
Abstract
Background:
Malignant pleural mesothelioma (MPM) is a rare and aggressive disease of the pleura with a dismal prognosis. Distant metastases most commonly occur in the liver, spleen, and thyroid gland. To our knowledge, ovarian metastases have never been described.
Case description:
We describe a case of a woman with recurrent malignant pleural mesothelioma presenting a single ovarian metastasis, surgically resected.
Conclusions:
This case report highlights the importance of using a complete staging protocol in patients with MPM to improve patient management. A whole-body computed tomography (CT) scan with contrast enhancement and possibly positron emission tomography–CT should be performed to identify any distant metastases before deciding on treatment strategy.
Introduction
Malignant pleural mesothelioma (MPM) is a tumor of mesodermal origin associated with a dismal prognosis with increasing incidence in western countries. 1 Symptoms are usually late-onset and nonspecific, the most common being dyspnea with pleural effusions and chest pain. Most MPM cases are associated with asbestos exposure. 1
MPM has very aggressive behavior and generally spreads locally to the chest wall, mediastinum, and diaphragm. Distant metastases most commonly occur in the liver (31.9%), spleen (10.8%), thyroid gland (6.9%), and brain (3.0%). 2 To our knowledge, ovarian metastases have never been described.
We present a case of MPM with a single distant metastasis to the right ovary.
Case description
We present a case of a 68-year-old woman with no history of professional asbestos exposure. After arriving at the emergency department with chest pain, mainly from the right side, she was diagnosed with a mass in the right thorax by a chest computed tomography (CT) scan. Transthoracic biopsy revealed histologic diagnosis of epithelioid MPM with solid and trabecular growth patterns and infiltration of the intercostal muscle. Immunohistochemistry results were CK 5/6+, WT1+, TTF1−, napsin A−, calretinin+, and Ki67 20%. No distant metastasis was observed on the CT scan with contrast enhancement (CE). The patient had good performance status (Eastern Cooperative Oncology Group performance status 1) and during the following 12 months, the patient underwent six cycles of chemotherapy with cisplatin plus pemetrexed; she came to our attention on maintenance therapy with pemetrexed only. In order to administer consolidative radiotherapy, positron emission tomography (PET)–fluorodeoxyglucose (FDG) was performed, showing right pleural FDG uptake (SUVmax 6.5) and a focal hypermetabolic capitation located in the right lower pelvis of probable ovarian origin (SUVmax 25.8) (Figure 1).
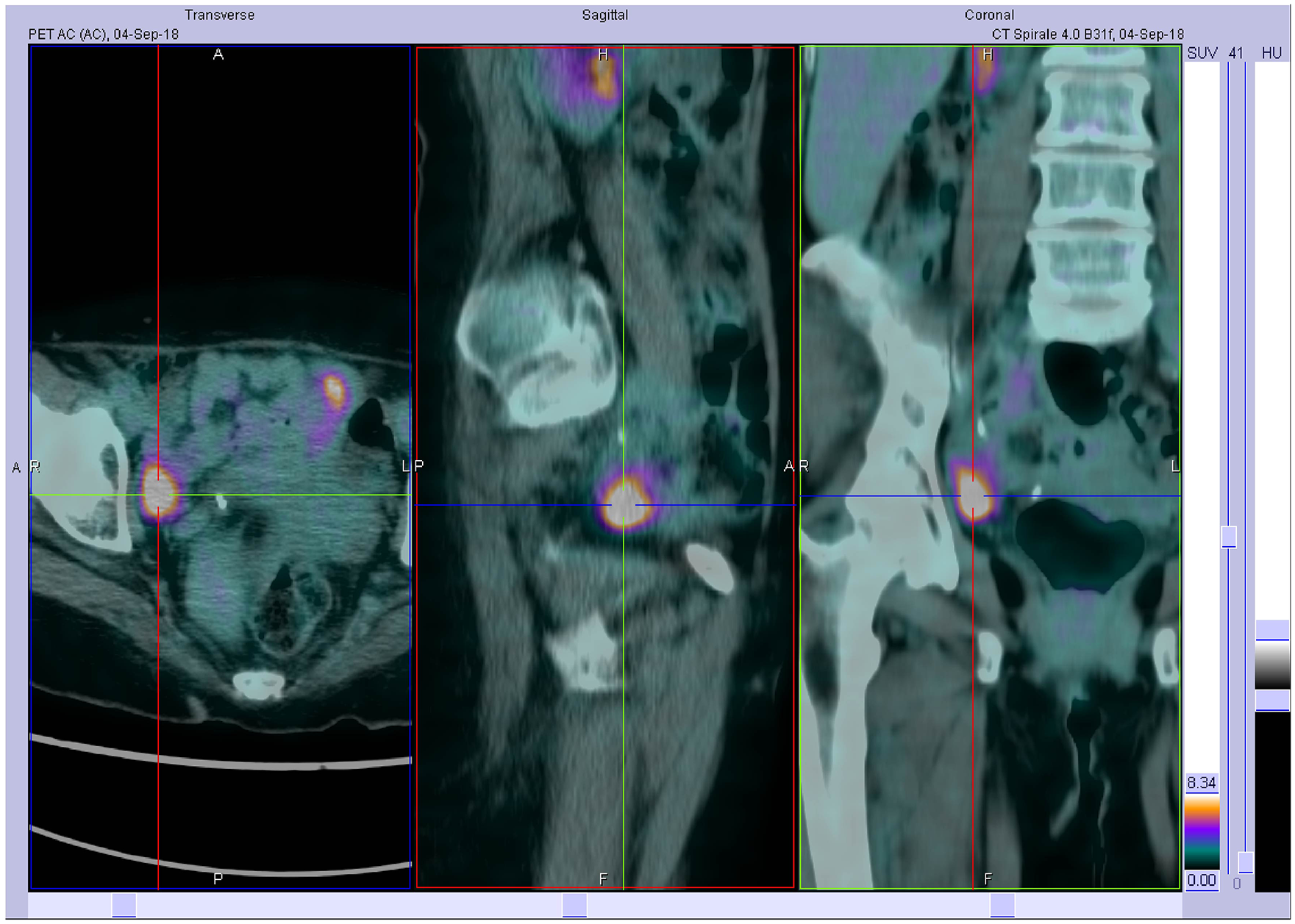
Detail of the right unilateral lower pelvis capitation (SUVmax 25.8) in correspondence with hypodense ovarian formation.
Transvaginal ultrasound showed a 34×20×16 mm mass, solid and unilocular, of the right ovary. Blood markers were CA 19.9, 17 U/mL (<40 U/mL); CA125, 6 U/mL (<35 U/mL); and HE4, 197 pmol/L (<140 pmol/L). The multidisciplinary board with the gynecologist decided on a radical surgical procedure in order to rule out any gynecologic primary cancer. The patient underwent bilateral ovariectomy with infracolic omentectomy.
Histopathologic examination of the right ovary showed massive infiltration of epithelioid cells with eosinophil cytoplasm and vesiculosus nuclei, intensely positive to calretinin, CK7, and WT1, and estrogen receptor and progesterone receptor negative (Figure 2).
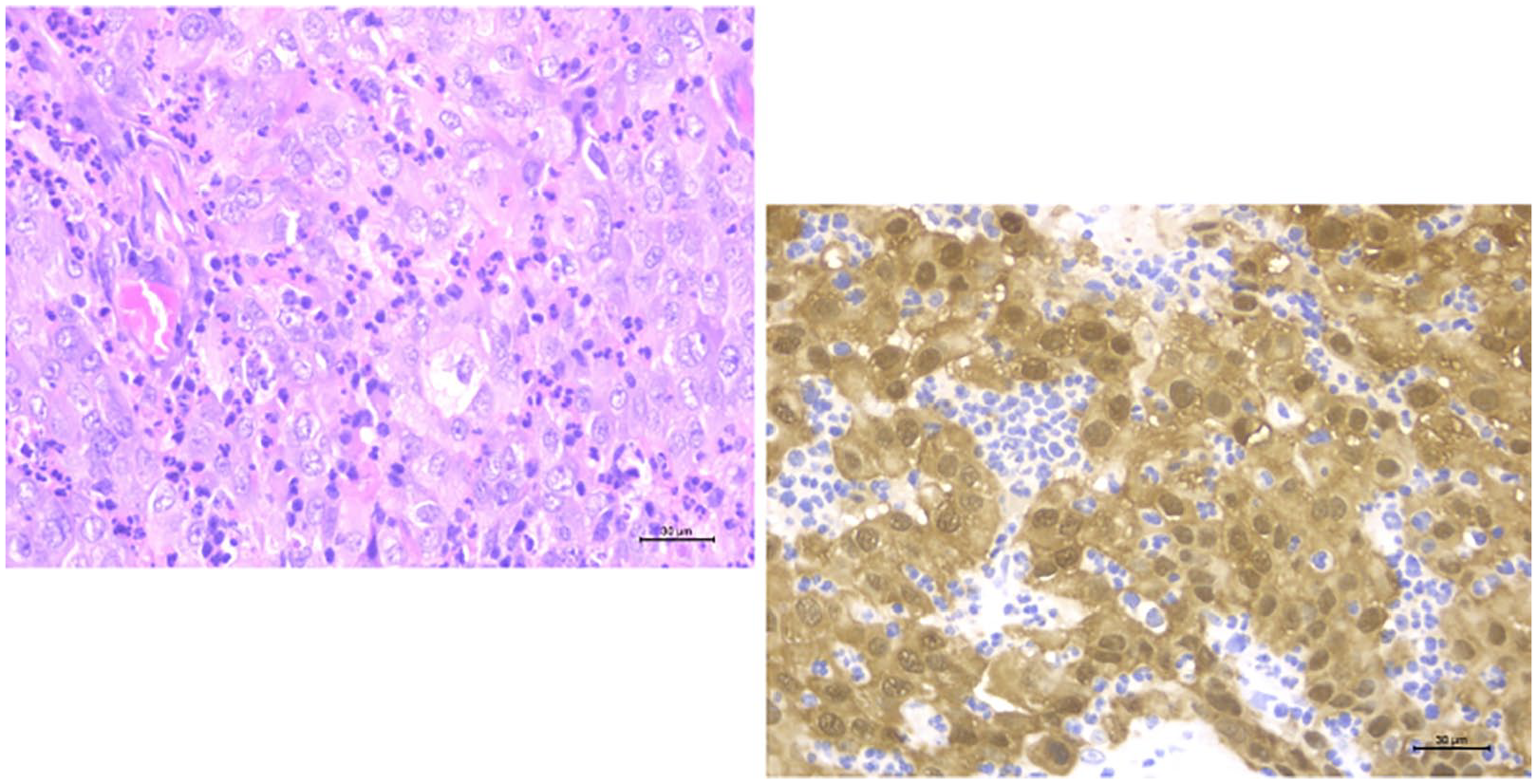
Histology of the right ovarian mass. Detail of hematoxylin & eosin showing the cuboid cells characteristic of malignant pleural mesothelioma (left panel) and immunohistochemistry for calretinin; the vast majority of cells are intensely positive (right panel).
CT scan 2 months after surgery showed no evidence of disease in the lower abdomen, while progressive disease of the primary tumor was reported. The patient is in good clinical condition with a performance status of 1 and has started second-line therapy with gemcitabine.
Discussion and conclusion
We describe for the first time a single ovarian metastasis of an MPM previously diagnosed by transthoracic biopsy and PET-CT. Immunohistochemistry of the right ovary was concordant with the transthoracic biopsy, identifying the ovarian mass as a metastatic localization of epithelioid type malignant mesothelioma.
The role of PET-CT in the diagnosis and staging of MPM is controversial; however, MPM is clearly FDG avid, and PET may help in staging and prognosis estimation. 3 PET-CT sensitivity and specificity for pleural lesions are 90%–95% and 75%–80%, respectively. 4
Calretinin and CK 5/6 are important immunohistochemical markers for MPM. 5 In the present case, these markers were highly expressed in tumor cells on immunohistochemical staining of both sites.
In conclusion, we should take into account the possibility of extrathoracic spread by MPM arising from pleura and adhere strictly to guidelines, which state CT scan with CE and PET-CT can help reveal rare but possible distant metastasis, before deciding on the multidisciplinary treatment strategy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Editorial assistance was provided by Luca Giacomelli, PhD, and Aashni Shah (Polistudium srl), funded by internal funds. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.