
Abstract
Background:
Adult granulosa cell tumor (AGCT) of the ovary generally has a good prognosis. Recurrences tend to be late and confined to the abdominopelvis. Bone metastases are extremely rare. We report an extremely rare case of AGCT with synchronous multiple bone metastases and discuss diagnostic procedures and management.
Case description:
A 35-year-old woman presented with abdominal bloating. On the day of surgery, acting on the complaint of right shoulder pain, an X-ray revealed a permeative lesion involving the neck of humerus, suggestive of a metastatic pathologic fracture. The patient underwent a full staging debulking surgery. Further imaging demonstrated multiple bone metastases. Histology confirmed an AGCT of the ovary. Diagnosis was established by a core bone biopsy from the left femur showing cells consistent with those seen with granulosa cell tumor. The patient received adjuvant chemotherapy with concurrent zoledronic acid as targeted therapy for her bone metastases. Endocrine systemic maintenance treatment was given. The patient rapidly deteriorated and died from her disease at 20 months from the initial diagnosis.
Conclusion:
Unpredictable biological behavior and clinical manifestations raise a high degree of suspicion for accurate AGCT diagnosis. Management of bone metastases often warrants input from the multidisciplinary team, and treatment may involve chemotherapy, palliative radiotherapy, or orthopaedic interventions.
Introduction
Adult granulosa cell tumors (AGCTs) of the ovary account for approximately 2% of all ovarian cancers. They mainly present at a later stage in life and are considered to have a good prognosis. 1 Lymphatic and distant vascular metastases to the liver, lung, kidney, and heart have been documented. Extra-abdominal metastases are rare, and bone metastases are even rarer. 2 We report an extremely rare case of AGCT in a young woman with synchronous multiple bone metastases and discuss diagnostic procedures and management.
Case description
A 35-year-old woman was referred with a massive increase in abdominal girth, urgency, and constipation. She reported gaining weight over the previous few months and “feeling foetal movements.” Following IVF treatment, she had given birth to a healthy child by caesarean section 15 months previously. She had breastfed for 14 months. Her body mass index was 26. She had type 2 diabetes and was on metformin. Physical examination revealed a large pelvic mass with size similar to that of a 38- to 40-week pregnancy.
Following initial ultrasound, magnetic resonance imaging confirmed a 23-cm complex mass arising out of the pelvis, likely related to the right ovary, resembling an ovarian dysgerminoma with associated mild ascites (Figure 1 [A]). Germ cell markers were negative; CA125 and lactate dehydrogenase were elevated. Inhibin levels were not available. The CA125 levels had tripled from presentation to surgery. Care was centralised following germ cell and gynaecologic oncology multidisciplinary team reviews, and the patient was scheduled for surgery. The patient did not opt for a fertility-sparing procedure.
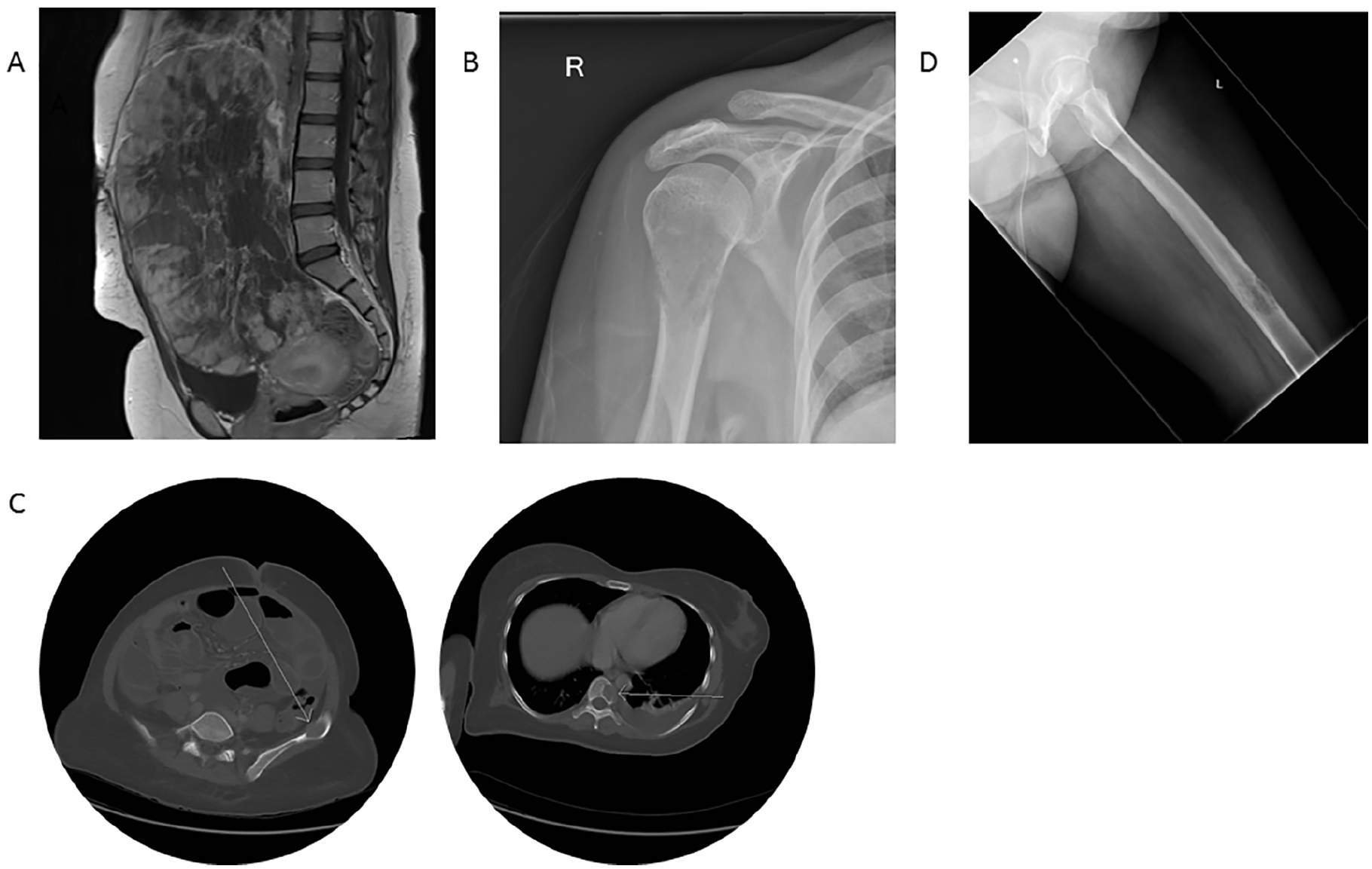
(A) T1-weighted magnetic resonance imaging shows a 23-cm complex mass separate from the uterine body, arising out of the pelvis, resembling an ovarian dysgerminoma (sagittal view). (B) Right shoulder X-ray shows a permeative lesion involving the right neck of humerus with a moth-eaten appearance of the cortex and medulla. (C) Axial non-contrast computed tomography shows lesions in the left iliac blade and in the bodies of T8. No alternative primary site was identified. (D) Femur and left knee X-ray shows permeative aggressive lytic lesion in the femoral shaft at the junction of the middle and distal thirds, in keeping with metastatic disease.
When the patient attended for surgery, she reported pain over her right shoulder of 10 days’ duration. An X-ray revealed a permeative lesion involving the right neck of the humerus with a moth-eaten appearance of the cortex and medulla suggestive of a metastatic pathologic fracture (Figure 1 [B]). Consensus among three senior consultants resulted in proceeding with surgery. She underwent a full staging laparotomy including total abdominal hysterectomy, bilateral saplingo-ooperectomy, omentectomy, pelvic and para-aortic lymphadenectomy, and mesenteric biopsies. Surgical findings were unremarkable except for a large complex right ovarian mass, which was removed intact. A postoperative computed tomography (CT) scan revealed several more lytic bone metastases including the right humeral head, right femoral head, and left femoral diaphysis, three lesions in the left iliac blade, and lesions in the T8 and T10 vertebral bodies (Figure 1 [C]). No alternative primary site was identified. Subsequently, a right femur X-ray revealed a permeative aggressive lytic lesion in the femoral shaft measuring approximately 50 × 19 mm (Figure 1 [D]). An anterior cortical breach with associated periosteal reaction was demonstrated, in keeping with an impending pathologic fracture. Biochemically, calcium levels remained within normal ranges throughout, despite the lytic bone lesions. At the orthopaedic review, it was determined that the patient was at high risk of pathologic fracture of her left femur. In addition to a non-weight-bearing plan, she was scheduled for prophylactic intramedullary nail placement and bone biopsy. Bone scintigraphy showed foci of increased tracer activity corresponding to previously identified bone metastasis sites. Serial CT imaging confirmed progressive bone metastasis. A bone core biopsy was taken during the intramedullary nailing. A mammogram showed no focal abnormality and serum electrophoresis was negative, ruling out multiple myeloma.
Histopathology of the right tube and ovary suggested an AGCT with an aggressive morphology. The specimen measured 200 × 180 × 180 mm and weighed 3.7 kg. The external surface was irregular with intact capsule. Attached unremarkable fallopian tube was identified. The cut surface of the tumor was solid and variegated with pale areas. The fat was adherent to the capsule. Microscopically, there were predominantly solid sheets and nests of malignant tumor cells with microfollicular and tubular patterns resembling Call-Exner bodies. The cells showed moderate degree of nuclear pleomorphism and frequent mitoses. Several foci of vascular invasion were seen. Immunohistochemistry was positive for inhibin, calretinin, and CD56, and negative for chromogranin, synaptophysin, pan-cytokeratin, epithelial membrane antigen, WT1, p53, and PLAP (Figure 2 [A] through [D]). Histology of the core bone biopsy from the left femur showed cells akin to those seen with tumor from the right ovary, staining strongly for calretinin and CD56 (Figure 3 [A] and [B]). Facilities to perform FOXL2 immunohistochemical stain and molecular studies were not available at our center.
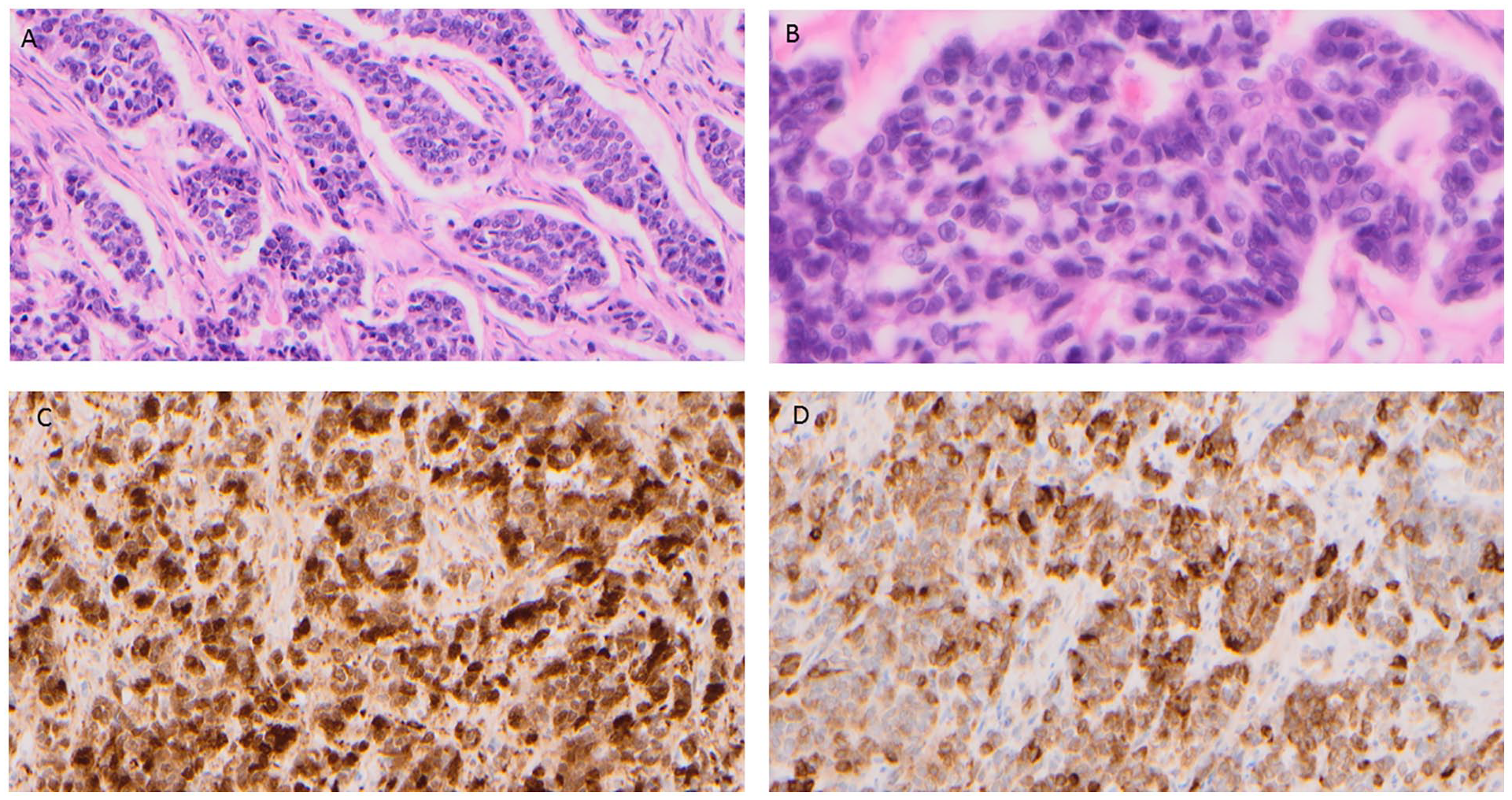
Hematoxylin & eosin–stained section of right ovarian tumour: (A) 20× magnification; (B) 40× magnification; (C) calretinin positivity, 20× magnification; (D) inhibin positivity, 20× magnification.
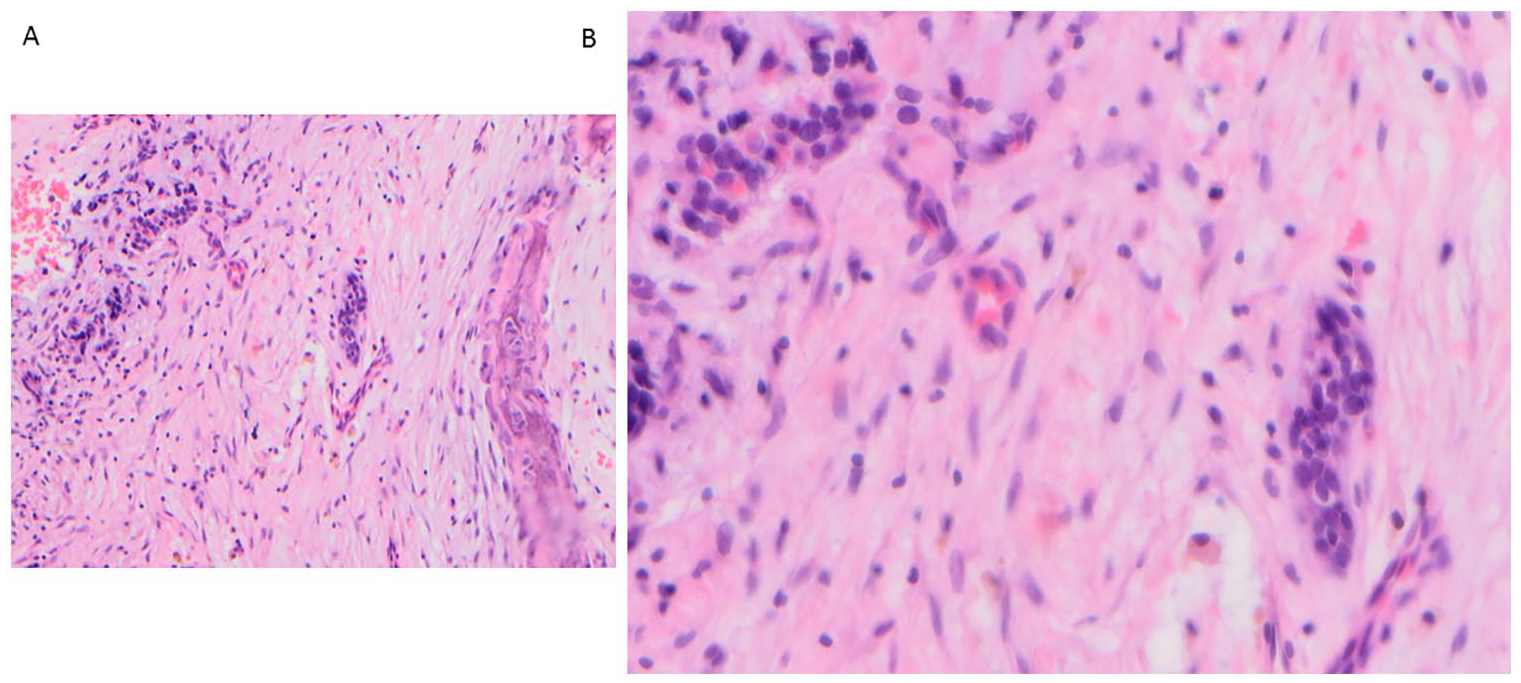
Metastatic adult granulosa cell tumour, reaming of intramedullary cavity left femur: (A) 20× magnification; (B) 40× magnification.
The differential diagnoses of juvenile granulosa cell tumor and small cell carcinoma of hypercalcaemic type were considered, but morphology and immunohistochemical profile did not favor either of these diagnoses. A clinical diagnosis of International Federation of Gynaecology and Obstetrics (FIGO) stage 4b AGCT of the ovary with multiple synchronous bone metastases was made.
A baseline CT scan prior to chemotherapy showed progressive bone metastasis disease and two new liver lesions. The patient was commenced on weekly carboplatin and paclitaxel chemotherapy for six cycles with concurrent zoledronic acid as targeted therapy for her bone metastases. Repeated imaging showed no new measurable disease in the abdomen and stable bone disease. She continued to receive zoledronic acid on a 4-weekly schedule and was offered palliative radiotherapy to bone metastasis sites of sustained pain. At 4 months after platinum-based chemotherapy completion, she experienced a marked pain increase. A further bone scan demonstrated new focal uptake areas in the lumbar spine, pelvis, and right femur. She was commenced on palliative endocrine therapy with alternating megace/tamoxifen and 4-weekly zoledronate infusions, resulting in temporary improved pain control. Subsequent bone scan showed new metastases within L1-L2, the left posterior iliac bone, and the right pubis. She underwent palliative radiotherapy to multiple bone sites.
Acute onset leg weakness triggered further imaging, which confirmed extensive multilevel bone disease but no evidence of cord compression. Subsequently, disease progression was manifested with significantly increased bulky liver disease, innumerable new pulmonary metastases, and interval tumor growth. The patient was admitted to hospice with symptoms suggestive of skull metastases. She rapidly deteriorated and died of her disease 20 months from her initial diagnosis date.
Discussion
Patients with AGCT are typically middle-aged postmenopausal women presenting with a pelvic mass or endocrine syndromes, due to a functional oestrogen secreting tumor. 1 In contrast to epithelial ovarian cancers, granulosa cell tumors are characterized by indolent growth with a tendency toward late intraperitoneal recurrence. Herein, we present an extremely rare case where simultaneous multiple bone metastases arose from an AGCT. This is the first case reported of bone metastasis alongside the primary rather than as a recurrence.
In high-grade ovarian cancer, non-serous histology and the presence of liver and lung metastases, all reflecting a vascular spread pattern, have been associated with de novo bone metastasic development resulting in a poor prognosis. 2 Bone metastasis is a complex multistep process that involves critical interactions between cancer osteoblastic and osteolytic cells. Studies suggest a direct relationship between increasing osteoclast activity and the risk of developing osteolytic bone metastases, which explains the preventative effects of anti–bone resorptive drugs regardless of menopausal status. 3 This extremely rare clinical presentation can be explained by at least two hypotheses that are not necessarily mutually exclusive. The first one is osteoporosis-induced bone metastasis by disseminated tumor cells; their detection in breast and ovarian cancer has been associated with reduced survival. 4 An alternative hypothesis lies between the close relationship of solid cancers and bone metastasis with sex hormones (particularly oestrogen). Murine models with a genetic propensity to develop spontaneous AGCTs with bone metastases have been used to imitate the human scenario. 5 Our patient had type 2 diabetes mellitus, which is known to increase marrow adiposity, thus resulting in skeletal frailty. Unopposed oestrogen environments, such as obesity, may be associated with AGCT development through endogenous oestrogen exposure. It is unclear whether recent pregnancy, a highly oestrogenic state, could have predisposed the patient to AGCT by excess oestrogen potentiating granulosa cell hyperplasia to the point of unregulated, autonomous oestrogen production, leading to malignant transformation. It is not surprising that such a rapidly growing tumor was clinically consistent with the development of widespread metastases. Hypothesis-generating studies with powerful study design are required to address this.
Mutant FOXL2 is a potential driver, although not pathognomonic, but the malignant behavior of AGCTs can be additionally driven by DNA mismatch repair deficiency. 6 Pathologically, AGCTs appear as large unilateral tan–yellow masses due to steroid production. The diagnosis of AGCTs is mostly based on the typical morphology of the granulosa cells with their coffee bean–like, angulated, and grooved nuclei. The presence of Call-Exner bodies makes correct diagnosis easier; however, they are not always found, and thus are not indispensable to diagnosis. Immunohistochemistry is essential for histologic diagnosis of suspected metastases, especially when alternative primary sites are considered. Immunohistochemically, AGCT is positive for inhibin, vimentin, and calretinin, negative for epithelial membrane antigen, placental alkaline phosphotase, synaptophysin, and lymphoid markers. Up to 60% of AGCTs can be androgen receptor–positive, suggesting a potential role for antiandrogen therapy. The potential role of immunotherapy appears more limited.
Our patient presented with several therapeutic challenges. The only absolute prognostic factor was the presence of extraovarian spread at the time of initial diagnosis. A recent Cochrane review study concluded that there was no difference in disease recurrence rates, based on execution and type of adjuvant chemotherapy or on the type of surgery or surgical approach, other than that surgical staging may be important. 7 In women with ovarian cancer and bone metastases, the median survival time can be prolonged from 3 months to 18 months with primary debulking surgery. 2 Following surgery, adjuvant chemotherapy with weekly carboplatin and weekly paclitaxel was chosen to balance toxicity, but treatment options were limited. The standard therapy for a AGCT would be a combination of bleomycin, etoposide, and cisplatin (BEP), but the optimal dose is not well-defined. 8 Different surgical approaches and/or adjuvant therapy appear not to affect the outcome. The Gynaecologic Oncology Group is currently conducting a randomized phase II trial (NCT01042522) of BEP versus a combination of paclitaxel and carboplatin for patients with newly diagnosed and recurrent chemotherapy-naive sex cord stromal tumors of the ovary. Some AGCTs also respond to hormone-based therapy. For instance, response to progestin therapy has been reported early in the treatment of recurrent AGCT. Nonetheless, concerns were expressed as our patient’s symptoms were too severe to rely on the slower response generally seen with hormone therapy. Given the progressive disease and her worsening symptoms, it was considered appropriate to change her systemic therapy.
Cancer progression is often paralleled by a decline in bone mass, increasing the risk of fractures. Chemotherapy was no longer an option, as the patient’s disease became resistant. The likelihood of a benefit from further chemotherapy was relatively modest, yet had to be considered. Another option was endocrine therapy. There is evidence from case reports showing some benefit from using an alternating regimen of megace/tamoxifen every 3 weeks, commonly used in endometrial cancer. Ultimately, we needed to accept that the zoledronate infusions would not control the metastatic progression due to the overly aggressive tumor morphology. While these antiresorptive agents can help mitigate cancer-associated osteoporosis in patients with cancer, concerns arise regarding long-term complications, including osteonecrosis of the jaw and atypical fractures of the femur.
In conclusion, this is the first report of an ovarian AGCT with synchronous multiple bone metastases. Only three cases of female AGCT relapse to the bones have been previously reported.3,9,10 It is critical to detect and diagnose patients with AGCTs as early as possible due to unpredictable biological behavior and clinical manifestations. Every symptom should be thoroughly evaluated when an AGCT diagnosis is made. Bone metastases are extremely rare and may be treated aggressively. Any factors associated with bone metastasis development can be potentially used for early screening and tailored treatment. Going forward, it would be interesting to examine what about AGCT promotes such rare bone metastases.
Footnotes
Acknowledgements
The authors thank the patient for her cooperation and participation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.