
Abstract
Neutropenia is the most frequent side effect of commercially available myelosuppressive drugs and its most significant complication is febrile neutropenia. It is associated with increased hospital admissions and higher probability of death. Prophylaxis with the administration of granulocyte colony-stimulating factor can prevent neutropenia caused by anticancer drugs. The correct administration of these drugs and the management of febrile neutropenia are extremely important in the treatment of patients with cancer.
Introduction
Myelotoxicity is a significant clinical problem for patients treated with chemotherapy. 1 Neutropenia, the most frequent side effect of commercially available myelosuppressive drugs, increases the risk of infections. 2 Febrile neutropenia, the most significant complication of neutropenia, is an important condition because it leads to an increase in hospital admissions and a higher probability of death, owing to related complications as well as undertreatment that compromises the patient’s prognosis.3,4
Prophylaxis with the administration of granulocyte colony-stimulating factor (G-CSF) represents an excellent therapeutic weapon in the prevention of neutropenia caused by anticancer drugs 5 : it promotes the growth of neutrophils and decreases the risk of infection, improving tolerance to cancer treatments. 6 A large number of different G-CSF are available in different countries; the first drug approved was filgrastim in 1991. In recent years, several G-CSF biosimilars have been tested and approved for the prophylaxis of neutropenia in patients with cancer. This represents an important innovation, considering that, in addition to the reduction of febrile neutropenia and related complications, health cost can benefit greatly from it. 7
Methods
The recommendations formulated in these guidelines use the Grading of Recommendations Assessment, Development and Evaluation (GRADE) and Scottish Intercollegiate Guidelines Network (SIGN) methodology8,9 (supplementary Tables e-1 and e-2).
The clinical recommendation expresses the clinical importance of an intervention or procedure and the strength of the clinical recommendation is graded on 4 levels (strong positive, weak positive, weak negative, strong negative) (supplementary Table e-3).
These guidelines are in line with the recommendations published by other scientific organizations (American Society of Clinical Oncology [ASCO], National Comprehensive Cancer Network [NCCN], European Organization for Research and Treatment in Cancer [EORTC], European Society for Medical Oncology [ESMO]).
Generalities
Febrile neutropenia is defined as a temperature >38.5°C for 1 hour, or a temperature of 38°C for 3 consecutive measurements at an hour’s distance from one another, in presence of a neutrophil count <500/μL. 10 The severity of febrile neutropenia, defined according to the National Cancer Institute criteria 11 (Table 1), and the relative duration, conditioned not only the risk of infections, but also the reduction or the delay of the cancer treatment, determining the repercussions in terms of treatment efficacy and prognosis. 4 The incidence of neutropenia varies between 2% and 50%, as it depends on various factors, such as patient-related risk factors, type of cancer, chemotherapy, and genetic susceptibility. 12 Hazard mortality of febrile neutropenia is high, estimated around 9.5%. 1
National Cancer Institute criteria for neutropenia.

LLN: lower limit of normal.
Management of neutropenia: clinical questions
What is G-CSF and why should we use it?
This problem can be counteracted by the use of the G-CSF, whose mechanism of action stimulates the production and activation of neutrophils, increasing their migration in the blood. Its use can be in primary or secondary prophylaxis.
Primary prophylaxis means the administration of G-CSF during the first cycle of myelosuppressive chemotherapy, with the aim of preventing potential complications related to the neutropenia that could develop. This allows keeping the effective doses of antineoplastic agents, optimizing the prognosis. This method of administration has shown a significant reduction in the risk of febrile neutropenia and death in patients treated with chemotherapy.13–16
There are data showing a reduction in hospitalization and use of antibiotics in patients undergoing G-CSF in primary prophylaxis. 17
The benefit is also evident in terms of reducing the risk of death (about −3%).18,19
Secondary prophylaxis instead indicates the use of G-CSF during chemotherapy cycles following an episode of febrile neutropenia, developed during the previous cycle. A previous episode of neutropenia is in fact a risk factor for the development of further febrile neutropenia during subsequent therapy cycles of about 50%–60%.20–22 Another goal of secondary prophylaxis is to speed up the recovery of neutropenia so as to avoid the delay in the administration of the cancer treatment. However, there are no data proving a benefit of using G-CSF in this setting.
Therapeutic use means the administration of G-CSF in afebrile patients during severe neutropenia or in patients undergoing febrile neutropenia.
Currently there are 4 recombinant G-CSF formulations: filgrastim (nonglycosylated), lenograstim (glycosylated), pegfilgrastim (filgrastim in pegylated version), and lipefilgrastim (filgrastim in glycosylate version). Biosimilar versions exist for filgrastim and pegfilgrastim. The pegylated version differs for the different plasma half-life, much longer than the nonpegylated version (3–4 hours), and allows a single administration of the drug per chemotherapy cycle.23–25
The toxicity profile of these drugs is excellent. Postadministration bone pain, 26 and much more rarely exacerbation of inflammatory reactions, rash, and Sweet syndrome, 27 thrombocytopenia, increased lactic dehydrogenase, uric acid, and alkaline phosphatase have been reported. A possible risk of acute myeloid leukemia or myelodysplasia is also reported in patients receiving G-CSF during chemotherapy treatment.28–30
When is primary prophylaxis indicated with G-CSF?
The latest updates of the main international guidelines, ASCO, ESMO, Infectious Disease Society of America (IDSA), consensus-based guidelines from the NCCN, EORTC, and Italian Association of Medical Oncology (AIOM) recommend primary prophylaxis in chemotherapy regimens when the incidence of febrile neutropenia is ⩾20%1,10,12,31–33 (level of evidence 4). Previous guidelines recommended a 40% cutoff. 34 The cutoff update is due to the publication of randomized trials that showed cost-effectiveness when the risk of febrile neutropenia with a chemotherapy drug exceeded 20% incidence.14,17
In patients with risk between 10% and 20%, the use of G-CSF is subject to a general evaluation of the patient33,35,36 (Table 2).
Risk factors of febrile neutropenia.
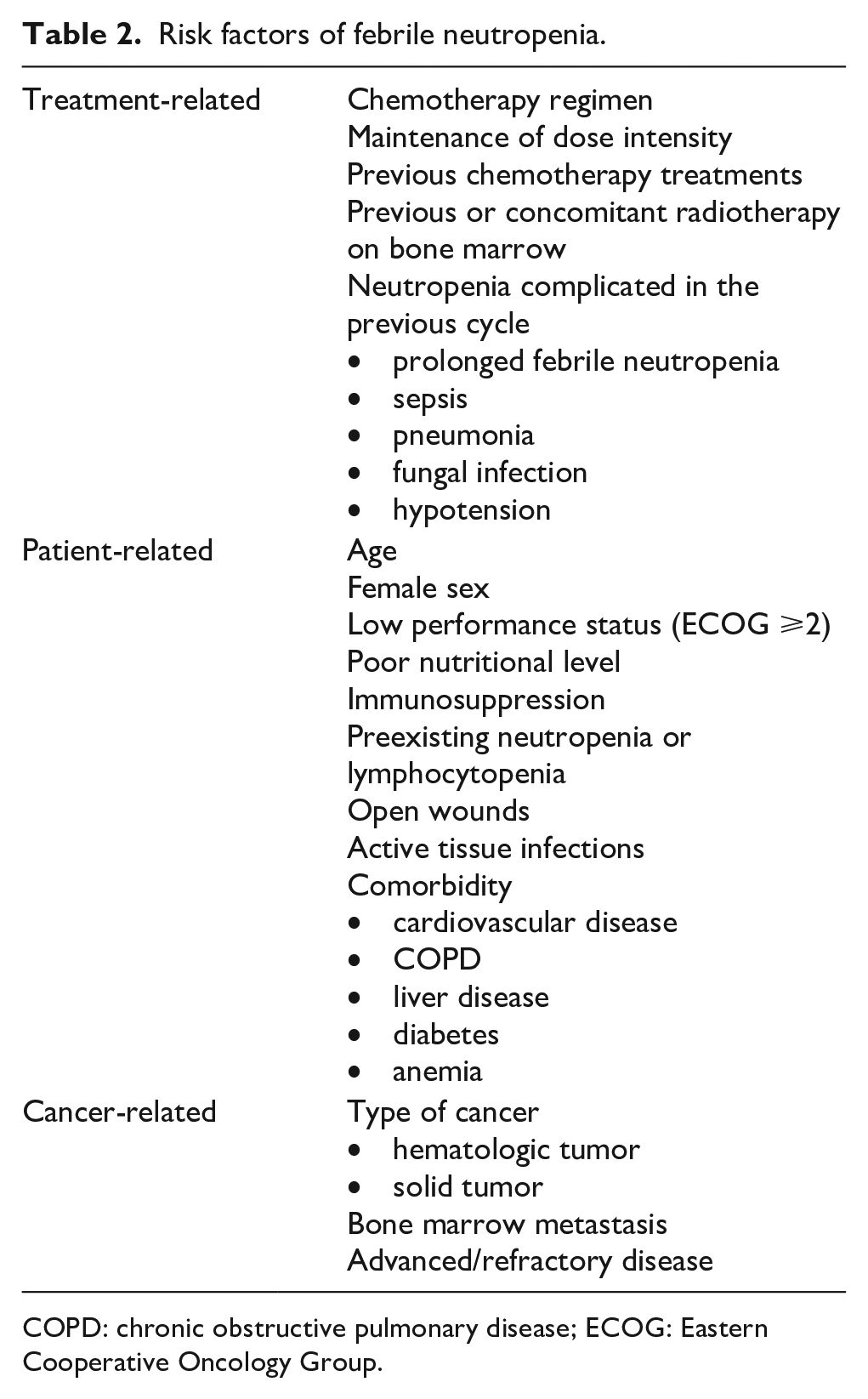
COPD: chronic obstructive pulmonary disease; ECOG: Eastern Cooperative Oncology Group.
Clinical recommendations (Figure 1)
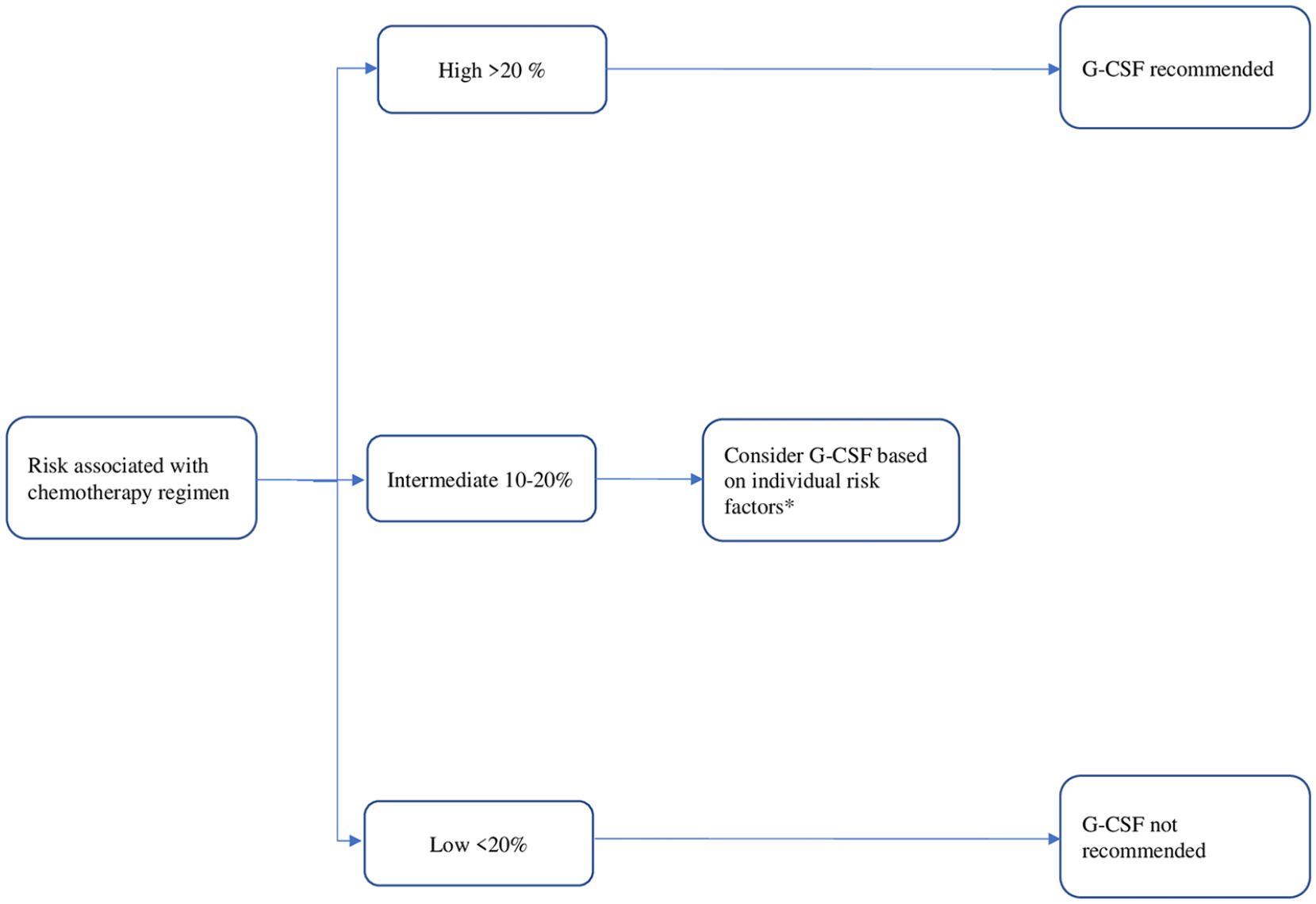
Primary prophylaxis flow chart. G-CSF: granulocyte colony-stimulating factor.
The use of G-CSF is recommended in primary prophylaxis in patients receiving chemotherapy at high risk (>20%) of febrile neutropenia (D: Strong positive).
The use of G-CSF in case of risk of febrile neutropenia between 10% and 20% is recommended in the presence of patient-related risk factors (Table 1); these should be reconsidered at each treatment cycle (D: Strong positive).
Primary prophylaxis is not recommended in patients with risk of febrile neutropenia <10% (D: Strong positive).
When is secondary prophylaxis indicated with G-CSF?
The ASCO, ESMO, and AIOM guidelines suggest that secondary prophylaxis should be considered in those patients who have already had a secondary complication of neutropenia (fever or delayed drug administration) in a previous cycle of chemotherapy, if dose reduction could affect overall survival or disease-free survival1,10,12,31–33 (level of evidence 4). In other circumstances, the dose reduction should be indicated as an initial measure.12,31
Clinical recommendation (Figure 2)
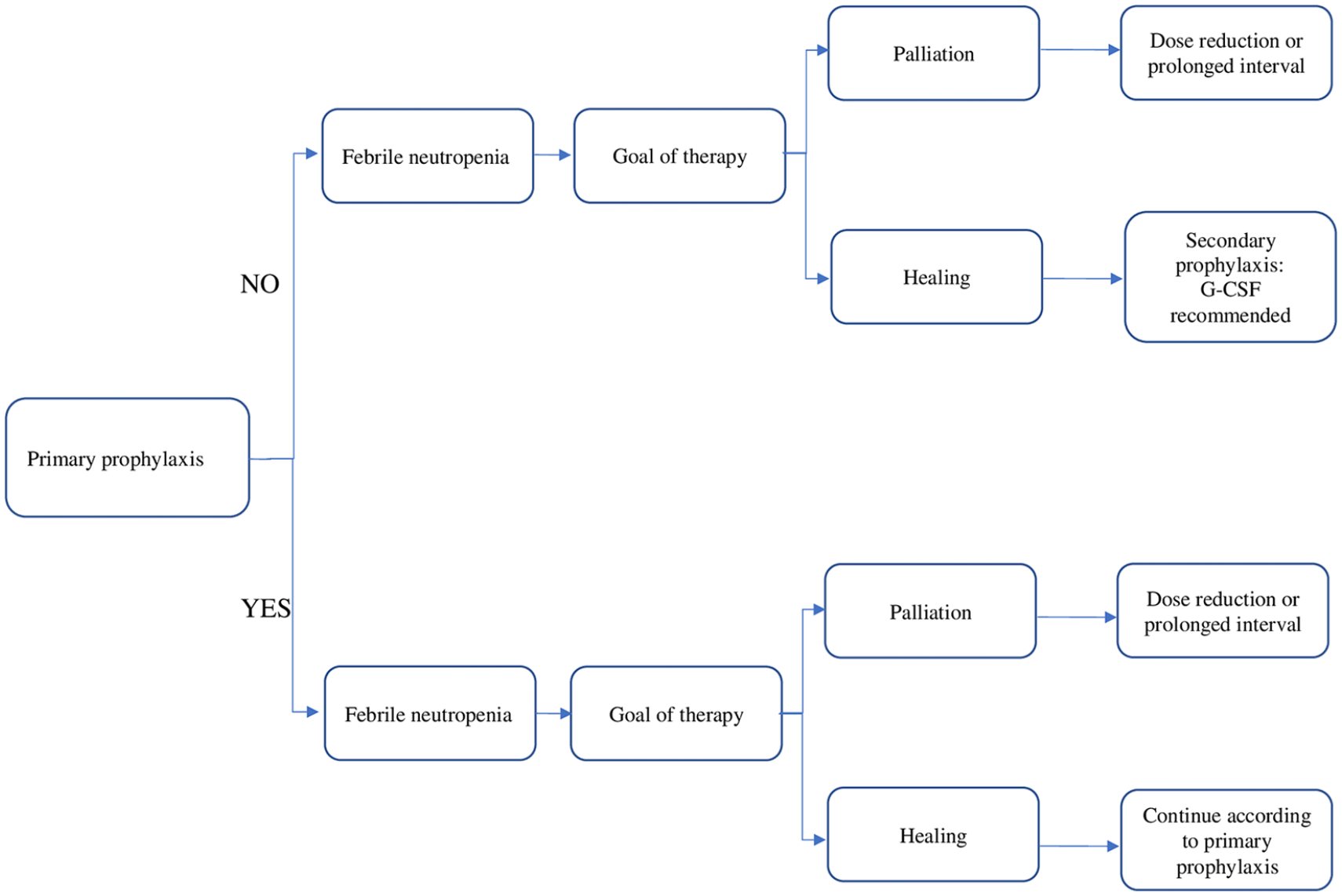
Secondary prophylaxis flow chart. G-CSF: granulocyte colony-stimulating factor.
The use of G-CSF in secondary prophylaxis is recommended in patients with a previous episode of febrile neutropenia, where a dose reduction is not recommended (D: strong positive).
When is the therapeutic use of G-CSF indicated?
As mentioned, the G-CSF for therapeutic purposes foresees its use in patients in a severe neutropenic state (absolute neutrophil count [ANC] <500/µL), whether they are afebrile or febrile. In the first case, there is no established role for the use of G-CSF and, given that the only advantage would seem to be a slightly faster recovery of neutrophil count, its use is not recommended. No differences in terms of hospitalization or number of infections were identified. 37
The use of G-CSF for therapeutic purposes in addition to antibiotic therapy, in patients with febrile neutropenia, is controversial: in particular, different revision articles and meta-analyses show that there is no advantage in terms of mortality, showing, however, a reduction in the time of hospitalization and a more rapid recovery of the neutrophil count.38–40
Several independent risk factors that correlate with higher mortality and could benefit from the use of G-CSF in addition to antibiotics have been identified 41 (Figure 3).
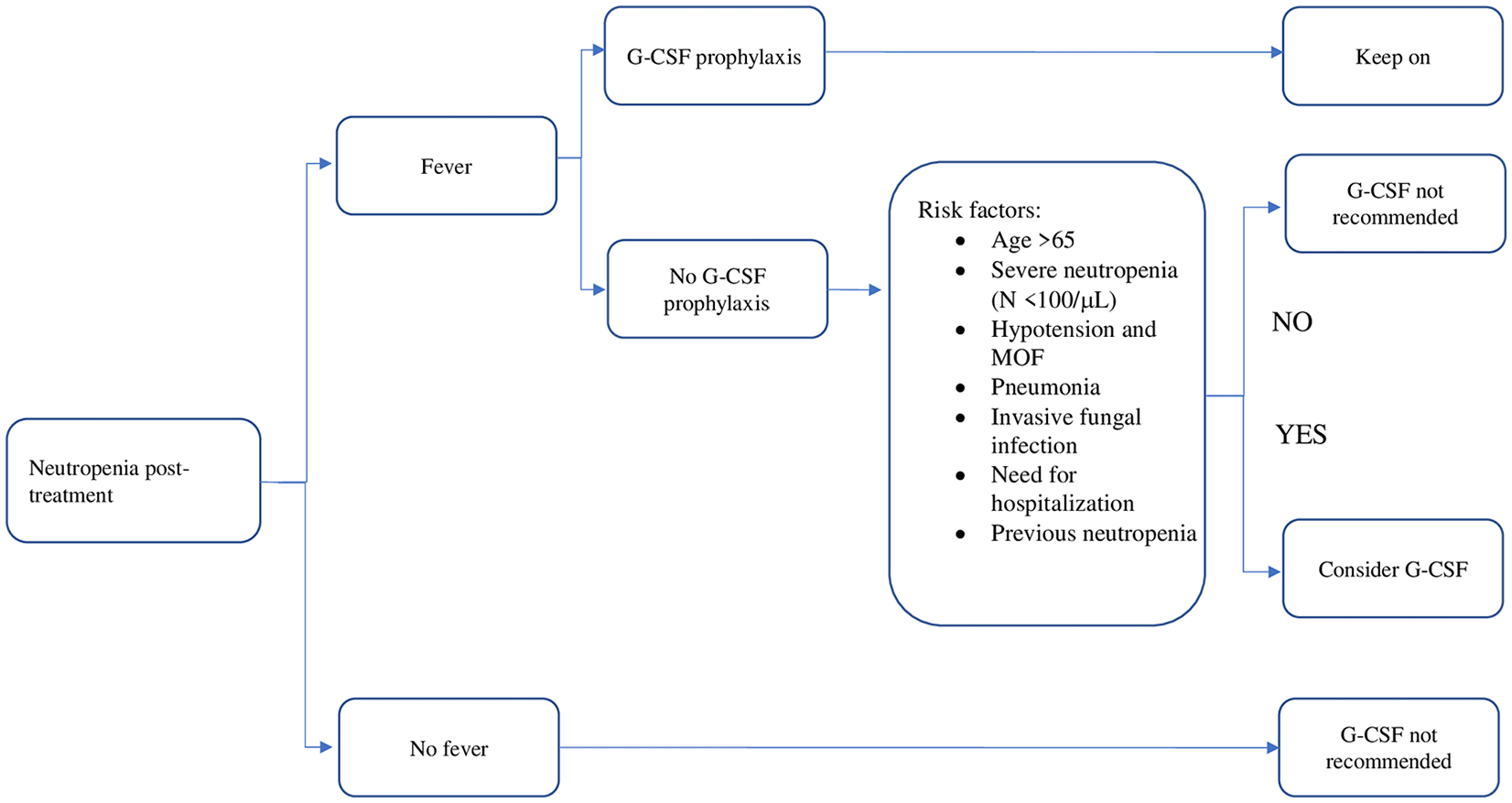
Therapeutic use of granulocyte colony-stimulating factor (G-CSF). MOF: multiorgan failure.
The guidelines differ in this recommendation: the ASCO, NCCN, and AIOM guidelines recommend against the use of G-CSF for therapeutic purposes in combination with antibiotic therapy in patients with severe neutropenia1,31,32 (level of evidence 4). However, they suggest to consider its use in selected cases (advanced age, comorbidity, prolonged neutropenic state); the IDSA guidelines recommend not to use the G-CSF for therapeutic purposes under any circumstances 10 ; the ESMO guidelines do not clearly specify this setting. 12
Clinical recommendations (Figure 3)
Therapeutic use of G-CSF is not recommended in patients with febrile neutropenia (D: weak negative)
G-CSF should not be used routinely in combination with antibiotics (D: weak negative)
G-CSF can be used to reduce the duration of neutropenia (D: weak positive)
Which dose and for how long is the G-CSF administered?
For prophylactic purposes, G-CSF should be administered between 24 and 72 hours after the administration of chemotherapy and continued until the number of neutrophils is >1,000/μL1,10,12,31–33,35,42 (level of evidence 4). The recommended dose is 5 μg/kg. If pegylated G-CSF is chosen, it will be administered between 24 and 72 hours after chemotherapy in single dose, at a dose of 6 mg. Given the potential sensitivity of rapidly dividing myeloid cells to cytotoxic chemotherapy, administration in the previous 48 hours and concomitantly with chemotherapy is contraindicated. 43
Alternative administration schedules, usually shorter, may have similar efficacy; however, this approach has not been compared to the standard in any randomized trials. 44
Clinical recommendations
In primary and secondary prophylaxis, the use of G-CSF (5 μg/kg/d SC) must be started between 24 and 72 hours after the end of the chemotherapy cycle and must be continued until neutrophils are >1,000/μL, after nadir (D: strong positive).
Single administration of pegfilgrastim/lipegfilgrastim (6 mg SC) should be performed between 24 and 72 hours after the end of the chemotherapy course (A: strong positive).
G-CSF administration is contraindicated within the previous 48 hours and in conjunction with chemotherapy (D: weak negative).
The use of G-CSF with daily administration in adult patients with solid tumors may be considered also according to schedules lower than 6 days of administration, within chemotherapy regimens that do not allow the administration of the minimum number of 6 days (D: weak positive).
Which type of G-CSF is advisable?
There is no difference in the use of short-acting compared to long-acting G-CSF, if used correctly.15,25 In clinical practice, the majority of clinicians do not use daily G-CSF correctly. Common practice is to treat patients with daily G-CSF for less than 7 days, sometimes less than 6 days, and this translates into higher risk of chemotherapy-induced neutropenic complications.45–47 A recent review found that the risks of febrile neutropenia-related complications were generally lower for prophylaxis with long-acting G-CSF than daily G-CSF. 48 Moreover, a recent meta-analyses showed that the incidence of febrile neutropenia is higher with the use of short-acting G-CSF compared to long-acting G-CSF and that there is a trend in favor of the use of long-acting G-CSF in relation to the incidence of hospitalization for febrile neutropenia and incidence of chemotherapy dose reduction and delays. 49 Another point in favor of pegfilgrastim is related to convenience and patient adherence. A single administration of G-CSF is easier, more comfortable, and does not require hospital visits and tests to evaluate ANC levels.
Among commercially available long-acting G-CSF, Neulasta is the oldest approved, most commonly used, and associated with the most experience and clinical data. 50 However, its cost is considerably higher than that of short-acting G-CSF, and this has represented a reason to consider it the second choice in clinical practice. In recent years, several biosimilars of pegfilgastrim have shown equal efficacy in terms of reduction of febrile neutropenia, severe neutropenia, and tolerability. Therefore, they are approved and available for the prophylaxis of chemotherapy complications, representing an excellent solution for healthcare cost. 6
The use of the different types of G-CSF is influenced by the type of chemotherapy. In fact, in patients receiving weekly chemotherapy, filgrastim is recommended. However, in patients receiving split-dose chemotherapy, pegfilgastrim can be an option, and in this case, it is recommended 24 hours after the last chemotherapy dose and >14 days before the next dose. 51 The metabolism of both molecules is different: renal clearance for short-acting and nonrenal clearance for long-acting. Overall, both short-acting and long-acting G-CSFS are agents with high efficacy, safety of use, and good tolerability when used correctly. However, the pharmacokinetic characteristics of long-acting agents allow a simplified method of administration, so they can contribute to greater adherence to treatment of particular categories of cancer patients 1 and they can reduce variability in terms of timing and duration of administration.
Discussion
In oncology, personalization of treatment is increasingly frequent and detailed, so the management of myelotoxicity represents a considerable commitment for the clinician. Knowing the impact on mortality and possible complications is necessary to improve the outcomes of patients and reduce health care costs. It would be interesting to have available data that can highlight adherence to the treatment, according to indications of the various guidelines, and these data are being reported. 52 Lack of adherence to these indications often reflects clinical management problems. For example, a common finding in daily practice is the use of nonconventional schedules of short-acting G-CSF (i.e. less than 6, or even 4, days of administration), based mostly on experiential criteria, instead of evidence-based data. Another problem is represented by neutropenic prophylaxis through the use of G-CSF, in the treatment protocol characterized by a close interval administration, as happens with weekly administrations of chemotherapy, or prophylaxis in a different form of neutropenia, as happens with the cyclin inhibitors (CDK4/6). Some molecules are being developed that could remedy this problem.
The arrival on the healthcare market of biosimilars, both of the short-acting G-CSF and of the long-acting G-CSF, contributes to healthcare costs, which is increasingly becoming a key point in optimizing treatments.
Conclusion
The management of neutropenia must be a fundamental element of clinical practice in oncology, having a strong impact on prognosis and on health care costs. Continuous updating of guidelines is fundamental to guarantee the best quality of healthcare.
Supplemental Material
Supplementary_material – Supplemental material for Management of chemotherapy-induced neutropenia in patients with cancer: 2019 guidelines of the Italian Medical Oncology Association (AIOM)
Supplemental material, Supplementary_material for Management of chemotherapy-induced neutropenia in patients with cancer: 2019 guidelines of the Italian Medical Oncology Association (AIOM) by Antonino C. Tralongo, Andrea Antonuzzo, Paolo Pronzato, Andrea Sbrana, Marianna Turrini, Federica Zoratto and Marco Danova in Tumori Journal
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.