
Abstract
Objective:
Although acute pancreatitis (AP) is a self-limited disease under supportive and medical treatment, it can have life-threatening potential in some patients. Results of studies reporting outcomes of AP-associated pancreatic malignancy are controversial. The aim of this study was to evaluate the severity and prognosis of pancreatic cancer (PC)–related AP by modified Balthazar score.
Methods:
A total of 354 patients hospitalized and followed up in our clinic between 2013 and 2019 were included in the study. Demographic data of all patients were recorded. The etiology of all cases was determined. According to the etiology, the cases were divided into 2 groups: AP related to pancreatic malignancy and AP due to nonmalignant causes. The patients underwent computed tomography of the abdomen within the first 12 hours of admission and after 3 to 7 days. Patients were evaluated and classified by modified Balthazar classification.
Results:
Malignancy-related AP was detected in 18 (5.1%) patients. A total of 336 cases (94.9%) were related to nonmalignant causes. There was no statistically significant difference in the severity of AP in both groups at admission and after 3 days (p > 0.05). The changes (regression, progression, or no change) in the disease severity at the first and the subsequent imaging were examined. There was no significant relationship between the 2 groups (p > 0.05).
Conclusion:
AP may be the clinical manifestation of PC or PC may induce AP in various ways. It was shown that the underlying malignancy did not adversely affect the severity and course of AP.
Introduction
Acute pancreatitis (AP) is an inflammatory pancreatic disease with sudden onset. 1 AP, which is self-digestion of the pancreatic tissue, is characterized by edema, bleeding, and necrosis in the pancreatic parenchyma and extrapancreatic tissue. The etiology of AP is commonly associated with gallbladder stones, alcohol consumption, and hypertriglyceridemia. Other causes include malignancy, invasive procedures, trauma, infections, drugs, genetic factors, and endocrine and metabolic disorders.1,2 A total of 5%–25% of AP cases are idiopathic.3,4
Recent studies have reported that AP may be an early finding of pancreatic cancer (PC). PC is the 12th most common cancer in the United States and is the 4th most common cause of cancer-related deaths.5,6 The incidence of PC with its high mortality and morbidity rates is predicted to increase over time and is estimated to become the second most common cause of cancer-related deaths by 2030. 7 In the literature, the rate of AP in patients with PC is variable and has been reported between 6.8% and 13.8% in various studies.8,9
Regarding the clinical course of AP, although most patients recover with supportive treatment in a short time, some patients may have life-threatening complications. 10 Although aging, obesity, early medical treatment, and hyperlipidemia are documented as independent risk factors affecting the course of AP, the relationship between AP and PC has not been adequately investigated.11–13 In studies examining the clinical course of AP related to malignancy, the data are contradictory. 14 In this study, we aimed to evaluate the severity and progression of PC-induced AP by modified Balthazar score.
Methods
Study design
A total of 354 inpatients with the diagnosis of AP in the gastroenterology department of our hospital between 2014 and 2018 were evaluated retrospectively. Diagnosis of AP was based on the guidelines of the American College of Gastroenterology. 15 Patients with chronic pancreatitis, patients with allergy to contrast agents, and pregnant women were excluded. Demographic data of all patients were documented. The etiology of AP was determined in all patients. Bile stones, alcohol consumption, drug/toxic and infectious causes, post–endoscopic retrograde cholangiopancreatography (ERCP), hyperlipidemia, hypercalcemia, genetic diseases, malignancy, and structural anomalies were evaluated as etiologic factors. Patients with unknown etiology were evaluated as idiopathic AP. All patients were evaluated with abdominal computed tomography (CT) imaging. However, small tumors can be hidden in advanced AP and considering that small tumors can be overlooked in CT imaging, magnetic resonance imaging (MRI) and magnetic resonance cholangiography (MRCP) were performed in all patients without etiology. Endoscopic ultrasonography (EUS) was performed in patients without pathology on MRI and MRCP. Patients with no pathology on EUS were evaluated as idiopathic AP. In all cases with AP due to an underlying malignancy, the diagnosis of PC was established on the imaging in our institution. There are common causes such as chronic pancreatitis, alcohol abuse, and genetic diseases that can lead to AP and PC. Patients with PC were excluded from the study if there was a common cause that can cause AP and PC. Once all the other causes of AP were excluded, the diagnosis of AP due to malignancy was posed. According to the etiology, the patients were divided into 2 groups as AP due to pancreatic malignancy and AP due to nonmalignant causes.
Severity of AP
All patients underwent contrast-enhanced abdominal CT in the first 12 hours and 3 to 7 days. Besides pancreatic necrosis and peripancreatic fluid collection, extrapancreatic findings such as ascites, pleural effusion, extrapancreatic parenchymal abnormalities (subcapsular collection, hemorrhage, or infarction), gastrointestinal tract involvement (inflammation, intramural fluid collection, or perforation), and vascular complications (arterial bleeding, venous thrombosis, or pseudoaneurysms) were evaluated. The Modified Balthazar score is used to evaluate disease severity in patients with AP (Table 1). Patients with scores of 0–2, 4–6, and 8–10 were identified as mild, moderate, and severe AP, respectively. 16
Modified Balthazar computed tomography severity index.
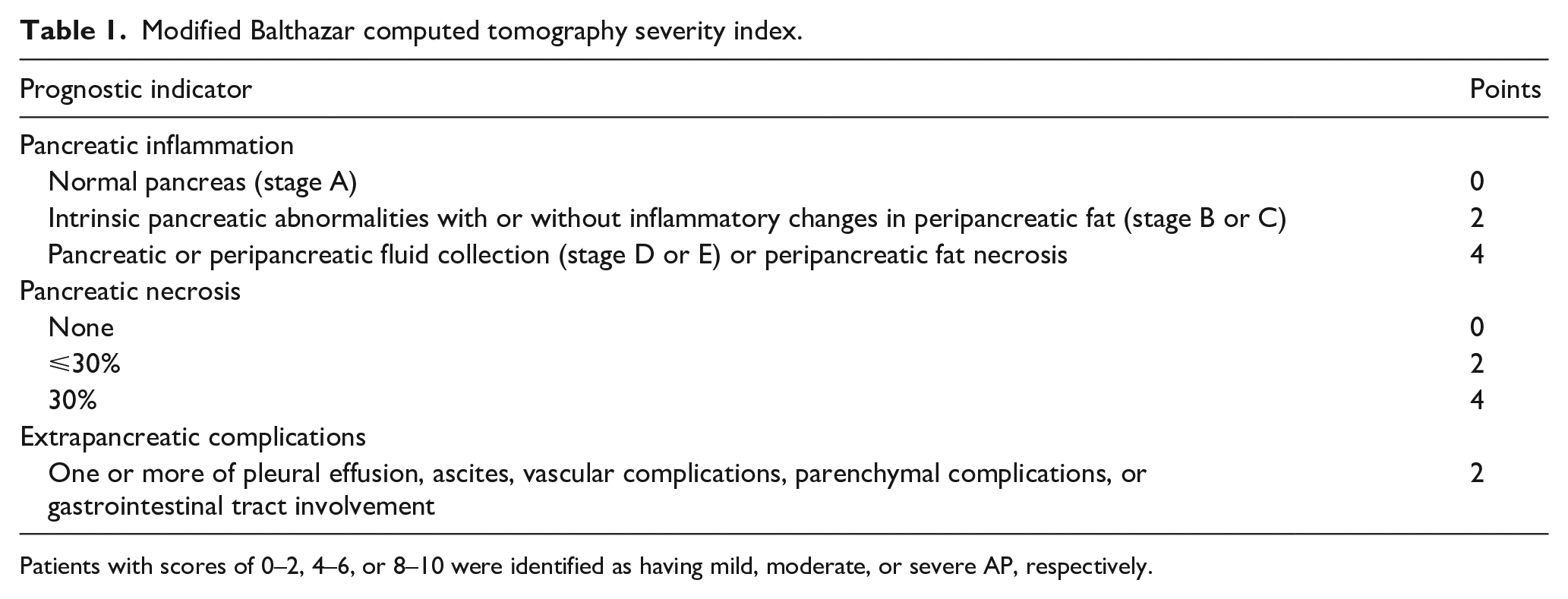
Patients with scores of 0–2, 4–6, or 8–10 were identified as having mild, moderate, or severe AP, respectively.
Ethics statement
Ethical approval for this study was obtained from the ethics committee of our institution. Principles of the Declaration of Helsinki and ethical standards of our institution’s human experimentation committee were followed.
Statistical analysis
The results were analyzed with the Statistical Package for Social Sciences 22.0 (SPSS, IBM Corp, Armonk, NY). Continuous variables were expressed as mean (± standard deviation) and categorical variables were expressed as frequency (%). Distribution was analyzed by Kolmogorov-Smirnov test, histogram, ± standard deviation (SD). Nonparametric variables of the different groups were analyzed by Mann-Whitney U test and parametric data were analyzed by independent t test. Categorical variables were analyzed using the chi-square test. p < 0.05 was considered statistically significant.
Results
A total of 354 patients with AP were included in the study. A total of 206 (58.2%) of the patients were female and the mean age of all patients was 54.8 ± 17.9 years (range 18–100 years). The number of patients with AP due to pancreatic malignancy was 18 (5.1%). A total of 336 patients (94.9%) presented AP of nonmalignant etiology. When we analyzed the subgroups of AP-related nonmalignant etiology, 193 (57.4%) cases were biliary, 50 (14.9%) drug or toxin substance, 28 (8.3%) secondary to ERCP, 10 (3%) hyperlipidemia, 8 (2.4%) alcohol-induced, 14 (4.2%) due to other causes (structural pathologies such as pancreas divisium and annular pancreas, hypercalcemia), and 33 (9.8%) patients had no cause (idiopathic AP).
Tumor stages of PC cases were analyzed. Stages of pancreatic cancer at the time of diagnosis were stage I (n = 1), stage II (n = 4), stage III (n = 5), stage IVa (n = 4), and stage IVb (n = 4). Regarding the severity of AP in both groups, there was no statistically significant differences between the two groups based on the modified Balthazar classification, evaluated by tomographies at the time of admission and after the third day of admission (p > 0.05). In addition, the changes in the severity of the disease (regression, progression, or no change) at the time of admission and the subsequent imaging were compared. There was no significant relationship between the two groups (p > 0.05) (Table 2).
Demographic characteristics and computed tomography (CT) scores in patients with acute pancreatitis (AP).
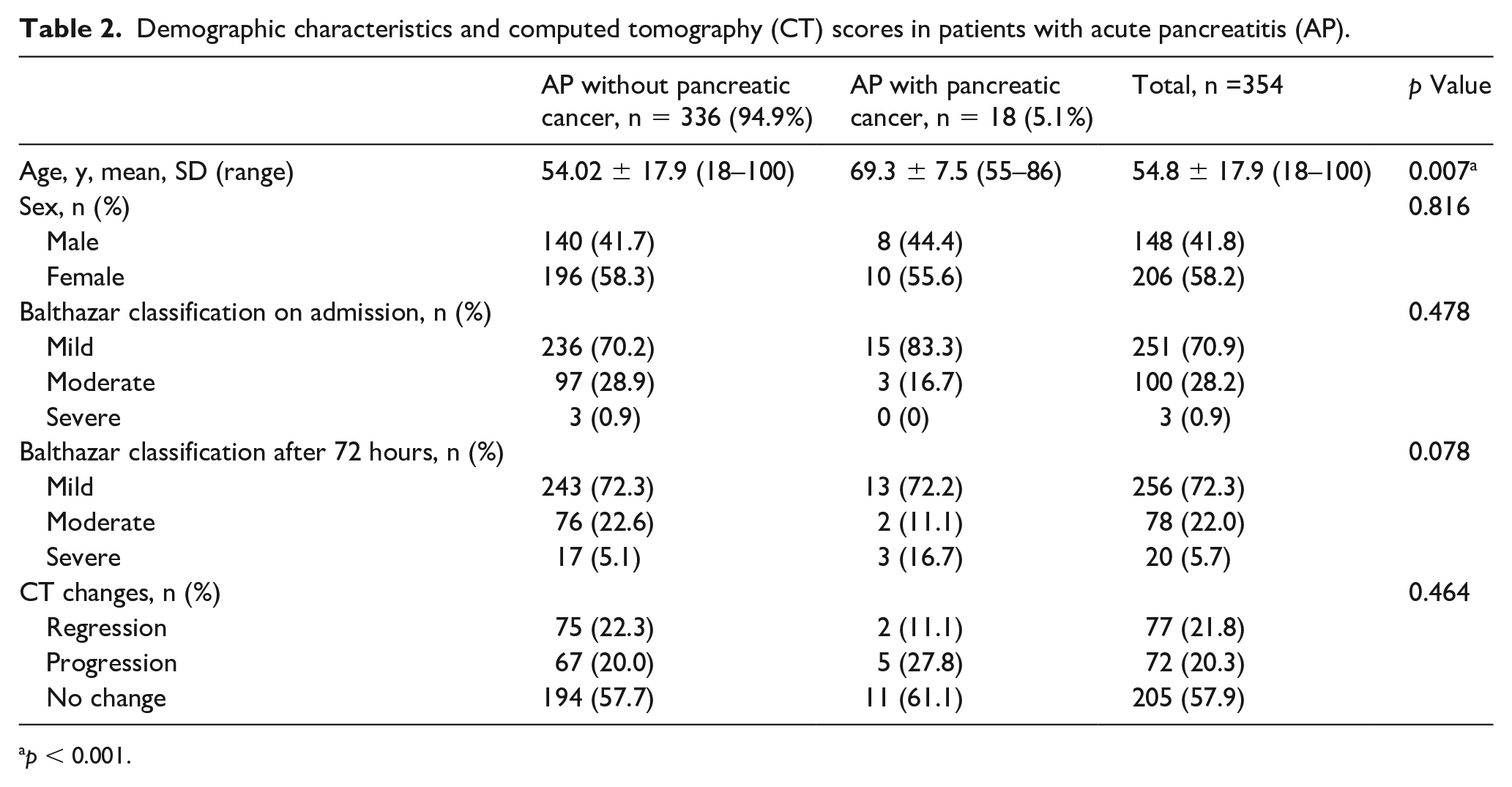
p < 0.001.
Mortality in all patients was analyzed. Whereas no deaths occurred in 18 patients with AP-related pancreatic malignancy, 5 of 336 patients with AP-related nonmalignant causes died. None of the cases ending in death occurred in the first 3 days.
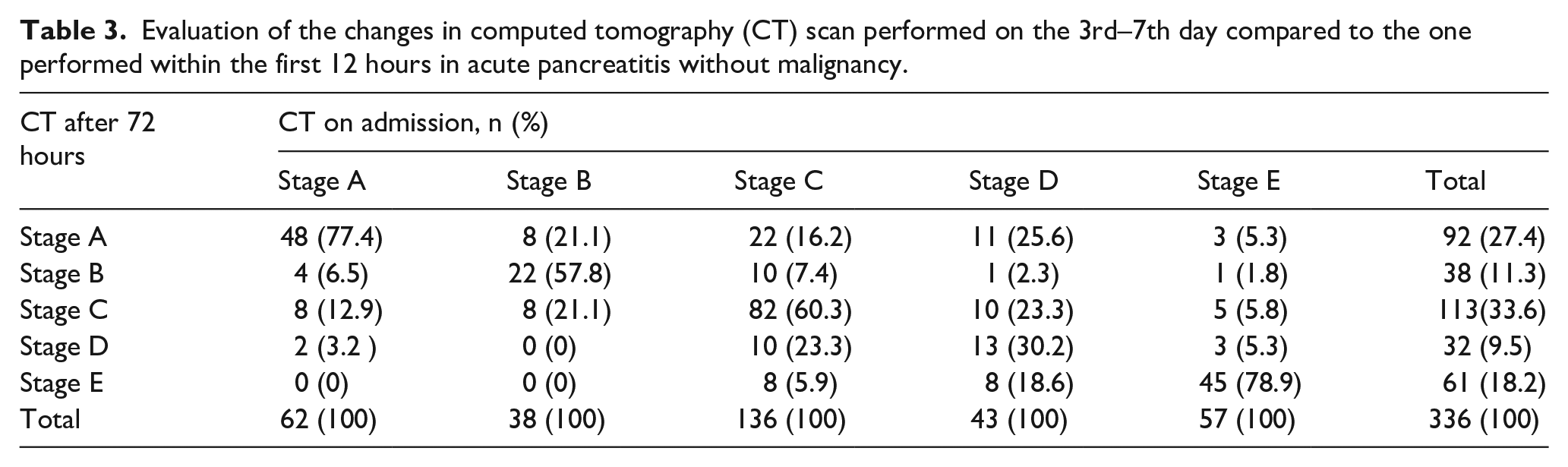
The progression of disease severity in both groups was analyzed. Of the 336 patients with nonmalignant etiology, 62 were in stage A on admission. On the imaging at the after third day, 48 (77.4%) patients remained stage A, while the others progressed to stage B, C, or D. Of the 38 patients with stage B on admission, 22 (57.8%) patients remained stage B, 8 (21.1%) patients regressed to stage A, and 8 (21.1%) patients progressed to stage C after 72 hours. Of the 136 patients with stage C on admission, 82 (60.3%) patients remained stage C on control imaging, 32 (23.5%) patients regressed to stage A or B, and 18 (30.2%) patients progressed to stage D or E after 72 hours. Of the 43 patients with stage D on admission, 13 (30.2%) patients remained stage D, 22 (51.4%) regressed to stage A, B, or C, and 8 (18.6%) patients progressed to stage E after 72 hours. Of the 57 patients with stage E on admission, 45 (78.9%) patients remained stage E, and 12 (18.2%) patients regressed to lower stages (Table 3).
Evaluation of the changes in computed tomography (CT) scan performed on the 3rd–7th day compared to the one performed within the first 12 hours in acute pancreatitis without malignancy.
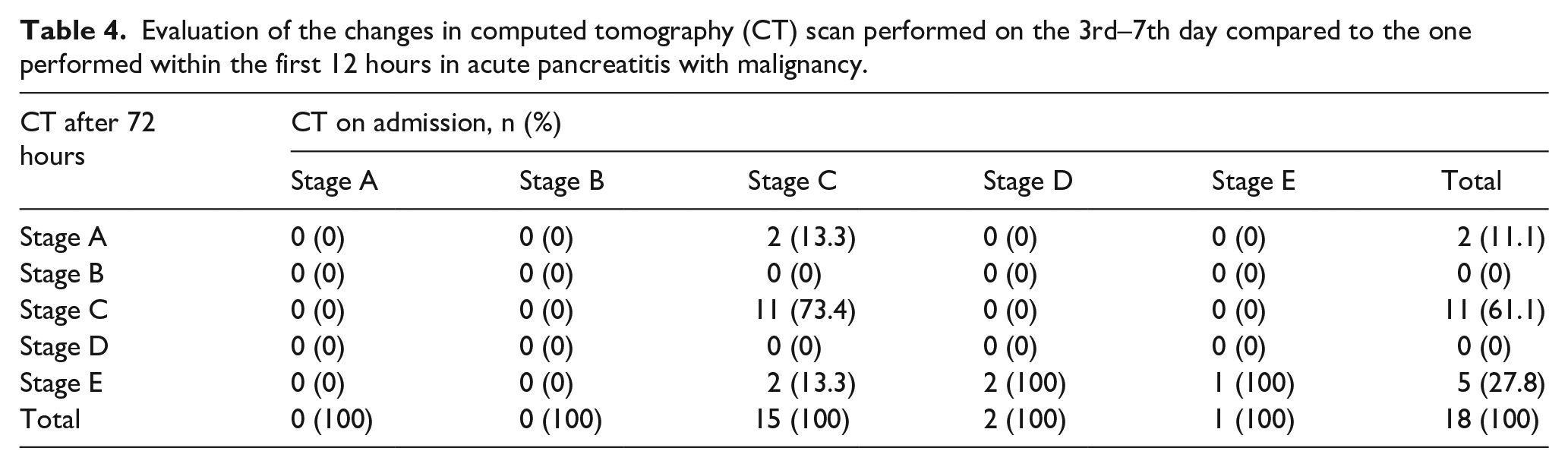
In the AP with pancreatic malignancy group, there were no patients with stage A or B. Of 15 patients with stage C on admission, 11 (73.4%) patients remained stage C, 2 (13.3%) patients regressed to stage A, and 2 (13.3%) patients progressed to stage E after 72 hours. Both of two stage D patients showed progression to stage E (100%). One patient with stage E remained stage E on control imaging (Table 4).
Evaluation of the changes in computed tomography (CT) scan performed on the 3rd–7th day compared to the one performed within the first 12 hours in acute pancreatitis with malignancy.
Discussion
PC is a rare etiology of AP and it has been reported that the prevalence of PC in individuals presenting with AP varies between 0.9 and 3.6%.9,14,17 However, the relationship between PC and AP is not clearly explained in the studies. The studies had shown AP to be induced by pancreatic tumor mass via pancreatic duct obstruction and may be the first clinical symptom of PC.18,19 Mujica et al. 14 reported that in addition to mechanical obstruction of the pancreatic duct, PC may induce AP by causing an ischemic condition caused by blood vessel obstruction by malignant cells or by direct activation of pancreatic enzymes by neoplastic tissue. However, there is no clear evidence as to whether PC is synchronous in patients with AP. 15 It should be taken into consideration that malignancy may also develop after AP. Data from experimental and epidemiologic studies suggest that AP may lead to PC. In a study involving 6000 patients with AP, a positive relationship was demonstrated between AP and PC. 20 In a study comparing 41,669 patients diagnosed with AP and 208,340 healthy individuals, it was found that patients with AP were at increased PC risk compared to the general population. Although the risk is highest in the first 2 years following AP diagnosis, after both 5 and 10 years of follow-up, it has been shown that the risk of pancreatic cancer is still twice that of the control group in patients with AP. 21
Due to pancreatic edema and necrosis in patients with AP, it is reported that it is difficult to differentiate mass lesions on imaging and therefore PC diagnosis may be delayed. AP diagnosis in patients with PC may be delayed due to symptoms of the primary disease masking AP symptoms. Likewise, Mujica et al. 14 reported that the 1-year overall survival rate in patients with PC was 20% but 28% in patients with PC presenting with AP. This suggests that patients presenting with AP may be diagnosed earlier for underlying malignancy.
The most commonly used assessment tools for AP disease are Ranson, Imrie, Acute Physiology and Chronic Health Assessment (APACHE) II, bedside index for severity in acute pancreatitis (BISAP), harmless acute pancreatitis score (HAPS), and Balthazar scores.22–24 Studies have reported that CT performed in the early stage shows a normal pancreas in 14%–30% of patients with AP and necrosis was not evident in the early hours, thus it is recommended that CT be performed after 72 hours. 25 In patients with AP, CT scanning also includes the detection of secondary findings such as tumor spread beyond the pancreas, invasion of surrounding structures, lymphadenopathy, or liver metastasis. 9
Clinical course of AP may be mild and self-limited, but it may also be severe, resulting in multiorgan failure and mortality. There are many factors playing an active role in the course of AP (age, hyperlipidemia, body mass index [BMI]). Studies have shown that the majority of patients with gallstone-induced AP have a mild clinical course. It has been reported that obesity is an independent risk factor for AP. Especially in Asian populations, patients with AP with high BMI tend to develop worse clinical outcomes and more severe course. 26 In this respect, different risk factors may contribute to AP severity based on different etiologies. 27 Although studies have reported that the pancreatic parenchymal morphology may be closely related to the clinical course of the disease, it is not clear whether pancreatic cancer is a predictor factor in the course of AP.28,29
Minato et al. 30 reported that there was no significant difference in age or sex between patients with AP with PC and patients with AP without PC. In addition, it was reported that 17 (94%) of 18 patients with AP with PC and 101 (72%) of 141 patients with AP without PC showed mild course. The difference was shown to be significant (p < 0.05). Gayam et al. 31 reported that there was no significant difference in age or sex between patients with AP with PC and patients with AP without PC. Mujica et al. 14 in a multicentric study including 45 patients with AP with PC reported that 60% of the patients were male and the mean age was 58 years. In terms of disease course, 40 (89%) cases were reported to be mild. In our study, although there was no sex difference, the AP with PC group was found to be significantly older. Comparing the severity of AP and changes in the course of the disease, evaluated by modified Balthazar classification, there was no significant relationship between the two groups. Based on these results, pancreatic malignancy does not adversely affect the progression of AP. Considering that AP has a worse clinical course in the elderly, it can be postulated that the progression of AP in patients with malignant disease is positively affected. Likewise, when the inflammatory process is considered to be the mainstay of AP development, the destructive effect of the mass and the secondary immunosuppressive state may limit the progression of inflammation in malignant cases.
This study has some limitations. It is a single-center retrospective study and other risk factors that play a role in disease progression are not discussed in detail. The strengths of our study are the high number of patients, clear identification of all etiologies, and evaluation of abdominal tomographies at the time of admission and at 72 hours by the same radiologist.
In conclusion AP may be the clinical manifestation of PC, and PC may induce AP in various ways. There is no significant difference in the severity and course of the disease in patients with AP due to malignancy compared to nonmalignant AP. Considering that patients with malignancy are older, the underlying malignancy does not have a negative effect on the clinical course of AP. In order to clarify this, multicentric studies with higher sample size are needed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.