
Abstract
Background:
Despite ongoing developments, pancreatic cancer remains one of the most difficult tumors to treat. Even the most effective chemotherapy regimens, only marginally improve the outcome of Pancreatic cancer patients, which rarely exceeds one year. A small subset of Pancreatic cancer patients, carriers of germline variants of BRCA1/2, are clinically relevant as therapeutic targets in pancreatic cancer, both for the first-line and maintenance therapy, as they are more responsive to platinum-based chemotherapy agents and PARP inhibitors. Though, a little is known about the efficacy of olaparib monotherapy in later lines, or in poor responders to platinum-based regimens.
Methods:
We describe a case of a patient with pancreatic cancer harboring BRCA2 mutation, treated with radical surgery, adjuvant treatment and three different palliative chemotherapy regimens at disease recurrence (FOLFOX in first line with progression-free survival of five months, gemcitabine and nab-paclitaxel in the second line with progression-free survival of six months and FOLFIRI in the third line with progression-free survival of three months) before olaparib off-label treatment.
Results:
Interestingly, the patient remained 10 months on olaparib treatment, without disease progression, and without any side effects from the treatment.
Conclusion:
In conclusion, this case highlights the clinically relevant progression-free survival with olaparib treatment in later line and the potential of better health-related quality of life in this small subset of Pancreatic cancer patients.
Keywords
Introduction
Germline variants in cancer susceptibility genes, in particular BRCA1/2, are clinically relevant targets in metastatic pancreatic ductal adenocarcinoma (PDAC), both for the first-line and maintenance therapy. The patients harboring BRCA1/2 mutations are more responsive to platinum-based chemotherapy agents and poly (ADP-ribose) polymerase (PARP) inhibitors,1,2 adding a new therapeutic chance for this small subset of PDAC population. Generally, sensitivity to platinum-based chemotherapy is expected to predict the sensitivity to PARP inhibitors, although platinum chemotherapy elicits cell death through both homologous recombination (HR) dependent and non-HR-dependent mechanisms, thus reducing predictive power. 3 Golan et al. 4 conducted a retrospective study of 71 PDAC patients with BRCA 1/2 mutations showed that those treated with platinum agents achieved significantly longer overall survival (OS) than those treated with non-platinum agents (22 vs 9 months, p=0.039). Therefore, platinum-based first-line chemotherapy is the preferred regimen in PDAC patients with BRCA1/2 germline variants. The phase III trial of Golan et colleagues 4 showed a better progression-free survival (PFS) in PDAC patients with germline BRCA1/2 mutations receiving olaparib as maintenance after no disease progression for at least four months of platinum-based first-line chemotherapy. Though, little is known about the efficacy of olaparib monotherapy in later lines, or in poor responders to platinum-based regimens.
Case description
A 49-year-old female patient had been diagnosed in 2003 with a luminal B locally advanced breast cancer. She was treated with radical surgery and adjuvant radiotherapy, chemotherapy and hormonal therapy. She was regularly follow-up for breast cancer with no recurrence.
In November 2018, at the age of 64 years, she was admitted to hospital for back pain and nausea. A CT scan revealed a mass of 21x17 mm at head of pancreas with no blood vessel infiltration and no distant metastases. The value of tumor marker CA 19-9 was increased (126.78 IU/mL). The patient had been judged resectable upfront by a multidisciplinary team and underwent pancreaticoduodenectomy in November 2018. The histological examination confirmed the presence of poorly differentiated pancreatic adenocarcinoma, pT2pN0 stage II per TNM staging 8th edition. 5 After surgery, in January 2019, she started gemcitabine in monotherapy for six months, concluding in June 2019, with no evidence of recurrence at the CT scan in June 2019. Nevertheless, in January 2020, elevation of tumor marker CA 19-9 (1197 IU/mL) was detected and CT scan showed disease recurrence, with liver and peritoneal metastases. Before starting the first-line chemotherapy, a BRCA test documented a germline mutation of BRCA2 (C.8247_8248delGA p.Lys2750Aspfs*13). Moreover, KRAS mutational status and microsatellite status was also analyzed, confirming a mutation of KRAS (exone 2, c.35G>A, p.Gly12Asp) and microsatellite stable tumor (MSS).
In January 2020, the patient started first-line chemotherapy containing platinum (FOLFOX) reaching stable disease per RECIST 1.1 as best response after three months of treatment. After another two months of treatment, in August 2020, the CT scan documented liver progression. As progression disease after first-line platinum-based chemotherapy was documented, the maintenance with olaparib was not used. The patient received subsequent palliative chemotherapy lines (gemcitabine and nab-paclitaxel in the second line with PFS of six months and FOLFIRI in the third line with PFS of three months). After the competition of third-line chemotherapy, the patient was still in good clinical condition (ECOG PS 0). No phase III trial evidence is available for use of olaparib in monotherapy in later palliative setting, but, considering the presence of BRCA2 mutation and absence of therapeutic alternatives, we applied for olaparib off-label to the Ethics Committee (Comitato Etico dell’Area Vasta Emilia Nord). After approval, the patient started olaparib in June 2021. The therapy was very well tolerated with no side effects from the treatment. The duration of the response to olaparib was 10 months, with partial response as the best response obtained. Tumor markers levels dropped after olaparib treatment (baseline values: CEA 42 ng/mL, CA 19-9: 1935 IU/mL, at the best response: CEA 11 ng/mL, CA 19-9: 436 IU/ml). Unfortunately, a CT scan in May 2022 showed progression of both peritoneal and liver metastases (Figure 1 and 2). The patient underwent one more anticancer therapy line (clinical trial PCT-29 with chlorambucil). Subsequent therapy was not indicated for worsening general conditions and the patient continued with best supportive care. She died in June 2022 after 43 months from pancreatic cancer surgery and 29 months after metastatic disease diagnosis.
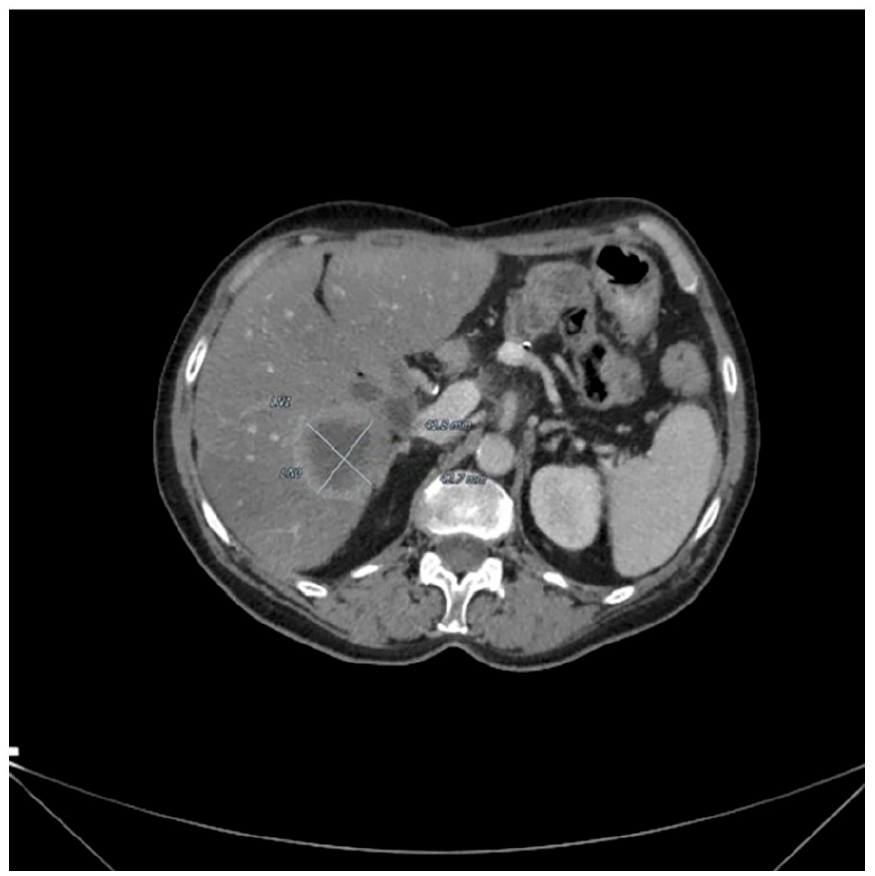
Baseline CT scan showing nodular target lesion in the 6th liver segment (42x43 mm).
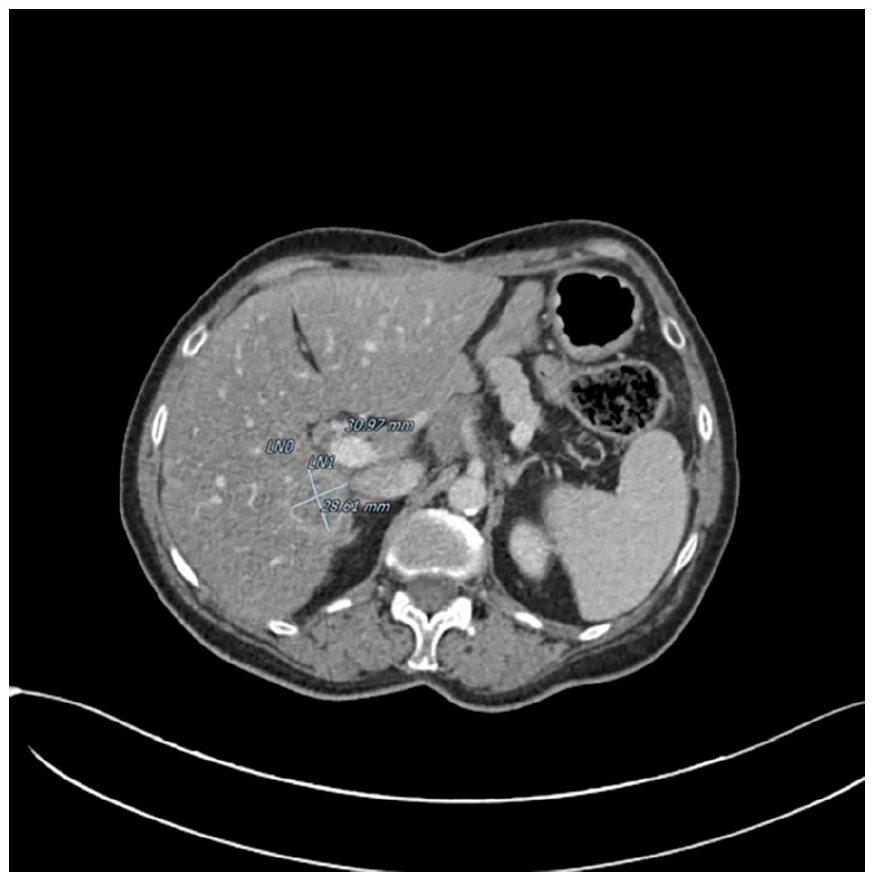
Reduction in size of the target hepatic lesion in the 6th segment (30 x 28 mm).
Conclusions
In this report, we describe the case of a female patient, carrier of BRCA2 mutation, affected by pancreatic cancer. The patient was treated with radical surgery and subsequent adjuvant chemotherapy and three different palliative chemotherapy regimens at disease recurrence (FOLFOX, gemcitabine and abraxane, FOLFIRI) before olaparib treatment. Interestingly, the patient remained on olaparib treatment for 10 months, without disease progression, and without side effects from the treatment. The PFS of 10 months obtained by the olaparib treatment was higher than any previous palliative chemotherapy in earlier line (FOLFOX in first line with PFS of five months, gemcitabine and nab-paclitaxel in the second line with PFS of six months and FOLFIRI in the third line with PFS of three months).
The phase III trial of Golan and colleagues 4 showed a statistically significant better PFS in patients affected by PDAC receiving olaparib as maintenance after no disease progression for at least four months of platinum-based first-line therapy. PFS reached 7.4 months in the treatment group vs. 3.8 months in the placebo group (p=0.004), though no advantage in OS was documented. 4 The investigators reported an update on the study outcomes in 2021 6 . The median OS was 19.2 months for olaparib group and 19.0 months for placebo group, but it was not statistically significant. Interestingly, three-year OS was 33.9% for olaparib group and 17.8% for placebo group. 6 Moreover, some other studies investigated the role of PARP inhibitors in PDAC. For example, the combination of veliparib with gemcitabine and cisplatin as first-line therapy was explored in a phase II trial of advanced PDAC patients with BRCA1, BRCA2, and PALB2 mutations. No statistically significant differences in terms of OS, PFS, or overall response rate (ORR) were seen between the two arms. 7 Another PARP inhibitor, rucaparib, showed a 37% response rate in PDAC patients with somatic or germline variants in BRCA1, BRCA2, or PALB2 genes. 8
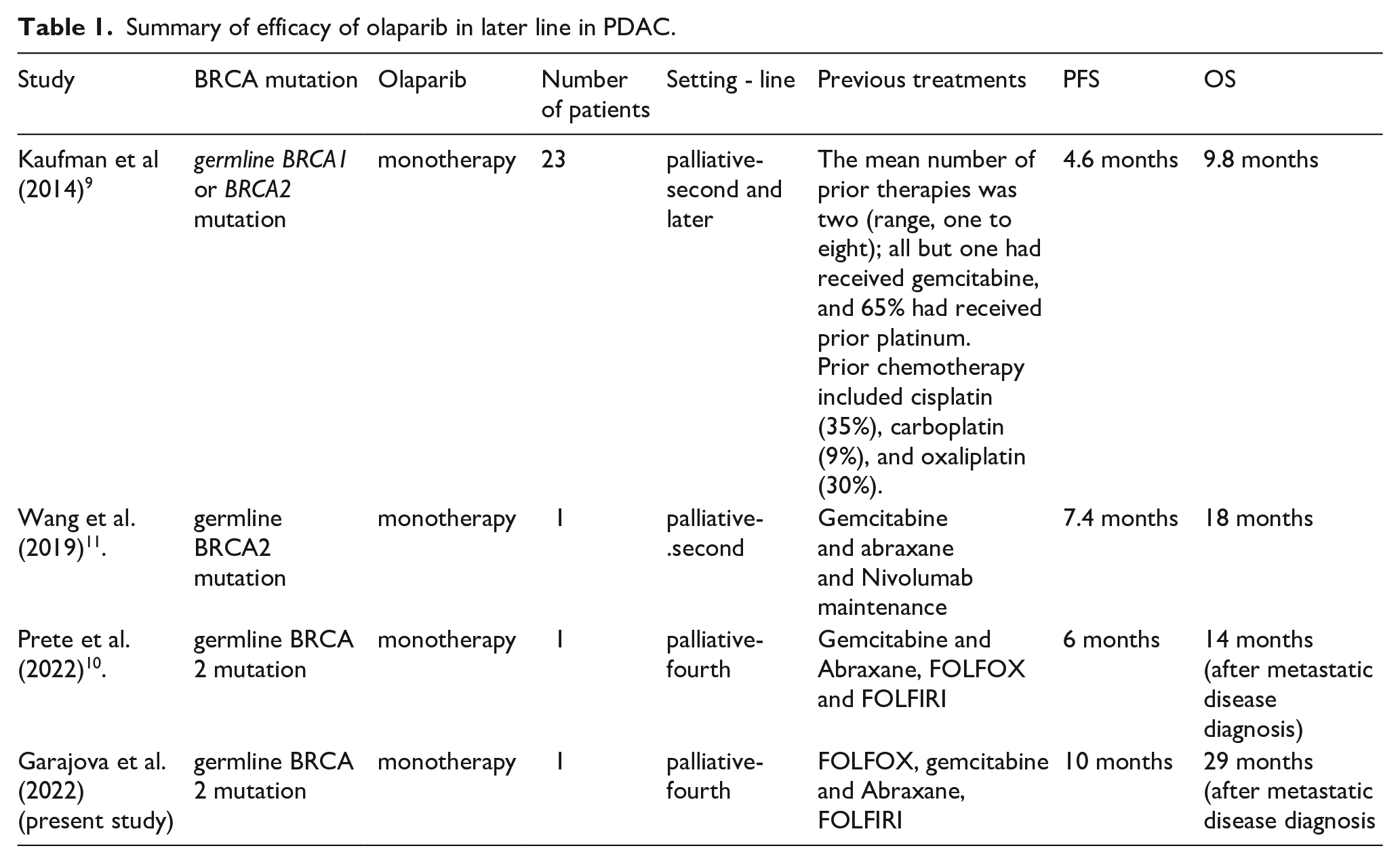
Though, little is known about the efficacy of olaparib monotherapy in later lines, or in poor responders to platinum-based regimens (Table 1). Kaufman et al. 9 conducted a phase II study with olaparib in monotherapy enrolling patients with a germline BRCA1/2 mutation and different cancer types, including PDAC patients pre-treated with gemcitabine. The tumor response rate was 21.7%. Further, 35% of PDAC patients showed stable disease after two months of treatment. Recently, Prete et al. 10 described a case report of a 61-year-old metastatic PDAC female patient harboring germline BRCA2 mutation. The patient received three previous chemotherapy palliative lines (gemcitabine and nab-paclitaxel in the first line, FOLFOX in the second line, FOLFIRI in the third line), before olaparib off-label treatment. The authors documented a partial response after two months of treatment. The radiologic and clinical response was maintained for six months. The authors highlighted the potential of olaparib as single agent after progression with standard treatment in BRCA-mutated PDAC. 10
Summary of efficacy of olaparib in later line in PDAC.
Even if evidence of PARP inhibitor efficacy in later lines in PDAC treatment are scarce, it seems that germline mutation of BRCA1/2 in cancer patients represents a target population for whom PARP inhibitors could be beneficial. Germline BRCA1/2 mutation carriers have shown prolonged tumor responses in different tumor types such as ovarian, breast and prostate cancers. 9 Limited data are available on the activity of olaparib in poor responders to platinum. Kaufman et al. 9 included 193 patients with platinum-resistant ovarian cancer in their study. Although, also in the platinum-resistant population, the tumor response rate after olaparib treatment was 31%, confirming its activity also in this population. It is likely that some mechanisms of resistance to platinum are similar to the mechanisms of resistance to PARP inhibitors, although, it seems that there is not always cross resistance. 9
In conclusion, we presented a case of clinically relevant PFS in pre-treated PDAC patients, carrier of BRCA2 mutation. Importantly, olaparib monotherapy was very well tolerated with any side effects and this case report underlines the potential of better health-related quality of life in this small subset of PDAC patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.