
Abstract
Introduction:
Approximately 25%–30% of patients with non-small cell lung cancer (NSCLC) develop central nervous system (CNS) metastases during the course of the disease; this percentage is higher in patients with epidermal growth factor receptor (EGFR) mutations. Leptomeningeal metastases, infrequent in the advanced setting, have a particularly dismal prognosis. Osimertinib, a third-generation EGFR inhibitor, can provide effective and durable response in this setting.
Case Description:
We present a 62-year-old man with progressive vomiting, headache, short-term memory impairment, and left lower limb hyposthenia. Computed tomography (CT) showed bilateral lung nodules, multiple lymphadenopathies, liver and bone metastases, and CNS and leptomeningeal dissemination, including multiple parenchymal nodules located at supra- and infratentorial brain. Bone needle biopsy documented TTF1+ lung adenocarcinoma. Whole brain radiotherapy (WBRT) and symptomatic treatments were started. Next-generation sequencing reported deletion of exon 19 of EGFR and mutation 8 of TP53. Osimertinib 80 mg was promptly started and WBRT interrupted. Some days after the patient experienced repetitive seizures and neurologic worsening, antiepileptic drugs and dexamethasone were implemented, with gradual improvement. Radiologic evaluation, including brain MRI and thorax–abdominal CT, showed partial response on CNS as well as extracranial sites, which was sustained.
Conclusions:
First-line treatment with osimertinib can be safe and effective in EGFR-mutated NSCLC even in presence of multiple negative predictive factors (poor Performance Status, diffuse leptomeningeal involvement, TP53 comutation), suggesting that deferring local treatments can be feasible in this setting, allowing the patient to maintain a good quality of life.
Introduction
Approximately 5%–10% of patients with non-small cell lung cancer (NSCLC) present with central nervous system (CNS) metastases at diagnosis and 25%–30% will develop metastases during the course of disease. This percentage is even higher in patients with epidermal growth factor receptor (EGFR) mutations; it is unknown whether this higher incidence is due to the longer survival time in these patients (with consequent more time to develop brain metastases) or due to an intrinsic biologic mechanism of these tumors. 1
Osimertinib is an oral third-generation tyrosine kinase inhibitor (TKI)/EGFR inhibitor that selectively binds EGFR when it holds sensitizing or T790M-resistance mutations. Osimertinib represents a standard of care for patients with EGFR-mutated NSCLC in second-line after developing resistance mutation and in the first-line metastatic setting and it will likely be available for the adjuvant setting soon. Intracranial activity of this drug has been demonstrated in preclinical works and in the phase III FLAURA trial.2,3 Data on its activity on leptomeningeal disease are lacking because these patients are generally not included in the largest clinical trial and because when leptomeningeal disease becomes symptomatic the very rapid evolution leads to clinical deterioration that does not allow any therapy except for palliation. 4
Finding the best way to treat patients with CNS metastases or leptomeningeal metastases, sparing toxicities from local treatments, is crucial considering the poor life expectancy of these patients, with a median survival of only 3–4 months. 5
We describe the case of a 62-year-old man presenting with symptomatic CNS and leptomeningeal metastases from NSCLC with EGFR and TP53 comutation who obtained intra- and extracranial benefit from osimertinib without receiving whole brain radiotherapy (WBRT).
Case report
A 62-year-old former smoker reported progressive nausea associated with episodes of vomiting and headache in August 2020. Based on the symptoms worsening, along with short-term memory impairment and left lower limb hyposthenia in September 2020, he underwent thoraco-abdominal computed tomography (CT) that showed different nodules in the left lower lobe of the lung, hepatic parenchymal lesions, multiple diffuse osteolytic lesions, and thoracic lymphadenopathies.
Radiologic assessment continued with brain magnetic resonance imaging (MRI), which documented multiple nodular areas of pathologic enhancement at the cortical–subcortical junction of both cerebral hemispheres, in the right pontine region and the left midbrain, compatible with disease spread. Leptomeningeal thickening was observed along the profile of the pons and bulb (Figure [A]). A spinal MRI showed no signs of spinal CNS metastases.
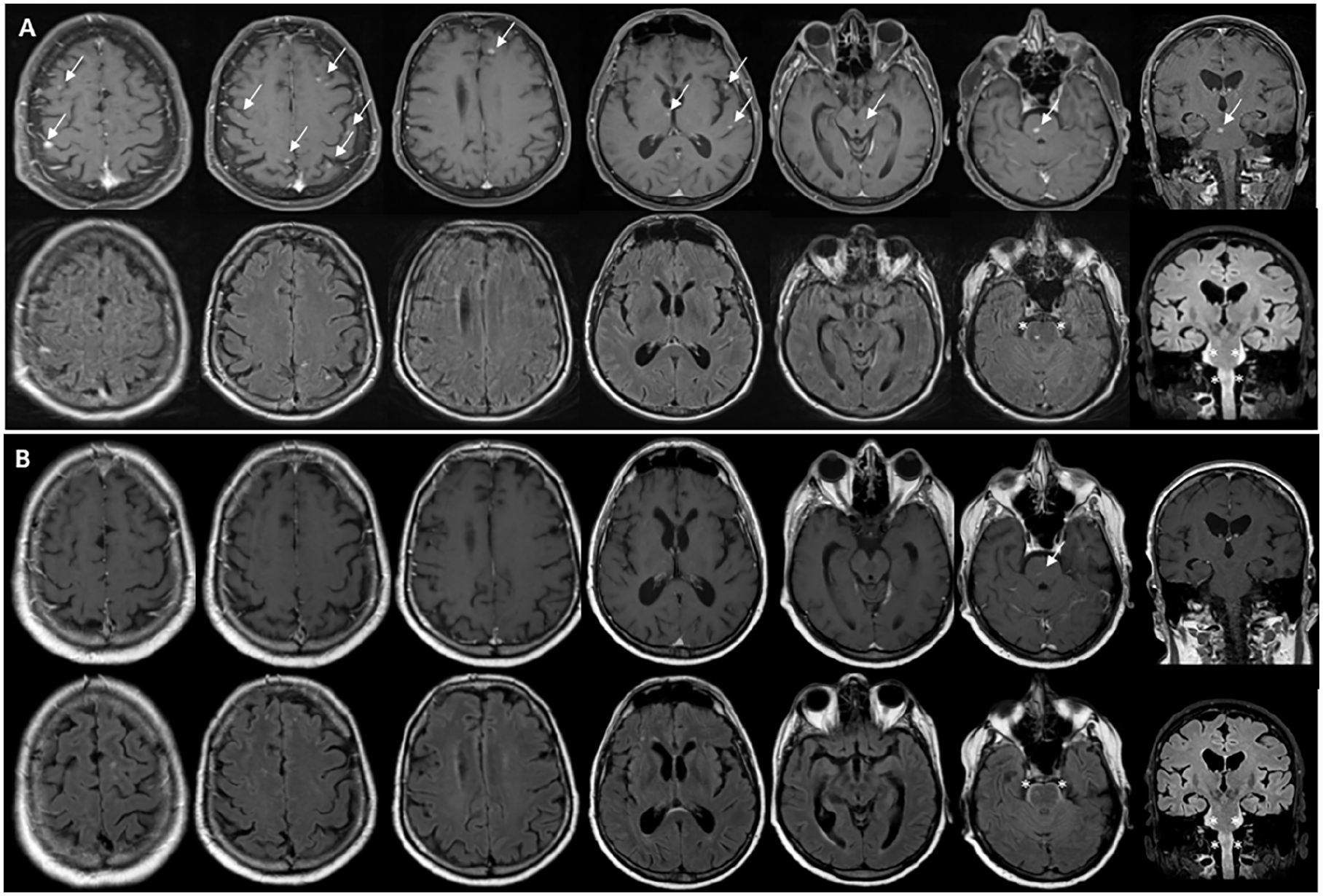
Brain magnetic resonance imaging with contrast enhancement. (A) (Top, T1-weighted images with contrast enhancement; bottom, fluid-attenuated inversion recovery [FLAIR] sequence): in November 2020 (before osimertinib), multiple small contrast-enhancing nodular parenchymal lesions (arrows) at the cortico–subcortical junction of both cerebral hemispheres were seen, in the right pontine region and the left midbrain, compatible with disease spread, and leptomeningeal thickening (asterisks) without contrast enhancement was observed along the profile of the pons and bulb (bottom right in axial and coronal images). (B) (Top, T1-weighted images with contrast enhancement; bottom, FLAIR sequence): in March 2021 (4 months after starting osimertinib treatment), pathologic contrast enhancement remitted, except for the pontine enhancement, which was reduced (top), without changes in FLAIR alterations along the brainstem (bottom); no new lesions were detected.
Percutaneous CT-guided bone needle biopsy of the focal lytic alteration of the right iliac bone was performed and the diagnosis was lung adenocarcinoma TTF1+. All molecular alterations on the tissue sample were requested as for standard of care including EGFR and BRAF mutations using DNA next-generation sequencing (NGS) (IonTorrent panel on 50 genes), ALK and ROS1 rearrangement using an RNA NGS (Archer panel on 14 genes), and PD-L1 expression on immunochemistry. Due to the smoking history (more than 40 years ago), a liquid biopsy for EGFR was performed, showing exon 19 deletion of EGFR gene.
Palliative radiotherapy was performed on dorsal and lumbosacral spine and left proximal femur (DT 8 Gy/1 Fr, 3 DCRT, ELK).
Because of the neurologic symptoms, while awaiting molecular results, symptomatic treatment and palliative WBRT were initiated and 10 fractions with 2 Gy were planned. However, on the same day, the results of liquid biopsy were available, demonstrating the deletion of exon 19 of the EGFR gene. Therefore, the case was collegially rediscussed and the therapeutic plan changed: osimertinib 80 mg once daily was started and the WBRT was suspended (based on the potential encephalic activity of such first-line treatment). Analyses on tumor tissue confirmed these findings, including the presence of TP53 comutation (mutation at the level of exon 19 of the EGFR gene in 51% of the DNA analyzed and mutation at the level of exon 8 of the TP53 gene in 51%), excluding fusion alterations and PD-L1 expression.
In November 2020, the patient experienced repetitive tonic seizures and was admitted to the neurologic hospital unit, where he was treated with antiepileptic drugs and intravenous dexamethasone. The seizures were controlled within a few hours; however, neurologic examination showed slowness, confusion, and gait instability (Karnofsky Performance Status [KPS] 60). The patient’s cognition and motor status gradually clinically improved, to the extent that he was able to be married during the hospitalization period. Within a few days, he was discharged on osimertinib 80 mg daily, antiepileptic (lacosamide) medication, and progressively tapered dexamethasone.
Forty days after baseline brain MRI and 4 months after the clinical onset, a new brain MRI showed a marked reduction in the already known multiple CNS lesions with enhancement at cortico–subcortical junction of both cerebral hemispheres; the remaining findings (including the peripontine alterations) were unchanged (Figure [B]). The neurologic examination documented further improvement (KPS 80); in addition, the patient experienced no other seizures and no more bone pain, allowing progressive tapering of symptomatic analgesics. The first follow-up thoraco-abdominal CT evaluation demonstrated a partial response in all the extracranial disease sites.
A new thoraco-abdominal CT was performed as per standard of care after 2 months and no signs of disease progression were shown, but a pulmonary embolism was detected. The patient had no respiratory symptoms. He was put on anticoagulant therapy and continued osimertinib.
Brian MRI performed in March 2021 showed remission of the enhancing brain nodules except for the pontine one, which was reduced; the nonenhancing alteration along the brainstem was stable.
Discussion
TKIs are routinely used in the treatment of oncogene-addicted NSCLCs. The third-generation EGFR inhibitor osimertinib changed the treatment of patients with CNS metastases, modifying the local treatment algorithm. CNS locoregional therapies, i.e. neurosurgery and radiotherapy, represented the most effective treatments for intracranial disease, principally due to the low capacity that most drugs offer to cross the blood–brain barrier. The small size of the molecule (molar mass 499 g × mol–1) allows osimertinib to penetrate into the CNS and express its activity on intracranial sites. This was demonstrated by CNS objective response rates (ORRs) of 54% and 70% in the AURA/AURA2 and AURA3 trial, respectively, and 66% in the recently published phase III trial FLAURA, with a CNS median duration of response (mDOR) in the latter study of 15.2 months.6,7
Leptomeningeal involvement is rare in metastatic NSCLC (3%–4% of patients with NSCLC, up to 9.4% in EGFR-mutated patients), for which treatment options are poor and few data exist on TKI activity. In an exploratory analysis on 22 patients treated with second-line osimertinib within AURA trials (after a previous first/second-generation TKI), leptomeningeal ORR was 55%; in the FLAURA trial, which randomized patients to receive osimertinib versus first-generation EGFR TKIs in first-line metastatic setting, 4 of 5 (80%) patients with leptomeningeal involvement treated with osimertinib 80 mg achieved a complete radiologic leptomeningeal response. The largest experience derives from the phase I BLOOM trial, in which 41 patients with de novo radiologically detected leptomeningeal metastases from EGFR-mutated NSCLC were enrolled to receive 160 mg of osimertinib (doubling the approved dose) in first-line setting or as second-line after T790M resistance mutation development. The study showed a leptomeningeal ORR of 62% with mDOR of 15.2 months. Median overall survival (mOS) was 11 months and the 12-month survival rate was 48%, far superior to historical cohorts of patients with NSCLC with leptomeningeal involvement treated with first-generation EGFR inhibitors (median survival of 88 days from Erlotinib start, median survival of 4.4 to 9.5 months from leptomeningeal metastases).8,9 However, in this cohort, half of the patients (49%) received previous first-generation TKIs, which is no longer standard of care, and almost half received previous radiotherapy, thus not allowing an evaluation of the effect of sparing brain radiotherapy on clinical outcomes. 10
The “double-dose” approach purposed in the BLOOM study was also evaluated in a recent phase II trial, comparing efficacy and safety of osimertinib 160 mg in lung adenocarcinoma with brain metastases and leptomeningeal metastases. Both cohorts consisted of 40 patients, with a more pronounced benefit observed in the leptomeningeal group compared to the historical cohort (median progression-free survival [mPFS] of 8.0 months, mOS of 13.3 months), suggesting that increasing the CSF drug concentration could counterbalance the refractoriness of the leptomeningeal localization and reverse the dismal prognosis associated with this clinical setting. However, all patients received previous TKIs (which is no longer the standard of care) and 12.5% and 20.0%, respectively, in the brain metastases and leptomeningeal group, previously received standard dose osimertinib. Moreover, 47% and 65% of patients were treated with radiotherapy (stereotactic body radiation therapy or WBRT), not permitting evaluation of the opportunity to avoid local treatments in this setting. The safety profile was consistent with previous reports without significant adverse events, and only 7 of 80 patients required dose adjustment. 11
Supplementary Table 1 shows other case reports on leptomeningeal responses to osimertinib. Impressive ongoing response in terms of duration has been reported. Combinations with antivascular drugs (i.e. bevacizumab) and radiation therapy were also reported. Of note, osimertinib activity on leptomeningeal metastases after first-generation TKIs is documented even in absence of resistance mutation (i.e. exon 20 T790M).
Other factors are reported to affect the response to the latest TKIs. In a recent metaanalysis, TP53 comutation in EGFR-mutated patients with NSCLC was reported in 43.7% of cases, with a negative impact on mPFS and mOS (hazard ratio of 1.76 and 1.83, respectively). 12 In addition, patients with comutations showed increased risk of developing CNS metastases during the course of the disease compared with EGFR alteration alone (34.5% vs 6.9%). Different classifications of TP53 alterations have been proposed (disruptive vs nondisruptive; exon 8 vs non–exon 8 mutations), but none of these demonstrated a better accuracy to detect EGFR-TKI primary resistance. To our knowledge, no case of intracranial response in EGFR–TP53 comutated patients has been reported.
Conclusions
Our case demonstrated that first-line treatment with osimertinib can be safe and effective in EGFR-mutated patients with NSCLC even in presence of multiple negative predictive factors (poor Performance Status, diffuse CNS involvement with leptomeningeal disease, and TP53 comutation). Osimertinib is an efficient alternative to WBRT, which remains a palliative treatment, to perhaps consider as second-line, and permits the patient to maintain a good quality of life.
Supplemental Material
sj-pdf-1-tmj-10.1177_03008916211052330 – Supplemental material for Carcinomatosis under control by osimertinib in EGFR and TP53 mutated lung adenocarcinoma
Supplemental material, sj-pdf-1-tmj-10.1177_03008916211052330 for Carcinomatosis under control by osimertinib in EGFR and TP53 mutated lung adenocarcinoma by Leonardo Provenzano, Valeria Cuccarini, Marco Platania, Luca Canziani, Andrea Spagnoletti, Fabio M. Doniselli, Marica Eoli, Arsela Prelaj and Elena Anghileri in Tumori Journal
Footnotes
Acknowledgements
The authors thank the patient and his health care team.
Declaration of conflicting interest
A.P. declares personal fees from Roche, AstraZeneca, and BMS outside the submitted work. The other authors report no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.