
Abstract
Background:
Pembrolizumab, a humanized immunoglobulin monoclonal antibody directed against the programmed cell death 1 receptor, demonstrated robust efficacy and a manageable safety profile across multiple tumor types in clinical trials.
Aim:
To investigate the efficacy and safety of first-line pembrolizumab for patients with non-small cell lung cancers (NSCLCs) in clinical practice.
Methods:
In this observational monocentric retrospective study, 38 patients with PD-L1 >50% were enrolled between November 2017 and November 2018.
Results:
The global median overall survival was 11.08 months (95% confidence interval [CI], 5.98–not reached) and the global median progression-free survival was 6 months (95% CI, 3–not reached). In the univariate analysis, clinical performance status score and the development of immune-related adverse events were the only 2 clinical factors significantly correlated with overall survival.
Conclusion:
The results of the present study suggest that pembrolizumab seems less effective in the real-life population than in the pivotal clinical trials in patients with NSCLC but remains an effective treatment option for patients with NSCLC. Longer follow-up is needed.
Introduction
Non-small cell lung cancer (NSCLC) represents more than 80% of lung cancers, and approximately 70% of patients are diagnosed with advanced stage, inoperable, or metastatic disease.1,2 Despite recent diagnostic and therapeutic advances, the prognosis remains poor for most patients, and the all-stage 5-year observed survival rate is about 20%.3–5 Approximately 40% of newly diagnosed NSCLC cases are stage IV. The goal for treating these patients is to improve survival and reduce disease-related adverse events. 6 Current first-line treatment strategies are based on the presence of genetic mutations such as epidermal growth factor receptor (EGFR)–positive mutation or rearrangement of anaplastic lymphoma kinase (ALK). 7 However, as these genetic mutations are not present in most patients with NSCLC, cytotoxic chemotherapy represents the only treatment option for these patients and the first-line therapy usually consists of a combination of a platinum salt with a third-generation agent.
The key role of immune system evasion by tumors in cancer pathogenesis led to the development of new drugs targeting immune checkpoints.8–10 Among them, pembrolizumab, a humanized monoclonal antibody directed against the programmed cell death 1 (PD-1) receptor, was approved for first-line treatment of metastatic NSCLC with PD-L1 tumor proportion score ⩾50% without EGFR/ALK aberrations. Pembrolizumab also demonstrates robust efficacy and a manageable safety profile across multiple tumor types.11–17 Its efficacy and safety in patients with untreated advanced NSCLC were evaluated in KEYNOTE-024 trials that compared pembrolizumab monotherapy with platinum-based chemotherapy.18,19 In this study, pembrolizumab showed good efficacy with a median progression-free survival (PFS) of 10.3 months versus 6.0 months in the chemotherapy group and overall survival (OS) was 30.0 months with pembrolizumab versus 14.2 months with chemotherapy. At 6-month follow-up, the estimated rate of OS was 80.2% in the pembrolizumab group versus 72.4% in the chemotherapy group.18–20
Pembrolizumab also demonstrated favorable safety profile compared to platinum-based chemotherapy, providing long-term clinical benefit and favorable tolerability, and the most common immune-mediated adverse events encountered were hypothyroidism or hyperthyroidism, pneumonitis, and severe skin reactions, which occurred in the KEYNOTE-024 trial in 16.9%, 8.4%, and 7.8% of patients, respectively. 18
Even though pembrolizumab has been approved by multiple regulatory authorities and incorporated into clinical practice guidelines, additional clinical trial follow-up is required to determine whether the efficacy and safety of pembrolizumab are sustained. In addition, evidence from cancer clinical trials can be difficult to generalize to real-world populations. 21
The aim of the present study was to investigate in clinical practice the efficacy and safety of first-line pembrolizumab for patients with advanced NSCLC with PD-L1 tumor proportion score ⩾50% without EGFR/ALK alterations, so as to present real-life treatment outcomes.
Methods
Ethical approval
Approval was obtained from the Assistance Publique Hôpitaux de Marseille (AP-HM) ethics committee (RGPD 2019-09).
Design and setting
This observational monocentric retrospective study was conducted with patients starting a pembrolizumab regimen as treatment for previously untreated NSCLC between November 2017 and November 2018. Retrospective identification of patients was made possible by CHIMIO® software (Computer Engineering, Paris, France). After identification, patients’ clinical data (age, sex, adverse events, brain metastases, PD-L1 tumor proportion score evaluated using the Dako®22C3 antibody concentrate) were collected from the institutional patient database and CHIMIO® software. The end points evaluated were OS and PFS. Primary efficacy and safety analysis were conducted in all patients who received at least 1 dose of pembrolizumab.
Patients
Patients enrolled in this study were aged ⩾20 years and had histologically or cytologically confirmed squamous or nonsquamous NSCLC, stage IIIB/IV disease according to UICC-TNM classification [8th edition]), whatever their Eastern Cooperative Oncology Group (ECOG) performance status (PS). Patients’ PD-L1 tumor proportion score (TPS) was 50% or greater.
As mentioned in pembrolizumab approval, pembrolizumab was given at a dose of 200 mg in first-line monotherapy, every 3 weeks in each 3-week cycle until progressive disease or unacceptable toxicity was observed. At the end of each cycle, patients underwent diagnostic imaging.
Exclusion criteria
Patients involved in a clinical trial were excluded from this study.
Efficacy assessments
Response to treatment was evaluated by CT imaging. Tumors were assessed by investigators per RECIST v1.1 at baseline and every 9 weeks thereafter until disease progression, according to a local standard of care. When clinically indicated, additional CT was performed between scheduled scans. Treatment beyond radiologic progression was admitted in presence of clinical benefit. OS and PFS were analyzed using the Kaplan-Meier method, with the first dose of pembrolizumab as the starting point. The data cutoff date was 23 May 2019.
Safety assessments
Safety assessment included routine physical examination and laboratory assessment less than 24 hours prior to every administration of pembrolizumab. Immune-related adverse events (irAEs) were evaluated according to the NCI Common Terminology Criteria for Adverse Events (CTCAE), version 4.0. irAEs were grouped according to prespecified categories (endocrine irAEs including thyroid disorders, hepatogastrointestinal irAEs including colitis and diarrhea, renal irAEs including nephritis, pneumologic irAEs including pneumonitis, skin irAEs, musculoskeletal irAEs, other irAEs [including autoimmune hemolytic anemia, and asthenia as described in a previous study focused on the irAE spectrum in patients with NSCLC 22 ]) and were followed up every 3 weeks until these events resolved, were resolving, or had stabilized. irAEs and grade observed after the first dose of pembrolizumab and 28 days after the last dose were tabulated.
Statistical analysis
Categorical variables were described by numbers and percentage. The Kaplan-Meier method was used to estimate OS and PFS. Survival distributions were compared by the log-rank test between different subgroups. Subgroups were defined by sex, age, clinical performance status (ECOG PS), PD-L1 tumor proportion score, presence of cerebral metastasis at the initiation of pembrolizumab, and irAEs. The tests were performed bilaterally and were considered statistically significant when p ⩽ 0.05. The statistical analysis was performed with R software (version 3.1.0).
Results
The cohort consisted of 41 patients, 20 men and 21 women, mean age 62.07 years (Table 1). The median follow-up was 7.60 months. During the study, a median of 7 doses of pembrolizumab was given (range, 1–26; mean, 9.49). In 29.3% of patients, pembrolizumab was administered fewer than 4 times. A total of 20% of patients with ECOG PS 0–1 and 54.6% of patients with ECOG PS ⩾2 received fewer than 4 cures (p = 0.05).
Demographic and baseline characteristics of patients.
ECOG: Eastern Cooperative Oncology Group; NSCLC: non-small cell lung cancer; PS: performance status.
Efficacy
The global median OS was 11.08 months (95% confidence interval [CI], 5.98–not reached [NR]) (Figure 1) and the global median PFS was 6 months (95% CI, 3–NR). At 6-month follow-up, the estimated rate of OS was 58.5%. OS for patients with an ECOG PS 0–1 and ⩾2 were 18.04 months (95% CI, 9.7–NR) and 2.73 (95% CI, 0.99–NR), respectively (Figure 2). Patients who experienced irAEs showed a PFS of 17 months (95% CI, 4–NR) and an OS of 18.04 months (95% CI, 11.08–NR) (Figure 3). Among them, PFS and OS were 17 months (95% CI, 6–NR) and 18.04 months (95% CI, 11.08–NR) for patients who developed grade 1–2 irAEs and 0.5 month and 0.22 month (95% CI, 0.1–NR) for patients who developed grade 3–4 irAEs.
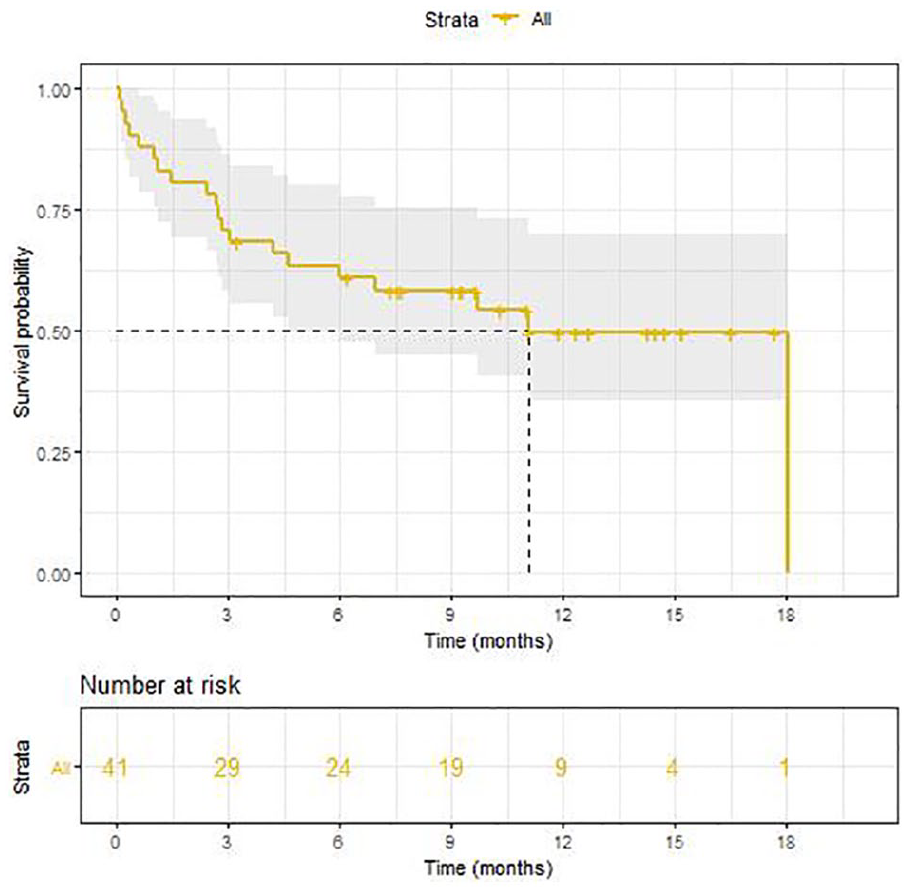
Overall survival for entire cohort.
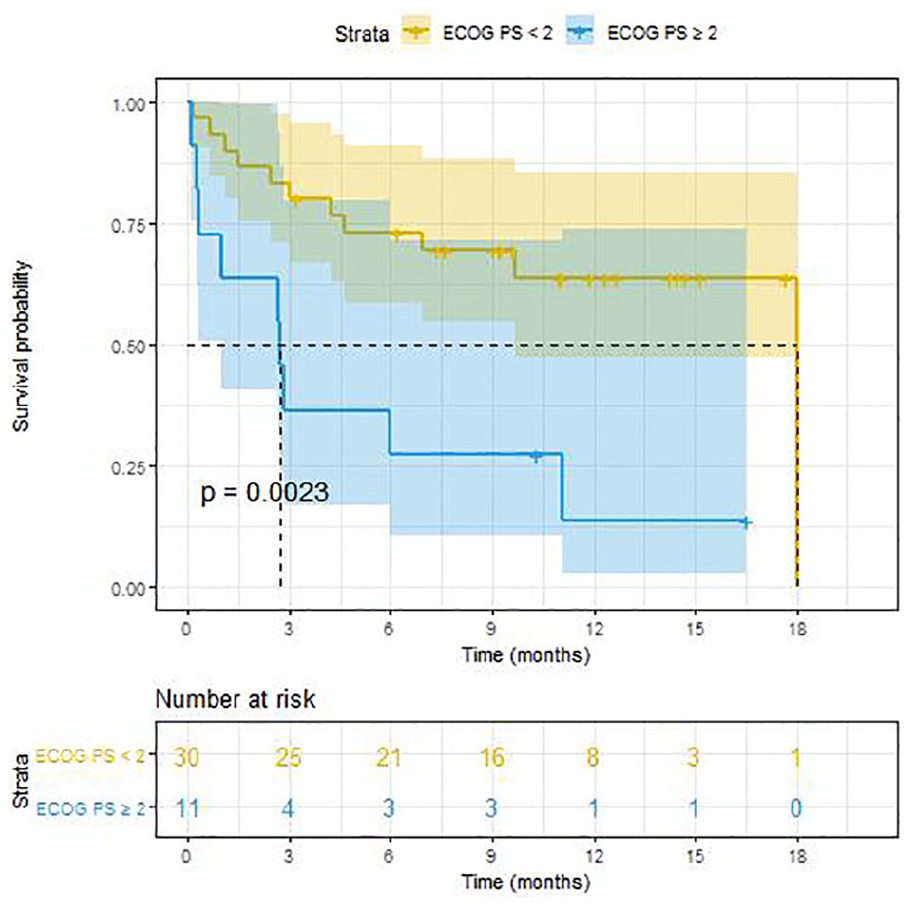
Overall survival based on Eastern Cooperative Oncology Group (ECOG) performance status (PS).
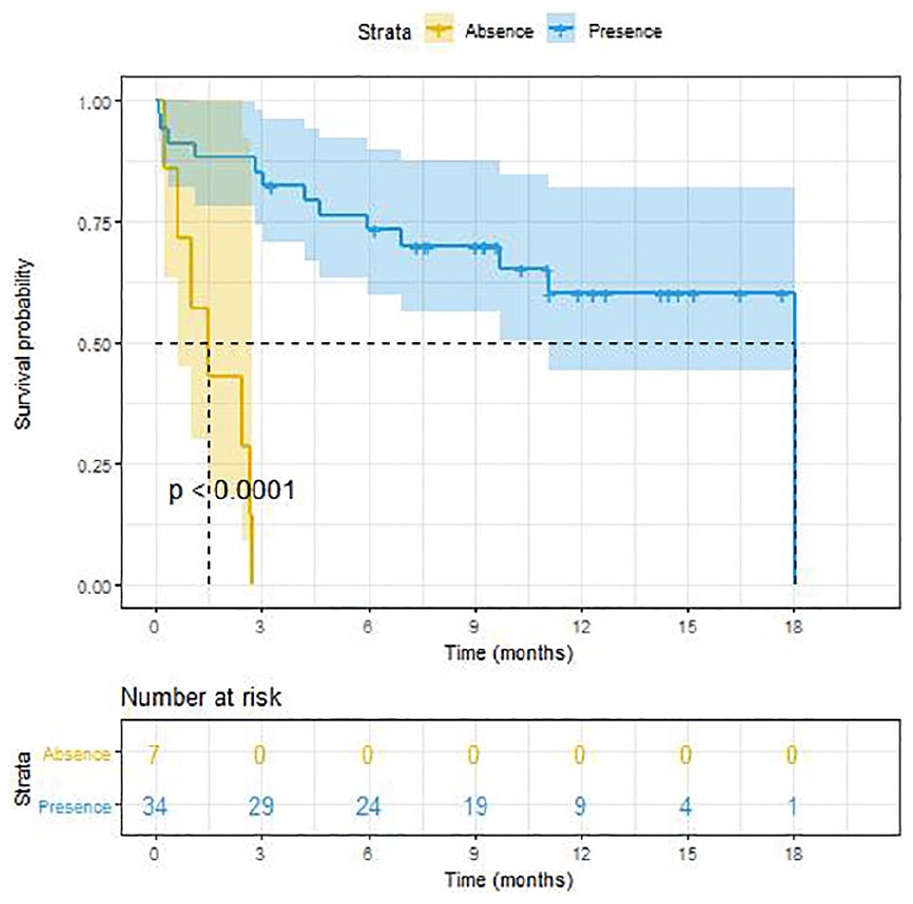
Overall survival based on immune-related adverse events.
At the data cutoff of the study, 1 patient (2.4%) showed a complete response, 11 patients (26.8%) a partial response, 5 patients (12.2%) disease stabilization, and 24 patients (58.5%) progressive disease. One patient (2.4%) showed radiologic pseudoprogression. No patients developed hyperprogression.
In the univariate analysis, ECOG PS score at the time of pembrolizumab initiation and presence of irAEs were the 2 factors significantly correlated with PFS and OS (Table 2).
Overall survival (OS) and progression-free survival (PFS).
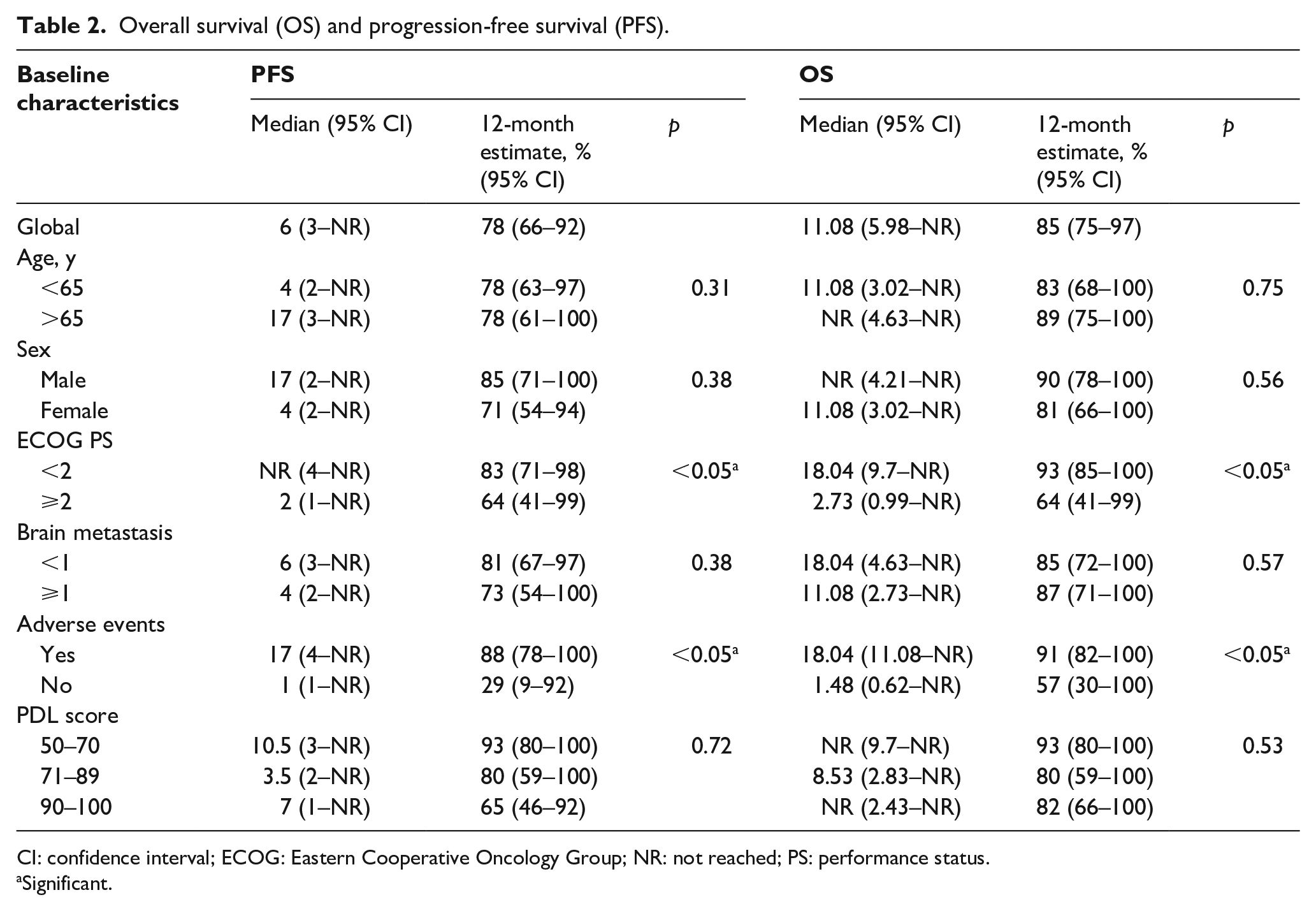
CI: confidence interval; ECOG: Eastern Cooperative Oncology Group; NR: not reached; PS: performance status.
Significant.
After discontinuation of treatment, 8 patients received subsequent systemic cancer therapy based on platinum salt chemotherapy.
Safety
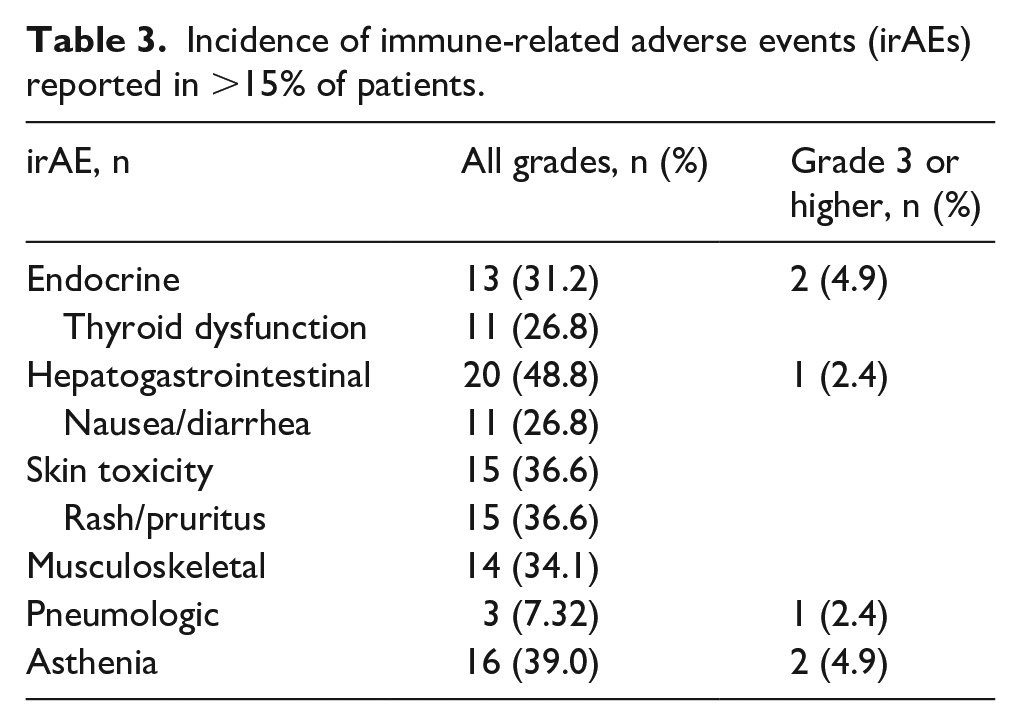
irAEs of all grades were reported in 34 patients (82.9%). Endocrine or skin irAEs occurred in 20 patients (48.8%) and consisted of grade 1–2 irAEs in 18/20 cases (90%). A total of 9.7% of the cohort experienced a grade 3–4 irAE. Among them, 2 died of acute pancreatitis or pneumonitis 10 days and 8 days after the last pembrolizumab infusion occurred, concurrently with disease progression. Grade 3–4 irAEs occurred only in patients with ECOG PS 2–3. A total of 12.1% of the entire cohort required medication with corticosteroid, but none needed immunomodulatory agents. Treatment was temporarily interrupted in 4 patients who developed grade 1–2 irAEs and treatment was discontinued in 2 patients who developed grade 3–4 irAEs (Table 3).
Incidence of immune-related adverse events (irAEs) reported in >15% of patients.
Discussion
Treatment with pembrolizumab has been shown to lead to significant improvement in OS, with better tolerability than platinum-based chemotherapy in randomized controlled clinical trials. Pembrolizumab has therefore become the standard treatment for patients with NSCLC with PD-L1 tumor proportion score ⩾50% without EGFR/ALK aberrations. However, there are limited published data on real-word experience with pembrolizumab in lung cancer.
The primary objective of our study was to assess the efficacy of pembrolizumab in the management of NSCLC. The KEYNOTE-024 and KEYNOTE-042 clinical trials were used as comparator as they demonstrated superiority of pembrolizumab against platinum salts–based chemotherapy taken as standard of care, especially in patients with PD-L1 TPS >50% for the KEYNOTE-042 study.
Patients’ baseline characteristics in the 3 cohorts were similar regarding age, sex, and stage of disease. However, there was a higher incidence of brain metastases (36.7% vs 11.7% vs 6%) and patients with ECOG PS ⩾2 (25.8% vs 0% vs 0%) in our cohort than in KEYNOTE-024 and KEYNOTE-042 trials, which was expected in a real-world population. Pseudoprogression was observed in only one patient, confirming that the incidence of this phenomenon in NSCLC is low, ranging from 1.5% to 3%. 23
In real life, the effectiveness of pembrolizumab in advanced NSCLC is less clearly demonstrated. 24 The global median number of pembrolizumab doses in our study was 7 for patients with NSCLC whereas it was 10.5 in the KEYNOTE-024 clinical trial. As our study contained a high proportion of patients with an ECOG PS score ⩾2 and a high proportion of patients receiving fewer than 4 doses, especially those with an ECOG PS score ⩾2, the finding of shorter PFS and OS in our study was not surprising, because ECOG PS score, despite being a subjective measure, is an important prognostic factor in metastatic NSCLC.18,19,24,25 OS in our study is similar to that described previously in a study conducted in real life, where a global median OS of 9.5±3.2 months (95% CI, 3.2–15.9) was observed. 26 After explorative subgroup analysis and as previously described, in our study ECOG PS score at the time of pembrolizumab initiation and presence of irAEs of any grade were the 2 factors significantly correlated with PFS and OS.22,25,27–29 OS for patients with an ECOG PS 0–1 and ECOG PS 2–3 was 18.04 and 2.73 months (p < 0.05), respectively, and approached those for patients with PDL score ⩾50 observed in KEYNOTE-042, where a median OS of 20.0 months was observed. 30 These results are similar to those reported in a previous study conducted in everyday clinical practice where patients with ECOG PS 2–3 had lower median OS than those with ECOG PS 0–1 (5.8 vs 16.7 months; p < 0.0001).
Patients with irAEs showed a markedly improved efficacy over patients without irAEs (PFS of 17 and 1, respectively, and OS of 18.04 and 1.48 months, respectively [p < 0.05]). 31 Recently, in a study on irAEs as predictor of therapeutic efficacy of anti-PD-1 antibodies conducted on patients with NSCLC, median PFS and OS of patients who experienced irAEs of any grade were 10.1 months and 20.5 months, respectively, and median PFS and OS of patients without irAEs were 20.5 and 8.5 months, respectively. 22 Consistent with the available data, our results confirmed the correlation between clinical benefit from anti-PD-1 treatments and the development of irAEs, as the mechanisms that underlie tumor response during immunotherapy are the same ones responsible for irAEs.
irAEs of grade 1–2 were associated with better clinical outcomes, PFS and OS of 17 months and 18.4 months versus 1 and 1.48 months, respectively, for patients who developed no irAEs. This evidence confirmed that less clinically impacting irAEs, such as skin irAEs and endocrine irAEs, could be those with a positive predictive role. 22 Only 12.1% of patients required treatment for the management of irAEs but some prescriptions such as topical corticosteroid prescriptions are not always mentioned in our institutional patient database. PFS and OS for patients who developed grade 3–4 irAEs were 0.5 month and 0.22 month. The small number of patients in this group does not allow conclusions.
The safety profile of pembrolizumab observed in this study differs from observations described in KEYNOTE-024 and KEYNOTE-042.18,30 Overall incidence of total irAEs of any grade was higher in our cohort (82.9%) than in KEYNOTE-024 (73.4%) or KEYNOTE-042 (63%) but some previous studies conducted in clinical practice highlighted the increased incidence of irAEs in comparison to those observed in clinical trials.31–34 In addition, we observed higher rates of dysthyroidism (26.8% versus 16.9% in KEYNOTE-024 and 18% in KEYNOTE-042) and asthenia (39.0% versus 10.4% in KEYNOTE-024 and 8% in KEYNOTE-042). 18 This has been similarly reported in a real-world experience with pembrolizumab toxicities in patients with advanced melanoma where asthenia was reported in 34.5% of patients and endocrine-related toxicities in 29.3% of patients. 31 The incidence of grade 3–4 irAEs is consistent with those described previously in real life.28,32 The incidence of irAEs leading to the discontinuation of treatment was 9.7% and was similar to the observed rate in KEYNOTE-024 and KEYNOTE-042 (7.1% and 9.0%, respectively) and in previous studies conducted in real life (ranging from 8.5% to 12.1%).18,28,32 In addition, as in our study grade 3–4 irAEs occurred in ECOG PS 2–3 patients, careful consideration should be taken for pembrolizumab administration for patients with a poor ECOG PS. 32 Finally, even though 2 deaths occurred a few days after the last pembrolizumab infusion, they cannot be formally considered as treatment-related death because of some confounding factors such as rapid disease progression.
There are limitations to the present study, such as the small size of the population and a relatively short median follow-up, which renders in-depth analysis, including multivariate analysis, difficult. Even though irAEs are a time-dependent covariate, it should be noted that based on the product monograph, median time to onset of irAEs ranges from 1.4 to 5.1 months, which is less than the observation time of our study. 35
Conclusion
The results of the present study suggest that pembrolizumab seems less effective in a real-life population than in the pivotal clinical trials in patients with NSCLC but remains an effective treatment option for patients with NSCLC. The occurrence of low-grade irAEs could be associated with an improvement of PFS and OS. Further work to clarify this association to reveal the underlying biological mechanisms of efficacy is required.
Footnotes
Author contributions
M.M., N.A., M.E.G.: Conception of the work. F.C., M.P.: Data collection. R.G.: Data statistical analysis. M.M., F.C.: Data interpretation. M.M.: Paper writing. N.A., P.V., F.B.: Critical revision of the article, writing, review, and editing. F.C., M.P., M.E.G., N.A., P.V., F.B., M.M.: final approval.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.B. receives lecture fees and research funding from Astra-Zeneca, Bayer, Bristol Myers Squibb, Boehringer-Ingelheim, Eli Lilly Oncology, F. Hoffmann-La Roche Ltd., Novartis, Merck, MSD, AbbVie, ACEA, Eisai, and Amgen. The other authors have no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.