo Moro,” the University Hospital Consortium “Polyclinic of Bari,” and the National Cancer Institute of Bari–Istituti di Ricovero e Cura a Carattere Scientifico (IRCCS) “Giovanni Paolo II” for the development of an integrated model of assistance and research was signed on October 30, 2018. The integration is requested and supported by the Regional Council as a necessary tool for the application of the priority strategic lines expressed in the assistance, training, and research sectors and sanctioned with the establishment of the Regional Oncological Network (Rete Oncologica Pugliese [ROP]) with Decree of the Regional Executive No 221 of 28 February 2017. The strong integration among these 3 institutions, in the context of the development of ROP, aims to favour the further development of the significant acquired skills and the best use of existing and functioning high-tech facilities. In particular, the objectives of this Memorandum of Intent are (1) to develop and consolidate a broader clinical case history, with positive repercussions on the teaching activity of the current degree courses and of the specialization schools in the medical health area of the University of Bari and (2) achieve professional synergies between AOUs and IRCCS, useful for strengthening territorial excellence through a partnership that focuses on resources, avoids duplication, and allows significant organizational economies.
This integration will allow IRCCS to:
(1) Effectively interpret the role of coordinator of the ROP
(2) Further implement the high quality offer (with consequent increase in turnover)
(3) Improve scientific production within the priority project of “precision medicine”
(4) Use the Institute’s Biobank and Good Manufacturing Practice laboratories at full capacity; these 2 infrastructures, which are able to favour both the development of research and the improvement of the quality of care, also represent a tool to allow more updated and more effective teaching methods
The collaboration among the 3 institutions, therefore, takes place within a specific planned framework, in which, according to the agreement, relationships and synergies can be achieved in the field of health care, health education, and research. These synergies are not simply closely connected, but allow mutual interaction and involvement. Therefore there is an emerging importance of the interaction of networks and interdependencies between universities and institutions. The integration policies alone can strengthen the synergistic action required by universities, businesses, and the public administration to face and overcome the challenge of innovation and research, through a complex process of strategic coordination. This type of integration must be included in a logic of “multilevel governance” in which the action of regional systems is integrated into a national and international strategic framework, such as that of the Organization of European Cancer Institutes, whose objective is to satisfy the request to make Europe “the most competitive and dynamic knowledge-based economy in the world.”
MOLECULAR PATHOLOGY IN AGGRESSIVE TYPE OF TUMOURS: AN INTRODUCTION
Giorgio Stanta
National Cancer Institut, Aviano, Italy
Clinical research is often used for specific aggressive tumours even in today’s patients. This type of clinical application was recently highlighted by the committees of the European Commission Initiative on Breast Cancer.
As a consequence, a network of oncology institutions with clinical research capability, such as the Comprehensive Cancer Centres with Organization of European Cancer Institutes (OECI) accreditation, has been developed in Europe.
The reproducibility of molecular analyses is not guaranteed either in diagnostics or in clinical research and the interchangeability of molecular results among clinical institutions is problematic. These analyses are particularly necessary in the aggressive type of tumours, with the aim of giving patients the best possible treatment.
To reach a sufficient level of reproducibility in oncology, it is necessary to consider at least 3 main issues: preanalytical conditions of the biological material analysed, high level of standardization of methods, and control of intratumour heterogeneity. Several initiatives have already been set up to improve the quality of molecular analyses. These are projects aimed to standardize the preanalytical conditions (SPIDIA4P project with the collaboration of CEN and BBMRI-ERIC), next-generation sequencing (NGS) at clinical level (Instand-NGS4PT, project proposal), and tissue sampling for intratumour heterogeneity (collaboration with ESP), and to implement a rapid clinical validation of biomarkers (HERCULES). OECI working groups have been already created in order to standardize liquid biopsies and NGS–whole-exome sequencing by preparation of preliminary documents. OECI is involved in all these initiatives, directly or indirectly. Bari OECI Pathology Day is organized in order to assess the need for clinical research in some types of aggressive tumours and in the second session to explore the possibility of developing clinical projects on aggressive tumours such as glioblastoma and aggressive types of paediatric cancers within the organization.
HIGH-GRADE SEROUS OVARIAN CANCER: TOWARDS IMPROVED MOLECULAR DIAGNOSTICS AND TARGETED TREATMENTS
Olli Carpén
Research Program for Systems Oncology and Medicum, University of Helsinki and Helsinki Biobank, Helsinki, Finland
High-grade serous ovarian cancer (HGSC) is the most common ovarian cancer subtype and deadliest gynaecologic malignancy. A vast majority of patients are diagnosed at advanced stage, when the disease has metastasized to peritoneal cavity or beyond. Patients are treated by surgery, when possible, either before chemotherapy (primary debulking surgery) or after neoadjuvant therapy (interval debulking surgery). The standard chemotherapy regimen includes platinum-taxane combination. Typically, after initial complete response, the disease relapses within 12 to 18 months,1 and gradually becomes refractory to treatments. The current 5-year overall survival probability is below 30%. To improve the outcome of HGSC, there are at least 3 options: (1) develop methods for earlier detection, (2) improve stratification of patients based on molecular features for optimal treatment, and (3) apply methods to monitor the evolution of the disease and identify targeted changes at a stage when the disease becomes resistant to the currently used therapy.
The most commonly used methods for HGSC detection are imaging, either ultrasound or computed tomography, and blood-based cancer biomarkers, especially CA-125 and HE4. There is some evidence that longitudinal CA-125 measurements of healthy women, combined with vaginal ultrasound aid detection of ovarian cancer at an earlier stage, may lead to improved survival.2 The challenge with CA-125 is its relative nonspecificity: elevated CA-125 values are commonly detected in benign conditions, including endometriosis and benign ovarian neoplasms. Recently, promising results have been obtained with a CA-125 test that distinguishes cancer-specific CA-125 and CA-125 from benign sources. The test combines conventional CA-125 measurement with analysis of its glycan structures, which differ depending on whether CA-125 is produced by benign or malignant cells.3
Outcome-associated biomarker identification in HGSC is especially challenging due to the complex genomic alterations characterizing this disease. The only characteristic alteration is inactivation of P53 and the absence of the common oncogenic mutations.4 Homologous recombination (HR) DNA repair deficiency is a common feature in HGSC (seen in about half of the patients) and indicates response to standard chemotherapy and novel PARP inhibitors (PARPi).5 In 10% to 15% of patients, the HR deficiency is a result of inherited or somatic mutation of BRCA1 or BRCA2 gene. Importantly, a recent phase III trial demonstrated that PARPi first-line maintenance therapy, in combination with the conventional platinum-taxane treatment, provides substantial benefit for BRCA-mutated ovarian cancer with an impressive 70% reduced risk of disease progression or death within 41 months.6 It remains to be seen whether a similar benefit is acquired in patients whose HR deficiency is acquired by other mechanisms, including mutations in other genes of the same HR pathway, BRCA1 methylation, or other epigenetic mechanisms.
In the clinical setting, BRCA1/BRCA2 profiling of HGSC tumours is a common practice, but it is far from adequate for predicting platinum sensitivity. There are alternative promising methods to probe HR deficiency, including analysis of mutational signatures by whole genome sequencing,7 analysis of ovarian cancer organoid cultures,8 or HR testing in ovarian cancer primary cell cultures.9 It remains to be seen, whether any of these methods will be useful in future diagnostic practice.
There is compelling evidence that cellular heterogeneity within a tumour is highly determinant for drug resistance, cancer progression, and a prerequisite for the presence of cancer stem cells.10 Therefore, it is easy to understand that the conventional single biomarker approach is unlikely to provide sufficient information for prognostication, especially in a complex cancer like HGSC. With recently introduced multiplexed immunohistochemistry and digital imaging techniques it will be possible to profile tens of markers simultaneously and capture the spatial arrangement and functional state of cancer cells,11 and thereby improve biomarker discovery. This approach may prove to be extremely useful for identification of a biomarker set for HGSC patient stratification and for targeted treatment decisions.
The search for (tissue) biomarkers that reflect tumor biology are critically dependent on the quality of the patient cohorts. In HGSC, the outcome is heavily dependent on the stage of disease at diagnosis, surgery end result (whether or not all visible tumour was successfully removed, R = 0), and whether the patient had primary or interval debulking surgery. In our own cohort of over 900 patients, those with optimal primary debulking result (R = 0) have over 40% higher 5-year survival probability than patients with suboptimal debulking result (R > 0). Also, the survival of primarily debulked individuals was significantly better than of the patients undergoing interval debulking. If the type of surgery and surgery end result is neglected in biomarker discovery projects, it is likely that the biomarkers will not indicate biological variables. Similarly, the stage of disease (dissemination) at diagnosis, execution of chemotherapy regimens, performance status, and comorbidities play an important role in outcome and therefore these clinical variables need to be taken into account in the generation of research cohorts. Figure 1 shows disease trajectories of 3 patients with similar clinical presentation and treatments but very different overall survival time ranging from 505 to over 3000 days. It is likely that in this example the biology of the tumours plays an important role in the outcome. To conclude, an approach that combines carefully curated tumour specimens with comprehensive clinical information, novel biomarker discovery platforms, and computational methods is needed to understand the biology of HGSC and to develop methods for stratifying patients to targeted treatments and optimal selection of drug combination.
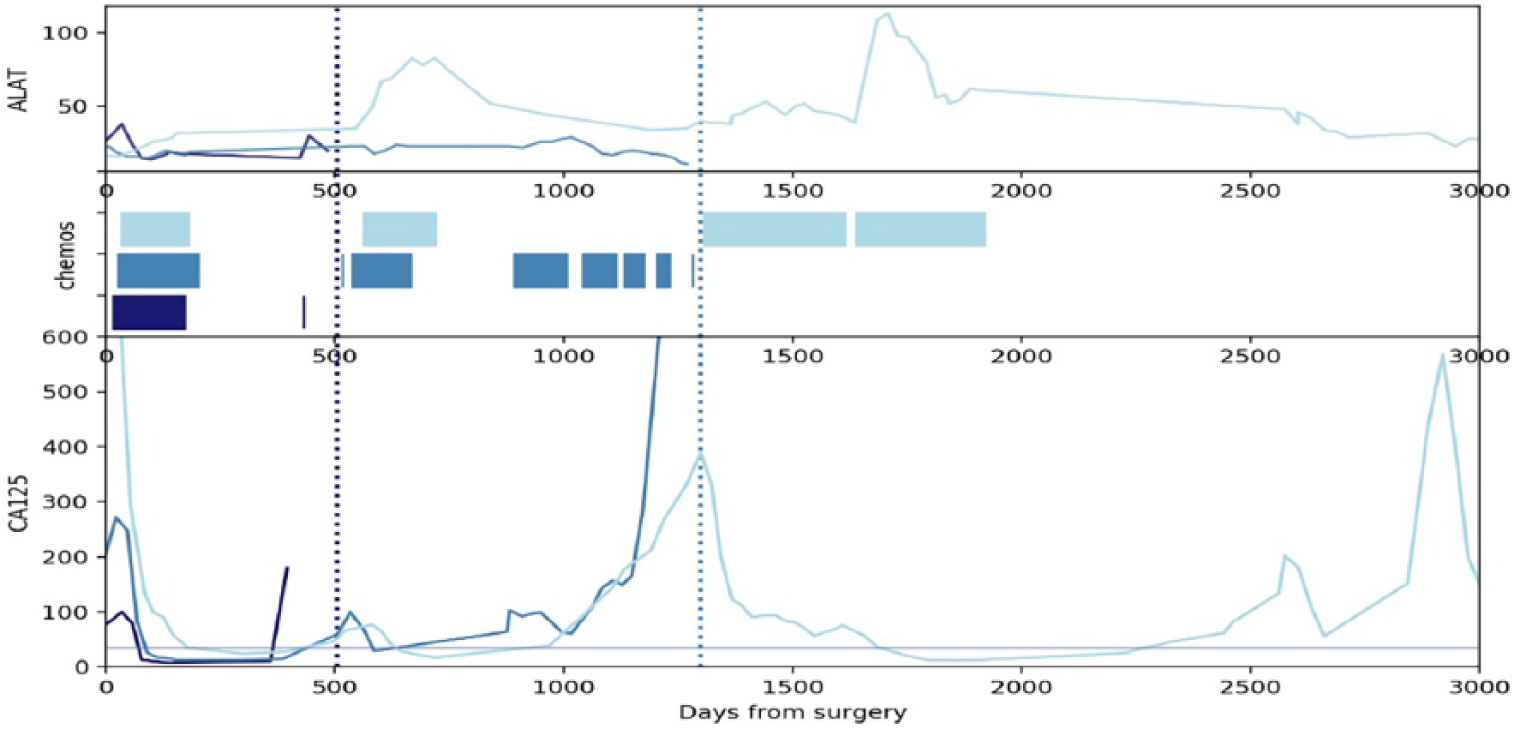
Disease trajectories of 3 individual HGSC patients with similar presentation but different outcome. All patients were of same age category and had similar performance status (ASA2). The disease stage at diagnosis was IIIC. All patients underwent primary debulking surgery with optimal result (R0, no visible tumour left), followed by standard 6 cycles of platinum-taxane chemotherapy. All patients were biochemically at remission following chemotherapy (CA-125 <35 IU/mL). One of the patients (dark blue) had a platinum-free interval <6 months, and was therefore regarded as platinum resistant. She died shortly after initiation of the second round of chemotherapy (survival 505 days, marked by left pointed line). The second patient (medium blue) relapsed 520 days after diagnosis. She had a short response to a second round of platinum-taxane, but upon progression, she received 3 alternative chemotherapy regimens without clinical benefit. She survived 1320 days (right pointed line). The third patient (light blue) relapsed 540 days after diagnosis, but responded well to a second round of platinum-taxane. She relapsed again 1000 days after diagnosis, and received a third round of platinum-taxane followed by a second chemotherapy regimen. While her CA-125 values are fluctuating, she is alive 3000 days after diagnosis. Elevated alanine aminotransferase values during chemotherapy suggest liver toxicity. Courtesy of Jani Salmi, University of Helsinki and Helsinki biobank.
The third strategy to improve HGSC outcome involves monitoring of cancer evolution during treatments. During disease surveillance, it is not sufficient to just detect a relapse, but one needs to understand the molecular changes that may be encountered at the relapse stage. Especially, as relapses typically are refractory to platinum-taxane combination, we should be able to profile the genomic changes and whether they would open up possibilities for alternative therapeutic approaches. Currently, the most likely option for disease monitoring involves longitudinal cell-free DNA analysis. In my presentation, I present recent studies in which this technique has been successfully tested in HGSC for the first time.
Vaughan S, Coward JI, Bast RC Jr, et al. Rethinking ovarian cancer: recommendations for improving outcomes. Nat Rev Cancer 2011; 11: 719–725.
Jacobs IJ, Menon U, Ryan A, et al. Ovarian cancer screening and mortality in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): a randomised controlled trial. Lancet 2016; 387: 945–956.
Gidwani K, Huhtinen K, Kekki H, et al. A nanoparticle-lectin immunoassay improves discrimination of serum CA125 from malignant and benign sources. Clin Chem 2016; 62: 1390–400.
Bell D, Berchuck A, Birrer M, et al. Integrated genomic analyses of ovarian carcinoma. Cancer Genome Atlas Research Network. Nature 2011; 474: 609–615.
Mirza MR, Pignata S, Ledermann JA, et al. Latest clinical evidence and further development of PARP inhibitors in ovarian cancer. Ann Oncol 2018; 29: 1366–1376.
Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med 2018; 379: 2495-2505.
Davies H, Glodzik D, Morganella S, et al. HR Detect is a predictor of BRCA1 and BRCA2 deficiency based on mutational signatures. Nat Med 2017; 23: 517–525.
Hill SJ, Decker B, Roberts EA, et al. Prediction of DNA repair inhibitor response in short term patient-derived ovarian cancer organoids. Cancer Discov 2018; 8: 1404–1421.
Tumiati M, Hietanen S, Hynninen J, et al. A functional homologous recombination assay predicts primary chemotherapy response and long-term survival in ovarian cancer patients. Clin Cancer Res 2018; 24: 4482–4493.
Tammela T, Sanchez-Rivera FJ, Cetinbas NM, et al. A Wnt-producing niche drives proliferative potential and progression in lung adenocarcinoma. Nature 2017; 545: 355–359.
Blom S, Paavolainen L, Bychkov D, et al. Systems pathology by multiplexed immunohistochemistry and whole-slide digital image analysis. Sci Rep 2017; 7: 15580.
LUNG CANCER MOLECULAR EVALUATION
Reinhard Buettner
Institute of Pathology and Centre for Integrated Oncology, University of Cologne Medical Centre, Germany
Current state of lung cancer molecular testing for stratifying therapies: Lung cancer serves as a paradigm for biomarker testing in molecular pathology as practically all therapeutic decisions on first- or second-line therapies depend on molecular analyses of tumour biopsies (summaries in Figure 1). This approach has totally changed oncologic landscapes as 10 years ago practically all patients received upfront combined chemotherapies with the exception of patients with EGFR-mutant lung adenocarcinomas.1 With the foreseeable advent of combined IO therapies in first-line therapies, the landscape will change again into a situation where the vast majority of patients will not receive any chemotherapy at all as first-line therapy.
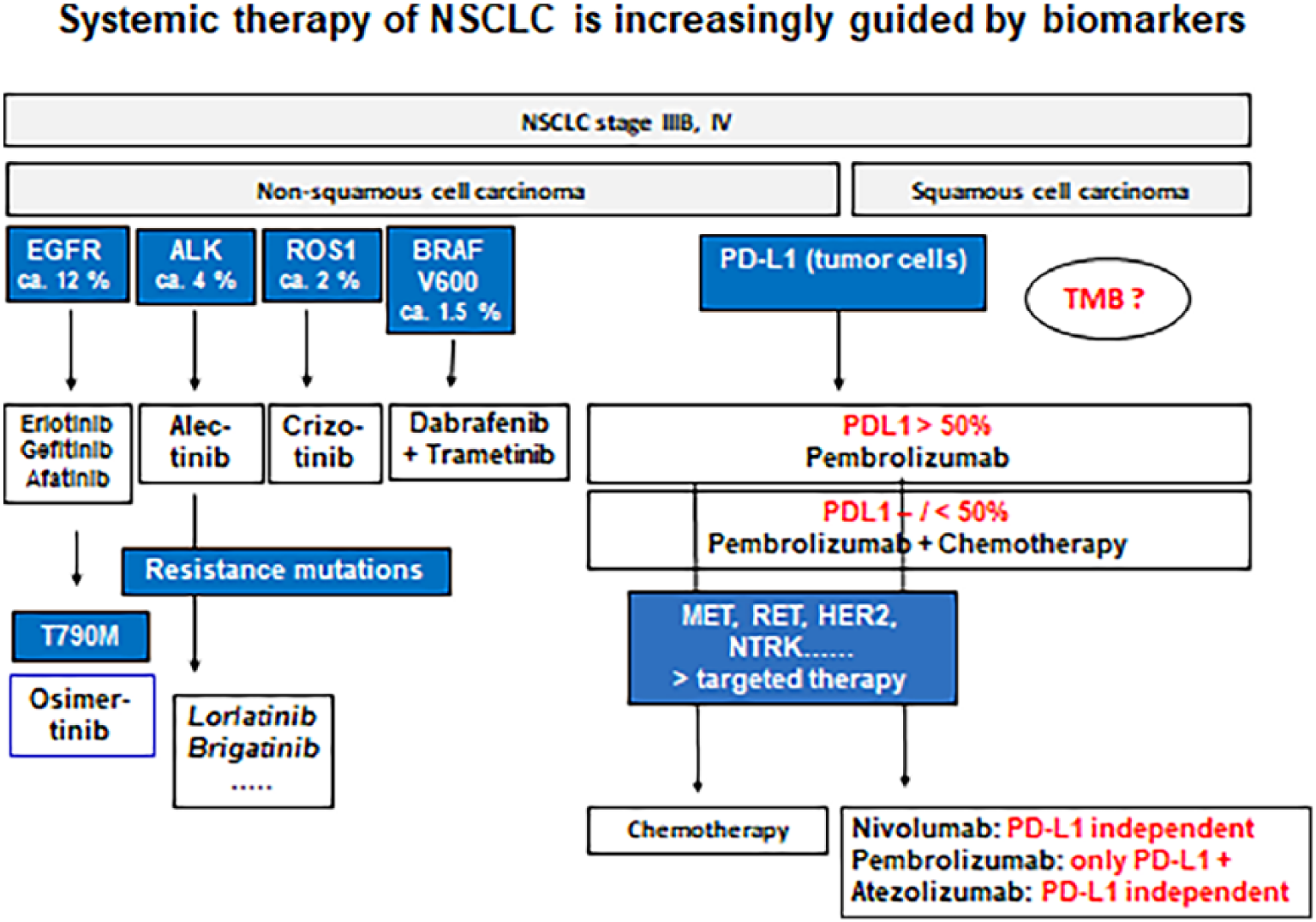
Biomarker-guided therapy lines on non-small cell lung cancers (NSCLC) according to European Medicines Agency approvals or inclusion into current clinical trials.
In contrast, the clinical practice of testing lung cancer patients did not cope with the development.2 Systematic data obtained from the CRISP registry reveal that a significant portion of patients are not being tested for important molecular parameters before initiation of first-line therapy. Hence, thousands of patient-life years and years with better quality of life are being wasted, despite a massive increase in therapy costs.3 Therefore, the Cologne Lung Cancer Group initiated the National Genomic Medicine (NGM) Lung Cancer, supported by the German Cancer Aid to change current test and treatment practice aiming at a deep coverage of all regions within Germany.
Implementation of the NGM: The focus of NGM is on the implementation of innovative molecular diagnostics and personalized therapy as a general practice in clinical routine in Germany. This is enabled by an ongoing development of diagnostics of molecular pathology within the network centres, interdisciplinary counselling of referring partner sites, offering innovative clinical trials and central evaluation. In particular, a focus of NGM is on the development of regional networks to treat the patients with lung cancer close to their homes, using for that the partner sites whenever it is possible. As treatment individualization becomes more complex, depending on the diagnostic results, clinical care networks will be essential to facilitate rapid innovation transfer and development of new individualized treatment approaches in clinical trials.
Important clinical research questions remaining within the scope of NGM include prediction of therapy response to rare EGFR mutations, mechanisms of therapy resistance in translocation-positive lung cancers with p53 mutation, implementing predictive algorithms for immune oncology (PredictImmune), analysis of pan-negative tumours, and early prevention of acquired therapy resistance.4,5 Another important issue is to evaluate best practices for monitoring patients under therapy.
A genomics-based classification of human lung tumours. Sci Transl Med 2013; 5: 209ra153.
Nowak F, Calvo F, Soria JC. Europe does it better: molecular testing across a national health care system: the French example. Am Soc Clin Oncol Educ Book 2013; 332–337.
Griesinger F, Eberhardt WEE, Nusch A, et al. Molecular testing, frequency of molecular alterations and targeted 1st-line treatment of patients with non-small cell lung carcinoma in Germany: first results from the prospective German Registry CRISP (AIO-TRK-0315). JCO 2018; 36: e21236.
Alidousty C, Baar T, Martelotto LG, et al. Genetic instability and recurrent MYC amplification in ALK-translocated NSCLC: a central role of TP53 mutations. J Pathol 2018; 246: 67–76.
Kron A, Alidousty C, Scheffler M, et al. Impact of TP53 mutation status on systemic treatment outcome in ALK-rearranged non-small-cell lung cancer. Ann Oncol 2018; 29: 2068–2075.
MOLECULAR PATHOLOGY OF MALIGNANT GLIOMAS
Dominique Figarella-Branger
Marseille Public University Hospital System (AP-HM) and Aix-Marseille University, French National Centre for Scientific Research CNRS, the Institute of NeuroPhysiopathology (INP), Marseille, France
Gliomas are characterized by 2 patterns of infiltration: diffuse and circumscribed. Circumscribed gliomas are usually benign and in most cases, total surgical excision is curative. In contrast, diffuse gliomas are usually highly infiltrative and they always evolve towards higher grade of malignancy (from grade II to grade III then IV). Importantly, diffuse gliomas are characterized by genetic alterations that are clearly distinct in adult versus paediatric (adolescent) patients.1,2 The updated 4th edition of the WHO Classification of Tumours of the Central Nervous System (2016) is based on evidence that incorporation of biomarkers into an integrated diagnosis provides a more reproducible and clinically meaningful classification than histopathologic features alone.3,4 According to this classification, diffuse adult gliomas are stratified according to the presence or absence of 2 main genetic alterations: IDH mutation and 1p/19q codeletion. The IDH-mutant diffuse gliomas include diffuse astrocytoma, IDH-mutant (WHO grade II), anaplastic astrocytoma, IDH-mutant (WHO grade III), glioblastoma, IDH-mutant (WHO grade IV), oligodendroglioma, IDH-mutant, 1p/19q-codeleted (WHO grade II), anaplastic oligodendroglioma, IDH-mutant, and 1p/19q-codeleted (WHO grade III). IDH-wild-type diffuse astrocytic gliomas are now recognized as distinct clinical and genetic entities that generally have much more aggressive clinical behaviour than the IDH-mutant diffuse glioma. Although most of them demonstrate pathologic features of glioblastomas including microvascular proliferation and necrosis and are therefore classified as glioblastoma, IDH-mutant (WHO grade IV) and others mimic on pathologic examination WHO grade II or III astrocytomas. In these cases, however, the Consortium to Inform Molecular and Practical Approaches to CNS Tumour Taxonomy–Not Official WHO (c-IMPACT-NOW) has recently addressed the grading of these gliomas, concluding that an IDH-wild-type diffuse glioma with EGFR amplification, TERT promoter mutations, or the combination of gain of chromosome 7 and loss of chromosome 10 could be considered “diffuse astrocytic glioma with molecular features of glioblastoma, WHO grade IV.”5,6 This points to some major genetic alterations occurring in glioblastoma, IDH-mutant (WHO grade IV), i.e. EGFR amplification, TERT promoter mutations, or the combination of gain of chromosome 7 and loss of chromosome 10.7,8 In addition, other genetic alterations have been recorded by the TCGA as well as methylation profiling.7,9 Other molecular markers such as CDKN2A/B homozygous deletion are of prognostic value in some subsets of IDH-mutated gliomas.10,11
This histomolecular classification is of utmost importance since it is predictive of the prognosis.12–14 Besides, few genetic alterations are predictive of treatment response. In this context, MGMT promoter methylation remains the major alteration to be analysed, although the technical approaches may vary from one centre to another.15,16 Other alterations such as FGFR3-TACC fusion represent druggable targets.17,18
In contrast, paediatric gliomas lack IDH mutation and most of them, especially diffuse midline gliomas, are characterized by histone mutations.1,2 Because of the dismal prognosis of the diffuse midline gliomas, they are now recognized in the 2016 WHO classification as “diffuse midline glioma, H3K27M-mutant, grade IV” and therefore regardless of pathologic features. Recent studies have highlighted the distinct genetic features of paediatric gliomas.19,20
To conclude, malignant gliomas are characterized by several genetic alterations that are differentially observed in adult versus paediatric population. The occurrence of selected molecular alterations are of utmost value for the diagnosis of these tumours but also predictive of the treatment response or druggability prediction.
Wu G, Broniscer A, McEachron TA, et al. Somatic histone H3 alterations in pediatric diffuse intrinsic pontine gliomas and non-brainstem glioblastomas. Nat Genet 2012; 44: 251–253.
Schwartzentruber J, Korshunov A, Liu XY, et al. Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma. Nature 2012; 482: 226–231.
Louis DN, Perry A, Burger P, et al. International Society of Neuropathology: Haarlem consensus guidelines for nervous system tumor classification and grading. Brain Pathol 2014; 24: 429–435.
Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 2016; 131: 803–820.
Louis DN, Aldape K, Brat DJ, et al. Announcing cIMPACT-NOW: the Consortium to Inform Molecular and Practical Approaches to CNS Tumor Taxonomy. Acta Neuropathol 2017; 133: 1–3.
Brat DJ, Aldape K, Colman H, et al. cIMPACT-NOW update 3: recommended diagnostic criteria for “Diffuse astrocytic glioma, IDH-wildtype, with molecular features of glioblastoma, WHO grade IV.” Acta Neuropathol 2018; 136: 805–810.
Verhaak RG, Hoadley KA, Purdom E, et al. Cancer Genome Atlas Research Network: Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell 2010; 17: 98–110.
Eckel-Passow JE, Lachance DH, Molinaro AM, et al. Glioma groups based on 1p/19q, IDH, and TERT promoter mutations in tumours. N Engl J Med 2015; 372: 2499–2508.
Sturm D, Witt H, Hovestadt V, et al. Hotspot mutations in H3F3A and IDH1 define distinct epigenetic and biological subgroups of glioblastoma. Cancer Cell 2012; 22: 425–437.
Shirahata M, Ono T, Stichel D, et al. Novel, improved grading system(s) for IDH-mutant astrocytic gliomas. Acta Neuropathol 2018; 136: 153–166.
Reis GF, Pekmezci M, Hansen HM, et al. CDKN2A loss is associated with shortened overall survival in lower-grade (World Health Organization Grades II-III) astrocytomas. J Neuropathol Exp Neurol 2015; 74: 442–452.
Cancer Genome Atlas Research Network, Brat DJ, Verhaak RG, et al. Comprehensive, integrative genomic analysis of diffuse lower-grade gliomas. N Engl J Med 2015; 372: 2481–2498.
Suzuki H, Aoki K, Chiba K, et al. Mutational landscape and clonal architecture in grade II and III gliomas. Nat Genet 2015; 47: 458–468.
Tabouret E, Nguyen AT, Dehais C, et al. For POLA Network. Prognostic impact of the 2016 WHO classification of diffuse gliomas in the French POLA cohort. Acta Neuropathol 2016; 132: 625–634.
Hegi ME, Diserens AC, Gorlia T, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med 2005; 352: 997–1003.
Quillien V, Lavenu A, Karayan-Tapon L, et al. Comparative assessment of 5 methods (methylation-specific polymerase chain reaction, MethyLight, pyrosequencing, methylation-sensitive high-resolution melting, and immunohistochemistry) to analyze O6-methylguanine-DNA-methyltranferase in a series of 100 glioblastoma patients. Cancer 2012; 118: 4201–4211.
Di Stefano AL, Fucci A, Frattini V, et al. Detection, characterization, and inhibition of FGFR-TACC fusions in IDH wild-type glioma. Clin Cancer Res 2015; 21: 3307–3317.
Singh D, Chan JM, Zoppoli P, et al. Transforming fusions of FGFR and TACC genes in human glioblastoma. Science 2012; 337: 1231–1235.
Mackay A, Burford A, Molinari V, et al. Molecular, pathological, radiological, and immune profiling of non-brainstem pediatric high-grade glioma from the HERBY phase II randomized trial. Cancer Cell 2018; 33: 829–842.
Korshunov A, Ryzhova M, Hovestadt V, et al. Integrated analysis of pediatric glioblastoma reveals a subset of biologically favorable tumours with associated molecular prognostic markers. Acta Neuropathol 2015; 129: 669–678.
THE EUROPEAN COMMISSION INITIATIVE ON BREAST CANCER
Luciana Neamţiu
European Commission–Joint Research Centre
In Europe, breast cancer is the most common diagnosed cancer and the leading cause of cancer death in women. It is estimated that in 2018, more than 400,000 new cases were diagnosed, accounting for 28% of all new female cases. In the same year, 131,000 women were estimated to die from breast cancer, accounting for 17% of all female cancer deaths in Europe and making it the most common cause of female cancer death.
The incidence of breast cancer is continuously increasing in almost all European countries, while mortality rates are decreasing in many countries. Five-year survival of women with breast cancer is 82%, with variations from 87% to 66%, indicating possible inequalities in breast cancer care for European women.1
To tackle any relevant discrepancies in the quality of care among member states, the European Commission has launched the European Commission Initiative on Breast Cancer (ECIBC). The ECIBC aims to ensure and harmonise the quality of breast cancer services across European countries.
The ECIBC has 2 main areas of activity:
Establishing a European quality assurance (QA) scheme for breast cancer: a voluntary European QA scheme for breast cancer services that addresses all care processes, including screening, diagnosis, treatment, rehabilitation, follow-up and survivorship, and end-of-life care (Figure 1).
Developing evidence-based recommendations to support the European QA scheme: the European guidelines for breast cancer screening and diagnosis (European Breast Guidelines); to support the QA scheme for the processes of care from treatment to end of life, a platform of guidelines collecting the existing evidence-based guidelines covering all other breast care processes is set up.
Developing evidence-based recommendations to support the European QA scheme: the European guidelines for breast cancer screening and diagnosis (European Breast Guidelines); to support the QA scheme for the processes of care from treatment to end of life, a platform of guidelines collecting the existing evidence-based guidelines covering all other breast care processes was set up.
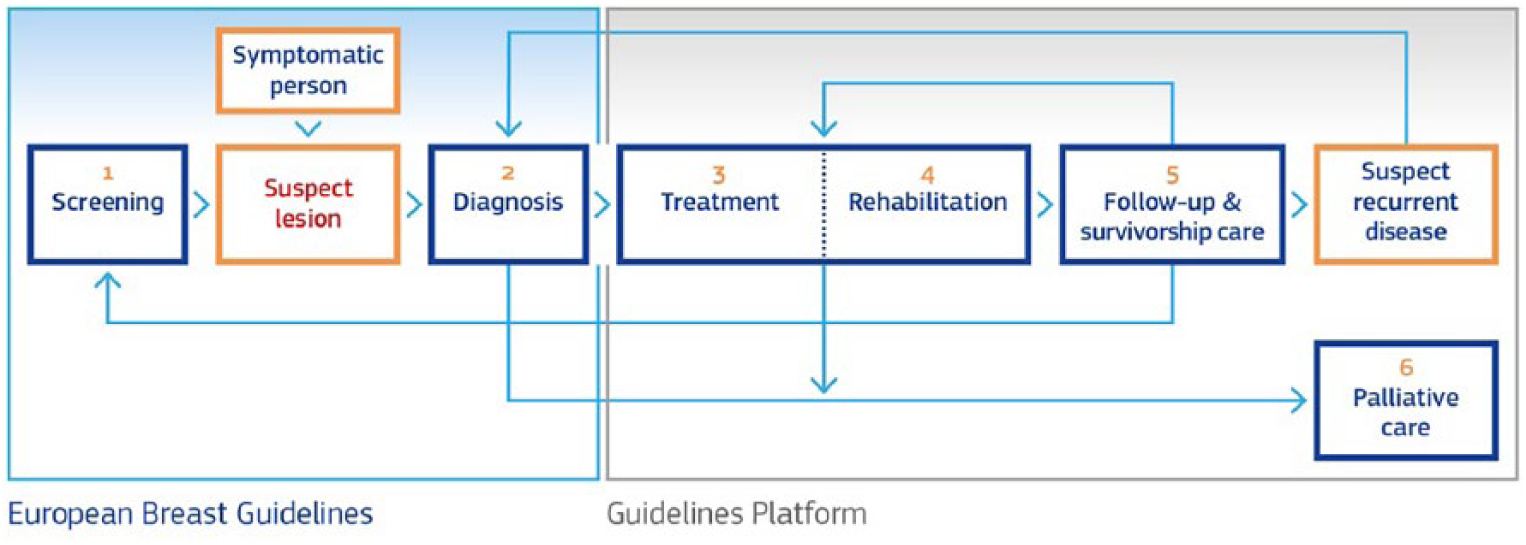
Breast cancer care pathway covered by the QA Scheme.
The QA Scheme: Experts selected through public open calls support the JRC to develop the ECIBC: the Guidelines Development Group (GDG) and the Quality Assurance Scheme Development Group (QASDG). Both groups include professionals with a wide range of expertise as well as patients. Conflicts of interest of the GDG and QASDG members are assessed and managed accordingly. The European Breast QA Scheme is a collection of requirements and indicators, focused on the person’s needs and based on evidence-based guidelines. The scheme is designed to be implemented on a voluntary basis by services in need and to improve their quality of care. Breast cancer services fulfilling the requirements will be certified. The development of the QA scheme is supported by the QASDG. Its main steps are as follows: definition of the scope of the scheme, development of the requirements and indicators, and piloting of the scheme. First, the QASDG has defined the care pathway for breast cancer screening and care. Based on this care pathway, the QASDG has drafted the scope of the QA scheme, a document containing the interventions and services that are covered by the European QA Scheme, the dimension of quality that will be included and how the scheme can be implemented in Europe. The scope was amended after a public call for feedback where stakeholders were invited to provide their opinions.2
To develop the requirements and indicators, a literature search (including indicators’ databases, guidelines, and quality assurance schemes) was done and the requirements/indicators for all breast cancer care processes were retrieved. These are then rated for feasibility and relevance in Delphi-like rounds by the QASDG until a final selection of requirements and indicators is established. See Methodology.3
To date, the requirements for treatment, rehabilitation, follow-up, and survivorship care, as well as for palliative care, have been finalised and are approved. The QASDG is still working on the requirements/indicators for screening, diagnosis, and training of professionals. The concept of the manual for breast cancer services has been defined as well. The manual includes a classification of the requirements that follows 4 quality domains: (1) clinical effectiveness, (2) facilities, resources, and workforce, (3) personal empowerment and experience, and (4) safety. The manual will help services that wish to be certified according to ECIBC to prepare for the certification. A software tool to help breast cancer services seeking certification with computation of the indicators is being developed by the JRC. Before the full implementation of the scheme, a pilot test will be conducted.
Acknowledgements
The QASDG members are listed in https://ecibc.jrc.ec.europa.eu/qa-team. The authors thank current and former JRC colleagues (Massimo Ambrosio, Giulia Bocchi, Anke Bramesfeld, Silvia Deandrea, Nadya Dimitrova, Marta Garcia-Escribano, Grazia Federico, Annett Janusch-Roi, Donata Lerda, Ciaran Nicholl, Sazan Pakalin, Elena Parmelli, Liisa Pylkkanen, Zuleika Saz-Parkinson, Beatriz Torighelli, and Asli Uluturk) as well as additional external colleagues (https://ecibc.jrc.ec.europa.eu/contractors).
European Union. European Cancer Information System, https://ecis.jrc.ec.europa.eu (2019, accessed 12 March 2019).
Deandrea S, Neamțiu L, Ambrosio M, et al. Report on the Call for Feedback About the Scope of the European Quality Assurance Scheme for Breast Cancer Services. Luxembourg: Publications Office of the European Union; 2016.
Methods of the Voluntary European Quality Assurance Scheme for Breast Cancer Services: Selection of requirements and indicators, https://ecibc.jrc.ec.europa.eu/-/methods-of-the-voluntary-european-quality-assurance-scheme-for-breast-cancer-services (accessed on 12 March 2019).
ALLIANCE AGAINST CANCER BIOBANKING SYSTEM
Angelo V. Paradiso1, Mariagrazia Daidone2, Barbara Parodi3, Anna Sapino4, Gerardo Botti5
1National Cancer Institute–IRCCS “G Paolo II,” Bari, 2National Cancer Institute–“Fondazione IRCCS,” Milan, 3Cancer Polyclinic Hospital–IRCCS “San Martino,” Genoa, 4Cancer Institute–IRCCS Candiolo, Turin, 5National Cancer Institute–IRCCS “G. Pascale,” Naples, Italy
Alliance Against Cancer (Alleanza Contro il Cancro) (ACC) is the largest Italian organization for cancer research, established in 2002 by the Italian Ministry of Health. ACC represents a network of high standard institutes such as scientific institutes for research, hospitalisation, and health care (Istituti di Ricovero e Cura a Carattere Scientifico [IRCCS]) for comprehensive cancer patient care and research. The ACC currently consists of 25 scientific institutes of hospitalization and care, the Italian Association for Cancer patients (AIMaC), Italian Sarcoma Group, the National Centre of Oncological Hadrontherapy (CNAO), and the Higher Institute of Health (ISS), which houses the offices. The primary aim of ACC is to promote the network among cancer institutes in order to pursue clinical and translational research and bring state-of-the-art diagnostics and advanced therapeutics to patient care. ACC can apply for national/international research funds and collaborate in the development of clinical research in the field of cancer implementing results, co-developing cancer drugs, or diagnostic procedures. ACC may request national/international research funds and collaborate in the development of clinical research in the field of cancer outcome implementation and co-develop anticancer drugs or diagnostic procedures.
Eight working groups are active in the ACC, dealing with the main types of cancer (cancer of the colon, breast, lung, glioblastoma, melanoma, and sarcoma) and clinical research (genomics and immunotherapy). These are collaborative groups formed by the best national reference experts who are in charge of planning clinical research and optimizing the use of new drugs for each individual tumour pathology. Main activities of all these working groups is the identification of new risk-predictive biomarkers, prognosis, drug response and their toxicity, together with the development of molecular targeting drugs and innovative bioimaging techniques. These lines of research are all based on the availability of biological material from patients and subjects at risk, in order to study biomorphologic, biomolecular, and genetic characteristics, to correlate with the development of the disease and its treatment. The development of all these goals requires a strong and standardized morphologic analysis of the tissues by the pathologist and the availability of biological tissue, necessary for recent and extremely sensitive innovative technological tools. Thus the ACC has recently activated a pathology working group, led by Gerardo Botti (National Cancer Institute “G. Pascale” in Naples) and Anna Sapino (IRCCS in Candiolo), with the purpose of coordinating the activities of pathology units and standardizing the procedures for tissue biobanking in the framework of ACC network projects. The strategy of the working group aims at (1) deep involvement of the pathology services in planning of future research activities of ACC; and (2) adopting uniform high-quality biobanking activity standards concerning biospecimen collection, storage conditions, and data handling. The recently established Pathology & Biobanking Working Group (P&B-WG) first focused its attention on analytical validation of laboratory procedure for DNA/RNA extraction from formalin-fixed paraffin-embedded (FFPE) samples. The aim of the so-called RING trial is to analyse FFPE tissue and haematoxylin & eosin staining (to assess cellularity) in order to proceed with DNA and RNA extraction. The plan is to involve in the project 30 participating centres, 6 groups of 5 participants and 1 reference centre. Overall, data from 150 experiments (5 centres × 5 rounds × 6 groups) including extraction and evaluation of quality material will be performed. It is expected that 5 cycles (1 per month) will evaluate (1) extraction reproducibility in relation to the reference centre (centre 6) and to the other centres; and (2) reproducibility of nucleic acid and quality/quantity of the individual centres in the various cycles (consistency of the result). A second phase of P&B-WG activities will address specifically the cryopreservation procedures in tissue biobanking. For these activities, the ACC network will conduct its program in close connection with the Italian Node of European Biobanking and Biomolecular Resources Research Infrastructure (BBMRI).1 Most ACC institutes have their biobank facilities included in BBMRI. The Italian network, coordinated by M.L. Lavitrano (Univerità Milan Bicocca), counts more than 80 biobanks within Italy. In specific, all biobanks of IRCCS cancer institutes of ACC collaborate with BBMRI.it. In addition, the BBMRI.IT network includes a dozen biobanks from other members of the ACC (Figure 1). Finally, 3 members of P&B-WG of ACC (A.V.P., M.D., B.P.) are also active and long-standing members of the national committee of BBMRI Italia. BBMRI Italia has already produced standard materials for biobanks and biological resource centres, together with a directory of Italian biobanks included in the BBMRI-ERIC Directory.2 For the P&B-WG programs of ACC, it will be important to use all the work and documents that BBMRI.it made available and all the scientific connections that have already been established with international entities involved in biobanking. By establishing biobanks, ACC represents the cutting edge of biobanking activities in Italy and will take part in this cooperation by implementing a new way of working (Figure 2) based on global collaboration, availability of relevant associated data, and the ability to put together ad hoc3 and large cohorts of samples as well for rare disease conditions.
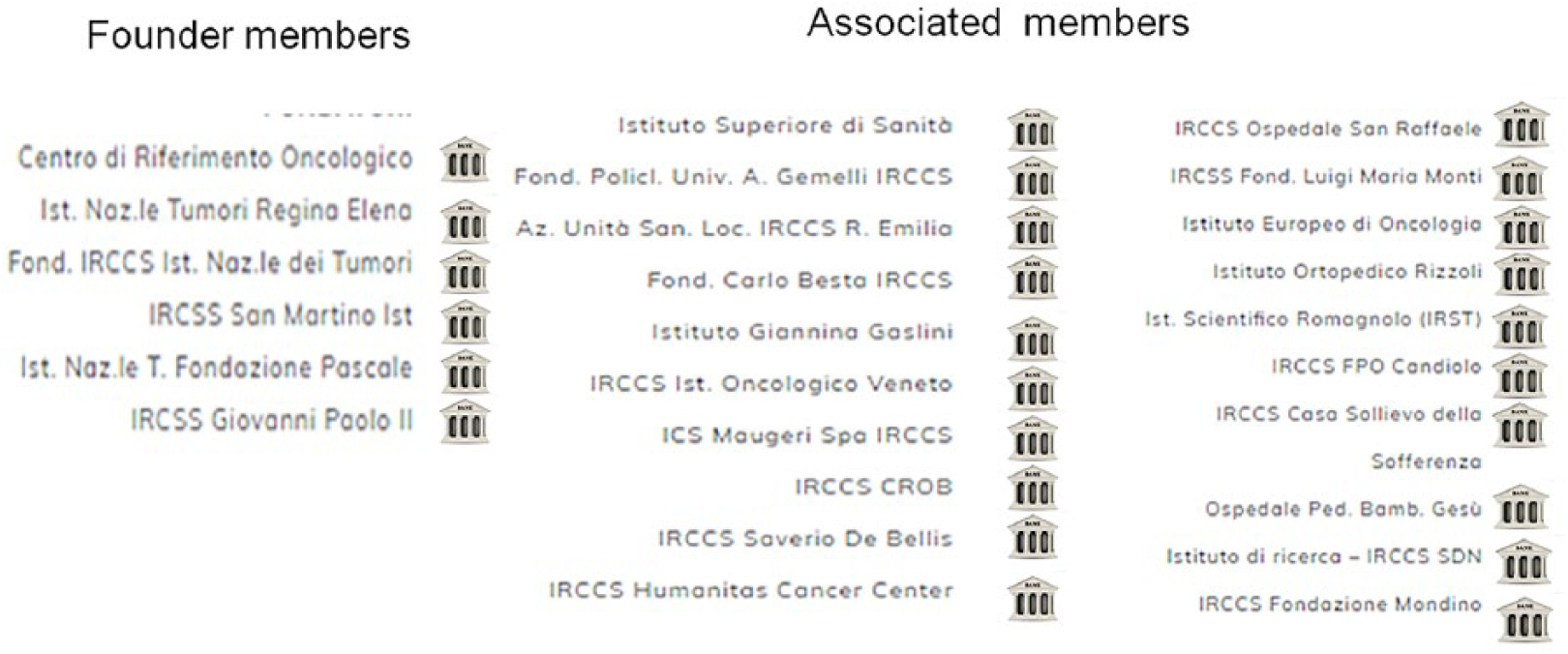
List of ACC members with biobank structures registered in BMRI catalogue.
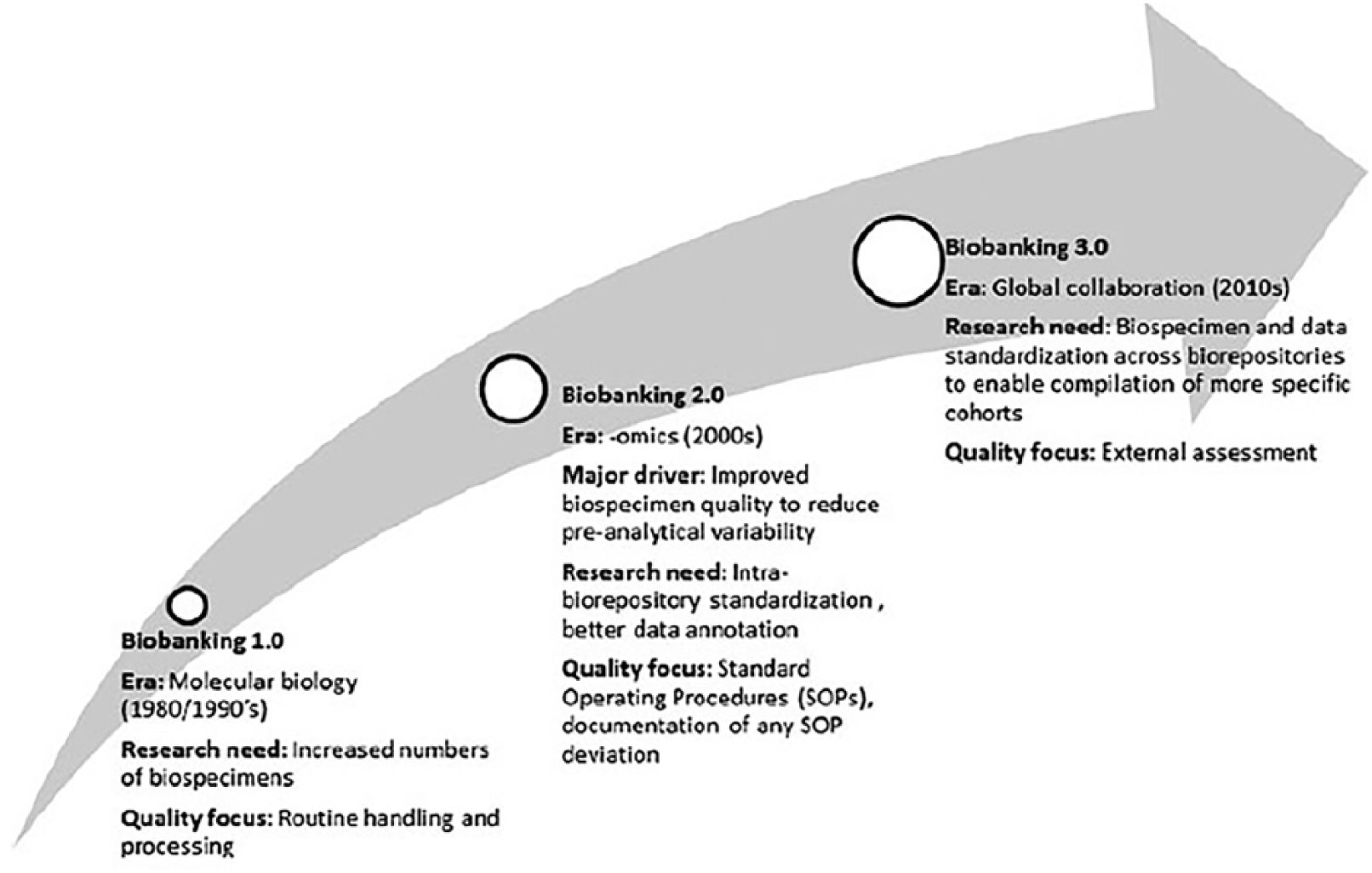
The evolution of human research biorepositories: from molecular biology to omics and then to global collaboration (modified from Barnes et al, 2017).
Calzolari A, Valerio A, Capone F, et al. The European Research Infrastructures of the ESFRI Roadmap in Biological and Medical Sciences: status and perspectives. Ann Ist Super Sanita 2014; 50: 178–185.
Holub P, Swertz M, Reihs R, et al. BBMRI-ERIC Directory: 515 Biobanks with over 60 million biological samples. Biopreserv Biobank 2016; 14: 559–562.
Paradiso AV, Daidone MG, Canzonieri V, et al. Biobanks and scientists: supply and demand. J Transl Med 2018; 16: 136.
ALLIANCE AGAINST CANCER (ALLEANZA CONTRO IL CANCRO [ACC]): WORKING GROUPS ACTIVITIES AND PRELIMINARY RESULTS
Marco G. Paggi1*, Rita Falcioni1*, Ruggero De Maria2, Pier Giuseppe Pelicci3†, Gennaro Ciliberto1†
1IRCCS–Regina Elena National Cancer Institute, Rome, 2IRCCS–Foundation Policlinico Universitario “A. Gemelli,” Rome, 3IRCCS–European Institute of Oncology, Milan, Italy
*These authors contributed equally to this work as co–first authors. $These authors contributed equally to this work as co–last authors.
Alliance Against Cancer (Alleanza Contro il Cancro [ACC]), the Italian network of cancer institutes, is institutionally devoted to sustain translational and clinical cancer research. ACC is committed to swiftly steer all cancer-related scientific and clinical knowledge towards better and more efficient patient care. To this end, ACC has established several working groups (WG) that focus on the most relevant cancer types. Each group is composed of experimental, translational, and clinical experts, focusing their efforts on actively sustaining cancer patient diagnosis, prognosis, and therapy. Currently, the mainstream of WG activities is the genomic characterization of tumours, which offers a large number of opportunities in clinical applications. In fact, ACC aims to strengthen and improve the role of high-quality personalized medicine in Italian oncology, generating a more efficient approach to the patient in order to provide new and significant prospects in cancer research and, above all, the rapid application of the resulting knowledge for the diagnosis and therapy of cancer patients. This can lead to a far-sighted use of present and new therapeutic approaches, combining better clinical performance with benefits that are also economically advantageous for the National Health System.
ACC is the largest Italian organization for cancer research, established in 2002 by the Italian Ministry of Health in order to create a network of high-level cancer institutions for patient care and research (Istituti di Ricovero e Cura a Carattere Scientifico [IRCCS]). The aim of such networking among Italian cancer institutions is to promote translational and clinical research, with the aim of supporting a rapid transition of scientific knowledge “from bench to bedside,” thus providing cutting-edge diagnostic and therapeutic procedures for cancer patients. The organization chart of the ACC and its purposes has been extensively described elsewhere1 and an up-to-date description of its overall activity can be summarized as follows: >4,200 researchers, >5,100 scientific publications with a normalized impact factor of >24,000, >268,000 patient hospitalizations/year, and 1,000 active clinical trials (https://www.alleanzacontroilcancro.it/en/).
The core of ACC is based on the activity of its WG. There are 9 fully active WGs scattered nationwide and aiming to address the major aspects of cancer related to 7 different types of cancer in a multidisciplinary approach, as well as extensive immunotherapy and a cross-genomic and bioinformatics task force. Currently, the fully active WGs are as follows:
Genomics and bioinformatics
Lung cancer
Breast cancer
Colon cancer
Glioblastoma
Melanoma
Sarcoma
Immunotherapy
Hematologic malignancies
These WGs, as well as their distribution at national level, are shown in Figure 1. Each WG is coordinated by a Secretary of the Executive Committee, a Head of Pre-Clinical Operations, and a Head of Clinical Operations, and is composed of a specialized team that includes translational investigators, pathologists, medical oncologists, surgeons, radiologists, radiotherapists, and nuclear medicine specialists, all committed to promoting cooperation and the exchange of ideas and information.
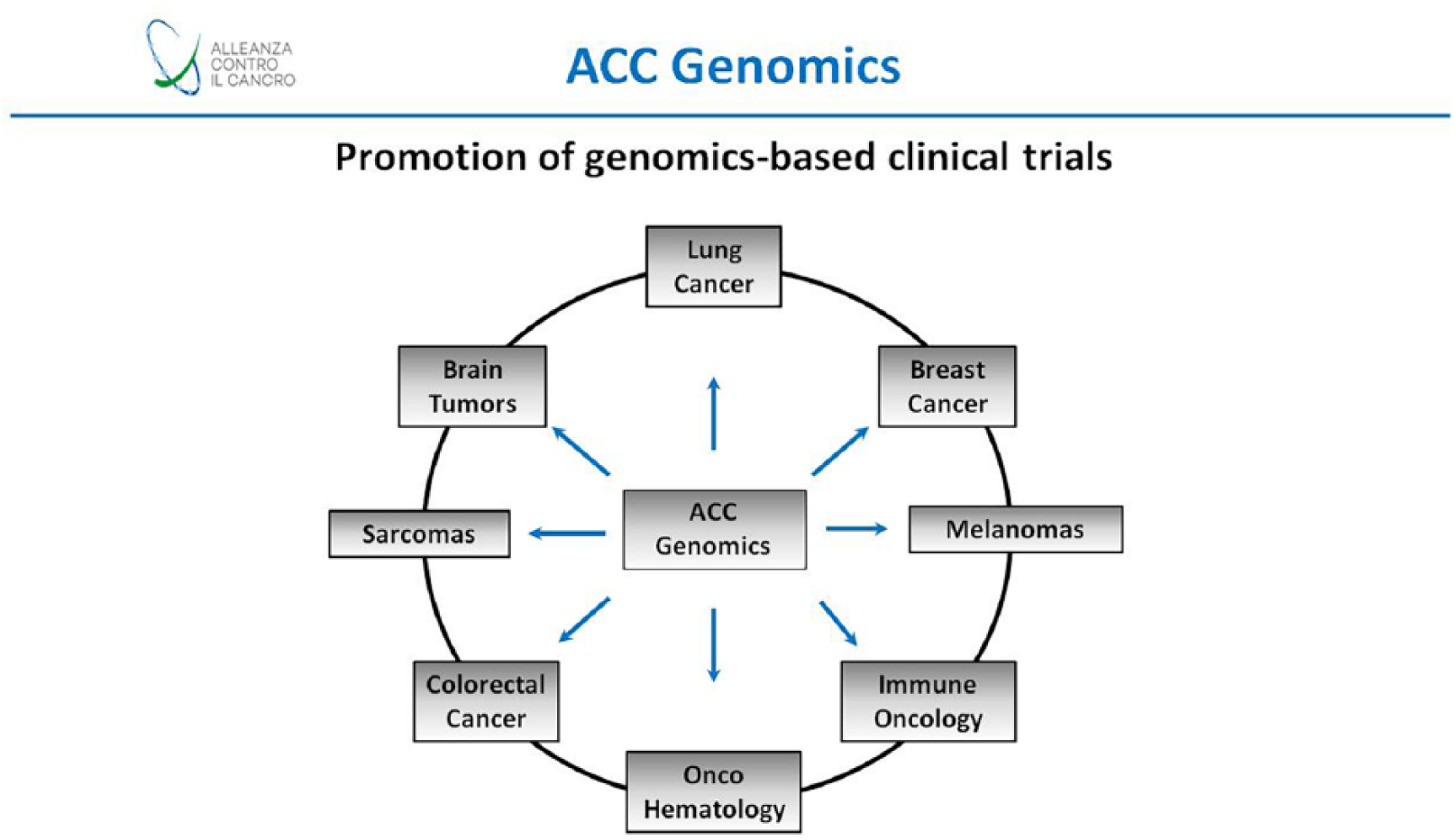
ACC genomics.
Cancer patients seeking treatment in any of the IRCCS belonging to the ACC network will receive added value compared to the routine procedures obtainable elsewhere. Their normal and tumour biological samples will be stored in biobank facilities belonging to the Italian node of Biobanking and BioMolecular Resources Research Infrastructure (BBMRI.it). Patient samples and their data will be collected anonymously in shared databases available to all participating institutions.
Patient samples will be regularly subjected to omics analysis. One of the main objectives, in all WGs, is the constant upgrading of existing infrastructures in order to perform genomic analyses for all patients (next-generation sequencing [NGS] molecular diagnostics). This procedure is the most important step in identifying the molecular signatures that can be used for a specific patient, laying the foundations for targeted therapies and personalized medicine.
The ACC network project for 2019 stems directly from the activity of the last 2 years, in which the ACC pursued the following objectives:
Organization of laboratories able to perform NGS analyses in each of the participating institutes, based on shared technology platforms.
Creation of a bioinformatics community, distributed in various institutes and involved in the interpretation and sharing of NGS data workflows
Organization of a shared data centre for archiving and analysing NGS data, at Cineca
Promotion of multicenter clinical studies guided by genomic information
Beyond these common activities, each WG can boast a strong specialization within the specific field of interest. We now summarize the results of each WG, highlighting their well-defined experimental and clinical activities that are closely related to their specific tasks.
Genomics and bioinformatics WG: This group is coordinated by Dr. Luca Mazzarella at the European Oncology Institute in Milan. This WG is structured to provide support to all the WGs dedicated to pathology.
Objectives and results
This WG is a research platform that was created to make molecular analysis technologies more easily accessible to the researchers in the ACC network in order to develop genetic panels and process their results. This WG first designed ACC Lung-Oncochip (see below) and more recently the GerSom panel, a platform that allows simultaneous analysis of germline and somatic variants in the tumour genome, with a connected IT infrastructure supporting data storage and interpretation.
The objectives are the initial validation of a targeted enrichment panel, including all clinically relevant genomic information and a parallel implementation of a supporting IT infrastructure in the whole ACC genomic project.
Lung cancer WG: This group is coordinated by the San Raffaele Hospital in Milan, which directs the clinical studies. The protocol was written by Dr. Vanesa Gregorc, in agreement with the other members of the ACC network, while the planned translational part in patients receiving immune checkpoint inhibitors was designed in collaboration with the immunotherapy WG (see below). The electronic case report form, which includes the molecular and clinical data of the recruited patients, was created in accordance with Clinical Research Organization High Research.
Objectives and results
The study provides validation of the ACC genomic pulmonary panel in patients with non-small cell lung cancer (NSCLC) using the ACC onco-chip for lungs as a molecular screening tool. It is mainly based on the evaluation of the diagnostic accuracy of the panel in the identification of 2 types of molecular alterations for which routine diagnostic tests are available: mutations that activate EGFR and rearrangements of EML4-ALK. The ACC has recently developed a sequencing panel for the identification of genomic alterations in 182 genes.2 Targets include the following:
161 genes considered “actionable,” defined as the presence of at least one drug with obvious clinical activity associated with a specific gene alteration. Such clinical evidence includes the approval of the guidelines published by the Food and Drug Administration or by the National Comprehensive Cancer Network that use alterations identified as a prospective stratification biomarker, retrospective analyses that exploit such alterations as poststratification markers, or case reports of exceptional response.
33 additional genes, considered as drivers (for example, fundamental genes for NSCLC biology), from at least 2 of 6 bioinformatics pipelines
89 transcripts of gene mergers considered as “actionable” with the same criteria as above, extracted from the TCGA fusion gene database related to NSCLC (http://54.84.12.177/PanCanFusV2/);
141 germinal variants from 86 associated genes, in the field of oncology, with altered pharmacokinetic drug response, extracted from the PharmGKB database (https://www.pharmgkb.org/)
In 2018, the lung WG launched the first clinical trial of a multicenter clinical study based on NGS analyses of patients with advanced lung cancer.
Breast cancer WG: This group is coordinated by the San Martino Hospital, Genoa, which directs the clinical studies. The protocol was written by Dr. Lucia Del Mastro, in agreement with the other members of the ACC network.
Objectives and results
The aim of this network is the identification of new prognostic/predictive biomarkers by developing 2 translational studies.
NEOGENE project: The purpose of this study is to identify specific mutations in triple-negative breast tumours resistant to neoadjuvant therapies or HER2+ subtypes without hormone receptor expression.3
Since in both subtypes the complete pathologic response is obtained in about 50% of cases and to date there are no known factors that can identify which tumours will be resistant to treatment, the analysis and comparison of genetic alterations before and post treatment will allow the use of targeted treatments against specific mutations in nonresponsive tumours. In this study, the WG proposes different approaches, based on liquid biopsy (in particular on circulating tumour DNA4 and on microRNA), or on the analysis of DNA and tumour RNA on formalin-fixed paraffin-embedded (FFPE) samples, where it is also possible to compare the presence of lymphocytic population (tumour-infiltrating lymphocytes in pre and post neoadjuvant tumour therapy).5
Development of RNA-seq protocol: The WG has completed a series of preliminary tests aimed at identifying the most reliable RNA-seq protocol on fixed and archived samples. The tests concerned the comparison between 7 different methods of 3 suppliers (Illumina, Lexogen, Thermo) on a series of 24 RNAs extracted from 8 mammary tumours, in which for each tumour one fragment was frozen, one put under standard conditions (FFPE), and one fixed in cold (a condition in which RNA shows a limited degradation compared to the LFA standard). On the same samples, the expression of the genes of the PAM-50 classifier will be evaluated using nanostring technology as a reference to understand whether some oestrogen receptor–positive or HER2-negative breast tumours could metastasize.
Colon cancer WG: This group is coordinated by the Humanitas Research Hospital in Rozzano, province of Milan, which directs the clinical studies. The WG Plan has been written by Dr. Luigi Laghi, in agreement with the other members of the ACC network.
Objectives and results
The objective of this study is to compare the burden of genetic damage present in primary tumours (stage II/III and IV) and in the respective metastatic lesions (metachronous for stages II and III, synchronous for stage IV).
The simultaneous study of the expression profile of primary–secondary lesions will provide information on the functional translation of damage at the level of expression. This will allow comparison of the prognostic value of the 2 omics approaches (genomics vs transcriptomics, including the molecular signature associated with tumour stroma components and determinants of the worst prognosis) to assess the impact on clinical management.
Furthermore, the use of a panel developed by ACC Genomics will also allow us to identify the pathology related to (inherited) predispositions and will therefore be an important prerequisite for the validity of the use of the NGS methodology in clinical practice for the systematic profiling of these diseases, today carried out in a fragmentary and nonhomogeneous way on the national territory.
Being a retrospective study, the case studies, once selected, will be prepared (nucleic acid extraction) in a centralized way (Humanitas) to be transferred to the centres designated for NGS analysis. The data will then be evaluated in relation to the clinical–pathologic characteristics of the samples (stage, time of onset of secondary lesion, treatment and outcome). All data will be mainly shared between the members of the WG operating committee.
Glioblastoma WG: This group is coordinated by the Veneto Oncology Institute, Padua, which directs the clinical studies. The protocol was written by Dr. Stefano Indraccolo, in agreement with the other members of the ACC network.
This WG is essentially concerned with high-grade astrocytoma and glioblastoma multiforme (GBM), classified morphologically as a grade III and grade IV astrocytoma.
GBM, despite optimal treatment,6 is associated with disproportionately high morbidity and mortality and, despite all the recent advances in molecular characterization, its prognosis remains dismal.7 The well-known heterogeneity of the GBM tumour clearly represents a condition that predisposes to resistance to drugs and recurrent disease.
Objectives and results
This WG is committed to achieving exhaustive genetic characterization in high-grade paediatric astrocytomas and adult GBM through the following specific tasks:
Realization of the genetic characterization of the primary GBM cell lines, with a particular interest towards those derived from a clinical recurrence. A total of 106 primary GBM cell lines were characterized by whole-exome sequencing (WES) and were made available to WG investigators for collaborative research.
Extension of the study project on long-term survival (>5 years) of GBM patients. A multicenter study was designed and launched for the genetic analysis and profiling of the tumour microenvironment on about 1,00l long-term survival GBM patients. A multicenter trial based on a multimodal approach on long-term survival GBM patients is being set up.
A 51-gene NGS panel dedicated to malignant gliomas has been developed.
A liquid biopsy project was launched on CSF (liquor) using the NGS panel developed by the WG.
Melanoma WG: This group is coordinated by the Dermatological Institute of the Immaculate Conception in Rome, which directs the clinical studies. The protocol was written by Dr. Giandomenico Russo, in agreement with the other members of the ACC network.
Objectives and results
Despite the impressive progress achieved with immunotherapy and targeted therapy in patients with high-grade melanoma, numerous problems concerning disease relapse and resistance are yet to be resolved. To this end, this working group is carrying out 2 separate projects:
Project 1: Retrospective validation of a new NGS panel (the so-called lung chip) for the mutational analysis of melanoma samples previously treated with BRAF and/or MEK inhibitors or with anti PD1/PDL1 antibodies. The main objective is the validation of a modified version of the lung chip as a diagnostic molecular screening. Sample size: 300 cumulative tumour and normal samples.
Project 2: Setting up an organoid-based preclinical model of the disease in order to produce reliable models of progression and therapy. The first step is the creation and banking of organoids (OTS repository) from patients with melanoma. Subsequently, the OTS biomolecular and phenotypic characterization will be performed, in order to generate reliable and significant results on the effect of the melanoma response to drug treatment.
Sarcoma WG: This group is coordinated by the Rizzoli Orthopaedic Institutes of Bologna, which directs the clinical studies. The protocol was written by Dr. Katia Scotlandi, in agreement with the other members of the ACC network.
Objectives and results
This WG aims to carry out a prospective multicenter clinical study for the identification of gene fusions on all bone and soft tissue sarcomas that express translocations that are difficult to detect with traditional techniques. The activity will be focused on patients with sarcoma included in the prospective clinical studies of the Italian sarcoma group.
Specifically, this study proposes to do the following: (1) give continuity to the recently started NGS study on all sarcomas of bones and soft tissues (e.g. Ewing’s sarcoma, synovial sarcoma, liposarcoma, osteosarcoma, and chondrosarcoma) to detect new gene fusions that are unrevealed with traditional techniques and/or with unknown genetic characterization; (2) apply the omics analyses by sequencing the entire exome (WES) and RNAseq in cases that are negative to the fusion panel. These technologies respond to the need to acquire new knowledge for not yet well genetically characterized pathologies; and (3) verify the biological significance of potential new pathogenetic factors identified through the previous objectives in experimental models that this WG has developed in the last 2 years of activity (patient-derived xenotransplantation, 3D cultures).
Furthermore, according to the well-documented experience on these issues by WG members,8 a key topic will be the collaboration with pathologists and clinicians that guarantees access to benign sets of sarcomas with centralized pathologic review and complete follow-up. This fact will allow not only adequate recruitment of these rare diseases but also rapid validation and clinical translation of the new findings.
Immunotherapy WG: This group is coordinated by the Bambino Gesù Pediatric Hospital in Rome, which directs the clinical studies. The WG plan was written by Dr. Concetta Quintarelli, in agreement with the other members of the ACC network.
Immunotherapy is the most successful approach for cancer patients and has been able to revolutionize patient outcome and quality of life in selected cancers, e.g. lung melanoma and adenocarcinoma.
Objectives and results
Since this therapeutic approach is rather expensive and not always successful, the key question is how to select responsive or nonresponsive patients (prediction of therapeutic response). To this end, this WG designed a retrospective IHC assessment of markers associated with patient outcome by testing the prognostic reliability of Immunoscore in 130 primitive tumours or in patients with early node-negative NSCLC. The evaluations (WES, RNAseq, human leukocyte antigen typing, TCR sequencing, and immunohistochemistry) are performed in selected ACC structures and analysed centrally by the Bioinformatics WG.
Hematologic malignancies WG: This group is coordinated by the European Oncology Institute of Milan, which directs the clinical studies. The protocol was written by Dr. Pier Giuseppe Pelicci, in agreement with the other members of the ACC network.
The increasing number of successful treatments in cancer patients has led to a corresponding increase in the onset of haematologic malignancies in long-term survivors.
Objectives and results
This working group is currently focused on the risk assessment of therapy-related myeloid neoplasms (t-MN) in patients with breast cancer under adjuvant/neoadjuvant treatment with anthracyclines and patients with non-Hodgkin lymphoma treated with chemotherapy immunotherapy (anti-CD20).
Specifically, the role of the following factors in the development of t-MN will be defined: (1) type of genetic alterations in the germline (hereditary variants); (2) number and size of CHIP clones, number and type of mutated CHIP genes (at different time intervals before and after chemotherapy); (3) interaction between germline mutations and somatic CHIP mutations; (4) accumulation of DNA damage after chemotherapy; and (5) correlation between preexisting (germline, CHIP) and subsequent (t-MN) genetic alterations.
Conclusion: Commitment of the ACC for better diagnosis and treatment of cancer patients: The efforts of all the WGs of ACC are therefore decisively oriented towards a modern and better approach to cancer, with the aim of challenging the most relevant scientific, translational, and clinic issues through a prism of the omics approach. Indeed, the genomic characterization of tumours is a direct approach to provide better therapeutic opportunities for cancer patients and increase the appropriateness of cancer treatment. This strategy will allow patients to participate in the best adapted clinical trials concerning not only their disease, but also the molecular alterations of their (somatic) disease and their genetic (germline) profile.
The main pathway of genomic characterization of the patient and of the tumour will rapidly lead to high-quality personalized medicine in oncology at a national level, where the initial investments will be amply rewarded by a more efficient therapeutic approach, thus reducing pharmaceutical costs for unnecessary, if not harmful, therapies and allowing a more appropriate use of novel and established drugs.
Palombo F, De Paoli P, De Maria R. Alleanza Contro il Cancro: the accreditation system of the Excellence Network of Italian Cancer Centers in the precision medicine era. Tumori 2015; 101 (Suppl 1): S64–S66.
Melloni GE, Ogier AG, de Pretis S, et al. DOTS-Finder: a comprehensive tool for assessing driver genes in cancer genomes. Genome Med 2014; 6: 44.
Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014; 384: 164–172.
Dowsett M, Sestak I, Lopez-Knowles E, et al. Comparison of PAM50 risk of recurrence score with oncotype DX and IHC4 for predicting risk of distant recurrence after endocrine therapy. J Clin Oncol 2013; 31: 2783–2790.
Solinas C, Carbognin L, De Silva P, et al. Tumor-infiltrating lymphocytes in breast cancer according to tumor subtype: current state of the art. Breast 2017; 35: 142–150.
Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005; 352: 987–996.
Diamandis P, Aldape KD. Insights from molecular profiling of adult glioma. J Clin Oncol 2017; 35: 2386–2393.
Urbini M, Astolfi A, Pantaleo MA, et al. HSPA8 as a novel fusion partner of NR4A3 in extraskeletal myxoid chondrosarcoma. Genes Chromosomes Cancer 2017; 56: 582–586.
Barnes RO, Shea KE, Watson PH. The Canadian Tissue Repository Network Biobank Certification and the College of American Pathologists Biore-pository Accreditation Programs: Two Strategies for Knowledge Dissemination in Biobanking. Biopreservation and Biobanking 2017; 15(1): 9–16.
HOW IMPORTANT IS PATHOLOGIST INVOLVEMENT?
Eliseo Mattioli1, Anna Altavilla1, Leonardo Resta2, Ettore Attolini3, Lucia Bisceglie3, Antonella Caroli3, F. Alfredo Zito1
1Anatomic Pathology Department, National Cancer Institute IRCCS “G. Paolo II,” Bari, 2Anatomic Pathology Department, University of Bari, 3Regional Health Agency (AReS), Bari, Italy
New technologies have allowed the pathologist to play an increasingly important role in research.
However, the involvement of pathologists in routine practice and research programs is strongly related to the local conditions in terms of instrumental equipment, number and typology of cases, and especially in terms of opportunity to collaborate with different professionals (molecular biologists, geneticists, technicians).
The high cost of new technologies and related personnel has required a reorganization of the anatomical pathology laboratories (APLs) on the territory by the legislator.
In 2013, the Apulia Regional Committee, at the request of the Regional Secretary of the Italian Anatomic Pathology Scientific Society (SIAPEC), set up a technical committee composed of the directors of the pathologic anatomy units and some regional committee officials.
The questions this committee sought to answer were as follows:
How many APLs are there currently in Apulia?
How many active pathologists are there currently in Apulia?
What is the workload of each pathologist?
How many APLs are needed in a territory with about 4 million inhabitants and how should these APLs be distributed?
Would it be useful to have the same laboratory IT system (LIS) for all APLs?
What are the minimum accreditation criteria?
What is the model to organize and distribute the APLs?
To answer these questions, the technical committee has organized a multistage study:
Collection of data on the number of cytohistologic cases per year and the number of medical, technical, and administrative staff members present in the various pathology units of the region (reference year 2014)
Collection of the documents regarding pathologists’ workloads according to SIAPEC guidelines and national and regional legislative documents1,2 on hospital assistance standards
At the same time, another technical committee was created for the construction of the LIS, composed of pathologists, computer technicians, and regional officials
The committee met about once a month and exchanged data via email.
As a result, at the time of the index year (2014), 94 active pathologists were counted in the region.
Data on the number of cytologic and histologic examinations were received from the local health authorities (ASLs) of Bari, Taranto, Lecce, Foggia, and Brindisi; from the University of Bari; from the IRCCS Cancer Institute of Bari; and from the “Casa Sollievo della Sofferenza” Hospital and the “Miulli” General Hospital. The number of cytohistologic examinations was estimated at around 210,000 cases (patients) per year, excluding PAP tests; the number of PAP tests was around 100,000 cases.
Based on these data, a network of APLs modelled after a hub and spoke pattern was proposed.
In July 2018, the Apulia Regional Committee, accepting all the requests of the technical committee, approved the foundation of the Apulian Pathology Network.3
The resolution provides the following
The presence of one hub and one spoke in each province; the hub must manage cytohistologic diagnoses, molecular pathology, and other complex assays; the spoke should preferentially deal with cervico–vaginal screening
The connection of hub and spoke via the same LIS to share data and to foster the regional electronic health records and the tumour register
The establishment of criteria for the construction of a modern personnel plan, in which the involvement of the pathologists in their various activities (workload, participation in interdisciplinary teams, ROSEs, number of hospitals served) is quantified as a percentage score
Assessment of the structural and technical requirements of the network
Apulia is the first Italian region to create a network that will allow standardized access to cytohistologic examinations for all Apulians. The hubs will be provided with all the necessary tools to deal with the most complex cases, also improving the diagnostic skills of pathologists. The high number of clinical cases will also allow improved research and a well-stocked tissue bank.
Ministry of Health. Guidelines for traceability, collection, transportation, storage and archiving of cells and tissues for anatomic pathology diagnostic assays, http://www.salute.gov.it/imgs/C_17_pubblicazioni_2369_allegato.pdf (2015, accessed 5 May 2019).
Ministry of Health. Ministerial Decree no. 70/2015, Regulations about qualitative, structural, technological and quantitative standards of hospital assistance, http://www.camera.it/temiap/2016/09/23/OCD177-2353.pdf (2015, accessed 5 May 2019).
Regional Committee Resolution no. 1335, Establishment of the Regional Pathology Network. Definition of additional structural, organizational and technological minimum requirements, http://www.regione.puglia.it/documents/10192/19676300/Bollettino+numero+114+-+Ordinario+-+anno+2018/92d87491-447c-4603-a8e9-0bea4902b60b;jsessionid=3E1F5ADC7750A671A7E5EABDDDE6C0B4 (2018, accessed 5 May 2019).
THE NATIONAL PLAN FOR INNOVATION OF THE HEALTH SYSTEM BASED ON OMICS SCIENCES
Antonio Federici1, Claudio D’Amario2
1Directorate of Prevention, Ministry of Health, Rome, 2General Director, Directorate of Prevention, Ministry of Health, Rome, Italy
According to the WHO,1 “With the mapping of the human genome, the genetics revolution has begun.” “Revolution,” among others, refers to culture, biotechnology, informatics, ethical, and social sciences innovations.
Progress in genomics has crucial implications for public health because it offers the opportunity to differentiate individuals and groups most likely to develop certain pathologic conditions within populations. In the last 2 decades, the use of words ending in “omic” has extended, from the initial “genomics,” to a wide range of biomolecular disciplines addressed to the study of specific aspects considered as a whole. Therefore, the omics sciences study pools biological molecules with various functions within living organisms2 and have the primary objective to analyse as a whole, e.g. genes contained in DNA (genomics) and their multiple functions (functional genomics), DNA transcription product RNA (transcriptomics), proteins encoded by DNA through RNA (proteomics), and molecules that interact within an organism or metabolites (metabolomics).
In this context of research and innovation, on one side, it should be considered that the plethora of high-throughput technologies available for the omics sciences and their rapid evolution requires the scientific community to adopt greater harmonization and standardization in data generation and analysis methods, and, at the same time, the existence of extensive possibilities for the implementation of new data mining tools. Therefore, one of the current challenges is to overcome the gap between the production of omics data and the progress of high-throughput technologies and our ability to manage, integrate, analyse, and interpret this large amount of data. Consequently, in the next decade, genomics and other omics sciences will play a decisive role within big data.3
On the other hand, in light of the existing health challenges, policy makers should capture the potential of genomics to meet public health goals through health policy. While genomics offers a growing range of approaches to help prevent, diagnose, and treat diseases, appropriate policies are necessary to ensure that the right tools reach the right people at the right time.4
The balancing of innovation, based on scientific achievements, versus effectiveness, quality, safety, and sustainability, is a challenge that in the last years the European Union has focused on. The European Union wants to stay at the forefront of genomic and personalized medicine globally, and improve its scientific capabilities and industrial competitiveness for the benefit of patients and the economy.5
At the Member States level, according to the Italian Chief Medical Officers survey initiative,6 few countries have implemented a structured national policy.7 In Italy, the National Prevention Plan foresees, since 2012, the macro-area of personalized medicine, along with primary/secondary/tertiary traditional prevention areas. In 2013, to implement the Personalized Prevention Plan, the State–Region conference approved and published the national initiative on public health genomics.8 A further step forward has recently been made with the approval of a National Plan for Innovation of the Health System based on omics sciences.9
The Plan aims to meet the challenge of a comprehensive approach to innovations taking into account that such an innovation is deeply intertwined with the economic growth of the country, above all with regard to the cross-cutting topic of the IT. Furthermore, according to Organisation for Economic Co-operation and Development,10 the Plan also aims to support the careful implementation and the intelligent use of big data in the health care sector and to foster the eventual achievement of significant benefits both in terms of population health and economies.11
The Plan is also committed to implement the recently issued European Union Council conclusions on personalized medicine for patients.12
The Plan outlines the ways in which innovation in the omic field should reshape the National Health System (NHS) in the areas of prevention, diagnosis, and care, taking into account effectiveness (evidence-based) and sustainability (cost-effectiveness) of the NHS, to improve the health of the individual and the population.
The Plan aims to:
Increase all stakeholders’ awareness on the innovation of omics sciences and its effects on the health of individuals and populations enhancing the capacity of the society to cope with the cultural, ethical, and psychological aspect of the “genomic revolution”
Put in place a strategy of “government of innovation” of genomics and related fields
Evaluate and implement the opportunities currently offered by genomics and by the other omics sciences for the health of the population
Therefore, the main objectives are to:
Transfer genomic knowledge into the practice of health services, in a patient-centric approach
Increase the effectiveness of prevention, diagnosis, and treatment of diseases at a higher burden, taking into account individual differences in genetic heritage, lifestyles, and environment, and providing professionals with the resources needed to customize interventions
Promote the cultural, scientific, and technological innovation of the healthcare system
The Plan focuses on several topics, including genomics in the diagnosis of mendelian and complex diseases (e.g. tumours), personal prevention (preconception tests, pre- and postnatal tests, neonatal screening), genomics in therapy (pharmacogenomics and personalized tumour therapy). In addition, the Plan highlights the functions of the central government and actions to support the implementation of the Plan. It also sets priorities for research and innovation by addressing topics such as the following:
Big data and computational medicine
Literacy technologies
Opportunities for system sustainability by replacing drugs
Greater efficiency of pharmacogenomics research
Opportunities for system sustainability through pre-primary prevention aimed at reducing the burden of disease
Opportunities for system sustainability through secondary prevention aimed at reducing the burden of breast cancer
Opportunities for system sustainability through early diagnosis aimed at reducing the burden of cancer disease
Undiagnosed patients
Among other topics, as mentioned above, the Plan pays special attention to cancer, given its medical relevance and the great deal of scientific knowledge, due to the already available high-quality research results.
In particular, the Plan focuses on promoting genetic testing for germinal mutation in the case of BRCA 1–2, Lynch, and prostate cancer (in relatives and to estimate the risk of metachronous cancer) and for somatic mutations; in both cases, updated guidelines are strongly requested. A further priority is to exploit the opportunities of personalized therapy.
The Italian Ministry of Health has already started implementing the governance requested by the Plan, taking into account the devolution of powers of the NHS. This governance is a part of the comprehensive call for building the capacity of the whole system to dial with such a difficult task of implementing the Plan. A further transversal relevant aspect in the implementation process is to promote a comprehensive and coordinated approach to training (of specialists), education (of professionals), and literacy (of the population).13
It is also clear that it will be impossible to conceive and implement such a policy without the cooperation of professionals and citizens, through their scientific societies and organizations.
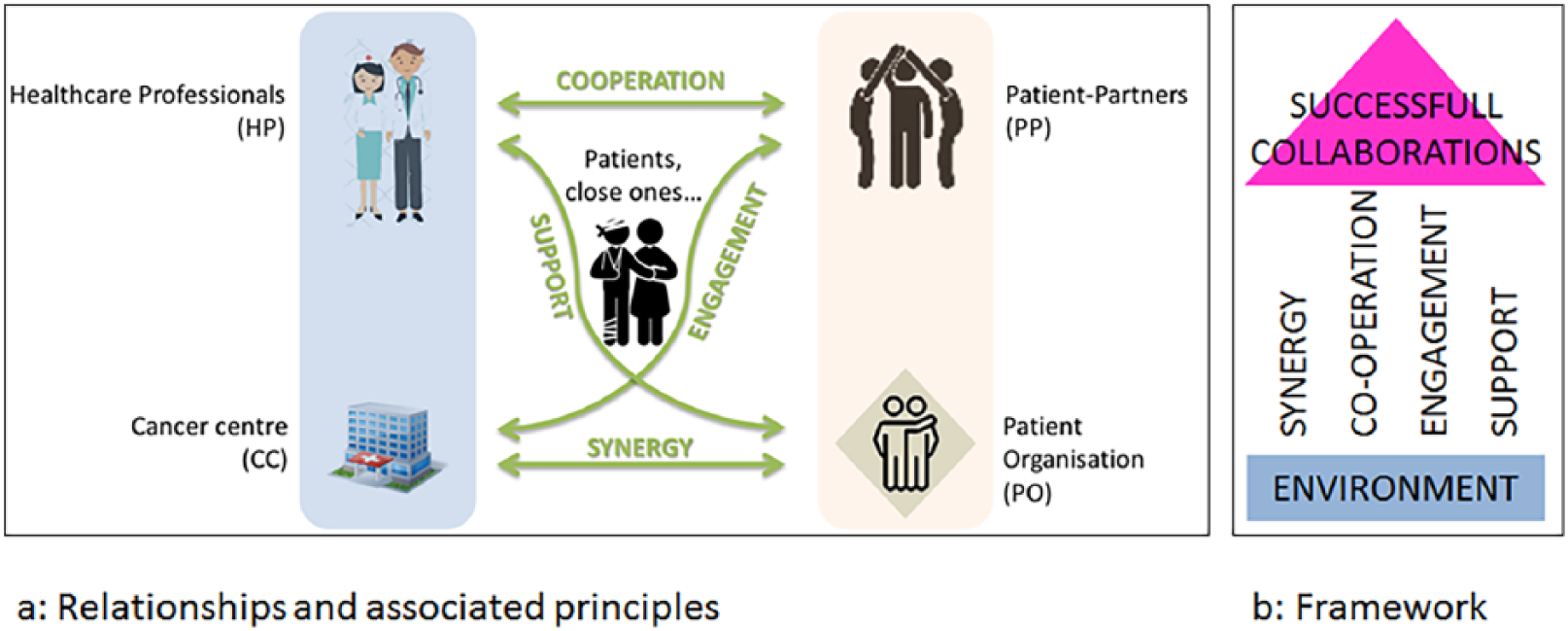
Conceptual framework for successful collaborations between individuals and organisations in cancer centres.
The figure contains the following elements: (a) the web of relationships existing between the different actors and relationship-based principles; (b) a schema of the framework where principles taken all together, and setup on the environment, are the pillars of the framework for successful collaborations.
WHO. Human Genomics in Global Health: Genomics and policy, http://www.who.int/genomics/policy/Genomicsandpolicy/en/ (accessed February 21, 2019).
Lin J, Qian J. Systems biology approach to integrative comparative genomics. Expert Rev Proteomics 2007; 4: 107–119.
Alyass A, Turcotte M, Meyre D. From big data analysis to personalized medicine for all: challenges and opportunities. BMC Medical Genomics 2015; 8: 33.
WHO. Human Genomics in Global Health: Genomics and policy, http://www.who.int/genomics/policy/Genomicsandpolicy/en/ (accessed February 21, 2019).
Towards access to at least 1 million sequenced genomes in the European Union by 2022, https://www.euapm.eu/pdf/EAPM_Declaration_Genome.pdf (accessed February 25, 2019).
Boccia S, Ricciardi W, McKee M, et al. Chief medical officers meeting on implementing a public health genomics approach. Epidemiol Biostatistics Public Health 2015; 12: 1–2.
Mazzucco R, Pastorino T, Lagerberg M, et al. Current state of genomic policies in healthcare among EU member states: results of a survey of chief medical officers. Eur J Public Health 2017; 27: 931–937.
Simone B, Mazzucco W, Gualano MR, et al. The policy of public health genomics in Italy. Health Policy 2013; 110: 214–219.
Conferenza Stato-Regioni. Piano per l’innovazione del sistema sanitario basata sulle scienze omiche. www.regioni.it/sanita/2017/11/06/conferenza-stato-regioni-del-26-10-2017-intesa-sul-documento-piano-per-linnovazione-del-sistema-sanitario-basata-sulle-scienze-omiche-537534/ (2017, accessed 5 May 2019).
OECD Directorate for Employment, Labour and Social Affairs Health Committee. Why and How Countries Can Promote the Use of Health Care Big Data? Paris: OECD; 2015.
OECD. Public Health in an Age of Genomics, OECD Science, Technology and Industry Policy Papers, No. 8, OECD Publishing, http://dx.doi.org/10.1787/5k424rdzj3bx-en (2013, accessed 5 May 2019).
Personalised medicine for patients: council conclusions, http://data.consilium.europa.eu/doc/document/ST-15054-2015-INIT/en/pdf (accessed 7 December 2015).
Tognetto A, Michelazzo MB, Ricciardi W, et al. Core competencies in genetics for healthcare professionals: results from a literature review and a Delphi method. BMC Med Educ 2019; 19: 19.
PATIENT INVOLVEMENT IN EUROPEAN CANCER CENTRES: FROM THEORY TO PRACTICES AND TO CHANGE
Patrick Miqueu1,2, Dominique de Valeriola1, 2
1Institut Jules Bordet, Université Libre de Bruxelles, 2Organisation of European Cancer Institutes (OECI), Collaboration for Good Practices with Patients (CGPP) working group, Brussels, Belgium
Patient involvement in OECI cancer centres
Quality improvement in cancer care and research is a major goal shared by healthcare professionals, researchers, patients and their relatives, and the public. It is now recognized that patients are bringing a different and valuable perspective to the quality improvement process. The Organisation of European Cancer Institutes (OECI) promotes quality for cancer centres, through its Accreditation and Designation Programme based on the holistic concepts of comprehensiveness and multidisciplinarity, and values patient involvement.
Recent results of a survey achieved by the OECI Collaboration for Good Practices with Patients working group (CGPP) have demonstrated that cancer patients are increasingly involved in activities of OECI cancer centres and that these centres and patient organisations are collaborating. In May 2018, 76 OECI centres have been contacted to answer a questionnaire in order to collect real-world data on cancer patient involvement in our pluralistic European context. The survey has examined the level and variety of the patient involvement activity in European cancer centres, and described the relationships between cancer centres and patient organisations. It appears for 81% of the survey respondents that patient involvement and collaboration with patient organisations are widely adopted in OECI cancer centres in diverse areas of care and research.
These results support the framework of collaboration that has been produced conjointly by the OECI and the European Cancer Patient Coalition (ECPC) and presented during the 12th European Cancer Congress in 2017. The framework engages cancer centres to improve quality through the involvement of patients and collaborations with local and national patient organisations. It describes the relationships between the different actors (cancer centres, healthcare professionals, patient organisations, volunteers or patient–partners) and derives major principles to build a long-lasting cooperation, in order to solve local issues and advance policy topics. However, it also appears from the survey launched in 2018 that there is still a lack of specific indicators of performance to evaluate the impact of patient involvement on the quality of care and research. Indeed, even if the patient involvement activity is adopted in a majority of OECI cancer centres, it is still at its premises.
An OECI working group focused on patient involvement
Launched in June 2017, during the 10th OECI Oncology Days in Brno, the OECI CGPP working group is promoting, launching, sharing, supporting, and evaluating pilot projects that involve patients as a core activity. The vision of the group stands in solving recurrent issues in cancer care and research by promoting collaborations between cancer centres and patient organisations. The OECI CGPP working group is building a roadmap by collecting experiences of patient involvement and making an inventory of patient involvement–related projects launched in/by OECI centres. During the OECI Patient Day and during workshops organised by the working group, OECI centres are invited to present their projects and actions involving patients and relatives, as partners. The aim of these meetings is to share experiences and inspire other OECI centres and patient organisations. Finally, the working group aims to produce guidelines and provide guidance on the implementation of patient involvement actions; for example, by defining a common methodology of patient involvement, but also specific indicators of performance to assess the impact of patient involvement in projects and to update quality standards of the OECI accreditation and designation manual.
The OECI Patient Day
In order to map how OECI cancer centres are implementing the framework for collaborations built with the ECPC, the CGPP working group organises, for the first time, a dedicated 1-day conference during the OECI Oncology Days 2019: the OECI Patient Day. The OECI Patient Day welcomes contributions from professionals who involve patients and bring the perspective of the patients into their activities and developments. For this first edition, the coordinating committee of the OECI Patient Day has provided the opportunity to OECI centres to present specific patient involvement initiatives in collaboration, or not, with patient organisations. The respondents of the 2018 survey and the patient relations officers from the OECI centres that joined the OECI network in 2018 have been encouraged to submit abstracts. A total of 19 abstracts have been received, and reviewed and scored by 5 experts. A total of 11 abstracts were selected and will be presented in one of the 4 sessions: (1) “When Patient Improves Care”; (2) “Models of Patient Involvement in Care and Research”; (3) “Supporting Cancer Survivors”; (4) “Assessing the Quality of Patient Involvement” (the selected abstracts are published in the current issue). The OECI Patient Day will end with an open discussion with the audience in order to share and reflect on the experiences of all. This one-day conference is a wonderful opportunity to build a group of professionals committed to involve patients in cancer centres and to collaborate with patient organisations.
A new vision on quality
Good collaboration with patient organisations and a strong commitment for the involvement of patients are crucial for the OECI: it ensures that the main patients’ needs and concerns will be taken into consideration in cancer centre activities and general organisation. The involvement of patients at several levels, for example, in the core team of the CGPP working group, in the process of revision of the manual of the OECI Accreditation and Designation Programme, and in the cooperation with other bodies of the OECI will enrich the perception of professionals about quality. Today, quality is associated with a series of standards to respect and indicators to be measured. Quality, through the appraisal of the experiences of patients, is far from being easily synthetized by a list of items, however. Perception of quality care, through the eyes of patients, is somewhat different from the standards of professionals, and should be integrated into the OECI quality improvement process with an adequate methodology. According to the different steps of involvement (information, consultation, involvement, co-creation), there is still a large part of control in how patients are involved, but the movement is launched. The successful experiences of collaborations between patients and professionals of OECI cancer centres illustrate how capacities of patients can contribute to change of practices.
PATIENT INVOLVEMENT CAN BE UTILIZED IN DESIGNING OF EDUCATION IN CANCER REHABILITATION
Mervi Siekkinen1, Ritva Kosklin2, Hanna Ilus3, Teija Kemppainen4, Sirkku Jyrkkiö5, Pia Vihinen6
1Mervi Siekkinen, development manager, TYKS Cancer Centre and FICAN West, Turku University Hospital, 2Ritva Kosklin, Department of Oncology, Turku University Hospital, 3Hanna Ilus, Department of Medicine, Turku University Hospital, 4Teija Kemppainen, Cancer Charity Organization of Southwest Finland, 5Sirkku Jyrkkiö, Department of Oncology, Turku University Hospital, 6Pia Vihinen, TYKS Cancer Centre and FICAN West, Turku University Hospital, Turku, Finland
THE INNOVATIVE SOCIAL–HEALTH CARE PATHWAY SUPPORTING THE RE-EMPLOYMENT OF CANCER PATIENTS IN ITALY: THE ORGANIZATION PROJECT “UNA MANO”
Sara Paltrinieri
Local Health Authority, IRCCS of Reggio Emilia, Italy
In Reggio Emilia (RE), an industrialized Italian area in the Emilia-Romagna region, 95% of cancer survivors with good prognosis return to work (RTW), but almost half of them report barriers to work reintegration. Barriers could be attributed to the social environment at work, work tasks, health status, and patients’ perspective regarding their work ability. We have planned an innovative path of social–health assistance aimed at providing personalized interventions focused on tackling the problems encountered by cancer survivors in the RTW process.
The pathway of the organizational project “Una Mano” (authorization of the local ethics committee 2018/8410) was developed by the local health authority (LHA)–Istituti di Ricovero e Cura a Carattere Scientifico (IRCCS) of RE with the collaboration of Foundations Manodori and e-35 of RE. The project includes the LHA, the IRCCS of the RE, the Local Order of Physicians, voluntary nonprofit associations, professional and educational training organizations, social cooperatives, a trade union, and an accountant firm.
We have organized training events with the aim of sensitizing oncology departments, general practitioners, and occupational physicians on the innovative pathway in order to facilitate cancer survivors with interception of work difficulties.
The In-Forma Salute health service of the Medical Library of the LHA-IRCCS has been identified as the place to turn for cancer survivors employed in the diagnosis for recruitment. The occupational therapist of the project proceeds with the first screening to define the personalized intervention. Subsequently, the cancer survivors receive information assistance, health care, social assistance, or a combination of these. Since April 2018, we have intercepted 26 cancer survivors. In addition to information assistance, provided to all of them, 2 cancer survivors receive health care, from an occupational therapist and psychologist, and 6 cancer survivors receive social support, provided by social cooperatives and trade unions.
With personalized supports, we expect to facilitate work reintegration of cancer survivors in order to improve their quality of life and their well-being.
PATIENT INVOLVEMENT IN THE CREATION OF VALUE: PROSTATE AND BREAST CANCER CASE STUDIES
Chiara Ariotti
Humanitas Cancer Centre, Milan, Italy
Process: creation of new integrated care pathways and business cases that help us to ensure sustainability.
People: we work with all the actors involved along the pathway, including patients and caregivers.
Key Performance Indicator (KPI): we measure PROMs, PREMs, and process indicators
The first pathway we worked on is prostate cancer. The analysis of KPI, together with the mapping of patients’ pathway, led us to the identification of all the critical issues and to their resolution. In our first experience of reviewing clinical processes, we did not have a tool that we could have used to measure patients’ experience along the pathway. Hence we listened to the voice of our patients in the different touchpoint we had at the time and we started our first test from the patient and caregiver interview, investigating the impact of our innovations along the way. Another path we worked on is breast cancer. Here we interviewed the patients before mapping the new path.
Together with our patients we analysed their experience and highlighted critical issues and strengths. In order to better analyse the PREMs, we created a model that helped us sort the information: the 3P model.
By interviewing patients, we were able to support management in reviewing the pathway and our patients had a strong impact on our organization.
We have created surveys related to the pathways.
RECOGNIZING THE EXPERTISE OF PATIENTS AND PROMOTING THE INVOLVEMENT PROCESS
Martine Bouyssie
Institut Paoli Calmettes Marseille, France
The participation of patients in the French health system, and their expectations in terms of rights to information, are changing the role of health professionals. In order to strengthen and promote innovative partnership actions with patients whose common denominator is the individual and collective rights of health users, the Paoli Calmettes Institute has changed its conception of the relationship with the patient. In fact, the aim has become to position the patient as an actor in his or her care and safety. Patients have entered the life of the establishment since 2002 with the creation of a Patient Committee and today the strategic orientation of the establishment integrates health democracy. The first lessons focused on the importance of information provided to patients, from semantics to different communication vectors, in order to facilitate understanding between patients and professionals. The patient offers a different but complementary perspective to the decision-making bodies. There is an interaction between the culture of the patient experience and the hospital world with its regulations and financial needs in a constructive dynamic.
Progressively the presence of the patients has spread naturally throughout the establishment: its committees, works, and projects, including the promotion of the expert patient within the IPC. More recently, patients have been integrated into a working group tasked with collecting adverse events in pharmacovigilance. Therefore, today they contribute to some internal audits and facilitate the conception and implementation of a bad practices room. The integration of the users project is a positive recognition of the partnership. It represents a paradigm shift for professionals who somehow reveal their practices and organizations. Other projects are in preparation, such as trained patients able to analyse the root causes of organizational adverse events. Ultimately, patients offer their experience to IPC, and their vision, which is often more pragmatic, and less “protocolised.” This experiential exchange contributes to the improvement of organizations and practices in a dynamic of promotion of change.
OUTCOME OF PATIENT-CENTERED CARE SURVEY CONDUCTED IN CENTRAL EUROPE AND TARGETING PATIENT AND CAREGIVER STAKEHOLDER GROUPS
Laura Del Campo, Olga Sapoznikov, Francesca Traclò, Nicola Di Flora, Francesco De Lorenzo, Silvia Carelli, Alessandro Sproviero, INTENT group
Aimac–Masaryk Memorial Cancer Institute, Brno, Czech Republic
A survey aimed at evaluating stakeholder expectations from patient-centered care in regions of central Europe took place in fall 2018. It involved patients and caregivers from 4 countries: Czech Republic, Hungary, Italy, and Slovenia. The survey has been undertaken in the framework of INTENT Interreg project (https://www.interreg-central.eu/Content.Node/INTENT.html), which integrated project–partner institutions into joint cooperation for development of an innovative patient-centered cancer care model and guidelines for its implementation. Two types of questionnaires, designed specifically for patients and caregivers, covered significant fields that emerged from a consensus on definition and dimensions of patient-centered cancer care. A total of 1,148 patient questionnaires were collected and processed for the purposes of this study. The outcomes of the patient survey have shown that patients prefer direct contact with the cancer centre regardless of the purpose, as well as engagement of close family members into communication process during diagnosis and treatment. Waiting times were mentioned as the most common barrier in the field of accessibility. Furthermore, the interviewees stated that they would have preferred more time for their visit. The study also identified fields that, according to the patient’s point of view, could be taken over by volunteer organizations and services, which they would prefer to receive closer to their homes. An important result of the survey was the discovery that patients show interest in participating in cancer research projects, including not only clinical trials, but also the implementation of innovation technologies in reporting of patient-reported outcome measures.
Caregiver questionnaires contained similar dimensions to patient questionnaires. A total of 914 questionnaires were collected. The information provided in person or direct contact is indicated as the best way to provide information also in this group of reporters; the same applies for booking appointments for the patients they assist. Detailed outcomes of the survey will be specified during presentation.
HOW TO INCLUDE THE PATIENT’S VOICE?
Camilla Havsteen, Anne Skov Villadsen
Vejle Cancer Centre, Patients’ Cancer Hospital, Vejle, Denmark
The main objective at Vejle Cancer Centre is “patient first.” Patient involvement and collaboration is essential to the hospital for improving care and continually developing Vejle Cancer Centre as the patient’s cancer hospital. To reach our goals, we have several initiatives put in place. The starting point was the establishment of the Patient and Relative Council in 2012 as part of the strategic “patient’s cancer hospital” plan. Since then patients and relatives has been involved in strategic planning, and today patients and relatives are part of the Cancer Steering Committee, the Hospital Research Council, the Development Council, the Hospital Strategic Committee, and the Advisory Board of the Centre of Shared Decision-Making. The Patient and Relative Council has put in place several new initiatives, such as the patient education program “Dressed for cancer treatment,” the booklet “Good advice on patient safety,” and highlighted the need for topics such as sexuality and complementary treatment.
In addition to involvement in formalized organizational committees, patients and relatives are also widely involved in improvement work in clinics, e.g. lean improvement workshops. They bring other perspectives to the problem; the group dynamics are positively influenced and they observe the details of our daily work, which we do not notice ourselves. The motivation among staff to change the routines is increased when it benefits the patient.
Another program that we have is family conversation. It started as a pilot project and now it is a formalised offer for all patients and their families. Patients are offered a conversation with a nurse trained in family conversations.
PATIENT INVOLVEMENT IN NORWAY
Anne Grethe Ryen Hammerstad
Oslo University Hospital, Oslo, Norway
The project was funded by the Radium Hospital Foundation.
PATIENT INVOLVEMENT IMPROVES ONCOLOGIC CARE IN THE MAASTRICHT CANCER CENTER (MUMC+)
Bernd Kremer
Maastricht University Medical Center (MUMC+), the Netherlands
Patient involvement is a basic principle within the Maastricht Cancer Center (MCC). Therefore there is a patient panel available that is used in several care lines. This patient panel is active on all areas of oncologic activities, varying from care content to strategic choices. The principle of the oncology centre is “the patient stays, the doctor moves”; needs for privacy and peace, psychosocial and paramedical care have been formed in close cooperation with the patients.
Patients take part in various oncologic care lines and help to improve changes in care content and organisational interests (e.g. brochures, processes, and decision support system).
Within the MCC, patients played an active and important role in the area of case management. Strategic decisions on oncology are taken from the MCC to the cancer commission. Patients participate structurally, contribute to the discussions, and correct them where necessary.
Therefore, the patients are involved from the beginning.
In the end, patients are involved in scientific policy developments. Bridging the gap between research and assistance is of great importance to the organization. Strategic conferences are held together with patients, and researchers are engaged in conversation with patients to understand their perspective. Requesting a grant for scientific research is also criticized by patients. During the conference, examples of the aforementioned patient involvement that led to great improvements in our care are presented.
“GIVE WORDS TO WHAT IS UNSPEAKABLE”: EMPOWERING PARENTAL COMMUNICATION WITH CHILDREN REGARDING CANCER AND DEATH
Francesca Romito
National Cancer Research Center Istituto Tumori “G. Paolo II,” Bari, Italy
When a family faces a serious illness, all family members are involved in a process of adaptation to the new and stressful situation, with consequences at an emotional and relational level. Adults often think that the best thing to protect children from a painful reality is hiding the truth, but doing so they leave them isolated and alone in managing distressing emotions. There is a large amount of literature on the importance of involving children in family matters, especially when a traumatic event, like a cancer diagnosis, takes place. Children’s involvement is a necessary step for preventing their psychological distress and emotional suffering, also in the long term, after a traumatic event such as a parent’s illness or death. This knowledge is not acquired by all adults who are responsible for children’s education, like their parents and teachers.
For these reasons, the Psycho-Oncology Unit of the National Cancer Research Center in Bari, along with “Maria Ruggeri Foundation,” the Association for Patients with Rare Diseases, is conducting a project of primary prevention called “Give a word to what is unspeakable.” The preliminary phase of the project involved 7 primary schools and kindergartens in Bari, each of which hosts 2 meetings in which 2 psycho-oncologists had the opportunity to discuss with parents and teachers aspects of communication on cancer diseases and death.
The discussion is conducted with the help of videos, web-based support, and case reports. At the end of the 2 meetings, feedback is collected on the interest in the topic and on the perceived effectiveness of the discussion on the usual practices in the classroom and in family discussions.
THE PATIENT-AS-PARTNER APPROACH IN CLINICAL RESEARCH AT INSTITUT CURIE
Véronique Gillon
Curie Institute, Paris, France
The evolution of health issues, particularly with regard to the chronicity of the oncologic pathologies, makes partnership with the patient essential. The emergence of better informed patients, who wish to become more involved in the health choices concerning them, is increasing. It is not a question of these patients competing with the academic knowledge of professionals, but discussing with them their health pathways based on their lifestyle, their representations, and their experiential knowledge related to their cancerous disease.
At the Curie Institute, physicians and caregivers are becoming more aware of the help that volunteers and patient partners can give them and thus improve follow-up assistance. It is not about entering into competition or conflict but about finding complementarity.
Added to this is the acceleration of the hospital care path, which reduces the time spent by patients in our organizations and in hospitals (decrease in the average length of hospital stay, evolution of the clinic, and shared assistance between the city and the hospital or the treatment). In this evolving landscape, the Curie Institute has decided to optimize the place, role, and mission of our patients’ partners. Inspired by the Canadian model, the Curie Institute has developed and implemented its Partner Patient project dedicated to fulfil health democracy.
This project is structured in 4 areas: care, teaching, research, and e-health. It aims to define the empowerment of patients (or “power to act”) within our institution:
At the level of assistance, the Curie Institute associates user and patient representatives with the main projects of the hospital group; this approach enables them to participate in improving the quality of patient care through their experience and expertise. The activity of the partner patients consists of the following:
- At the “organizational and health” level: to review the care pathways and the documents given to patients - At the “system” level: to influence decision-making to meet the needs of the population and patients treated at the Curie Institute and our hospital partners - At the level of the contribution: to improve the training of health professionals and users
The Teaching Unit of the Hospital Group aims to integrate, develop, and perpetuate a framed involvement of patients’ partners in the evolution of advanced training of its target audiences.
The project of democracy in health carried out by SIRIC (Site of Integrated Research on Cancer, label awarded to the Curie Institute by the National Cancer Institute) and the Patient Partner project developed by the Hospital Group are opportunities to identify and share common actions, but also to develop new synergies through concerted action in the field of research. For example, associating patient representatives with decision-making authorities in research is the most obvious way to give them the opportunity to influence strategic decision-making.
The activity of the Patient Partner project consists of the following:
- Associate patient representatives with decision-making authorities
- Read documents such as briefing notes and informed consent forms
- Organize days and seminars of exchanges and debates on different topics
• Furthermore, new health information technologies open up perspectives to improve the quality and safety of the care pathway for the benefit of the patient, offering tools to the organizations, while generating information that can contribute to the progress of research. The Hospital Group has designed “MyCurie,” a completely secure portal for applications and patients, created specifically to provide personalized information on the assistance that people treated in our hospitals receive. This application, designed at every stage with Patient Partner within our institution, will be developed with a number of technological innovations in order to help and accompany our patients on their pathway.
RESHAPING RESEARCH THROUGH PATIENT INVOLVEMENT
Patrick Miqueu
Jules Bordet Institute, Brussels, Belgium
The active involvement of patients is now reshaping the cancer care and research landscape. In order to provide researchers and physician–investigators with another perspective on the issues and challenges encountered in cancer research, the Jules Bordet Institute has launched PISARO: a group of patients from the Institute dedicated to support and ameliorate research in oncology.
The mission of PISARO is to improve the relevance and impact of research projects initiated and supported by the Institute. For this purpose, PISARO involves patients in the early stages of the research process, and focuses on 2 main activities: 1) reviewing and collecting opinions on research protocols under development; 2) proofreading the information documents and consent forms of the patients.
PISARO is composed of patient–partners: namely, women and men who have been treated in the cancer centre, who wish to collaborate with the professionals and who are preferably members of patient organisations (not mandatory). A specific knowledge on research is not required when joining PISARO. Patient–partners are trained and supported before, during, and after the sessions, based on the topics covered. A patient involvement officer coordinates the group, assists researchers for interactions with patient–partners, and collects opinions.
PISARO is an advisory group; it is not yet mandatory for researchers to seek patients’ opinions. However, the constructive approach of the patient–partners’ group is highly appreciated by researchers who value patients’ input, and who want to gain impact and credibility in their grant applications, ethics committees’ submissions, and presentations to potential research participants.
IN SILICO DISSECTION OF DIFFUSE LARGE B-CELL LYMPHOMA MICROENVIRONMENT PROVIDES A 45-GENE PANEL FOR RISK STRATIFICATION
Sabino Ciavarella1, Maria Carmela Vegliante1, Marco Fabbri2, Simona De Summa3, Federica Melle2, Giovanna Motta2, Anna Enjuanes4, Alessandro Gulino5, Stefania Tommasi3, Anna Scattone6, Alfredo Francesco Zito6, Claudio Agostinelli7, Umberto Vitolo8, Annalisa Chiappella8, Elias Campo9, Claudio Tripodo5, Attilio Guarini1, Stefano A Pileri2
1Hematology and Cell Therapy Unit, IRCCS-Istituto Tumori ‘Giovanni Paolo II,’ Bari, 2Unit of Diagnostic Hematopathology, European Institute of Oncology, Milan, 3Molecular Diagnostics and Pharmacogenetics Unit, IRCCS-Istituto Tumori ‘Giovanni Paolo II,’ Bari, Italy, 4Genomic Unit, Institute of Biomedical Research August Pi i Sunyer (IDIBAPS), Barcelona, Spain, 5Tumor Immunology Unit, Dipartimento per la Promozione della Salute e Materno Infantile “G. D’Alessandro,” University of Palermo, Palermo, 6Pathology Department, IRCCS-Istituto Tumori ‘Giovanni Paolo II,’ Bari, 7Department of Experimental, Diagnostic and Specialty Medicine (DIMES), Bologna University School of Medicine, Bologna, 8Department of Hematology, Azienda Ospedaliero Universitaria Città della Salute e della Scienza di Torino, Torino, Italy, 9Hematopathology Unit, Pathology Department, Hospital Clínic, University of Barcelona, IDIBAPS, Barcelona, Spain
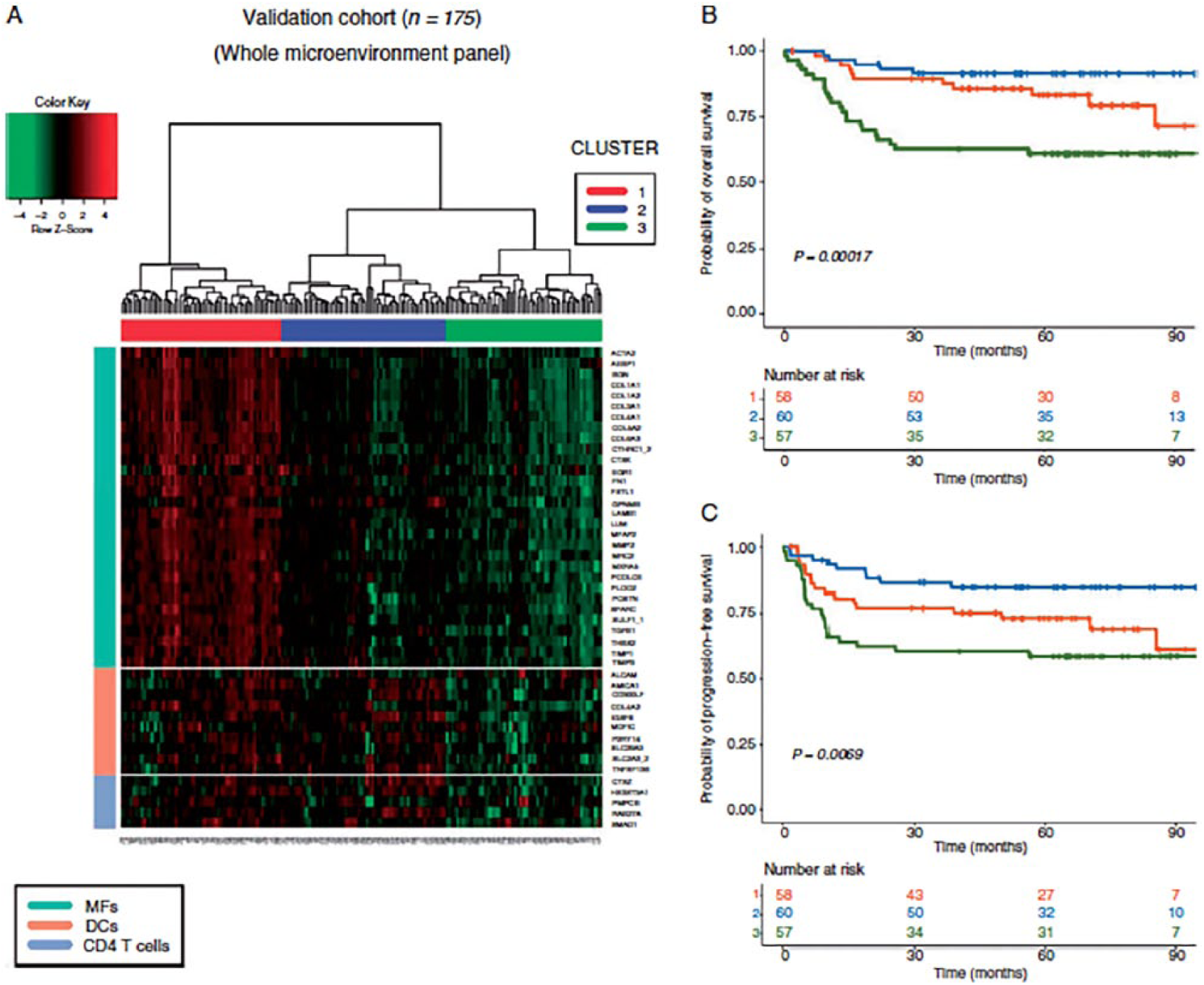
(A) The heatmap depicts the unsupervised hierarchical clustering of 175 DLBCL cases (NanoString technology) and identifies 3 different clusters according to high (cluster 1), intermediate (cluster 2), and low expression (cluster 3) of all genes in the microenvironment panel. The relative levels of transcripts are indicated according to the colour scale. Each row group comprises genes associated with specific tumour-infiltrating cell populations and each column a biopsy sample. Kaplan-Meier curves of overall survival (OS) (B) and progression-free survival (PFS) (C) demonstrate that patients in clusters 1 and 2 have significantly longer OS and PFS than those in cluster 3 (p < 0.05).
OPPORTUNITIES AND CHALLENGES OF EARLY PHASE CLINICAL STUDIES
Caterina Aversa, Johann S. de Bono
The Institute of Cancer Research, The Royal Marsden, London, UK
A better understanding of tumour biology, genomics, and the tumour microenvironment has led, over the last 2 decades, to a renaissance in anticancer drug development, which is shifting the paradigm of cancer care from conventional chemotherapeutics to targeted agents and immunotherapies.1 With this, we have seen the number of clinical trials testing novel anticancer drugs steadily increasing, raising the likelihood of successful development of these therapeutic strategies. Conversely, the risk of failure has increased substantially; indeed only a minority of early clinical trials lead to positive registration trials and the rates of negative phase III trials remain high.2
The rapidly enlarging body of basic, translational, and clinical research is providing an increasing large amount of preclinical evidence that merits interrogation in early clinical trials of novel therapeutic strategies with new anticancer agents and their combinations. However, promising laboratory results are often disappointingly not mirrored in patients in clinical trials, with increasing concerns about the true complexity of cancer biology and inter- and intrapatient disease heterogeneity.3 Overall, within this increasingly complicated landscape, the bespoke, customized design of innovative and hypothesis-testing, biomarker-driven, early clinical trials becomes crucial to reduce the translational gap, improve the delivery of better and more precise cancer care, and minimize treatment costs.
A key first step to increase the odds of success in the pursuit of this challenging task involves the use of highly rigorous methodology when designing clinical trials. Clearly, we must first ensure that sufficient financial resources are allocated and that an adequate number of patients can be recruited. More critically, however, we must first elucidate a clearly articulated research question to be answered by the clinical trial based on robust biological and scientific foundations and rational hypotheses. It is indeed vital that the critical question is identified upfront before the trial’s design is initiated. This central scientific question to be addressed by the clinical trial protocol must be clinically relevant, and likely to remain so for the future of the trial; that is, future-proofed for likely or potential changes in the standard of care. Hypotheses to be tested must arise from strong biological evidence and a good rationale, deriving whenever possible from different, reproducible sources.4 When developing such clinical trial protocols, researchers need to take into account the fact that the antitumour activity of the agent in question could be context-dependent, as for example seen with the differential activity of BRAF/MEK inhibitors in BRAF mutant melanomas and colorectal cancers.5
The acquisition of pharmacokinetic (PK) and pharmacodynamic (PD) data are essential to prove that the drug has satisfactory disposition and is impacting its primary mechanism of action with demonstrated target modulation. The incorporation of predictive biomarkers for patient selection, and the use of new generation trial designs, are other key components for the planning of high-quality, early-phase studies that can maximize the likelihood of success.6
Recent technological advances now allow a deeper understanding of the genomic background of tumours, and next-generation sequencing (NGS) methods are now widely available at reduced costs and rapid turnaround.7 In addition to this, transcriptomic, epigenetic, and proteomic analyses add to the available tools for biomarker analyses.8–10 While the main endpoint of early-phase trials remains the assessment of safety and tolerability, these trials increasingly represent an important setting for the first incorporation and testing of predictive biomarkers. Indeed, many Phase I units have now introduced routine NGS-based methods for the evaluation of clinical trial candidates and have proved that molecularly matched patient allocation can improve patient outcome.11 These strategies highlight the importance of large-scale genome and drug screening, including synthetic lethal screens, and for biomarkers to be identified and implemented in early drug development, prior to formal testing in later stages. Upfront identification of predictive biomarkers to be tested has the potential of accelerating drug development and eventual approval, minimizing the number of patients receiving an inactive drug. Such a successful example is represented by the development of poly(ADP-ribose) polymerase (PARP) inhibitors including olaparib, niraparib, and talazoparib, whose preclinical antitumour activity in homologous recombination defective tumour cells, including BRCA1 and BRCA2 defective cells, has led to their testing and several approvals for this molecular subset of tumours.12
Genomic analysis is usually performed on tumour tissue acquired by tumour biopsies. However, single biopsies may not be representative of the genomic heterogeneity that characterizes the majority of cancers; indeed this remains a major challenge for precision medicine to be applied.13 The presence of subclones originating from different genomic events can often be missed and confers de novo resistance impairing the activity of a drug. As obtaining multiple biopsies can be technically and logistically challenging, new and less invasive ways to access tumour nucleic acids have been developed, which can add to the study of tumour clonal evolution and tumour heterogeneity, with these being increasingly incorporated in trial designs.6 Circulating tumour cells (CTC) can reflect the genomic repertoire of primary and metastatic sites14 and can be harvested at multiple, different, time points during treatment with minimal patient discomfort.15,16 In addition, collection of circulating free DNA (cfDNA) can be of use, especially in the absence of CTCs, and can provide further insights on the tumour mutational repertoire and mechanisms underlying drug response and drug resistance.17
Phase I trials therefore represent the first and arguably the most important step for obtaining proof of mechanism and concept data to support the further evaluation of a novel anticancer compound. Depending on the novelty of the treatment and results obtained, Phase I trials may even lead to the accelerated approval of the drug such as in the striking case of pembrolizumab monotherapy in metastatic melanoma.18 Key to this is the identification of PD biomarkers that clearly reflect target modulation. Optimal PD biomarkers should be validated, reproducible, and correlate with a positive or negative outcome for the experimental compound in preclinical studies.19 Historically, collection of tumour tissue through biopsies has been the main platform for PD analysis. However, “liquid biopsies” analysing CTCs and cfDNA are now available to be implemented in clinical trials for PD analyses and can provide useful information in a less invasive manner.15,16
With regards to dose finding, the simple 3+3 dose escalation method has been widely used for dose selection of cytotoxic agents. However, this may not always be optimal due to more complex dose–efficacy relationships that characterize novel targeted and immunotherapy agents.20 More complex designs are increasingly being used to improve dose selection while acquiring preliminary antitumour activity data. Bayesian and adaptive designs adjust sample sizes and statistical analyses in real time as the trial progresses. As information on tolerability is obtained, these dynamic designs allow for contemporaneous, adaptive, flexible adjustments to select the most appropriate dose and schedule in attempts to optimize and accelerate dose escalation.21 In expansion cohorts, endpoints for efficacy can be included, with robust statistical powering, incorporating futility analyses to allow the trial to continue only if a certain number of responses are observed.22 Newer trial designs are also available to allow the inclusion of genomic information derived from NGS analyses. Umbrella trials enroll patients with the same tumour histology, but have different treatment arms onto which patients are allocated based on specific genomic aberrations. Conversely, basket trials include patients with common genomic aberrations regardless of tumour histology and represent rational tumour-agnostic drug development.23 Both designs are useful in testing multiple compounds and hypotheses within a single trial and can be excellent platforms for the testing and development of combinations of different drugs.
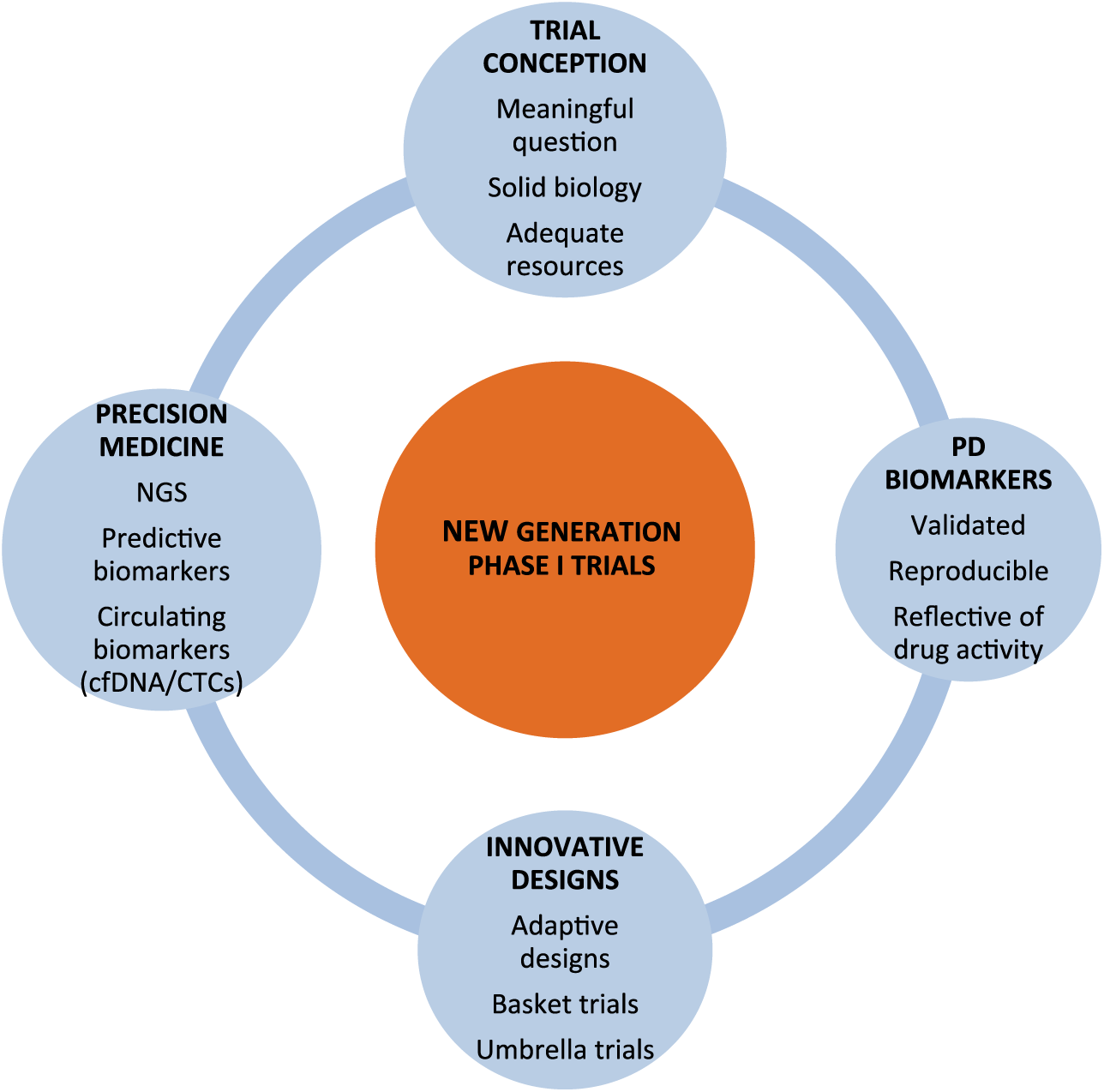
New-generation phase I trials.
In conclusion, modern anticancer drug development is rapidly evolving with our increasing understanding of the complexity of tumour biology, as well as the elucidation of cancer genomics and an appreciation of intra- and interpatient heterogeneity. This is leading to an increasingly refined precision medicine approach to early drug development involving biomarker-driven, hypothesis-testing, clinical trials. With the plethora of preclinical data available, rigorous trial design methodologies with the incorporation of predictive biomarkers, PK–PD data, as well as studies evaluating response and resistance determining treatment-induced clonal/subclonal evolution in tumour and/or circulating assays such as cfDNA and CTCs are likely to be key elements for successful anticancer drug development, making precision medicine a reality.
Hojjat-Farsangi M. Novel and emerging targeted-based cancer therapy agents and methods. Tumour Biol J Int Soc Oncodevelopmental Biol Med 2015; 36: 543–556.
Rubin EH, Gilliland DG. Drug development and clinical trials: the path to an approved cancer drug. Nat Rev Clin Oncol 2012; 9: 215–222.
Butler D. Translational research: crossing the valley of death. Nature 2008; 453: 840–842.
Yap TA, Sandhu SK, Workman P, et al. Envisioning the future of early anticancer drug development. Nat Rev Cancer 2010; 10: 514–523.
Ahronian LG, Sennott EM, Allen EMV, et al. Clinical acquired resistance to RAF inhibitor combinations in BRAF-mutant colorectal cancer through MAPK pathway alterations. Cancer Discov 2015; 5: 358–367.
Lopez J, Harris S, Roda D, et al. Precision medicine for molecularly targeted agents and immunotherapies in early-phase clinical trials. Transl Oncogenomics 2015; 7: 1–11.
Roychowdhury S, Chinnaiyan AM. Translating cancer genomes and transcriptomes for precision oncology. CA Cancer J Clin 2016; 66: 75–88.
Iyer MK, Niknafs YS, Malik R, et al. The landscape of long noncoding RNAs in the human transcriptome. Nat Genet 2015; 47: 199–208.
Jin S-G, Xiong W, Wu X, et al. The DNA methylation landscape of human melanoma. Genomics 2015; 106: 322–330.
Wilhelm M, Schlegl J, Hahne H, et al. Mass-spectrometry-based draft of the human proteome. Nature 2014; 509: 582–587.
Tsimberidou A-M, Wen S, Hong DS, et al. Personalized medicine for patients with advanced cancer in the phase I program at MD Anderson: validation and landmark analyses. Clin Cancer Res Off J Am Assoc Cancer Res 2014; 20: 4827–4836.
Kaufman B, Shapira-Frommer R, Schmutzler RK, et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J Clin Oncol 2015; 33: 244–250.
Yap TA, Gerlinger M, Futreal PA, et al. Intratumor Heterogeneity: seeing the wood for the trees. Sci Transl Med 2012; 4: 127ps10–127ps10.
Adalsteinsson VA, Ha G, Freeman SS, et al. Scalable whole-exome sequencing of cell-free DNA reveals high concordance with metastatic tumours. Nat Commun 2017; 8: 1324.
Frenel JS, Carreira S, Goodall J, et al. Serial next-generation sequencing of circulating cell-free DNA evaluating tumor clone response to molecularly targeted drug administration. Clin Cancer Res Off J Am Assoc Cancer Res 2015; 21: 4586–4596.
Alix-Panabières C, Pantel K. Challenges in circulating tumour cell research. Nat Rev Cancer 2014; 14: 623–631.
Bettegowda C, Sausen M, Leary RJ, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med 2014; 6: 224ra24.
Barone A, Hazarika M, Theoret MR, et al. FDA Approval summary: pembrolizumab for the treatment of patients with unresectable or metastatic melanoma. Clin Cancer Res 2017; 23: 5661–5665.
Altman DG, McShane LM, Sauerbrei W, et al. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): explanation and elaboration. PLoS Med 2012; 9: e1001216.
Ji Y, Jin JY, Hyman DM, et al. Challenges and opportunities in dose finding in oncology and immuno-oncology. Clin Transl Sci 2018; 11: 345–351.
Berry DA. Adaptive clinical trials in oncology. Nat Rev Clin Oncol 2012; 9: 199–207.
Simon R. Optimal 2-stage designs for phase II clinical trials. Control Clin Trials 1989; 10: 1–10.
Simon R. Critical review of umbrella, basket, and platform designs for oncology clinical trials. Clin Pharmacol Ther 2017; 102: 934–941.
ALLIANCE AGAINST CANCER: FROM ITALY TO EUROPE
Paolo De Paoli1, Silvia Careccia1, Gennaro Ciliberto1,2, Anna Sapino1,3, Pier Giuseppe Pelicci1,4, Ruggero De Maria1,5
1Alleanza Contro il Cancro–Alliance Against Cancer, Rome, 2Scientific Directorate, IRCCS Regina Elena National Cancer Institute, Rome, 3Scientific Directorate, Candiolo Cancer Institute-FPO-IRCCS, Candiolo (TO), 4IEO, European Institute of Oncology IRCCS, Milan, 5Scientific Vice-Direction, Fondazione Policlinico Universitario “A. Gemelli”–IRCCS, Rome, Italy
Alliance Against Cancer (Alleanza Contro il Cancro [ACC]), the largest Italian organization for cancer research, was established in 2002 by the Italian Ministry of Health as a network of 6 high-standard Institutes for Research, Hospitalization and Health Care (Istituti di Ricovero e Cura a Carattere Scientifico [IRCCS]). During the following years, ACC promoted a network among Italian oncologic institutions in order to develop specific, advanced projects in clinical and translational research. Indeed, many new full and associate members joined ACC, which currently comprises the National Institute of Health, 25 research-oriented hospitals, and 3 scientific/patient organizations, such as the Italian Sarcoma Group, the Italian Association for Cancer Patients (AIMaC), and the National Center of Oncology Adrotherapy Foundation (CNAO) (Figure 1). The ACC network project aims to bring diagnostic innovations and the most advanced therapeutic procedures to patients.1

The ACC. The ACC network is composed of 29 members, including 6 founders (at the top of the Figure), 20 full members (Ordinary Members), and 3 associated members (Adherent Associates).
The ACC network project
With the aim of establishing clinical trial programs for patients treated in Italian cancer centres and of facilitating their access to innovative drugs currently under development, ACC set up 7 working groups (WGs), one for each of the major cancer types for which there is a high degree of expertise in the network: lung, breast, and colorectal cancers, melanoma, glioblastoma, sarcomas, and haematologic cancers. In addition, 3 other WGs that crosscut the clinical research groups were established: the genomics WG, which was set up to make molecular analysis technologies more easily accessible to researchers in the network; the immunotherapy WG, which is mostly involved in the diseases currently known to benefit from immunotherapy; and the pathology and biobanking WG, which was established to produce standard common procedures to ensure the optimal conservation of samples.
Here we describe some of the projects that are moving towards a type of research aimed at developing precision medicine, and in which all the WGs are involved.
ACC Genomics
One of the major initiatives that characterize ACC is the tumour genetic screening program that aims to develop the first national clinical genomics study, at a cost that is well below the commercial platforms. It is for this reason that the Genomics WG was established. The program of the Genomics WG involves the characterization of tumours through next-generation sequencing (NGS) methods that, by drastically reducing the current costs of molecular diagnostics, will allow the individual patient to access more precise and effective therapies, thus avoiding unnecessary exposure to toxic and expensive treatments. To fully achieve this goal, ACC Genomics has designed a platform for the analysis of the tumour genome, which has a supporting IT infrastructure for data storage and interpretation.
The ACC Lung Cancer Project
The ACC flagship project sees the involvement of the Genomics WG and the Lung Cancer WG and concerns a multicenter study on lung cancer. In the last few years, the use of NGS, which allows simultaneous analysis of multiple genes, using relatively small amounts of tissue, has entered clinical practice. AAC has recently developed a genomic platform (“oncochip”) that enables the identification of all the molecular therapeutic targets of tumours and the gene modifications that regulate drug metabolism. Owing to this platform, it is possible to have information on the potential efficacy and on the toxicity of already approved or experimented drugs. The oncochip has already been validated retrospectively on tumour samples of non-small cell lung cancer (NSCLC) tumour tissue containing specific molecular alterations. The objective of the study, fostered by ACC and the Italian Ministry of Health, is to prospectively validate the oncochip in 1,000 cases of patients diagnosed with locally advanced or metastatic NSCLC undergoing treatment in 20 of the ACC Institutes. This is the first Italian prospective study to evaluate the use of NGS in classifying patients with NSCLC.
The ACC Breast Cancer NEOGENE and STRA-RNA Projects
The Breast Cancer WG has 2 projects that are aimed at identifying, through NGS techniques, prognostic and predictive biomarkers that will lead to personalized diagnostic and treatment approaches for breast cancer patients. The first project, NEOGENE, aims to identify specific mutations in tumours of patients with triple-negative breast cancer or with HER2+ and hormone receptor negative tumours that are resistant to therapies. These patients generally have a very poor prognosis due to failure to obtain pathologic complete response after neoadjuvant therapy. The identification of specific mutations lays the foundation for the development and use of targeted treatments on tumours that are not responsive to neoadjuvant therapy. The second project, STRA-RNA, aims at developing a molecular prognostic test, based on multigene expression analysis of the tumour tissue, that is more accurate and economical than those currently on the market. As well as the expertise of the researchers and the clinicians that make up the WG, the strength of the Breast Cancer WG, as for all the other ACC WGs, is in its numbers: 10,000 cases are treated every year in the 16 Institutes involved; very high when compared to the overall number of cases treated nationally.
The Mela-NGS Project
Despite the remarkable success of therapies with the BRAF and MEK kinase inhibitors and with immune checkpoint inhibitors in melanoma, there is still a need to develop new preclinical models that can quickly predict which drugs or combination of drugs can give an effective response for each individual patient. For this reason, the Melanoma WG aims to identify, through NGS technologies, biomarkers of therapeutic response in metastatic melanoma. The development of ACC’s oncochip (the Mela-chip, derived from the lung oncochip) is a step forward in the diagnostic use of low-cost NGS sequencing for the identification of possible new biomarkers. Moreover, for the evaluation of the activity of anticancer drugs and their combinations, this WG has generated a preclinical melanoma model starting from the patient’s tissue (organotypic tumour spheroids [OTS]). The OTS allow a detailed molecular and phenotypic characterization of the tumour (e.g. mutational, transcriptomic, and proteomic profile, cytokine secretion, clonal heterogeneity) that is useful for identifying potential new therapeutic targets and biomarkers of response/resistance to therapy.
Clinical research
The first ACC actions that were focused on the development of precision medicine highlighted the need to improve basic and clinical research together in a true translational research project. To this end, a Strategic Committee was created, called “Clinical Research and Drug Strategies,” with the aim of proposing ways to strengthen Italian translational research and to attract more funding. This committee proposed a project that aimed to enable the IRCCS members of ACC to foster quality assurance in clinical trials in order to ensure that the results of their trials are valid for regulatory purposes. In particular, the Committee proposed to develop academic clinical research, with a preference for projects that include the study of biomarkers, which can lead to changes in the registration of drug indications. These studies, which should meet quality criteria that can be verified according to Good Clinical Practice, in accordance with the current regulations, could boost the investments of pharmaceutical companies in Italy.
Quality-assured research environment
The Organisation of European Cancer Institutes (OECI) has developed the most commonly used accreditation program for cancer centres at the European level. In 2012, the Italian Ministry of Health decided to fund the accreditation program of Italian cancer centres.2 Ten centres completed the full cycle of the OECI Accreditation and Designation process over a 2-year period. In 2018, ACC established a committee that is dedicated to supporting the participation of Italy in OECI activities. This committee coordinates the reaccreditation (second round) of 10 Italian cancer centres and supports the centres that apply for accreditation for the first time. Furthermore, the committee has already sent a letter to the OECI president supporting the European Horizon FP9, an all-inclusive mission to fight cancer at all ages.
ACC Pathology and Biobanking
Given the importance of having standardized procedures for sample storage in a network project, ACC established the pathology and biobanking WG, involving the anatomical pathologists of all the clinical research WGs. The WG has organized a course with international experts involved in the drafting of ISO procedures, approved by the Italian National Unification Body, regarding the preanalytical phase of tissue processing. It also proposes to coordinate and plan the establishment of biobanks in order to promote the standardized collection and conservation of good-quality samples (mostly tissues) for subsequent analyses.
ACC acts as a research-funding agency
Since 2015, ACC has been a partner of the ERA-NET: Aligning National/Regional Translational Cancer Research Programmes and Activities (TRANSCAN-2), a 5-year project (2015–2019) funded by the European Commission under the EU framework programme Horizon2020. TRANSCAN-2 is a collaborative network of ministries, funding agencies, and research councils with programmes in translational cancer research. The network is composed of 28 partners from 19 countries. ACC acts in TRANSCAN-2 as a research-funding agency. Indeed, ACC funded a research project within the Fourth Joint Transnational Call 2017 (JTC 2017) on Translational Research on Rare Cancers. Moreover, for that call, ACC acts as Joint Call Secretariat to coordinate the application and selection process.
De Paoli P, Ciliberto G, Ferrarini M, et al. Alliance Against Cancer, the network of Italian cancer centers bridging research and care. J Transl Med 2015; 13: 360.
Oberst S, Boomsma F, Lombardo C, et al. Participation of Italian Cancer Centres of the Alleanza Contro il Cancro (ACC) in the Organisation of European Cancer Institutes (OECI) Accreditation and Designation program: a successful first national initiative. Tumori 2015; 101(Suppl 1): S6-S9.
THE MEDITERRANEAN ONCOLOGICAL ALLIANCE NETWORK AMORE (ALLEANZA MEDITERRANEA ONCOLOGICA IN RETE): AN OPPORTUNITY AND A CHALLENGE
Antonio Delvino1, Giovanni Battista Bochicchio2, Nicola Silvestris3, Alessandro Sgambato4, Gerardo Botti5, Elio Borgonovi6, Angelo Rosa7, Rosa Martino8, Pietro Milella9, Antonio Colasurdo10, Carmine Mariano11, Massimo Mancini12, Cristiana Mecca13, Attilio Bianchi14
1General Director, Cancer Institute “Giovanni Paolo II,” Bari, 2General Director, Cancer Institute, Rionero in Vulture, 3Scientific Director, Cancer Institute “Giovanni Paolo II,” Bari, 4Scientific Director, Cancer Institute Rionero in Vulture, 5Scientific Director, Cancer Institute “G. Pascale,” Naples, 6Bocconi University, Milan, 7 LUM “Jean Monnet” University, Bari, 8Sanitary Director, Cancer Institute “G. Pascale,” Naples, 9Sanitary Director, Cancer Institute “Giovanni Paolo II,” Bari, 10Sanitary Director, Cancer Institute Rionero in Vulture, 11Administrative Director, Cancer Institute “G. Pascale,” Naples, 12Administrative Director, Cancer Institute “Giovanni Paolo II,” Bari, 13Administrative Director, Cancer Institute Rionero in Vulture, 14 General Director, Cancer Institute “G. Pascale,” Naples
The Mediterranean Oncological Alliance Network Alleanza Mediterranea Oncologica in Rete (AMORe) was established on November 26, 2018, in order to reinforce the synergy between the regions of South Italy and aims to build an integrated network in order to promote cancer research and provide the best-practice treatment and care for cancer patients. This interregional Alliance was established by the 3 main scientific research and health institutes (Istituti di Ricovero e Cura a Carattere Scientifico [IRCCS]) dedicated to cancer research in South Italy: the National Cancer Institute of Naples–“G. Pascale” Foundation, the National Cancer Institute “Giovanni Paolo II” in Bari, and the Cancer Reference Centre of Basilicata in Rionero in Vulture (province of Potenza).
The purpose of this nonprofit Foundation is to set up a new modus operandi that, taking into account the needs of a constantly evolving medical environment and of a sustainable healthcare system, focuses on the real needs of cancer patients.
The introduction of innovations in the management of the services offered is essential to guarantee the best medical and technological practices while maintaining the sustainability of the Italian Health Service.
In recent years, we have witnessed the effects of the so-called “regional return plans,” with a substantial cross-cutting of services, which has led to a modest waste reduction, but also caused considerable negative impacts on patients.
The challenge can be faced only if the tendency will be to go beyond the traditional organizational models with the risk of not guaranteeing high clinical results despite improper use and the waste of human and economic resources. With this in mind, the goal of the health systems is to create an integration with other institutional sectors in order to meet the goals that are common to healthcare: ensuring fairness of access to services, ensuring safety and quality of care, and optimizing the use of resources through the achievement of high levels of efficiency. In fact, there is currently a geographic inequality in terms of access and quality of cancer care that has an impact on survival output. In fact, even if in all Western countries there has been a progressive increase in survival, the global comparison of 5-year survival from the diagnosis of cancer continues to show a geographic gap among different countries. In particular, in Europe the 5-year survival rate goes from 51% in the Eastern European countries to 63% in Italy (estimate based on cases diagnosed in the 2005–2009 period), compared to 69% in the United States and 67% in Australia.1–4 The geographic gradient is often present also in the national context among different regions. In fact, in Italy, despite the lower incidence of tumours in the South than in the North, in the southern regions, unlike the northern ones, there is no reduction in incidence and mortality due to the most common types of cancer, including breast cancer, colorectal cancer, and cervical cancer, observed in recent years. This probably reflects geographic discrepancies in terms of cancer screening programs and quality of service. The domino effect is a growing phenomenon of interregional health migration which, in the current framework of rationalization of the use of resources, takes on an explosive value. The search for solutions to guarantee fair access to services, high standards of quality, and economic sustainability must pass through a process of clinical, organizational, and functional integration.
This is the mission of the AMORe foundation: an integrated network that represents a synergistic collaboration among the 3 institutions, with the aim of guaranteeing high standards of care, even considering the large number of cancer patients globally. According to estimates by AIRTUM (Italian Association of Cancer Registries), the number of new tumours estimated for 2018 in the Italian regions involved in the AMORe project is approximately 55,900, which means more than 6 diagnosed every hour (30,050 in Campania, 3,250 in Basilicata, and 22,600 in Apulia). Faced with such a large number of patients, it is essential to implement organizational models that allow different structures and networks to collaborate and communicate with each other fluidly, in order to optimize the flexibility of the health system, share and spread knowledge, and consequently favour the improvement of therapy and assistance.
Specifically, 8 points of agreement have been established among the 3 institutes of the AMORe network:
Spread of knowledge on the causes, prevention, and treatment of cancer diseases
Scientific, clinical, medical, and experimental research in the field of neoplastic diseases
Physical and psychological assistance and rehabilitation of cancer patients, including the donation of material goods
The support of socially disadvantaged people with oncologic diseases
Training and improvement of personnel who will be, even indirectly, involved in medical and paramedical assistance and in the rehabilitation of cancer patients
Fundraising activities to achieve the goals mentioned in the previous points
Sharing of paths of diagnostic therapeutic assistance of performance assessment systems, in the care sector, in research, and on the main IT platforms
Promotion of innovative paths and procedures and management experimentation
The creation of an Interregional Network of Cancer Institutes, by means of a systematic collaborative agenda, and through constant comparison and exchange of skills and expertise, will ensure continuous improvement in the quality, the appropriateness, and the effectiveness of the assistance and services provided.
Therefore, it will be fundamental to define a common technological platform in which to collect homogeneous clinical and management data capable of supporting the research, and create a common system of indicators to be used for the evaluation of efficiency.
Among the objectives, there will be promotion of innovative organizational models centered on clinical ethics, clinical governance, policy sharing, appropriateness, and resource economics; completion of projects that benefit from foreign funding programs, in particular in relation to European Community funds; and accreditation as a Comprehensive Cancer Centre for each of the centres involved.
The sharing of clinico-experimental protocols is essential in order to achieve the priority objectives of the network and to offer the best therapeutic options to patients in the 3 regions, and beyond. It is also indispensable to have a computerized information system for sharing patient clinical data.
In conclusion, the integrated organization of Cancer Networks is the basis for the standardization of practices across all aspects of cancer care and can lead to a more favourable output in terms of effectiveness and economic performance. Integration is defined as “co-presence, mutual acceptance, mutual change: it is the cooperation of diversities” and, from this point of view, it becomes an essential condition for innovation. The complexity of the current clinical approaches requires the ability to embrace new models, increasingly rich in variables and new interactions in order to keep up with the rapid growth of knowledge and health needs expressed by patients.
These changes may at times prove uncomfortable, challenging, and difficult to explain but they are essential to remove inefficient, obsolete, and unnecessary processes that are no longer acceptable or sustainable.
The direction we are headed aims to improve patient management and outcomes while ensuring the sustainability of cancer care. We are confident that our patients will understand our objectives and hope that involved stakeholders will support our efforts.
Rossi S, Baili P, Capocaccia R, et al. The EUROCARE-5 study on cancer survival in Europe 1999–2007: Database, quality checks and statistical analysis methods. Eur J Cancer 2015; 51: 2104–2119.
Jemal A, Ward EM, Johnson CJ, et al. Annual report to the nation on the status of cancer, 1975-2014, featuring survival. J Natl Cancer Inst 2017; 109: djx030.
Australian Institute of Health and Welfare 2014. Cancer in Australia: an overview 2014. Cancer series. No 90. Cat. no. CAN 88. Canberra: AIHW.
AIRTUM Working Group. Italian cancer figures, report 2014: Prevalence and cure of cancer in Italy. Epidemiol Prev 2014; 38 (6 Suppl 1):1–144.
REFLECTIONS ON A COMPLEX TOPIC: THE MISSIONS: A NEW TOOL WITHIN HORIZON EUROPE, THE EUROPEAN RESEARCH AND INNOVATION PROGRAMME 2021–2027
Thierry Philip
OECI President
Horizon Europe’s new tool—Missions—will pave the way to achieve a wide range of objectives of remarkable societal relevance. The 6 selection criteria defined by the European Commission—cross-sectoral and cross-disciplinarily cooperation, co-design with citizens and end users, portfolio of measurable objective actions, impact on science and technology, society, and citizens—are the keywords defining the Programme.
This cutting-edge tool constitutes a new chapter of a story that began in 2000 when the Research Commissioner Philippe Busquin established the European Research Area, followed, in 2002, by the European Cancer Research Area where the Eurocan+ was launched. As a result, the network of excellence “EurocanPlatform,” the Transcan ERA-NET, and several other joint initiatives, concerning i.e. rare tumours, breast cancer, paediatric tumours, or quality evaluation, were set up.
The new Horizon Europe Framework Programme will be based on pillars (open science, global challenges, industrial competitiveness, and open innovation). The Missions belong to the second pillar and should be defined as clearly as the Apollo Mission: “Within 10 years, we will send a man to the moon and bring him safely back.”
The first document on a putative cancer mission was published in 2017, when the “Cancer Core Europe” network proposed a translational research programme to bridge the gap between clinical and preclinical research and between clinical and outcome research.
A different vision was published in 2018 by the Organization of European Cancer Institutes (OECI), together with EU-Life and European Cancer Organisation (ECCO), outlining a vision of a putative mission that should follow previous European actions, unify the cancer family by adopting a network of networks, and prioritize prevention, early diagnosis and screening, fundamental research, clinical research, outcome research, and patient needs.
In September 2018, the European Commission proposed 4 missions, which included a cancer mission, narrowed down to paediatric cancer. Paediatricians were able to clearly define a mission “to increase to 90% the survival of children with cancer and reduce toxicity by half.” They also provided a strategic plan for European paediatric oncology. SIOP already collaborates with the United States, Russia, China, South America, Africa, and India and already has several ongoing clinical trials and basic research programmes, as well as relations with patient organisations and industries. The collaborations developed in Africa are a practical example on how to improve results in less developed countries, fulfilling the vision of a mission of Professor Mazzucato.
Although the European Parliament clearly supported the European Commission proposal in October 2018, in November 2018 the European Research Council refused to settle to a Paediatric Mission, which was considered limited. Furthermore, despite strong support from France and Austria, a Paediatric Cancer Mission has not been chosen and the possibility of a broader cancer mission remains open.
The OECI has always supported the idea of a democratic mission alongside with other cancer organizations, thus refusing to consider the Cancer Core approach, while believing that they should be the main actors in a coordinated action with a panoramic European vision and partnership.
The OECI strongly supports the decision of the European Commission to appoint a specific council “to represent balanced sectors and interests” for each mission, reassuring that “the objectives of the mission should be established in co-creation and co-planning with all stakeholders,” and confirming the OECI point of view from the beginning.
A European OECI Mission Working Party was held in October 2018 with the participation of ECCO, EORTC, ECPC, ESO, UNICANCER, Alleanza Contro il Cancro (Alliance Against Cancer), EU-Life, IARC, Cancer Prevention Europe, and ECL. Cancer Core Europe did not participate in the gathering. However, all the abovementioned organisations were also invited to a Cancer Core Meeting in Vatican City in November 2018. The meeting was organized in a good spirit of dialogue and discussions are ongoing and aim to find a similar approach to the Apollo Mission.
Considering the results of the OECI Brussels meeting and the Cancer Core Vatican meeting, the role and place of nurses, economists, data specialists, and patient groups are paramount in the organisation of a putative mission.
In conclusion, the focus of the mission is still to be defined, and several hypotheses were proposed:
Focus solely on paediatric
Focus on the cancer tsunami among Europe’s ageing population
Focus on paediatric, young adults, and rare tumours
Focus solely on paediatric and adult tumours (or tumour subtypes) with a survival rate of less than 20% at 5 years
Focus on prevention, including research on early diagnosis and screening in order to reduce the burden on European health systems
Coordinate member states and the European cancer community in order to reduce inequalities and disparities in cancer therapy
OECI is ready to be a loyal partner in an interdisciplinary co–design project with measurable impact on citizens, society, patients, and innovation.
Public and patient perspectives should combine professional perspectives, and one of the big issues is to clearly define who are the best among the actors. Within a mission announcement for a peer review assessment, external evaluation is mandatory, but quality, efficiency, and true supplementary care should be measurable. The OECI Accreditation and Designation Programme (ISQUA certified), our core activity, will be useful for certifying comprehensive cancer centres, clinical cancer centres, and virtual cancer centres within a university hospital.
With or without a mission in the setting of adults, as paediatricians, we must define our vision of the fight against cancer for the next 10 years. National Cancer Networks and other national organizations should be associated (24 member states have a document that summarizes their cancer-fighting goals). Taking into account the importance of prevention, IARC should be one of the main actors in defining and setting a new vision to reduce the incidence. The aforementioned actions could be supported as part of a mission or to find legitimacy and financial sustainability as part of the tender in the 3 pillars of Horizon Europe.
FAQs Horizon Europe for RWP version 27. Non-paper of the Commission services. Luxembourg: European Commission; http://lino.lmt.lt/wp-content/uploads/2018/08/%C4%8Dia.pdf (2019, accessed 5 May 2019).
Celis J, Pavalkis D. A mission-oriented approach to cancer in Europe: a joint mission: Vision 2030. Molecul Oncol 2017; 11: 1661–1672.
Philip T, Almouzi G, Poortmans P. Vision 2030 for the optimal approach to cancer research and care in Europe: a mission or a network of networks. Tumori Epub 2018 Jun 1.
Vassal G, Schrappe M, Pritchard-Jones K, et al. The SIOPE strategic plan: a European cancer plan for children and adolescents. J Cancer Policy 2016; 17–32.
Mazzucato M. Mission-oriented research & innovation in the European Union: a problem-solving approach to fuel innovation-led growth. Luxembourg: European Commission; 2018: 1–36.
ECCO’S 5 ITEMS OF ADVICE ON EU MISSION CENTRED CANCER ACTIVITY
Philip Poortmans1, Richard Price2
1President, ECCO; Head of Department of Radiation Oncology, Institut Curie, 2EU Policy Affairs Manager, ECCO, Brussels Belgium
The European Cancer Organisation (ECCO) warmly welcomes a European Union more fully engaged in delivering mission-oriented cancer activity.1 It responds in great part to a previous call we made for the EU to reconnect with citizens and reinspire a generation by better addressing one of the primary and universal concerns possible: the common desire across countries and social groups to further combat cancer.2
Beyond this, as we await further detail of how exactly the EU intends to take up mission-orientated cancer activity from 2019 onwards, we would like to offer 5 primary elements of advice. A mission on cancer is honourable and laudable. However, how the mission is conducted is integral to eventual success. So we advocate that:
The mission is developed with evidence and need in mind
The mission is formed and shaped in an open and transparent manner
The full range of disciplines and stakeholders are brought to the fore in the effort of achieving the mission
Regular reporting and accountability for delivery of the mission is conducted
The need to assist health system development and address inequality is recognised and responded to
Selecting and developing a mission with need and evidence in mind
Cancer at the European level is a broad field of policy, with, among other variables:
Hundreds of individual tumour types, each with their own particularities, in respect to issues such as diagnosis, treatment, and follow-up care
Emergent science and technology impacting all treatment modalities and across all areas of the care pathway
Deviation in health system organisation and finance producing highly divergent outcomes
The list of potential missions that the EU might therefore choose to apply in respect to cancer could be almost endless. Yet selection must be made.
Temptation to choose a mission in respect to cancer based primarily on political considerations must be resisted if credibility and the widest buy-in from the expert community is not to be compromised.
ECCO therefore suggests an EU cancer-related mission be clearly demonstrated to have strong basis on need and evidence. In short, the evidence for why a certain mission in cancer was chosen, as opposed to other alternatives, must be given up-front and not left to others to fill in the blanks. All should be provided with confidence that the correct mission was chosen on the basis of the best information.
Related to the preceding point is a need to demonstrate an openness and transparency in taking forward EU mission-centred cancer activity. This will mitigate against the risk of an EU cancer mission being seen to have been formed, and operating, via a closed process, which again, may compromise the achievement of the widest possible support and endorsement.
ECCO therefore recommends the European Commission conduct at least one public consultation exercise in the early stages of progressing a cancer mission. This should outline the process undertaken so far towards mission selection, and seek views about the primary options for implementation under consideration. This can not only ensure the fullest informed process of delivery, but also canvass new ideas for implementation success and confirm and activate new supporters for delivery of the mission.
After selection, the importance of dynamic open information portals about the mission should not be understated. A cancer mission should, and will, excite the interest of the European public. Their likely thirst for information about progress, operation, and how to be involved in the mission should be actively responded to.
ECCO was founded by, and is sustained upon, the powerful shared sense of objective among all healthcare professionals working in cancer care: to improve outcomes for cancer patients via multidisciplinarity.3
So too with EU mission-centred cancer activity. No one professional group or stakeholder sector holds sufficient authority or opportunity to deliver landmark improvement by itself. Improvement in cancer care is delivered by teamwork.
ECCO urges that the frameworks for delivery of EU mission-centred cancer activity be embedded with a multidisciplinary and multistakeholder ethos from the outset. Governing components for delivering missions should be inclusive of differing perspectives, including the variety of concerned professional groups as well as patients. For this reason, we advise for a steering and/or advisory group for the mission composed of the range of disciplines and stakeholder audiences concerned.
We encourage EU mission-centred cancer activity to make strong use of reporting mechanisms for progress towards the goal. This will ensure clear lines of accountability for achievement are clearly inculcated.
ECCO recommends that within such reporting and accountability procedures:
Written published reports be made to the European Parliament every 6 months, with accompanying oral evidence
The individual in overall charge of delivery of an EU cancer-related mission be clearly identified to the outside world as such, and have no other responsibilities beyond the cancer mission
Reporting opportunities to the general public also be investigated, e.g. via open webcasts in which questions from the public can be taken and responded to
To avoid the EU cancer mission being divorced from national initiatives, reporting should also be considered to national parliaments and stakeholders.
While at the time of writing the precise choice of cancer mission is not yet known, it appears clear to ECCO that whatever the focus, to effect an improvement in cancer across all EU countries inevitably means addressing inequalities in healthcare provision and access in Europe, and helping systems to develop to standards required to achieve high performance goals and targets.
In short, we will not reach zero avoidable mortality for certain tumour types or patient groups, for example, without ensuring all countries have access to the range of tools required for this, be that strong prevention programmes, early diagnosis and screening programmes, the most effective treatment options, or high-functioning multidisciplinary teamwork and follow-up across sectors.
EU mission-centred cancer activity should therefore be aided by programmes of assistance in this regard. Without this, there is too great a risk that the mission may even exacerbate inequality in cancer care, with only some countries reaching the goal.
In summary, then, an EU Cancer Mission is an exciting, and indeed essential, move by the EU to show its power to effect life-changing improvements for citizens. We support EU mission-centred cancer activity with the fullest spirit of positivity. We offer advice, however, in the manner of delivery to ensure success from the outset. Beyond this, the ECCO community stands by to play its part in achieving inspiring results for the public and patient interest
Wallace N. Research ministers agree on broad themes for Horizon Europe missions, https://sciencebusiness.net/framework-programmes/news/research-ministers-agree-broad-themes-horizon-europe-missions (2019, accessed 21 March 2019).
Naredi P. The EU and cancer: it’s time for a bold vision Mr Juncker, https://www.ecco-org.eu/Global/News/Policy/2017/06/NEWS-The-EU-and-Cancer (2019, accessed 21 March 2019).
ECCO. About ECCO, https://www.ecco-org.eu/About-Ecco (2019, accessed 21 March 2019)
THE EUROPEAN CANCER PATIENT COALITION’S ROLE IN SECURING MEANINGFUL PATIENT INVOLVEMENT IN HEALTH TECHNOLOGY ASSESSMENT
Francesco de Lorenzo, Antonella Cardone, Alex Filicevas
European Cancer Patient Coalition, Brussels, Belgium
Access to new and innovative medicines remains one of the most significant inequalities across Europe. Cancer patients currently face the paradox of life-saving new medicines becoming available in Europe, yet not accessible to them, depending on which member state they reside in.1 While all cancer medicines must be authorised by the European Medicines Agency, based on evaluation of safety and efficacy data from clinical trials, for their marketing approval, Health Technology Assessment (HTA) and Pricing and Reimbursement (P&R) decisions are not centralised.
The therapeutic value of innovative medicines for patients, healthcare systems, and societies is determined by HTA. It is a valuable tool that can establish the real value of medicines, taking into consideration not only clinical impact, but also the quality of life (QoL) and social and societal impact. Maintaining or improving QoL can allow many patients to return to work and hence, in conjunction with extended survival, it can confer economic benefit to both patients and society.2
In the European Union, there are more than 50 national HTA bodies, all embedded in different institutional settings.3 Each member state decides individually which medicines should be reimbursed by the health systems, and at what price, attempting to balance the goal of improving access to innovative medicines with the need to ensure the sustainability of healthcare systems, and the efficiency of care.4 In this scenario, many cancer patients in the European Union still cannot access life-saving medicines.5
The European Cancer Patient Coalition (ECPC), established in 2003, is Europe’s largest cancer patient umbrella organisation, with over 450 cancer patient organisations in 46 countries. The ECPC vision is a Europe of equality, where all European cancer patients have timely and affordable access to the best treatment and care available throughout their life. The ECPC plays an essential role in Europe by effectively acting as the voice of cancer patients.6
The ECPC has extensively advocated for HTA harmonisation in the European Union. The ECPC white paper “Challenging the Europe of disparities,” launched in 2015, called for a harmonised HTA relative effectiveness assessment as a potential to reduce workload, create efficiencies, and underpin speedier patient access to life-preserving medicines by reducing delays.7
The ECPC has created momentum on EU cooperation in HTA during the process of amending the regulation 726/2004, “laying down Community procedures for the authorisation and supervision of medicinal products for human and veterinary use and establishing a European Medicines Agency,” when the proposed amendments were voted by the European Parliament in March 2016.
The European Cancer Patient Coalition’s advocacy milestones. ENVI: European Parliament’s Committee on Environment, Public Health and Food Safety; EP: European Parliament; HTA: Health Technology Assessment.
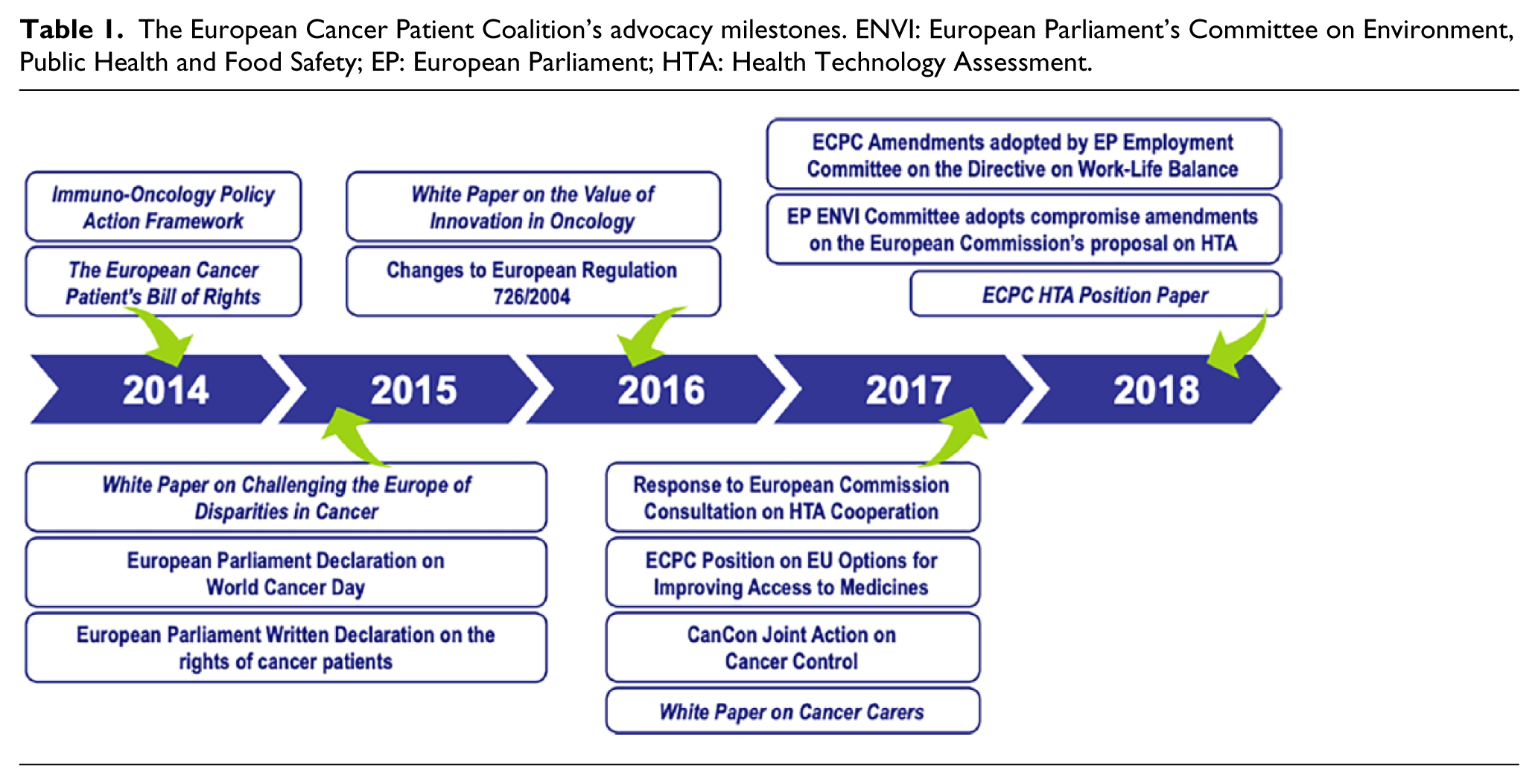
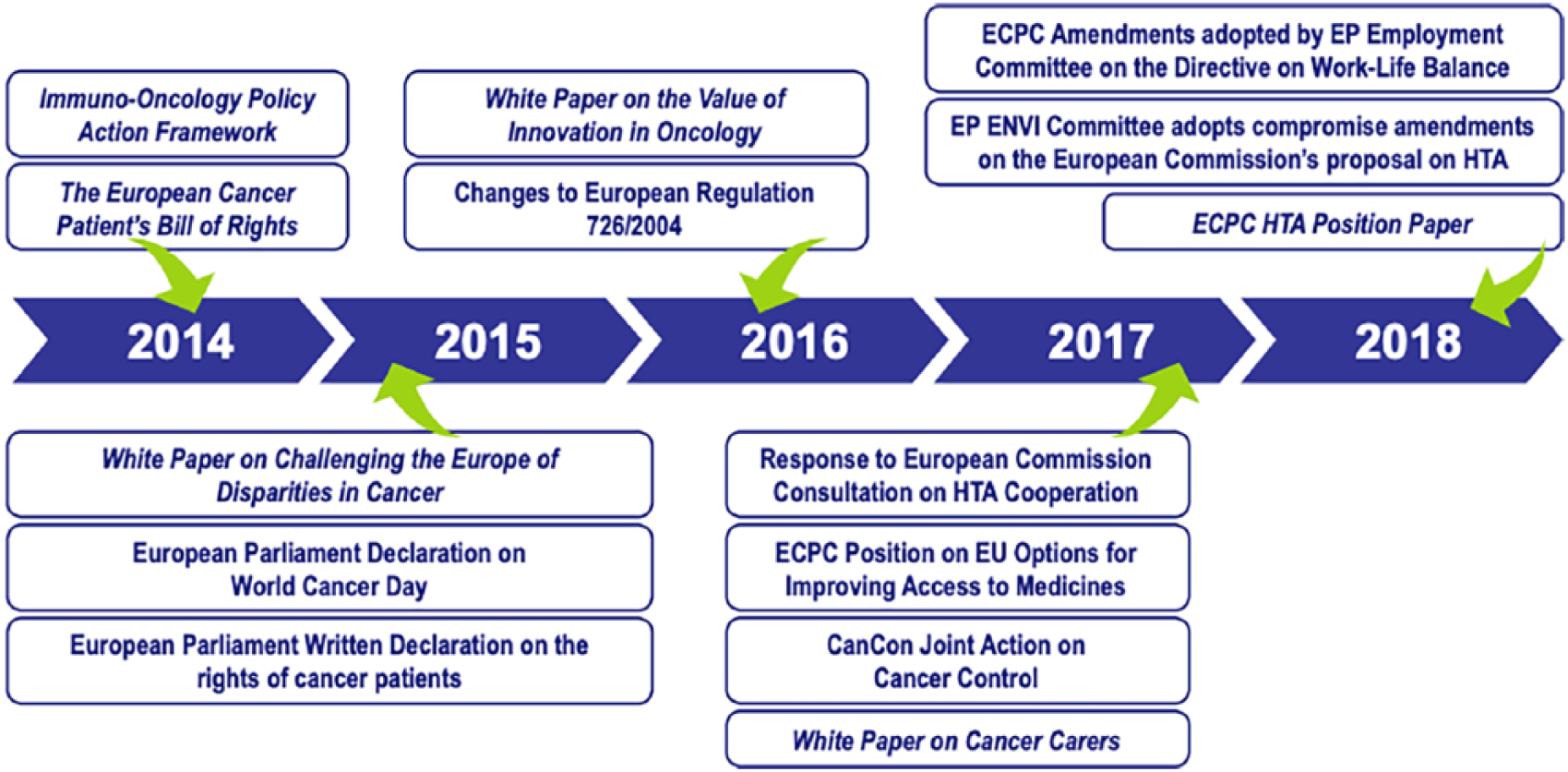
The ECPC response to the European Commission (EC)’s 2017 consultation on “Strengthening of the EU cooperation on health technology assessment” stated that increased EU cooperation will not only significantly reduce costs and duplication across HTA bodies, but decrease delays in access to innovative medicines, facilitate participation of patient organisations in the HTA decision-making process, and facilitate access to market.8
The significant variations in decision-making made by EU national governments, twinned with the lack of a harmonised HTA policy, result in unacceptable delays.9 If current P&R methods remain as they are, patient access to innovative treatments such as immunotherapy and biologics, new biomarker testing methodologies, and companion diagnostic kits will continue to face difficulties.10
In January 2018, the EC set out a proposal on the joint work on clinical aspects of HTA, which are typically based on global evidence, while the nonclinical aspects remain at member state level (see Table 2).11 This framework is called the Joint Clinical Assessments (JCAs), which paired with nonclinical assessment would inform the real value of medicine for P&R at member state level. The EP has already unanimously approved its position in February 2019 and strongly supports the EU JCAs.
HTA Core Model domains as developed by the EUnetHTA Joint Action.
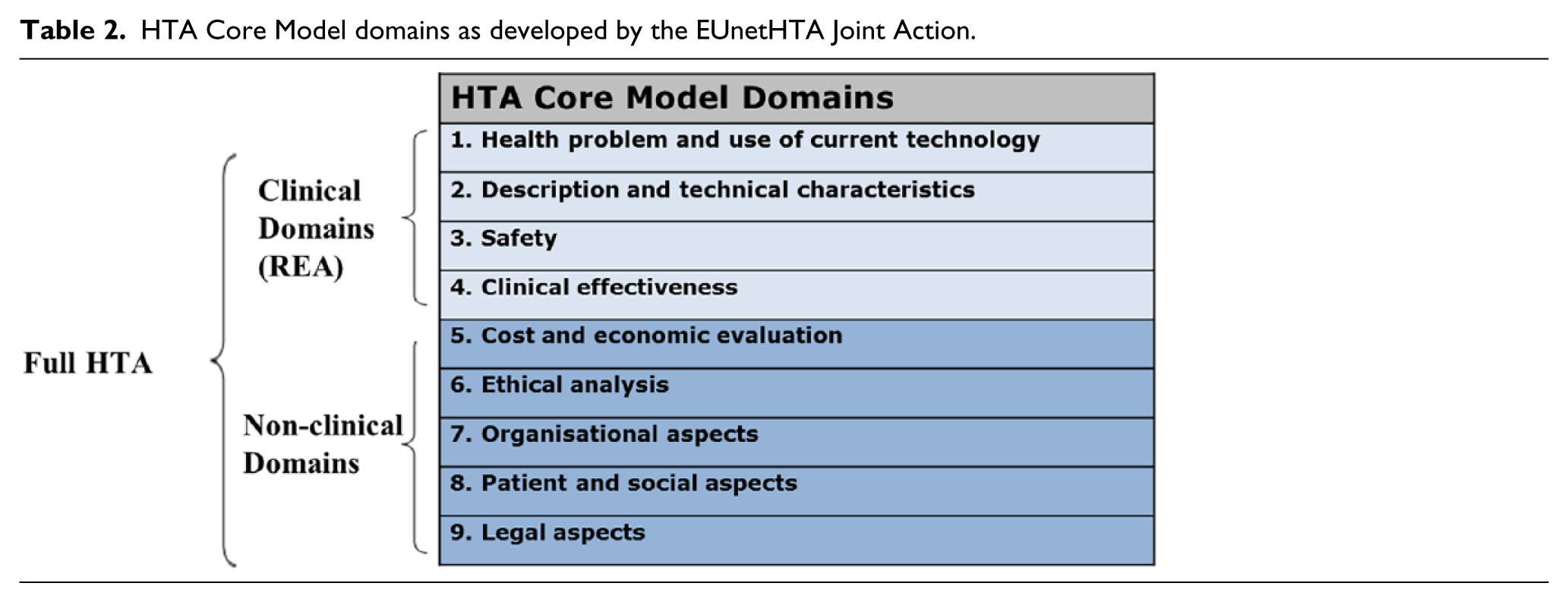
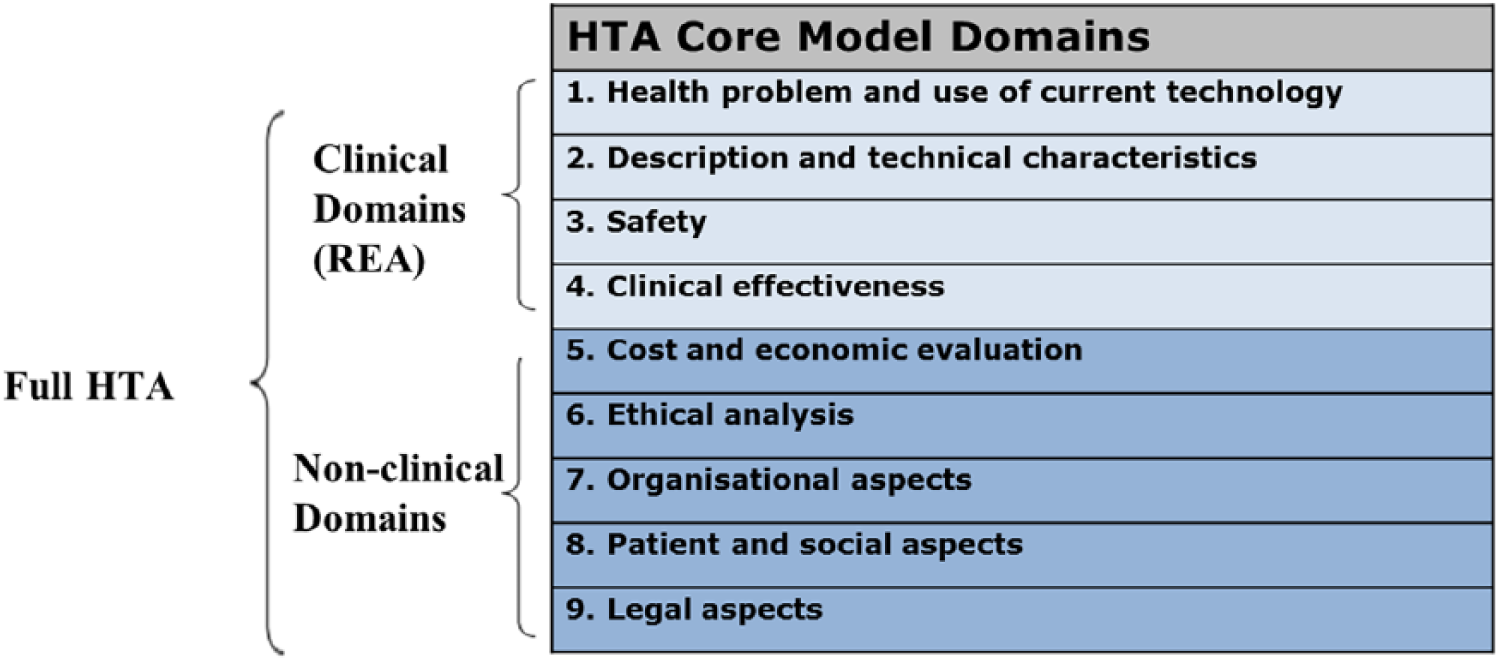
The challenge remains with member states. Up to now, what is established in the proposed EU regulation was not welcomed by all member states, several of which have expressed strong reservations in the mandatory uptake of the JCA reports.12 The Romanian Presidency of the Council of the EU has focused on moving forward to an agreement on other aspects of the regulation.
Patient involvement in the HTA at the national level must be mandatory, due to legal, ethical, patient, and social aspects, which are evaluated for pricing and reimbursement. It is increasingly recognised that patients can contribute to the HTA process in 2 areas: the experience of living with the particular condition that the new technology is intended to treat and preferences for general therapeutic approaches or specific attributes of the technology.13
The ECPC has led a campaign to support increased harmonisation on HTA across Europe, and for patients and their representatives to be formally and routinely included in HTA policy and operations.14
The HTA must better capture patient-derived evidence about how they feel, function, and live their lives, and derive a standardised, relevant, and acceptable assessment of this experience that goes beyond clinical efficacy.15 A new medicine with equal efficacy to an existing standard of care may not offer added value from a clinical perspective, but it may offer significant improvement on patients’ QoL and thus provide added value to the patient.
National HTA agencies generally lack patient involvement and some countries such as Denmark, England, Germany, Scotland, Sweden, and the Netherlands have structured meaningful patient engagement in the HTAs.15 It should be considered that best practices for patient engagement in HTAs already exist in some member states, but also overseas in Australia and Canada.
The political will to harmonise HTAs is crucial to enable real change. As member states continue to work in the Council of the European Union on coming to an agreement, there is an immediate need for stronger and empowered patient organisations at national level. The ECPC strives to enable these organisations to urge national policymakers to protect cancer patients’ right to participate in HTAs, and advocate for a formalised framework of patient involvement in the EU HTA, at national and regional levels.
In view of this, in 2019, the ECPC launched an online educational module on HTA.16 The module covers a range of information including medicines development process and their examination as part of HTA, why cancer treatments might be reimbursed in some countries but not in others, and how cancer patient organisations can get involved in the HTA.
de Lorenzo F, Apostolidis K. The European Cancer Patient Coalition and its central role in connecting stakeholders to advance patient-centric solutions in the mission on cancer. Mol Oncol 2019; 13: 653–666.
European Cancer Patient Coalition. The Value of Innovation in Oncology, http://ecpc.org/innovation (2017, accessed 25 March 2019).
European Commission. Inception Impact Assessment: Strengthening of the EU cooperation on Health Technology Assessment (HTA). Brussels: European Commission; 2016.
European Cancer Patient Coalition. The Value of Innovation in Oncology, http://ecpc.org/innovation (2017, accessed 25 March 2019).
European Cancer Patient Coalition. Challenging the Europe of disparities in cancer: a framework for improved survival and better quality of life for European cancer patients, http://www.ecpc.org/da/activities/policy-and-advocacy/policy-initiatives/europe-of-disparities (2019, accessed 25 March 2019).
European Cancer Patient Coalition. Vision, Mission & Strategy, http://www.ecpc.org/da/about-us/vision-strategy (accessed 25 March 2019).
European Cancer Patient Coalition. Europe of Disparities, http://www.ecpc.org/da/activities/policy-and-advocacy/policy-initiatives/europe-of-disparities (2019, accessed 25 March 2019).
European Commission. Online Public Consultation Report: Strengthening of the EU Cooperation on Health Technology Assessment (HTA). Brussels, Belgium: European Commission; 2016.
Ades F, Senterre C, Zardavas D, et al. An exploratory analysis of the factors leading to delays in cancer drug reimbursement in the European Union: the trastuzumab case. E J Cancer 2014; 50: 3089–3097.
Lorenzo F, Apostolidis K. The European Cancer Patient Coalition and its central role in connecting stakeholders to advance patient-centric solutions in the mission on cancer. Mol Oncol 2019; 13: 653-666.
European Commission. Proposal for a Regulation of the European Parliament and of the Council on Health Technology Assessment and Amending Directive 2011/24/EU. Brussels: European Commission; 2018.
Council of the European Union. Presidency Progress Report on the Proposal for a Regulation on Health Technology Assessment. Brussels: Council of the EU; 2018.
Facey K, Boivin A, Gracia J, et al. Patients’ perspectives in health technology assessment: A route to robust evidence and fair deliberation. Int J Technol Assess Health Care 2010; 26: 334–340.
European Cancer Patient Coalition. ECPC Position on Future Cooperation on Health Technology Assessment, http://ecpc.org//Documents/ECPC_HTA_Position_Paper_July2018.pdf (2018, accessed 25 March 2019).
Facey K, Hansen H, Single A. Patient Involvement in Health Technology Assessment. Singapore: Springer Nature; 2017.
European Cancer Patient Coalition. Patient Organisations in the Assessment of Cancer Treatments, http://ecpc.org/edu/hta (2019, accessed 25 March 2019).
DATA SHARING AS A CONTINUUM TO THE ROLE OF INTERNATIONAL NETWORKS: BEYOND CLINICAL RESEARCH
Denis Lacombe
Director, General EORTC Headquarters, Brussels, Belgium
Multi-institutional, international, and independent clinical trials have been instrumental in pushing the boundaries of knowledge, establishing new standards of care, and improving survival and quality of life of cancer patients.1 For the last 50 years, the European Organisation for Research and Treatment of Cancer (EORTC) has contributed to such advances. This progress has been made possible through the conduct of multidisciplinary trials that address day-to-day clinical challenges. They are designed to answer clinically relevant endpoints, for frequent or rare tumours as well as specific populations, leaving no patient behind. EORTC has a track record in melanoma, neuro-oncology, sarcoma, lung cancer, and many others. Organisations like EORTC have accumulated historical datasets that represent wealth for research. Over the years, the evolution of the technologies as well as the integration of translational research into clinical trials have enriched existing datasets with biological and imaging data that continue to build up as complex trials continue to develop. Data sharing therefore cannot be dissociated from the evolving role of independent networks in society and in revisited healthcare systems. The technological revolution has led to new types of clinical trials, generating different and multidimensional datasets that require novel bioinformatics solutions for appropriate interpretation.
However, the fragmentation of clinical datasets across different commercial and noncommercial stakeholders is an impediment to knowledge development, notably to address the patterns of relapse and resistance to numerous multiple agents being made available, often with limited intrinsic values. Therapeutic progress calls naturally to swift exchange of datasets but existing competing forces at both the commercial and noncommercial stakeholders tend to protect these sets from hypothesized future research which may or may not happen.2 Before anticipating what may be an optimal framework for data sharing, it may be valuable to develop views on what is the role of independent networks in the continuum of clinical research, to structure new datasets in a re-engineered environment. New types of datasets such as large screening platforms to address the biology of the cancer to late trials into healthcare systems, together with the collection of human biological material, force the various stakeholders to re-address completely their role in an ecosystem which is more interoperational, based on data agility. While data are infinite, biological samples are finite, and therefore sharing principles raise different challenges.3 The stakeholders must leave their comfort zone to create new workable trustworthy zones. EORTC has developed a data-sharing policy offering access to its collections: since 2001, 310 data-sharing exercises (recipients) conducted on 261 datasets and which have been shared 568 times.
Leveraging existing datasets should be seen as an opportunity to pay tribute to patients who volunteered for clinical trials.4 New vision on existing datasets can lead to new hypothesis and innovation. Nevertheless, data-sharing has proven to be a challenging exercise. Prompted by the International Committee of Medical Journal Editors (ICMJE),5 many organisations have implemented data-sharing policies. The challenges raised by dataset holders lie in appropriate use of datasets and proposed methodologies by requestors, protecting ethics of sensitive information under the General Data Protection Regulation (GDPR). Managing activities such as data sharing is not cost-free, and it implements the paths for decision process.6
Finally, incentives to share data are often lacking. It has been claimed that there is no regulatory or technical difficulty in sharing datasets, but the reluctance to share some or all of the datasets could be due to the lack of incentives and the fear of sharing.7
Managed access procedures seem the most suitable approach to embrace the challenges of data sharing. They should be reasonable and proportionate in the respect of patients and their informed consent, allowing a certain priority to those who generated the concerned datasets but in all cases must maximise timely availability to all potential researchers to improve knowledge and standards of care.
EORTC regulates access to data and biological material through 2 specific policies, and a 3rd policy addressing protection of personal data. While the clinical database is held at the EORTC HQ, the samples are centralized at Integrated BioBank of Luxembourg and omics data are stored at the European Genomic Archives (EGA).
The processes are organized in different conditions: EORTC HQ is the legal sponsor for its studies that act as gatekeeper. Within the GDPR, a careful balance between data controller and processor has been implemented in data and material transfer agreements. The operationalization was made possible by transforming the notion of ownership into a controlled process to guarantee the chain of custody, documented through a series of verifiable standard operating procedures.
Facilitating exchange of datasets between researchers but also across stakeholders requires environments that provide ethical, regulatory, quality, and methodologic assurance of the data process. The challenge is data structuring.
The platforms that support the structuring of data inside and outside of clinical trials, in particular at the time of precision oncology and real-world tests, are indispensable for facilitating the data exchange to all researchers. For example, the demonstration of this compliant environment has led EORTC to acquire vast series of pharmaceutical data (clinical data and biological materials) to further develop the science.8 Some companies have used equivalent environments to share their datasets.9
Recently, ASCO led a consensus meeting for a Clinical Trial Data Sharing Policy Among Oncology Journals.10 The main conclusions of this event highlighted first the lack of awareness of data archives and the need to develop incentives for researchers. It also emphasized that common global standards would be needed to access all the places where they reside, as well as guidelines for administration and governance, while addressing the financial burden.
Proposals for tiered model to share clinical trial data and samples have been presented by EORTC,11 as well as patient perspectives. Though sharing biological materials may require an additional level of review to ensure the proper use of finite material, data and materials sharing should optimally benefit from fully open access models. However, in practice, legal, ethical, and operational standards make full open access unfeasible. Duties under Good Clinical Practices and GDPR lead to responsibilities that remain in the remit of the sponsor. Controlled access allows, within knowledgeable environments, appropriate data sharing solutions. The additional flexibility, although limited to clinical data, is the use of completely anonymous datasets with greater regulatory agility, but with the inability to efficiently reconnect patients to medically applicable findings.
Whatever the solution might be, it is crucial that the scientific community tackles precisely the problems that are yet to be solved.12 Data sharing may be applicable to divergent datasets that contribute differently to the drug development process and to clinical research in general. The stakeholder role should be redefined according to a continuum in which the patient is at the centre from beginning to end. A new type of dataset, generated in early or late clinical trials, should be placed in a public health improvement perspective and where datasets could be re-interrogated indefinitely in the context of the new science.
Bertagnolli MM, Sartor O, Chabner BA, et al. Advantages of a truly open-access data-sharing model. N Engl J Med 2017; 376: 1178–1181.
Rosenbaum L. Bridging the data-sharing divide: seeing the devil in the details, not the other camp. N Engl J Med 2017; 376: 2201–2203.
Longo DL, Drazen JM. Data sharing. N Engl J Med 2016; 374: 276–277.
Sarpatwari A, Kesselheim AS, Malin BA, et al. Ensuring patient privacy in data sharing for postapproval research. N Engl J Med 2014; 371: 1644–1649.
Taichman DB, Backus J, Baethge C, et al. Sharing clinical trial data: a proposal from the International Committee of Medical Journal Editors. Rev Med Chil 2016; 144: 11–13.
Kiley R, Peatfield T, Hansen J, et al. Data sharing from clinical trials: a research funder’s perspective. N Engl J Med 2017; 377: 1990–1992.
Bierer BE, Crosas M, Pierce HH. Data authorship as an incentive to data sharing. N Engl J Med 2017; 376: 1684–1687.
Press release: GSK Vaccines to transfer tumour samples and data to the European Organisation for Research and Treatment of Cancer/EORTC, https://www.eortc.org/blog/2018/07/30/press-release-gsk-vaccines-to-transfer-tumour-samples-and-data-to-the-european-organisation-for-research-and-treatment-of-cancer/ (2018, accessed March 5, 2019).
Ross JS, Waldstreicher J, Bamford S, et al. Overview and experience of the YODA Project with clinical trial data sharing after 5 years. Sci Data 2018; 5: 180268.
Simon G, Initiative C, Drazen JM. ASCO convenes stakeholders to build consensus for a clinical trial data sharing policy among journals that publish clinical cancer research, https://connection.asco.org/magazine/society-member-news/asco-convenes-stakeholders-build-consensus-clinical-trialdata-sharing (2019, accessed 5 May 2019).
Broes S, Lacombe D, Verlinden M, et al. Toward a tiered model to share clinical trial data and samples in precision oncology. Front Med 2018; 5: 6.
Broes S, Lacombe D, Verlinden M, et al. Sharing human samples and patient data: opening Pandora’s box. J Cancer Policy 2017; 13: 65–69.
RADIOTHERAPY: SEIZING THE OPPORTUNITY IN CANCER CARE
Joanna Kazmierska1, Núria Jornet Sala2, Michelle Leech3, Chiara Gasparotto4, Barbara Alicja Jereczek-Fossa5, Yolande Lievens6, Umberto Ricardi7, John Yarnold8
1Greater Poland Cancer Centre, Poznan, Poland, 2Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 3Trinity College Dublin, Ireland, 4European Society for Radiotherapy and Oncology, Brussels, Belgium, 5Department of Oncology and Hemato-oncology of University of Milan and Department of Radiation Oncology of IEO European Institute of Oncology IRCCS, Milan, Italy, 6Radiation Oncology Department, Ghent University Hospital, Past-President, European Society for Radiotherapy and Oncology, Belgium, 7Department of Oncology, University of Turin, Turin, Italy, President, European Society for Radiotherapy and Oncology, Belgium, 8John Yarnold, Institute of Cancer Research, London, UK
The incidence of cancer is increasing, resulting in a rising demand for high-quality cancer care. In 2018, there were close to 4.23 million new cases of cancer in Europe, and this number is predicted to rise by almost a quarter to 5.2 million by 2040.1 This growing demand poses a major challenge to healthcare systems and highlights the need to ensure all cancer patients have access to high-quality, efficient cancer care.
To tackle this challenge, a European Cancer Mission is needed. This collaborative effort can bring together all the diverse stakeholders involved in the oncology scenario, putting the patient at the centre and defining common goals. The research community, the European institutions, and member states need to join forces and share a common vision, shaping collaborations to save lives and improve the quality of life of cancer survivors. With this spirit, the European Society for Radiotherapy and Oncology (ESTRO) Vision is “Radiation oncology: Optimal health for all, together.”2
Fundamental principles are at the core of the ESTRO Vision: value, inclusiveness, collaboration. Considering the ESTRO Vision as one of the building blocks of a European Cancer Mission, and expanding those fundamental principles to whole oncology care, we urge the community to go beyond the concept of curing cancer. “Optimal” relates to what matters to patients, not only in terms of cancer outcome in the broad sense, but also considering all other aspects that impact on the patients’ well-being and quality of life.3 The term “for all” highlights the need to be inclusive: on one side, ensuring that all patients, despite where they are and who they are, have access to the care they need, and on the other side, considering the whole cancer care pathway, ensuring multidisciplinary and multiprofessional care, collaboration, and appropriate communication, by breaking silos. Finally, “together” encourages stakeholders to build partnerships, covering the whole spectrum of optimal health: oncology societies, other health care professionals and organisations, healthcare providers, patients, industry, research organisations, and policymakers.
Radiation oncology is a key component of the solution that the European Cancer Mission should define.
With the growing demand for high-quality cancer care, we need to ensure that we are focusing on what offers the greatest benefit to patients. Based on the theory of value-based healthcare,3,4 health systems should maximise patients’ outcome, defined as the health outcome per dollar spent. The concept of a European Cancer Mission should create value for the patient, defined as the ability to receive the best possible treatment, and therefore increase the chances of surviving and optimising quality of life during and after treatment.
Radiotherapy is central in cancer cure.5 There is evidence that 40% of all cancers cured are eliminated by radiotherapy, either alone or acting in combination with other types of treatment.6 It is recommended as part of the treatment approach for more than 50% of cancer patients.7,8 However, there is a gap to be filled: at least 1 person in 4 needing radiotherapy does not receive it8 and at the same time, the demand for radiotherapy is expected to grow by 16% by 2025.9 Closing the gap in access to radiotherapy means saving lives and contributing to the eradication of cancer. If, by 2035, every cancer patient who needs radiotherapy has access to it, almost 1 million more lives will be saved every year worldwide.10
The cost of care is also an aspect that a common cancer mission should focus on. Value needs to be ensured for the healthcare system, an increasingly important consideration, if we look at the competing demands on limited financial resources. There is strong evidence that radiotherapy is a sound investment for healthcare systems. If we used radiotherapy to match demand, there would be a return of up to €5 for every €1 invested by 2035, depending on the model of care being adopted.10 While it requires a well-planned initial investment in equipment, infrastructure, and training, the long-term costs are low.10
Being a cornerstone of modern cancer treatment, radiotherapy should be a fundamental part of the common European Cancer Mission. In order to create value for the many citizens that are and will be in need of radiotherapy, barriers to the provision of optimal care to the patient, and specifically to the provision of radiotherapy, should be identified and overcome.
A European Cancer Mission can engage all stakeholders, from the scientific community to the policymakers, in signing off on common principles and ensuring that the focus on cancer is a priority for all. The scientific society also needs to define clear objectives and key questions.
ESTRO would like to highlight the need for appropriate positioning of radiotherapy within cancer policies, national cancer control plans, and models of care for the benefit of patients, today and tomorrow. To this end, ESTRO proposes a 5-point plan,11 defining how collaboration can ensure that all cancer patients who need it have access to high-quality radiotherapy as part of their care, whoever they are and wherever they live.
The European Cancer Mission should ensure the following:
1)
A common European Cancer Mission needs to ensure that radiotherapy is positioned appropriately in national cancer control plans and cancer policies. Additionally, funding is required to build and maintain capacity across Europe in technology and skilled personnel to ensure all patients who need it have access to high-quality radiotherapy, along with the promotion of innovation. Finally, national audits and usage of data on service utilisation have to serve the improvement of the future capacity planning and mitigate the impact of low resources on patients (e.g. long waiting times).
2)
A common European Cancer Mission has to ensure the roles of all radiotherapy professionals, along with the required qualifications, and mandate shared standards for education and training across Europe for all radiotherapy professionals to ensure employability and mobility of professionals between countries. Consistent training for all professionals has to be promoted, using the ESTRO core curricula,12 to ensure all professionals deliver evidence-based, best-practice care.
3)
A common European Cancer Mission should advocate for radiotherapy in European and national research agendas, focusing on outcomes important to all patients (both in the curative and palliative setting), as well as improvements in service delivery. International research collaborations need to be facilitated, aiming at scaling up of clinical trials, preclinical studies, and obtaining meaningful evidence of the clinical and economic impact of new treatment approaches in a range of settings and populations. The use of real-world data and big data analysis has to be expanded, to enable timely health technology assessment for innovative radiotherapy technologies. Innovation must be supported, ensuring that radiotherapy improve even further its efficacy and allow even more patients to benefit from effective, precise, and safe treatment.
4)
A common European Cancer Mission has to ensure, though education and collaborations, an acknowledgement and understanding of the role of radiotherapy and its integration into multidisciplinary treatment and decision-making.
5)
A common European Cancer Mission should focus on communication of relevant information to patients about radiotherapy, to help dispel myths and enhance their understanding of what to expect from treatments.
It is timely that governments, professional societies, patients and their representatives, all healthcare professionals, and the research community work together towards common goals. ESTRO believes that enabling stakeholders at European level and worldwide to define the desired changes and the efforts needed is essential for effective and efficient multidisciplinary cancer care.
International Agency for Research on Cancer. Global Cancer Observatory: 2018 Cancer tomorrow: Cancer Incidence and Mortality Worldwide: IARC CancerBase, http://gco.iarc.fr/tomorrow/ (2018, accessed 18 September 2018).
Lievens Y, Ricardi U, Poortmans P, et al. Radiation oncology: optimal health for all, together: ESTRO Vision, 2030. Radiother Oncol (in press 2019).
Lievens Y, Audisio R, Bansk I, et al. Towards an evidence-informed value scale for surgical and radiation oncology: a multi-stakeholders perspective. Lancet Oncol 2019; 20: e112–e123.
Porter ME. What is value in health care? N Engl J Med 2010; 363: 2477–2481.
Hanna TP, Shafiq J, Delaney GP, et al. The population benefit of evidence-based radiotherapy: 5-year local control and overall survival benefits. Radiother Oncol 2018; 126: 191–197.
Department of Health Cancer Policy Team. 2012 Radiotherapy Services in England 2012. London: Department of Health; 2012.
Borras JM, Barton M, Grau C, et al.. The impact of cancer incidence and stage on optimal utilization of radiotherapy: methodology of a population based analysis by the ESTRO-HERO project. Radiother Oncol 2015; 116: 45–50.
Borras JM, Lievens Y, Dunscombe P, et al. The optimal utilization proportion of external beam radiotherapy in European countries: an ESTRO-HERO analysis. Radiother Oncol 2015; 116: 38–44.
Borras JM, Lievens Y, Barton M, et al. How many new cancer patients in Europe will require radiotherapy by 2025? An ESTRO-HERO analysis. Radiother Oncol 2016; 119: 5–11.
Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol 2015; 16: 1153–1186.
Joanna Kazmierska, Núria Jornet Sala, Michelle Leech, Barbara Alicja Jereczek-Fossa, Yolande Lievens and John Yarnold. RADIOTHERAPY: seizing the opportunity in cancer care. Online Referencing https://mariecurielegacy.org/wp-content/uploads/2018/11/Radiotherapy_seizing_the_opportunity_in_cancer_care.pdf (2018, accessed 5 May 2019).
Eriksen JG, Beavis AW, Coffey MA, et al. The updated ESTRO core curricula 2011 for clinicians, medical physicists and RTTs in radiotherapy/radiation oncology. Radiother Oncol 2012; 103: 103–108.
THE ESSENTIAL ROLE OF PREVENTION IN REDUCING THE CANCER BURDEN IN EUROPE: A COMMENTARY FROM CANCER PREVENTION EUROPE
Carolina Espina1, Linda Bauld2,3, Bernardo Bonanni4, Hermann Brenner5, Karen Brown6, Joakim Dillner7, Ellen Kampman8, Mef Nilbert9, Paolo Vineis10, Matty P. Weijenberg11, Alison Cox3, Theo M. de Kok11, Daniela Fecht10, Giota Mitrou12, David C Muller10, Davide Serrano4, Karen Steindorf5, Hans Storm9, Mangesh A. Thorat6,13, Fränzel van Duijnhoven8, Elisabete Weiderpass1, Joachim Schüz1
1International Agency for Research on Cancer (IARC/WHO), Lyon, France, 2Usher Institute, College of Medicine and Veterinary Medicine, University of Edinburgh, 3Cancer Research UK, London, United Kingdom, 4European Institute of Oncology, Milano, Italy, 5German Cancer Research Center (DKFZ), Heidelberg, Germany, 6UK Therapeutic Cancer Prevention Network, Leicester Cancer Research Centre, University of Leicester, United Kingdom, 7Karolinska University Laboratory, Karolinska University Hospital, Stockholm, Sweden, 8Division of Human Nutrition and Health, Wageningen University, Wageningen, the Netherlands, 9Danish Cancer Society, Copenhagen, Denmark, 10MRC-PHE Centre for Environment and Health, School of Public Health, Imperial College, Norfolk Place, London, United Kingdom, 11GROW School for Oncology and Developmental Biology, Maastricht University, Maastricht, the Netherlands, 12World Cancer Research Fund International, London, 13UK Therapeutic Cancer Prevention Network. Centre for Cancer Prevention, Wolfson Institute of Preventive Medicine, Queen Mary University of London, London, United Kingdom
The potential of cancer prevention
In 28 out of 40 United Nations–defined European countries, cancer is now the leading cause of premature death and the second most common in the other 12, with a total of 1.93 million deaths and 3.91 million new incident cases in 2018.1 Those numbers are projected to rise to 2.55 million deaths and 4.75 million incident cases in Europe by 2040, as a result of population aging and growth, representing an overall increase in numbers of deaths by 32%.2 Notably however, these estimates are based on prediction models taking current incidence rates and time trends into consideration, so that preventive actions taken today could change this forecast, i.e. lead to lower than those expected numbers. The cancer cost in 27 countries in the European Union in 2009 was €126 billion, 60% incurred in non-healthcare areas, with almost €43 billion in lost productivity due to early death. Of the 4 cancers studied, lung cancer had the highest economic burden.3
Cancer prevention has a broad scope, encompassing primary, secondary, and tertiary prevention, and research in this domain ranges from the submicroscopic study of the mechanisms of carcinogenesis to the supramacroscopic analysis of the “causes of the causes,” also known as the social determinants of health.4 Recent studies from France, the United Kingdom, and Germany have estimated that around 40% of cancers in these countries could be prevented.5-9 Established means of primary prevention include legislation and policies (e.g. on tobacco, alcohol, or hazardous agents), vaccination programmes (e.g. human papilloma virus or hepatitis B), and education about healthy lifestyles and behaviours (e.g. tobacco, alcohol, diet, and UV exposure), as well as other risk-adapted medical prevention strategies (e.g. tamoxifen or aspirin). By cancer type, a proportion of 75% to 100% of all cancers of the lung, cervix, oesophagus, oral cavity, melanoma, and stomach in Europe are suggested to be preventable as a consequence of changes in established risk and protective factors; similarly, 25% to 74% of all colorectal, bladder, kidney, liver, uterus, pancreas, and breast cancers are potentially preventable.10 Primary prevention synergistically benefits other noncommunicable diseases by reducing exposures to shared risk factors, creating healthy environments for current and future generations.11,12 Secondary prevention or early detection through organized screening programmes can significantly reduce mortality from breast, cervical, and colorectal cancers, as well as incidence of cervical and colorectal cancers13; however, implementation of secondary prevention in Europe is scattered, as recently assessed.14 Tertiary prevention refers to care aimed at reducing morbidity, disability, and risk of second primary cancer, as well as at restoring function, and improving quality of life and participation in society in people diagnosed and being treated for cancer. The potential to expand preventive interventions remains large and the evidence base for a number of measures has been summarised in the 4th edition of the European Code against Cancer (ECAC) (http://cancer-code-europe.iarc.fr/index.php/en/).15 The ECAC is an integrated instrument for cancer prevention that informs the general public how to avoid or reduce exposures to established causes of cancers, to adopt behaviours to reduce cancer risk, and to participate in vaccination and screening programmes under the appropriate national guidelines. It also acts as a guide to aid development of national health policies in cancer prevention, as it has been shown by the adoption of the ECAC-proposed structure in the comprehensive National Cancer Plans of several European countries.16
Cancer Prevention Europe
Research is required to provide new evidence-based preventive interventions (including the continued search for additional causes of cancer) and to understand the factors that hamper their implementation within health care systems and in the community. In 2018, the international and multidisciplinary consortium Cancer Prevention Europe (CPE) was created to develop world-class prevention research to be translated into effective cancer prevention guidelines and policies at the national and international level.10,17 CPE is a consortium of leading European research institutions committed to prioritising cancer prevention through cooperation between countries and programmes in order to ensure a dedicated research agenda with long-term vision, and sustainable funding and infrastructure for such research. CPE will focus on expanding preventive interventions and strengthening cancer prevention in Europe by increasing awareness of the needs, the associated required resources, and reducing inequalities in access to cancer prevention across Europe.18 CPE will be broad in scope, covering a spectrum of research from human studies and laboratory science to policy research, as well as dissemination of the best evidence, quality indicators, and practices used. Assessment of the cost-effectiveness of different interventions, in relation to costs of treatment, care, and productivity loss will be a core component of the initiative. Emphasis will also be placed on the evaluation of the impact of preventive interventions (primary, secondary, and tertiary) and advocacy dimensions of the prevention agenda. The agenda for CPE includes (1) research into optimising the implementation of known preventive strategies (implementation research), (2) dissemination and research translation to inform policy and practice (advocacy), and (3) the identification of novel risk factors and targets for prevention (improvement and expansion). This agenda will be supported by a range of platforms, networks, and infrastructures and will draw together a wide network of partners. Training and capacity building will be integral to the initiative.
Cancer mission for Europe
Europe is heavily fragmented in all aspects of cancer burden. Cancer incidence varies considerably across European countries, partially due to differing risk factor prevalence and stages of implementation of primary prevention18; this is especially evident in the case of tobacco smoking.19 Even in countries at the forefront of cancer awareness, around 40% of cancers could be prevented; instead, numbers continue to rise.20 Cancer survival and mortality differs between European countries,21,22 as well as within countries across socioeconomic groups,23 even in a country of high social welfare such as Denmark.24 Cancer is not just a common cause of death but comes with physical suffering for the patient and psychological suffering for patients and their families, not counting the economic burden of €102 per citizen, as was estimated in 2009 for the European Union.3 A Europe-wide cancer prevention mission to strengthen and join forces in primary and secondary prevention, as well as tertiary prevention, diagnosis, and treatment, and palliative care, well-resourced for significant improvements in all regards, is timely and urgently needed to reduce the growing cancer burden in Europe. Cancer Prevention Europe has been founded to be one of the major drivers of such a mission.
Acknowledgements
Secretariat of and projects conducted by Cancer Prevention Europe are supported by the Cancer Prevention Europe member institutions. The authors thank Drs. Christopher P. Wild (former Director of IARC) and David Forman (IARC) for their roles in launching Cancer Prevention Europe.
Ferlay J, Colombet M, Soerjomataram I, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer 2018; 103: 356–387.
Global Cancer Observatory, International Agency for Research on Cancer, http://gco.iarc.fr/ (2018, accessed 10 February 2019).
Luengo-Fernandez R, Leal J, Gray A, et al. Economic burden of cancer across the European Union: a population-based cost analysis. Lancet Oncol 2013; 14: 1165–1174.
World Health Organisation, Commission on the Social Determinants of Health. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health: Final Report of the Commission on Social Determinants of Health. Geneva: World Health Organisation; 2008.
Soerjomataram I, Shield K, Marant Micallef C, et al. Cancers related to lifestyle and environmental factors in France in 2015. Eur J Cancer 2018; 105: 103–113.
Brown KF, Rumgay H, Dunlop C, et al. The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br J Cancer 2018; 118: 1130–1141.
Behrens G, Gredner T, Stock C, et al. Cancers due to excess weight, low physical activity, and unhealthy diet. Dtsch Arztebl Int 2018; 115: 578–585.
Gredner T, Behrens G, Stock C, et al. Cancers due to infection and selected environmental factors. Dtsch Arztebl Int 2018; 115: 586–593.
Mons U, Gredner T, Behrens G, et al. Cancers due to smoking and high alcohol consumption. Dtsch Arztebl Int 2018; 115: 571–577.
Forman D, Bauld L, Bonanni B, et al. Time for a European initiative for research to prevent cancer: a manifesto for Cancer Prevention Europe (CPE). J Cancer Policy 2018; 17: 15–23.
United Nations General Assembly resolution 66.2, 66th session, New York, 24 January 2012, Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases (A/RES/66/2).
World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: a Global Perspective. Continuous Update Project Expert Report 2018. London: World Cancer Research Fund/American Institute for Cancer Research; 2018.
Armaroli P, Villain P, Suonio E, et al. European Code Against Cancer, 4th edition: cancer screening. Cancer Epidemiol 2015; 39 Suppl 1: S139–S152.
Basu P, Ponti A, Anttila A, et al. Status of implementation and organization of cancer screening in the European Union Member States: summary results from the second European screening report. Int J Cancer 2018; 142: 44–56.
Schüz J, Espina C, Villain P, et al. European Code Against Cancer 4th edition: 12 ways to reduce your cancer risk. Cancer Epidemiol 2015; 39 Suppl 1: S1–10.
Espina C, Soerjomataram I, Forman D, et al. Cancer prevention policy in the EU: best practices are now well recognised; no reason for countries to lag behind. J Cancer Policy 2018; 18: 40–51.
Wild CP, Espina C, Bauld L, et al. Cancer Prevention Europe. Mol Oncol 2019; 13: 528–534.
Schüz J, Espina C, Wild CP. Primary prevention: a need for concerted action. Mol Oncol 2018; 13: 567–578.
Leon ME, Peruga A, McNeill A,et al. European Code against Cancer, 4th Edition: Tobacco and cancer. Cancer Epidemiol 2015; 39 Suppl 1: S20–S33.
Forbes LJ, Simon AE, Warburton F, et al. Differences in cancer awareness and beliefs between Australia, Canada, Denmark, Norway, Sweden and the UK (the International Cancer Benchmarking Partnership): do they contribute to differences in cancer survival? Br J Cancer 2013; 108: 292–300.
Allemani C, Weir HK, Carreira H, et al. Global surveillance of cancer survival 1995-2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 2014; 385: 977–1010.
Munro AJ. Comparative cancer survival in European countries. Br Med Bull 2014; 110: 5–22.
Vaccarella S, Lortet-Tieulent J, Saracci R, et al. Reducing social inequalities in cancer: setting priorities for research. CA Cancer J Clin 2018; 68: 324–326.
Dalton SO, Schüz J, Engholm G, et al. Social inequality in incidence of and survival from cancer in a population-based study in Denmark, 1994-2003: summary of findings. Eur J Cancer 2008; 44: 2074–2085.
TAKING QUALITY OF CANCER CARE, RESEARCH, AND EDUCATION TO THE NEXT LEVEL IN EUROPE: CHANGES TO THE OECI ACCREDITATION AND DESIGNATION PROGRAMME
Simon Oberst
Chair of the Accreditation and Designation Board of the Organisation of European Cancer Institutes and Director of Clinical Development at the Cancer Research UK Cambridge Centre
“Quality is never an accident; it is always the result of high intention, sincere effort, intelligent direction and skilful execution; it represents the wise choice of many alternatives, the cumulative experience of many masters of craftsmanship. Quality also marks the search for an ideal after necessity has been satisfied and mere usefulness achieved.” 1 So wrote the English essayist John Ruskin, and never has this been more true than with the task of achieving true quality in cancer care, research, and education for European cancer patients. The striving for continuous improvement involves the interaction of many disciplines and modalities, working together with educated patients towards the prevention, early detection, and cure of their cancer, with the data from their treatment being fed back into the learning and research loop for the benefit of future generations.
The Organisation of Cancer Institutes’ (OECI) Accreditation and Designation (A&D) Programme has now been running for 11 years, and by 2020 will have accredited 50 of the largest cancer centres in Europe.2,3 OECI readily acknowledges that in most European member states the majority of cancer diagnosis and care is delivered in hospitals that are not large cancer centres. Nevertheless, OECI’s thesis is that “by intelligent direction and skilful execution” (to use Ruskin’s words) the benefits of comprehensiveness in terms of integrating research, education, and care can be disseminated throughout the whole of a health economy. This can often be through these larger centres being hubs of networks nationally or regionally.
A key question is: What place does an A&D Programme fulfil within the quality improvement endeavour? Does it really stimulate change?4
First, the process provides a systematic opportunity for centres to assess themselves against OECI Quality Standards, which cover the following domains:
Governance
Organisation
Patient participation and empowerment
Multidisciplinarity
Prevention and screening
Diagnosis
Treatment
Research
Education and training
It is arguable that the process of self-assessment is just as revealing for a centre as the process of external assessment. The process requires the centre to engage in detail with the OECI Standards and mine data that multidisciplinary teams (MDTs) and management should ideally be collecting and using for improvement as routine. The emphasis is on determining whether the cancer centre has a properly functioning quality system and a culture of learning.
The second main process is that of external assessment. With OECI, this is based on a 2-day peer review with a balanced team of auditors from different disciplines including oncology, nursing, research, and quality, chaired by a person holding a director position in an OECI cancer centre. This process is adept at identifying the strengths of the centre and its opportunities for improvement. The process relies on effective interviewing, observation, and gaining audit evidence on the ground. Each standard is scored for compliance by the centre, and that scoring is compared to the centre’s self-assessment.
The third main strand of the cycle is the centre drawing up its improvement plan and agreeing that with OECI. Only a centre can improve itself, so this is the crucial process in the Deming Cycle that raises the local performance. The experience of OECI over more than 10 years is that even large comprehensive cancer centres can make improvements to harness their full potential.5 As OECI has followed up centres’ improvement plan actions after 1 year, we have seen improvement actions which in all probability would not have taken place apart from the OECI Accreditation Peer Review. Several centres improved clinical research process and increased recruitment of patients to trials; one centre introduced electronic processes covering the whole cycle of systemic therapy prescription through to administration to the patient; another centre created a comprehensive survivorship programme.
It is important that all accreditation programmes are themselves reviewed for independence and effectiveness. The OECI Standards were certified in 2018 by ISQua, the International Society for Quality in Healthcare External Evaluation Association.6 The OECI A&D Programme is the only cancer-specific programme to have this certification. Since the review, all recommendations are being implemented. For instance, there has been a need for better links with other certification systems (such as JACIE or ISO accreditations) to eliminate duplication, while ensuring that all necessary domains of care and safety are met.
At the Bari OECI General Assembly and Oncology Days, other revisions and updating of OECI’s A&D Programme will be announced and explained. These announcements will cover the following areas.
Re-accreditation processes
Like almost all accreditation systems, the OECI certificate lasts for 5 years and then requires a reaccreditation to remain current. OECI received representations from centres asking whether reaccreditation processes could be streamlined to obviate the need for a full completion of all the questionnaires and uploading documentary evidence. This was in a context where many of the processes, once established in the Deming Cycle, would go forwards in improvement or at least stay constant, rather than fall backwards. The OECI A&D Board considered the options and now recommends that approximately 20% of the Standards are deemed to be “core”: those which are so vital to quality that they absolutely need to be checked and newly documented every 5 years. Noncore standards, while still important and needing to be scored and described, would not necessarily require the uploading of new evidence of compliance. Furthermore, greater emphasis would be placed on the implementation of the Improvement Plan by the centre. In this way, the burden on centres should be reduced.
More logical format and new standards
Also announced in Bari is that the OECI Quality Standards are now presented in a more logical format which, in essence, follows the trajectory of cohorts of patients from prevention and screening to diagnosis, treatment, aftercare, and survivorship or palliative and end of life care. New or strengthened sections have been introduced around surgical oncology, molecular diagnostics, pathology, and radiology, while not drilling down into tumour-specific requirements.
Patient participation and empowerment
An enhanced section on patient participation and empowerment has been introduced in the revised standards. It is an OECI core principle that at a corporate level, patients should be involved in shaping cancer services for their community, and at an individual level great stress should be placed on empowering patients and their carers through information-giving, education, shared decision-making, and survivorship and holistic support. OECI believes that it has set the highest standards in European cancer care for these themes. Indeed, patient groups have been key to drawing up OECI revised standards.
All these areas of revision were tested with teams of experts at a meeting scheduled in Brussels in early April. These 40 experts included representatives of many of the treatment, research, and scientific societies in Europe in the field of cancer.
At the Bari OECI Oncology Days, 3 main themes emerging in Europe are addressed:
1) The development of Cancer Networks.7 These developments are progressing in many member states, and the networks are taking many different forms, from general cancer care networks (more or less conforming to the CanCon definition of a Comprehensive Cancer Care Network), to tumour-specific or rare cancer networks.8 OECI is developing quality standards for networks that will be piloted in 2020, complementary to the standards for cancer centres.
2) In Europe, in addition to institution-wide accreditation approaches, there is a parallel development of organ-centred approaches, which are able to drill more deeply into the detail of radiologic, pathologic, surgical, and clinical requirements for cancer in that organ. These have been developed by experts in those particular fields. Examples include the ECCO Essential Requirements for Quality in Cancer Care series, the German Cancer Society certification programme, EUSOMA accreditation for Breast, the European Commission Initiative in Breast Cancer, the European Association of Urology Prostate Cancer programme, and the Consensus Guidelines and accreditation programme for Neuroendocrine Tumours by ENETS.9-14 There is a desire in Europe if not to completely unify these approaches, then at least to map how they are complementary to one another and fit together in the whole cancer research and care landscape. There is also an obvious need to avoid unnecessary duplication of effort.
3) While acknowledging the need to drive up the quality of cancer care in general hospitals (where these are common in a healthcare economy), there is also a need to create new Comprehensive Cancer Centres (CCCs) in hubs in member states. Recent commentaries have suggested the need for one CCC for every small member state and per 5–10 million population in larger European states.15 This development will most likely come from the formation of University Medical Centres (UMCs) into CCCs by the more formal joining and programmatic alignment of University departments, research institutes, clinical cancer divisions with the UMC, and clinical research departments. OECI is building up expertise on how to create effectively working cancer centres, including through a programme structure, which involves researchers and clinicians working together in equal partnership and collaborating more strongly with industry.
In the context of a putative Cancer Mission in Europe, OECI would particularly like to see:
A policy stimulus to spur the creation of new cancer centres within UMCs and larger general hospitals, backed by evidence-based methodologies: an endeavour into which OECI has unique insight
The EU to put weight and financing behind systems of accreditation and benchmarking at both institutional (cancer centre) level as well as at tumour-specific level. OECI remains convinced that true comprehensiveness requires the interaction and crossover between different disciplines and MDTs, and that going forward in the genomic age, the collaboration between molecular diagnostics and therapy with repurposed therapeutics will become increasingly important.
Spielmann MH, Ruskin J. John Ruskin: a sketch of his life, his work, and his opinions with personal reminiscences. Cassell and company, 1900.
OCEI. Background of the OECI Accreditation Programme, https://www.oeci.eu/Accreditation/Page.aspx?name=BACKGROUND (accessed 5 May 2019).
Saghatchian M, Hummel H, Otter R, et al. Towards quality, comprehensiveness and excellence: The Accreditation Project of the Organisation of European Cancer Institutes (OECI) Tumori 2008; 94: 164–171.
Pomey MP, Lemieux-Charles L, Champagne F, et al. Does accreditation stimulate change? A study of the impact of the accreditation process on Canadian healthcare organizations. Implement Sci 2010; 5: 31.
The Deming Institute. PDSA cycle, https://deming.org/explore/p-d-s-a (accessed 7 May 2019).
International Society for Quality in Health Care External Evaluation Association; https://www.isqua.org/external-evaluation.html (accessed 5 May 2019).
OECI. How to establish patient-centred quality standards for various types of cancer networks. https://www.oeci.eu/Attachments/OECI_Paris_Meeting_19042018.pdf (accessed 5 May 2019).
CanCon. European Guide on Quality Improvement in Comprehensive Cancer Control (p 79), https://cancercontrol.eu/archived/uploads/images/Guide/pdf/CanCon_Guide_FINAL_Web.pdf (2017, accessed 5 May 2019).
Beets G, Sebag-Montefiore D, Andritsch E, et al. ECCO Essential Requirements for Quality Cancer Care: Colorectal Cancer: a critical review. Crit Rev Oncol Hematol 2017; 110: 81-93.
DKG, https://www.krebsgesellschaft.de/gcs/german-cancer-society/certification/publications_ii.html (2019, accessed 5 May 2019).
EUSOMA. Certification process, https://www.eusoma.org/en/certification-process/1-346-1-# (accessed 5 May 2019).
Mansel RE. Abstract P5-13-21: The European initiative in breast cancer (ECIBC): a program to reduce disparities in cancer care by accreditation of all breast centers in Europe, http://cancerres.aacrjournals.org/content/79/4_Supplement/P5-13-21 (2019, accessed 7 May 2019).
Wirth M. Fossati N, Albers P, et al. The European Prostate Cancer Centres of Excellence: A Novel Proposal from the European Association of Urology Prostate Cancer Centre Consensus Meeting, https://doi.org/10.1016/j.eururo.2019.01.033 (2019, accessed 7 May 2019).
ENETS. CoE Application, https://www.enets.org/coe_application.html (accessed 7 May 2019).
Oberst S. Bridging research and clinical care: the comprehensive cancer centre. Mol Oncol 2019; 13: 614–618.