
Abstract
Background:
Adrenalectomy is the gold standard for the treatment of primary adrenal ganglioneuroma. Preoperative differential diagnosis of ganglioneuroma is difficult and histopathologic examination is required to confirm the diagnosis.
Patient:
A 61-year-old woman, who was followed and treated by the medical oncology department because of lung carcinoma pathology squamous cell T4N0Mx, presented to our clinic due to a 15×8-mm nodule with a calculated relative wash-out rate of 40% in the right adrenal gland lateral edge, which was observed on computed tomography examination.
Conclusion:
Adrenal ganglioneuroma is a rarely seen, hormonally inactive, benign tumor. Final diagnosis can be made with histopathologic examination. Adrenalectomy is the standard treatment preferred for ganglioneuroma. Knowing the clinical appearance and good pathologic specialization are important adjunct matters in diagnosis. Laparoscopic adrenalectomy has become the gold standard in most patients with adrenal tumors.
Introduction
The incidental detection of adrenal masses in clinical practice has become widespread in parallel to developments in imaging methods. As reported in the literature, the prevalence of incidentally detected adrenal masses is 0.2%–3%. 1 Adrenal ganglioneuroma (AGN) is a generally benign, nonfunctional adrenal tumor that is rarely reported in the literature. Adrenalectomy is the gold standard for the treatment of primary AGN. Preoperative differential diagnosis of ganglioneuroma is difficult and histopathologic examination is required to confirm the diagnosis.
Incidentally detected adrenal masses (AI) are being diagnosed more frequently with developments in abdominal imaging techniques. These tumors consist of a wide lesion range including hormone inactive adenomas, subclinical hormone-secreting tumors, various benign lesions, and malignant adrenocortical carcinomas. A range of specific examinations should be performed to define the malignancy potential or any potential hormonal secretion for AIs. 2 As reported in the literature, the prevalence of AI is 0.2% in young patients and 3% in populations aged over 50 years. 1 Surgical resection is vital for large atypical or hormone active lesions because they are symptomatic and have the potential to become malignant. 3 In the past 20 years, laparoscopic adrenalectomy, which is a minimally invasive method, has become the standard surgical method for the removal of most adrenal masses. 4 We present a patient who was treated for lung cancer and had an adrenal mass detected in follow-up interpreted as metastasis. The patient underwent laparoscopic adrenalectomy.
Case Report
A 61-year-old woman, who was followed and treated by the medical oncology department because of lung carcinoma pathology squamous cell T4N0Mx, presented to our clinic due to a 15×8-mm nodule with a calculated relative washout rate of 40% in the right adrenal gland lateral edge, which was observed on computed tomography (CT) examination (Figure 1).
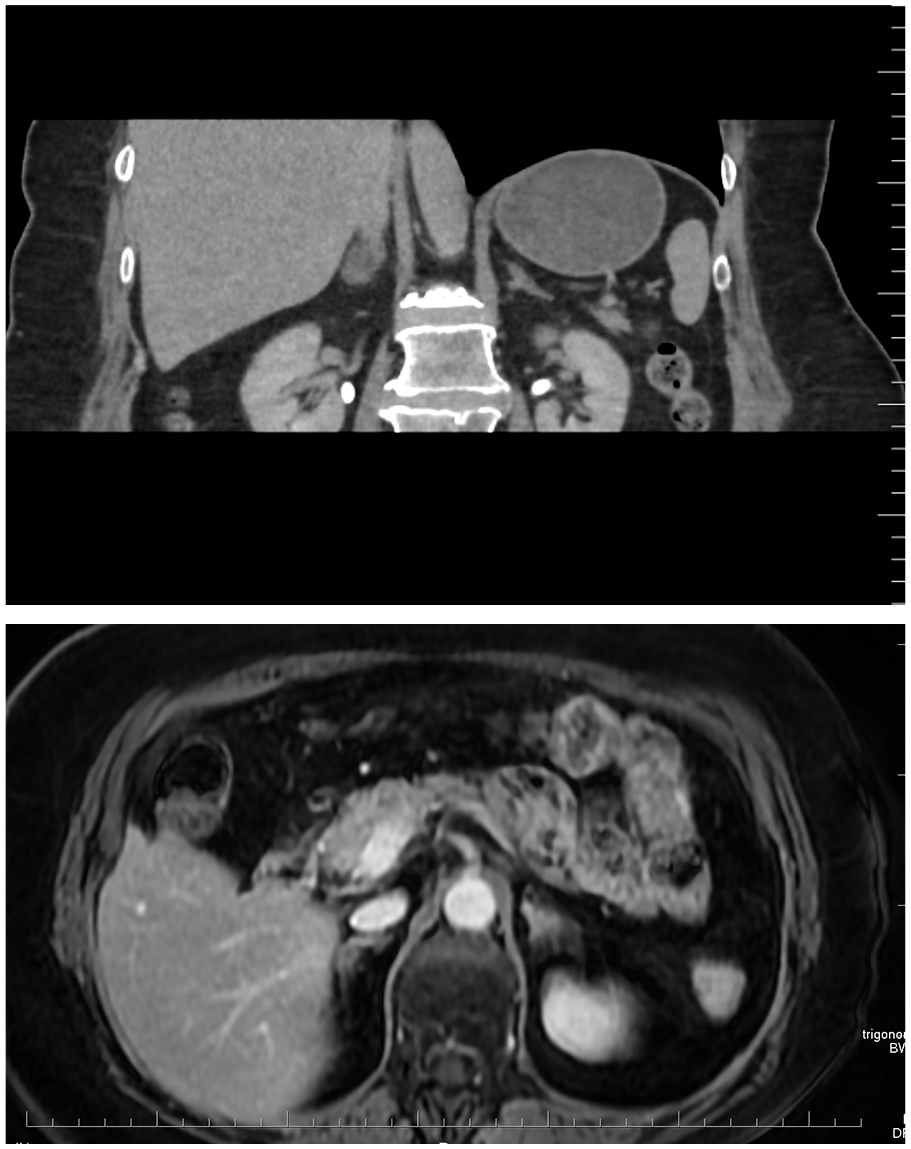
Upper abdominal magnetic resonance imaging and computed tomography examination reveal a 15×8-mm nodular lesion in the right adrenal gland lateral edge.
Laparoscopic right adrenalectomy was planned for histopathologic examination (Figure 2).
The patient was placed on the operating table in the left lateral decubitus position with the right arm in the reverse Trendelenburg position with a 45°–60° angle in the right lateral thoracotomy position. To increase the distance between the lower rib and the iliac crest, the operating table was laterally brought to 30° flexion. The surgery was performed using four ports including one for the liver retraction. After the liver was mobilized and retracted, the vena cava was placed in the middle and the adrenal gland was dissected. The right adrenal gland was removed by connecting with Hem-o-lok clips. The gland was removed using an EndoBag and was sent to the pathology department.
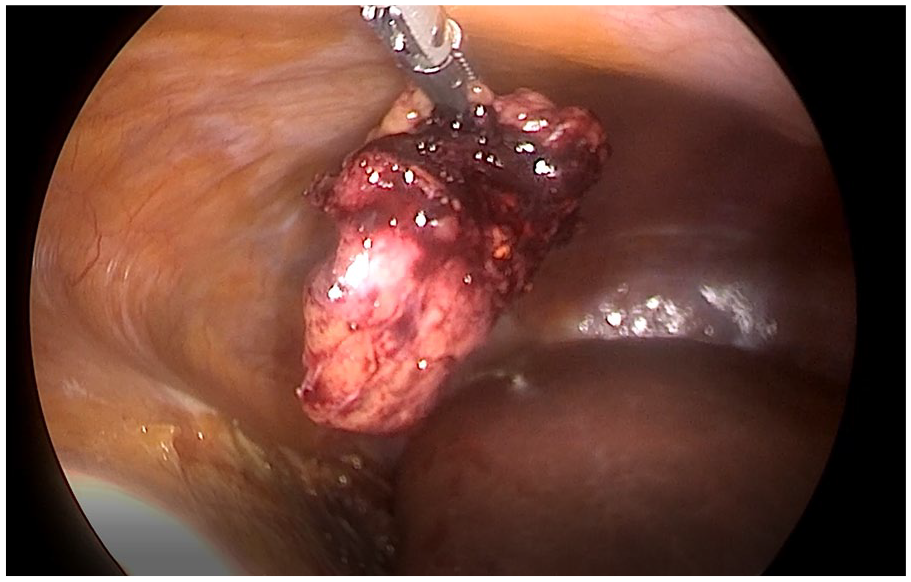
Laparoscopic right adrenalectomy for histopathologic examination.
In the histopathologic analysis of the sample, ganglion cells showing clustering in the focal area of the benign adrenal gland parenchyma in fibrous stroma and tumoral development characterized by intermittent fusiform cells were observed. The tumor was interpreted as ganglioneuroma. Postoperatively, the patient started to receive a liquid diet on the same day and a semisolid diet on the first postoperative day. Recovery was uneventful and the patient was discharged on the second postoperative day.
Discussion
Ganglioneuroma is a rare, benign, differentiated neurogenic tumor that emerges in neural crest cells. 5 Ganglioneuromas are most frequently seen in the posterior mediastinum and retroperitoneum. AGN is mainly seen in children and young adults. It has a benign histology and biologic behavior without hormone secretion. AGNs are generally asymptomatic and discovered incidentally during routine follow-ups. In most cases, AGNs are asymptomatic due to the nonfunctioning nature of the tumor.6,7 Sometimes, they can secrete catecholamine. 8 Some studies have revealed that ganglioneuromas are not related to endocrine hormonal activity9,10; however, they are expected to exist as a composite tumor with pheochromocytoma. 11
AGNs characteristically appear as well-defined masses having fibrous shapes in CT scans. They show hypodense characteristics in the precontrast phase with an increase in the postcontrast phase. A homogeneous appearance in the precontrast phase and heterogeneous appearance in the postcontrast phase are other characteristics of neurogenic tumors. 6 The presence of spot calcifications with no vascular involvement and the low-density contrast involvement in CT should cause the physician to suspect ganglioneuroma as a possible diagnosis. 10 Adrenal adenomas have a similar homogenous morphology to AGN; however, they are generally small, showing involvement with more than 50% contrast in images taken after contrast is given. 12 Macroscopically, ganglioneuromas are solid masses that are encapsulated by a homogeneous grayish surface. Microscopic features consist of mature ganglion cells that are mixed with fusiform cell clusters (positive for S-100 protein).6,9,11 Wide excisions are not necessary because AGNs rarely metastasize or recur. Postoperatively, no adjuvant therapy is required for patients with AGNs and their prognoses are excellent. 4
Conclusion
AGN is a rarely seen, hormonally inactive, benign tumor. Final diagnosis can only be made with a histopathologic examination. Adrenalectomy is the standard treatment preferred for ganglioneuromas. Knowing the clinical appearance and good pathologic specialization are important adjunct matters in diagnosis. Laparoscopic adrenalectomy has become the gold standard in most patients with adrenal tumors. The final approach selection for laparoscopic adrenalectomy depends on the specialty of the surgeon.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.