
Abstract
Introduction:
Surgical management of patients with multiple metastases from mucinous rectal carcinoma is feasible.
Case description:
We present a case of a 66-year-old woman with a late onset of peritoneal and coccygeal metastasis from a mucinous rectal carcinoma treated with cytoreductive surgery. After 30 months from rectal resection, the patient underwent exploratory laparotomy with resection of all tumor localizations by means of pelvic peritonectomy, complete supracolic omentectomy, jejuneal resection, appendectomy, and excision of the mobile part of the coccyx.
Conclusion:
This report aims to point out the atypical late-onset recurrence presentation and management of a mucinous carcinoma of the rectum.
Introduction
Metastatic disease is discovered in 20%–25% of patients with colorectal cancer (CRC) at initial diagnosis and it will eventually be diagnosed in up to 50% of patients with early-stage disease. 1 Substantial progress has been made during the last 2 decades: highly effective drugs and molecularly targeted agents have significantly improved systemic disease control and patient survival. 1
Although liver metastases are the most common manifestation of disease progression, different anatomic sites may be involved. In addition, different CRC genotypes may be related to unusual patterns of spread, malignant potential, and prognosis. 2 Besides disease-free interval, degree of tumor differentiation, number and volume of metastatic lesions, the anatomic site of the metastases has profound implications on the clinical management and prognosis of stage IV CRC. 3 Liver resection, when feasible, is the current standard treatment for liver metastases. Lung-limited disease shows a more favorable outcome, whereas survival of patients with bone, peritoneal, and brain metastases is poorer. 4
In patients with multiple metastases, combined distant and locoregional disease, or less common metastatic sites, the treatment strategy is less standardized. These patients are often treated by palliative systemic chemotherapy, and the role of surgery is not well-defined. In this report, we describe the successful surgical management of a patient with peritoneal and bone metastases from mucinous rectal carcinoma. The correlation of such an uncommon metastatization pattern with the patient’s clinical–pathologic features and oncogene mutation profile is also discussed.
Case report
In September 2017, a 66-year-old woman presented to our unit with a poorly differentiated mucinous rectal adenocarcinoma located 3 cm from the anal verge. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed a cT2 N0 tumor, without distant metastatic lesions. Her previous medical history was notable for a hystero-oophorectomy in 2004 for endometrial adenocarcinoma, followed by adjuvant radiotherapy (45 Gy).
The patient underwent an ultra-low resection of the rectum with total mesorectal excision, local-regional lymphadenectomy, and colorectal anastomosis. A defunctioning loop colostomy was performed. The postoperative course was uneventful. Pathologic examination revealed a mucinous adenocarcinoma of 7×3 cm located 1 cm from the distal margin and 14 cm from the proximal margin; circumferential margin was negative. Peritoneal regression grading score was 2 and tumor regression grade was 3, according to Mandard classification.
Final histology revealed pT2 G3 N0, with 11 local–regional lymph nodes examined. Extramural vascular invasion was present; intramural vascular and perineural invasion were absent.
Oncogenic mutations in the hotspot regions of 50 cancer-related genes (Hotspot Cancer Panel v2) were assessed in a primary tumor sample by means of targeted next-generation sequencing through the Ion Torrent Personal Genome platform (Life Technologies, Waltham, MA), as described previously. 5 Molecular analysis showed mutations p.G12V in exon 2 and p.Q61H in exon 3 of KRAS, mutation p.E271K in exon 8 of TP53, and mutation p.R465H in exon 9 and p.R479Ter in exon 10 of FBXW7, mutation p.P1441H_fs Ter32 in exon 15 of APC, and mutation p.R201H in exon 8 of GNAS.
Microsatellite instability, assessed by both immunohistochemistry (loss of hMLH1, hMSH2, hMSH6, or PMS2 expression) or using 5 mononucleotide repeat microsatellite markers (BAT-25, BAT-26, NR-21, NR-22, and NR-24), was absent.
Nine months after surgery, the patient underwent colostomy closure. Oncologic follow-up was uneventful until April 2019, when his carcinoembryonic antigen (CEA) rose to 674.8 ng/mL. CT scan showed small nodules in the Douglas pouch and one on the peritoneum above the rectum. Large nodules in the omentum conditioning omental cake and a large jejunal lesion (40 mm) were also identified. Pelvic MRI showed a 27-mm coccygeal rounded mass.
After discussion by our multidisciplinary colorectal cancer board, we proposed a comprehensive treatment approach consisting of preoperative systemic chemotherapy (s-CT) followed by surgical reevaluation for a possible complete cytoreductive surgery.
After six cycles of systemic treatment with FOLFOX and bevacizumab, CT scan showed a volume reduction of <30% in all the metastatic lesions, classified according to RECIST classification as stable disease. The patient was given an additional six cycles of the same chemotherapy, but the treatment had to be interrupted before the last administration for suspicion of rectovaginal fistula, later confirmed by pelvic MRI and fistulography. CT scan showed stability of the abdominal lesions and positron emission tomography scan a reduction in the uptake level of the rectal lesion and complete absence of uptake by pelvic lesions. CEA level was 431.5 ng/mL.
In March 2020, 30 months after the rectal resection, the patient underwent surgery with macroscopically complete resection of all tumor localizations by means of pelvic peritonectomy, complete supracolic omentectomy, jejuneal resection, and appendectomy. In addition, excision of the mobile part of the coccyx was performed (Figure). Peritoneal cancer index at surgery was 7. A colostomy was performed to treat the rectovaginal fistula. The postoperative course was uneventful. Pathologic examination revealed, in all specimens, a mucin-secreting, poorly differentiated adenocarcinoma with margins free of disease. After 7 months of follow-up, the patient is symptom free and CT scan is negative for recurrence.
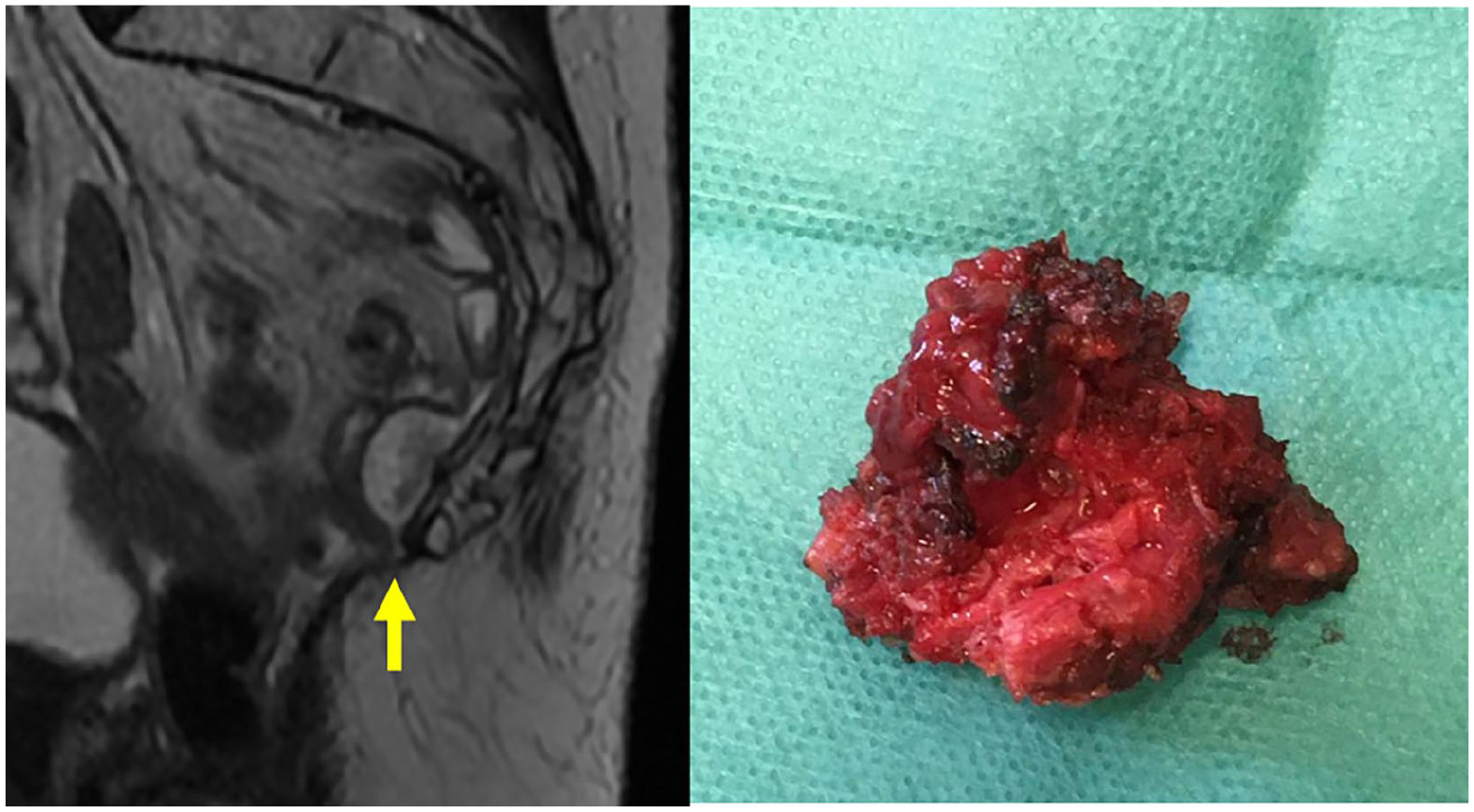
Magnetic resonance image of the coccygeal metastasis and picture of the surgical specimen.
Discussion
To our knowledge, this is the first report of a patient treated by simultaneous complete resection of peritoneal and bone metastases from CRC. Our group and other groups have reported series of patients with both liver and peritoneal metastases treated by cytoreductive surgery, hyperthermic intraperitoneal chemotherapy (CRS/HIPEC), and hepatic resections. 6
Together with early diagnosis and the development of highly effective systemic and targeted agents, the concept of local–regional metastatic disease represents one of the most relevant advancements in CRC management. 1 Comprehensive treatment plans involving s-CT, surgical resection, and/or local–regional treatments have become the standard for isolated liver, lung, or peritoneal metastases, 3 as well as preoperative radiochemotherapy and surgery for pelvic recurrences.
In the literature, the rate of stage IV CRC with multiple metastatic sites is about 40%–50%. 4 Initially, this was perceived as a contraindication for surgery, but today even patients with multiple sites of metastatic CRC are increasingly considered for surgical metastasectomies. 3 Nevertheless, the standard treatment for extrapelvic recurrences or combination of peritoneal and haematogenous metastases is not well-defined.
Resection of colorectal peritoneal metastases by CRS, with or without HIPEC, has increased patient survival over historical controls and in a randomized trial, as compared with palliative s-CT. Reported overall survival can reach up to 62 months if macroscopically complete cytoreduction is achieved. 7 The procedure is now endorsed by the European Society for Medical Oncology. 1
In our patient, HIPEC was not performed based on the recent randomized PRODIGE-7 trial that failed to demonstrate a benefit from oxaliplatin-based HIPEC in addition to s-CT and complete CRS. 8 The same lack of benefit was found with mitomycin-based HIPEC in a retrospective controlled nonrandomized study. 9 Extraperitoneal metastases are an adverse prognostic factor in patients undergoing CRS/HIPEC, although an important survival benefit can be achieved if peritoneal involvement is limited. Accordingly, as we are in the process of designing a clinical trial to define which subset of patients may benefit from HIPEC, the current state-of-the-art treatment for colorectal peritoneal metastases (i.e. s-CT and complete CRS) was offered.
The proportion of patients with concurrent resectable peritoneal and bone metastases from CRC is unknown. In recent population-based studies, peritoneal metastases were detected in 3.8%–4.3% of patients at first diagnosis, while bone metastases range from 3% to 10%. 10 Riihimäki et al. 10 reported that the percentage of patients with peritoneal metastases who also had bone metastases was 4% and 11% for colon and rectal cancer, respectively. Conversely, the percentage of patients with bone metastases who also had peritoneal metastases was 10% for colon and 7% for rectal cancer. 10
The pattern of metastatic spread in these patients is peculiar. The risk for peritoneal metastases development is higher in right-sided CRC and the lowest for rectal tumors located below the peritoneal reflection. On the other hand, mucinous carcinoma is known to be more prone to peritoneal metastases according to the Sugarbaker theory: the pressure exerted by mucin on the bowel wall results in tissue planes separation and peritoneal invasion. 11 Bone metastases have been reported to be more commonly associated with rectal and mucinous histology, as in this patient.
KRAS, NRAS, BRAF, and PIK3CA are downstream components of the epidermal growth factor receptor (EGFR) signaling pathway that regulates cell proliferation and survival. Growing evidence suggests that their mutations may affect prognosis and patterns of metastatic spread. 2 KRAS is the most commonly activated oncogene in CRC, associated with adenoma–adenocarcinoma transition and an higher incidence of lung, bone, and brain metastases. 12 It has also been reported to correlate with poorer prognosis after curative treatment of liver and peritoneal metastases. 12 The association of colorectal peritoneal metastases with mutated BRAF or wild-type PIK3CA has been reported.
FBXW7 is a tumor suppressor that, if mutated in CRC, seems to be associated with worse prognosis, but not with any clinical–pathologic variables (except for PIK3CA mutations). GNAS mutations are present in only 1%–3% of patients with CRC and are associated with the progression from villous adenoma to mucinous carcinomas and KRAS mutations, as in this patient, but also with right-sided primaries. 2
The present report strongly suggests that a complex and rare manifestation of metastatic CRC can be effectively and safely managed by a surgical and comprehensive approach in a highly specialized center. Therefore, in-depth knowledge of prognosis among patients with different metastatic profiles of CRC is important to put resection of metastases into perspective with other therapies. Better understanding of the correlation between site-specific metastatic patterns and clinical, pathologic, and genetic features would improve the management of these patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.