
Abstract
Background:
The Agenzia Italiana del Farmaco (AIFA) Determination 809/2015 sets all the requirements that clinical units and laboratories must meet in order to conduct phase I studies. Requirements include buildings, equipment, personnel, emergency management, as well as quality requirements defined in a set of standard operating procedures.
Methods:
In September 2018, the Italian Association of Medical Oncology working group, Clinical Research Coordinator, created an anonymous survey addressed to 51 medical directors of oncologic/hematologic clinical phase I units and all medical directors of generic and transversal units located in Italy and listed at the AIFA website.
Results:
Questionnaires from 24 institutions were collected, 9 previously inspected by competent authorities. All surveyed structures are certified to conduct profit studies and 1 is authorized to include healthy volunteers; 15 units implemented a Clinical Trial Quality Team in order to conduct nonprofit studies. At the time of data collection, a total of 398 proposals for phase I trials have been received, more than 50% coming from 3 institutes. A total of 144 phase I studies were active, with a median of 2.5 (Q1–Q3=0–6) studies for each center and asymmetric distribution of proposals.
Conclusion:
The considerable number of proposals received from the interviewed centers indicates that Italy plays an important role in the international pharmaceutical scene, despite bureaucratic procedures that threaten exclusion from decision-making. The AIFA Determination will be an important opportunity to acquire a competitive working approach.
Introduction
In clinical research, clinical trials (CTs) play a key role in the development of new treatments and/or new therapeutic strategies. In the last 50 years in the onco-hematology field, CTs have led to an increase in survival and improved the understanding of cancer risk, prevention, and screening. 1 Lately, the treatment strategy has undergone rapid changes, with a shift from chemotherapy to targeted agents and more recently to immunotherapy drugs.
CTs typically proceed through several distinct phases (I to IV), of variable duration, designed to meet specific endpoints. 2
The first stage is represented by phase I trials, conducted on a small group of healthy volunteers, or patients in selected situations as in trials with antiretroviral or oncology molecules, with the primary aim to establish safety and tolerability and to define the maximum tolerated dose of a new drug. 3 In addition, in the era of tailored therapy, a new set of challenges for early CTs must be developed, as to find the optimal dose for a targeted or immunotherapy agent.
As a result of the recent trend in clinical research, phase I studies have become increasingly complex and demanding to execute compared to phase II–IV trials. 4
Since new molecules, often high-risk drugs, are tested for the first time on humans in phase I CTs, the ethical aspect of these studies has always been subject to discussion5–7; for this reason, it has been deemed essential to take careful precautions and to comply with rigorous quality standards to protect the rights, safety, and well-being of the participants. 8
Although regulations and guidelines already require the implementation of vigilant oversight by competent authorities and ethics committees,9–14 tragedies have occurred.15–17
In Italy, an important step was made in 2015 with the aim to guarantee the safety of patients (and healthy volunteers) enrolled in phase I studies. Indeed, if in the past the selection of adequate structures to conduct these types of trials was based solely on the analysis of internal feasibility carried out by the sponsor, with the introduction of Determination 809/2015 it became the rule that only the sites willing to comply with specific requirements imposed by competent authorities could participate in (or conduct) phase I studies 18 (Figure 1).
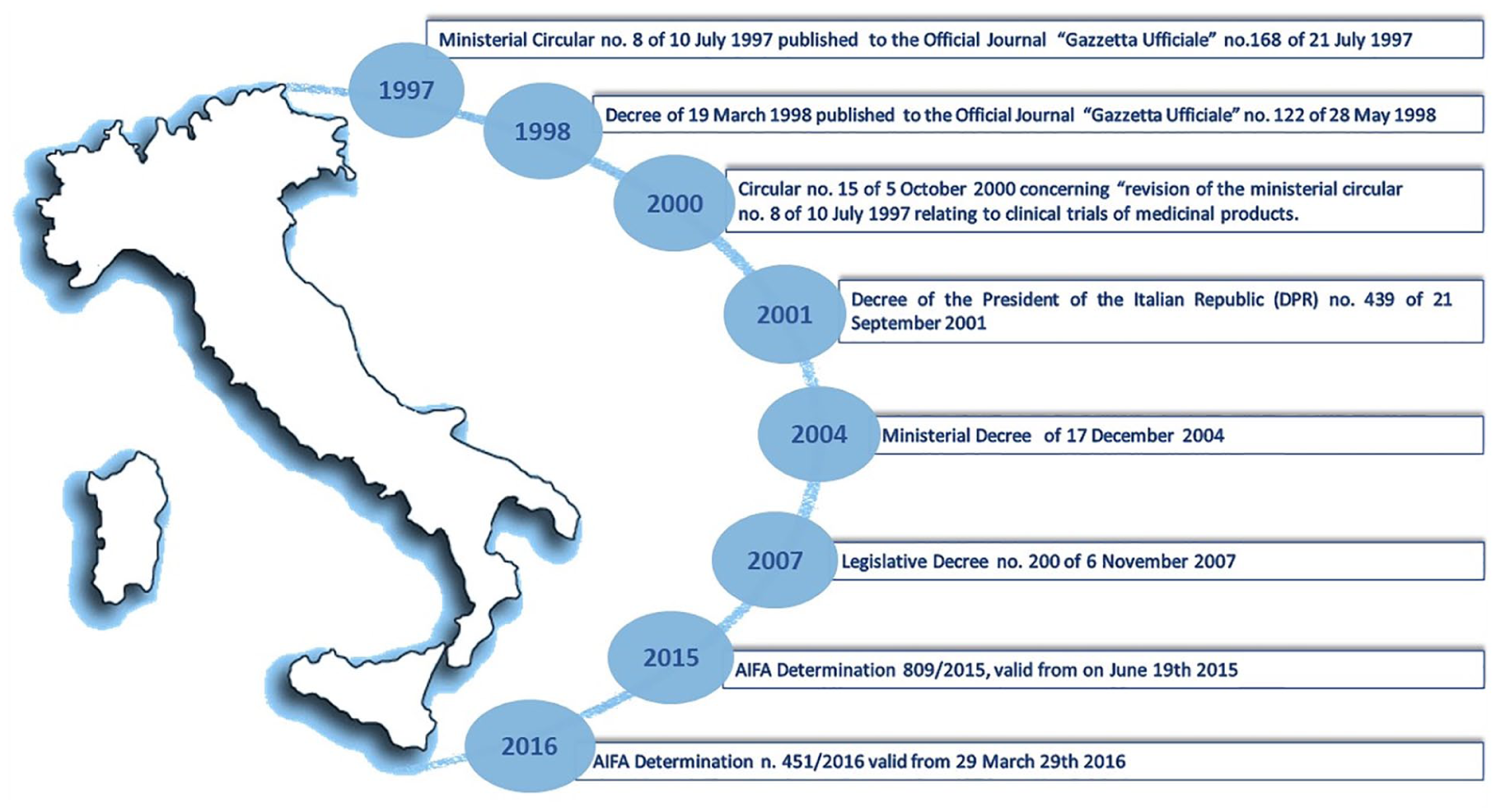
Timeline of main phase I studies law in Italy.
The Agenzia Italiana del Farmaco (AIFA) Determination 809/2015, valid from 19 June 2015 and made up of 1 general section and 3 appendices, lists exactly the requirements that clinical units and laboratories must possess in order to comply with the requirements of the competent authority and outlines how each unit and laboratory should provide a self-certification attesting this compliance. Requirements include buildings, equipment, personnel, emergency management, and quality requirements defined in a set of standard operating procedures.
Starting from 9 July 2016 and following a second determination clarifying in which form the self-certification was to be transmitted, 19 the new rules about Italian phase I trials have become effective.
Undertaking the self-certification process meant a huge investment for the institutions in terms of time and money. Indeed, with the new rules, the level of quality required in every area of research (structures, personnel, training, quality) has been greatly increased, especially for nonprofit studies, which until now had benefited from more flexibility.
All self-certified phase I clinical units and laboratories are published on the AIFA website. 20 The list is periodically updated and includes the hospital in which the unit is located, the region to which it belongs, and some important information, including the name of the phase I unit medical director and at least one contact.
With regard to clinical units, these could be generic functional units dedicated to multiple disciplines or could address a specific branch of Medicine (e.g., oncology, cardiology) and in a specific hospital one or more phase I units could coexist.
At the time of the AIFA Determination publication, few sites already held most of the requirements, while in many cases more complex work needed to be undertaken. 21
Two years after AIFA Determination 451/2016, we decided to conduct a survey among the self-certified sites to understand how they were prepared to obtain the requirements and what extent self-certification had impacted their research activity.
Methods
In September 2018, a working group of the Italian Association of Medical Oncology (AIOM), Clinical Research Coordinator, created an anonymous survey, revised and approved by the AIOM board. The approved version was made after a pilot test performed on 8 colleagues involved in phase I trials, to assess legibility, clarity, and completeness and to collect suggestions. Minor changes were required and a final general consensus was collected in a few weeks’ time.
The aim of the survey was to interview all medical directors of oncologic and/or hematologic clinical phase I units and of generic and transversal units listed at the AIFA website published on 30 September 2018. The link to the survey was sent by email to 51 contacts listed on the AIFA website, together with a short description of the aim of the project.
The questionnaire was created using Google and was organized in a series of linked pages (multiple-item screens), with electronic instructions to facilitate the flow. The survey was anonymous, voluntary, and took only a few minutes to complete. No incentive was given.
The completion link was active for a month and a reminder was sent within 1 week from the deadline.
The survey consisted of 14 questions, many of which were mandatory; almost all were multiple choice. If all mandatory answers were not completed, it was not possible to continue and confirm the questionnaire. A back button was provided to change answers before submitting them, after which no further changes were allowed.
The questions were organized in 2 main groups:
Unit characteristics
Date of self-certification (Q/year)
Self-certification fields (healthy volunteers, patients, pharmaceutical companies sponsored trial, academic trial)
AIFA inspection (yes/no)
Number of new people hired within the unit
Methods to promote knowledge of ongoing studies
Unit activity
Number of received phase I study proposals
Number of refused proposals and reasons for refusal (inadequate population, trial-specific requirements missing, poor scientific interest, presence of competitive trials)
Number of studies accepted but not activated in Italy
Number of proposals that failed selection and reasons for nonselection (inadequate population, any reason)
Number of received proposals still waiting for feedback and number of months since the proposal
Number of activated phase I trials
Number of ongoing phase I trials
Number of recruited patients
The survey was open from 20 October to 5 November, 2018, and a completion reminder was sent on 30 October.
Statistical analysis
Given the descriptive nature of the survey, a formally estimated sample size was selected; our expectation was to reach about 50% of responders to the survey. Descriptive analyses were performed with appropriate statistics.
Results are summarized as absolute frequencies and percentages for categorical variables and as median and interquartile range (Q3–Q1, difference between upper and lower quartiles) for continuous variables.
Results
A total of 24 completed questionnaires was collected, giving a response rate of 47%.
For the first survey domain, exploring the units’ characteristics, 13 (54.2%) units presented their self-certification during 2016, 7 (29.2%) in 2017, and 4 in 2018. All surveyed structures are certified for conduction of profit studies and only 1 (4.2%) is authorized to include healthy volunteers; 15 (62.5%) units implemented a Clinical Trial Quality Team (CTQT) for the promotion and conduction of nonprofit studies (Figure 2).
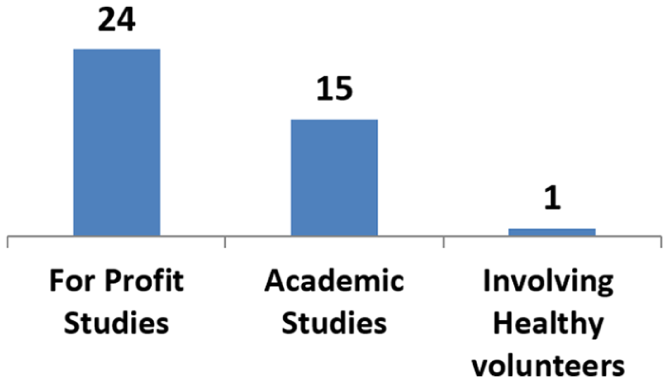
Characteristics of self-certified units.
About a third of the interview units (n=7, 29.2%) stated that it was necessary to recruit staff in order to meet the necessary requirements, for a total of 26 new professionals involved. Moreover, over 50% of the centers (n=16) organized as a network in order to promote knowledge and participation in active studies, mainly involving multidisciplinary boards, regional networks, and using website instruments.
Regarding the confirmation of requirements possession, 15 units (62.5%) had already been inspected by competent authority.
At the time of data collection, with a median time from the self-auto certification of 20 months (Q1–Q3=8–24 months), a total of 398 Confidential Disclosure Agreements for phase I trials was signed. Ten surveyed centers (41.7%) received fewer than 5 proposals, 8 centers (33.3%) a number between 6 and 10; 6 (25.0%) were invited to participate in over 10 studies (Figure 3). More than 50% of the total proposals were concentrated in 3 important institutes.
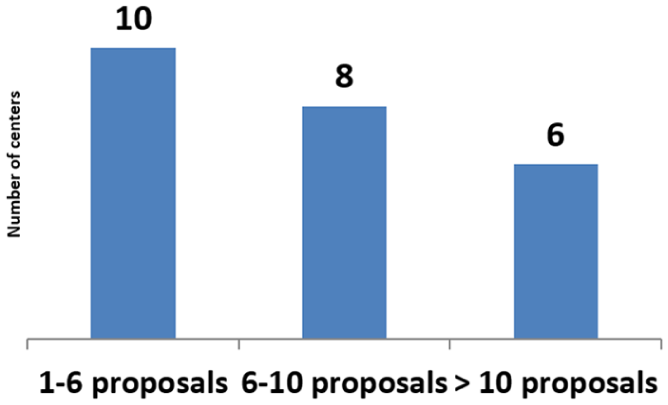
Number of received phase I studies proposals.
Fourteen (28.3%) of the surveyed units found themselves in the position of having to decline new study proposals: 13 (54.2%) refused at least 1 proposal while 4 (45.5%) refused more than 3 proposals, for a total of 60 refused studies. The main reasons for refusal were lack of specific requirements according to AIFA Determination (n=5), lack of scientific interest (n=6), poor target population (n=4), or presence of competitive trials (n=5) (Figure 4) (multiple choice allowed).
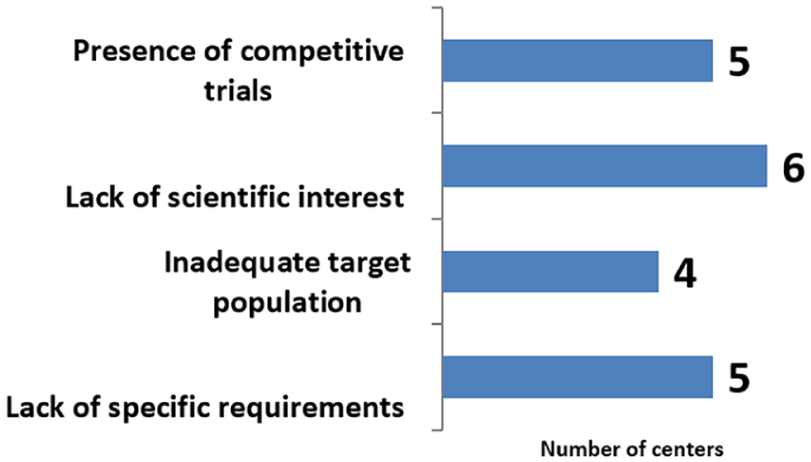
Reasons for the proposal rejection.
A considerable number of proposed studies have never been activated in Italy: in 9 (37.5%) of the interviewed units, a total of 41 phase I trials were, for various reasons, conducted outside of Italy. Moreover, 7 units (29.2%) were not selected following the site selection visit, for a total of 9 not activated studies; the main reasons were lack of study-specific requirements and insufficient target population (multiple choice allowed).
At the time of the survey, 12 units (50.0%) were waiting for the results of the selection, for a total of 53 pending proposals. Most of them (n=38, 71.3%) have been pending for less than 3 months, 7 (13.2%) from 3–6 months, while 8 proposals (15.1%) have not been contacted for over 6 months. Finally, 91 studies, involving 20 sites (83.3%), were in activation phase after the site selection.
Regarding the ongoing phase I trials, at the time of the survey, a total of 144 were active (36.0% out of the total proposals). It is important to note that each phase I trial could interest more than one center, therefore, every trial was considered more than once. About two thirds of the studies (n=96) were focused in 3 institutions; the remaining 49 proposals involved 14 centers, while the 7 centers left had no active studies at the time of survey. The median number of studies for each center was 2.5 (Q1–Q3=0–6), with a very asymmetric distribution of proposals among centers.
Discussion
The AIFA Determination has been issued with the intent of identifying a pool of highly specialized centers for the management of (and, in some cases, the promotion of) phase I clinical studies, and this is paramount from an organizational and ethical point of view. The imposed requirements are stringent regarding the necessary facilities, involved staff, and, mostly, the quality of the setting, the latter being uncommon in hospitals, especially in the public health system.
If the initial intent was to make a selection, the Determination became a driving force for most research centers, which made every effort to meet all the missing requirements. This is reflected in that the first request for self-certification was sent just 3 days from the first applicable day and, within a month, 13 structures (8 centers and 10 laboratories) were already self-certified. 22
The number has continued to grow, so much that, by February 2019, the self-certified facilities numbered 139: 61 solely for the clinical unit, 58 solely for the laboratory, and 20 for both facilities. 20
In May 2016, 1 month after the kickoff of self-certification procedures, a first survey of 80 research facilities (without distinction between already self-certified and non-self-certified structures) showed that few (<10%) of the responding centers possessed all the requirements according to the Determination, while the majority (71.4%) were working to implement what was missing. Most of the shortcomings concerned personnel, especially with regard to the professional profiles usually found only in pharmaceutical companies and in Contract Research Organizations (e.g. monitor, auditor, quality assurance). The same research had also anticipated what would then be confirmed by the high number of self-certifications submitted; only a small proportion of the centers interviewed declared that they were not interested in conducting phase I studies. 21
The need to implement research centers with new staff has been confirmed by our research as one-third of the interviewed structures stated that they had done so, for a total of 26 new professionals involved. It would be interesting to investigate which ones are most necessary professional figures and the magnitude of the financial investment needed to respond to the Determination’s demands. Another confirmed fact is centers’ evident rush to achieve self-certification, considering that over 50% had been provided within 9 months of the first day and only a minimum quota was adjusted in the last year.
The large number of proposals received from pharmaceutical companies could also suggest that there is a strong interest in investing in Italian infrastructure, despite being addressed to the same few recipients; it suggests once again that some structures might be considered more qualified and appealing compared to others. This is further confirmed by the asymmetric distribution of the number of ongoing phase I studies, two-thirds of which are concentrated in few locations (only in 3 out of the 24 institutions involved).
Moreover, our data confirm Italy’s interest in nonprofit research, given that more than half of the authorized facilities have adopted CTQT and decided to certify for the promotion of nonprofit studies.
The rate of rejected study proposals is low if we consider that for almost half of the centers it was zero. Besides understandable reasons of refusal, such as lack of interest, inadequate population, and presence of competitive studies, a significant proportion of units decided to not accept the proposal. Perhaps this could be due to lack of necessary requirements, as a sign that the Determination probably gave only a basic setting to the structure, which must be continuously monitored and implemented. Particular attention should be paid to this aspect in order to better protect healthy population.
These data are emphasized by results shown from another point from the survey regarding the promoter’s failure to select a center, thus endorsing the idea that the lack of specific requirements, together with an inadequate population, negatively impacted site selection.
A bit out of tune with the high number of proposals received by the centers is the equally high number of proposals not leading to site selection since the promoter ultimately decided to leave out Italy, a sign that Italy has a long way to go in terms of its bureaucratic slowdowns, that, for a while now, have penalized the country.23,24 Delays, however, are also affecting the sponsor, for a considerable number of proposals have been waiting for a response for a prolonged period.
The willingness of centers to be protagonists of this self-certification process is also demonstrated by the tendency, in more than half of the units interviewed, to promote awareness and knowledge as well as active participation in clinical studies, not only by arranging internal multidisciplinary groups but also by teaming up with other institutions and implementing web resources.
It is not easy to understand if the high number of certified centers (and the speed with which the requirements have been reached) is a symptom of an actual effort to adapt or a substantial underestimation of the requirements and of the consequences of a failed inspection. However, the fact that more than half of the structures interviewed have successfully passed the inspection of the competent authority can strengthen the first hypothesis.
Conclusions
The AIFA Determination has represented an important step for Italian research centers, which have had to exert all efforts, both from an economic and operational point of view, to adapt to the requirements of the competent authority. The receptiveness of the centers displays strong interest in the world of clinical research, despite the limited feedback resulting from inspections, in order to have a complete understanding of the centers’ success in adjusting to the requirements listed in the determination.
The considerable number of proposals received from the interviewed centers indicates that Italy plays an important role in the international pharmaceutical scene, despite bureaucratic procedures that threaten exclusion from decision-making.
It would be interesting to extend the present research to all self-certified structures, whose number has greatly increased, and make it a point to understand how to channel efforts in such a way to fulfill the requirements.
We are confident that these efforts will lead to powerful results: the initial investment followed by ongoing commitment and perseverance in maintaining the requirements will attract other, more complex studies. This growth will not only reduce costs of the National Health System, but also guarantee ad hoc funding for academic research.
In conclusion, the AIFA Determination will be an important opportunity to acquire a consistent modus operandi and a successful working approach that may become standard in all structures that intend to carry out clinical research, especially considering that the national legislation intends to extend the certification procedure to phase II and III trials. 25
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, or publication of this article.