
Abstract
Introduction:
Experiences related to pediatric oncology diagnosis cause great imbalances within the family structure. Assessing the frailties and needs of families and children with cancer from a psychosocial perspective is an important step in providing appropriate pediatric psychology care.
Methods:
The aim of this study was to develop an Italian translation of the last version of the Psychosocial Assessment Tool questionnaire (PAT 3.1) and to pilot-test it among pediatric oncological families. The guidelines for cross-cultural adaptation of health-related quality of life measures were followed. Specifically, two independent forward translations were produced, followed by a reconciliation step by a multidisciplinary expert committee and back-translation. Revision of the original text and all translations were performed by the expert committee leading to a final version, which was pilot-tested by cognitive debriefing on five families. Subsequently, the final Italian PAT 3.1 version was approved.
Results:
The Italian version of the PAT 3.1 generated in the present study is a useful instrument to examine the psychosocial risk of the families with a child with cancer.
Conclusions:
This instrument will be a valuable tool for future clinical trials and it will help clinicians to target specific pediatric psychology support intervention. The questionnaire will be further validated through a multicenter Italian study on psychosocial screening of pediatric oncology and pediatric general diseases.
Introduction
Each year, an estimated 400,000 children and adolescents aged 0-19 years develop cancer. 1 Although the five-year survival rate for this disease has increased to 80% in children and adolescents, 2 6000 children and young people still die of cancer each year. Cancer, therefore, remains a leading cause of death from disease in Europe. At the time of diagnosis, the emotions associated with the fear that the child may die, the knowledge that he/she will have to undergo invasive procedures and long-term therapies, and the uncertainty about the course of treatment, all lead to serious imbalances in the emotional setup of the family as a whole. The coping strategies that a family chooses to adopt for these elements of extreme distress contribute to defining the conditions for their adaptation throughout care and survival. 3 Thus, the challenges of daily life, the psychological conditions of parents from the time of diagnosis, the burden of care, 4 and the difficulties of siblings 5 all have negative effects on family functioning.
The importance of psychosocial intervention not only on the children with cancer but on all the family members is well-documented in the literature, and therefore it appears essential to continue focusing on families and children by identifying their unique needs and resources. 6 Furthermore, the implementation of initial screening tools is desirable in this area in order to better coordinate future interventions. 7 Assessing, from a psychosocial perspective, the frailties, needs, and resources of families and children with cancer, is an important step in providing appropriate supportive care. From this perspective, it seems essential to be able to provide new tools to investigate the area of psychosocial risk. Following this train of thought, the Psychosocial Assessment Tool (PAT), a screening tool developed by Kazak et al. 8 and based on the principles of the Paediatric Psychosocial Preventive Health Model (PPPHM), 9 is well recognized in pediatric psychology research. The PPPHM applies the socio-ecological framework derived from Bronfenbrenner's ecological systems theory, 10 according to which the child is at the center of a series of concentric circles, representing increasing distal interacting systems that ultimately affect the child’s well-being (Figure 1).9,11
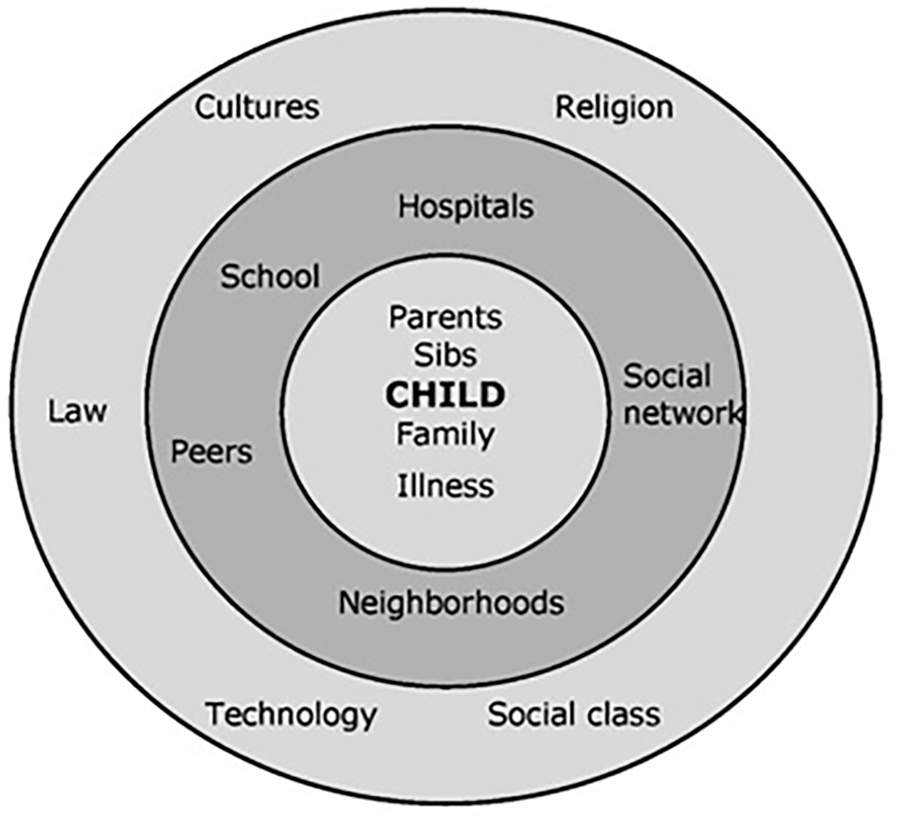
Socio-ecological model applied to children's health.
Therefore, the PPPHM allows the use of a screening model designed for all families of children entering the pediatric health care system and defines three levels of care.
The first level corresponds to Universal, the largest population, which identifies children and families who are in distress but can rely on adequate resources and coping strategies. Intervention with this population converges through general support, provision of necessary and useful information, and screening/monitoring for higher risk indicators throughout the care pathway.
The second level corresponds to Targeted, which identifies acute distress situations and the presence of risk factors. Finally, the Clinical level, the narrowest population, is characterized by persistent or worsening distress and high-risk factors (Figure 2). 9
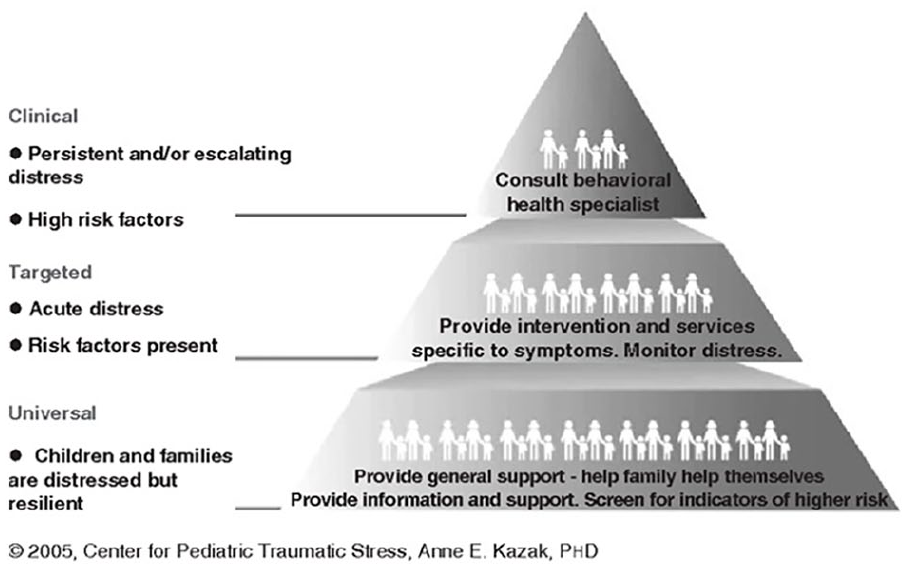
Level of care.
Serious illnesses or injuries in childhood, such as oncological diseases, can have harmful effects on the normal development of the child and the entire family system. 12
Therefore, a screening tool to help better target interventions to support children and their families is highly desirable for a team that aims not only to treat the disease, but also to care for the person and their family as a whole.
The work presented here describes the process of translating PAT 3.1 (Psychosocial Assessment Tool) into Italian following the best practice guidelines.
In addition to the description of the process of translation and cultural adaptation, pre-test data are presented to provide a useful reflection on the possibilities of this instrument. These data also represent preparatory work for validation on a suitable sample.
Methods
Materials
The PAT is a brief family psychosocial risk assessment questionnaire based on a socio-ecological model of families. This tool is intended to be a universal screening tool in pediatric health care. 8
The PAT, based on the PPPHM model, provides three main areas of risk: Universal, Targeted, and Clinical. Based on the level of risk identified, it is possible to structure an appropriate intervention for the family. Responses to the instrument items are classified dichotomously as indicative of risk. The PAT then generates a total score and seven subscale scores: Family Structure/Resources, Social Support, Child Problems, Siblings Problems, Family Problems, Family Beliefs, and Stress Reaction. The total score, which is the sum of the subscales, ranges from 0 to 7. The total score is then matched to the three risk levels of the PPPHM. 13
The instrument is easy to use in the pediatric setting, as the caregiver can complete it in 10 minutes or less. In response to the results of the PAT, it is important to conduct a more in-depth assessment to determine the most appropriate care arrangements. However, the PAT remains one element of a complex framework whose goal is to structure an appropriate intervention for the family. The translation, adaptation and pilot testing were provided by the Pediatric Psycho-oncology Unit of the Regina Margherita Children's Hospital of Turin Italy, one of the main pediatric referral centers of the northern Italy, in order to implement it in its clinical and research practice and make it available to the various Italian pediatric fields. Written informed consent was approved by the Ethics Committee of the hospital (Protocol Number: 0018330, 20/02/2018).
Process of translation, cultural adaptation and pilot testing
In order to proceed with the translation of the tool into Italian, we requested permission from the Reference Committee for PAT 3.1, which provides guidelines to follow. Once the necessary authorization was obtained, a working group dedicated to the project was set up and they proceeded with the translation and back-translation with the help of two bilingual translators who worked independently. During the translation process, efforts were made to ensure that the language used was scientifically correct but at the same time appropriate and understandable enough for caregivers of patients with different levels of schooling. In the course of translation, we adapted some items concerning the level of schooling, the patient's insurance coverage, and other specific Italian socio-cultural aspects.
After receiving approval with respect to back-translation, we convened a mini-panel of internal hospital professionals (physicians, psychologists, a nurse, and a social worker) and asked them to report to us any critical issues or misunderstandings found in PAT 3.1. Finally, we asked five monolingual caregivers of pediatric patients to respond to the translated version of the PAT 3.1, and conducted brief interviews in order to collect any misunderstandings or linguistic inconsistencies. For each step, we consistently updated the PAT 3.1 reference committee. The PAT 3.1, initially used only in pediatric oncology, has been adapted for use with other pediatric conditions, with published studies in cardiology, craniofacial disorders, cystic fibrosis, differences of sexual development, inflammatory bowel disease, medical complexity, organ transplantation, pain, sickle cell disease, hematopoietic stem cell transplantation, and weight management. 13 Our center therefore proposes use of this assessment tool in all departments of the children's hospital.
Results
Data from the pre-testing phase of PAT 3.1, part of the translation process, are presented below.
Since this was a pre-testing phase, the administration was preceded by a focus group aimed at gathering opinions, criticisms, and points of view with respect to the areas examined, how they are discussed, and any other concerns or doubts. The general opinion that emerged from the focus group was that the tool was able to appropriately investigate the psychosocial areas examined, the items were clear and comprehensible, and, in its entirety, PAT 3.1 was judged to be a valuable tool for gathering information. At a later point, PAT 3.1 was individually administered to the caregivers involved. Table 1 presents the demographic data of the examined sample.
Sample demographics (n = 5).
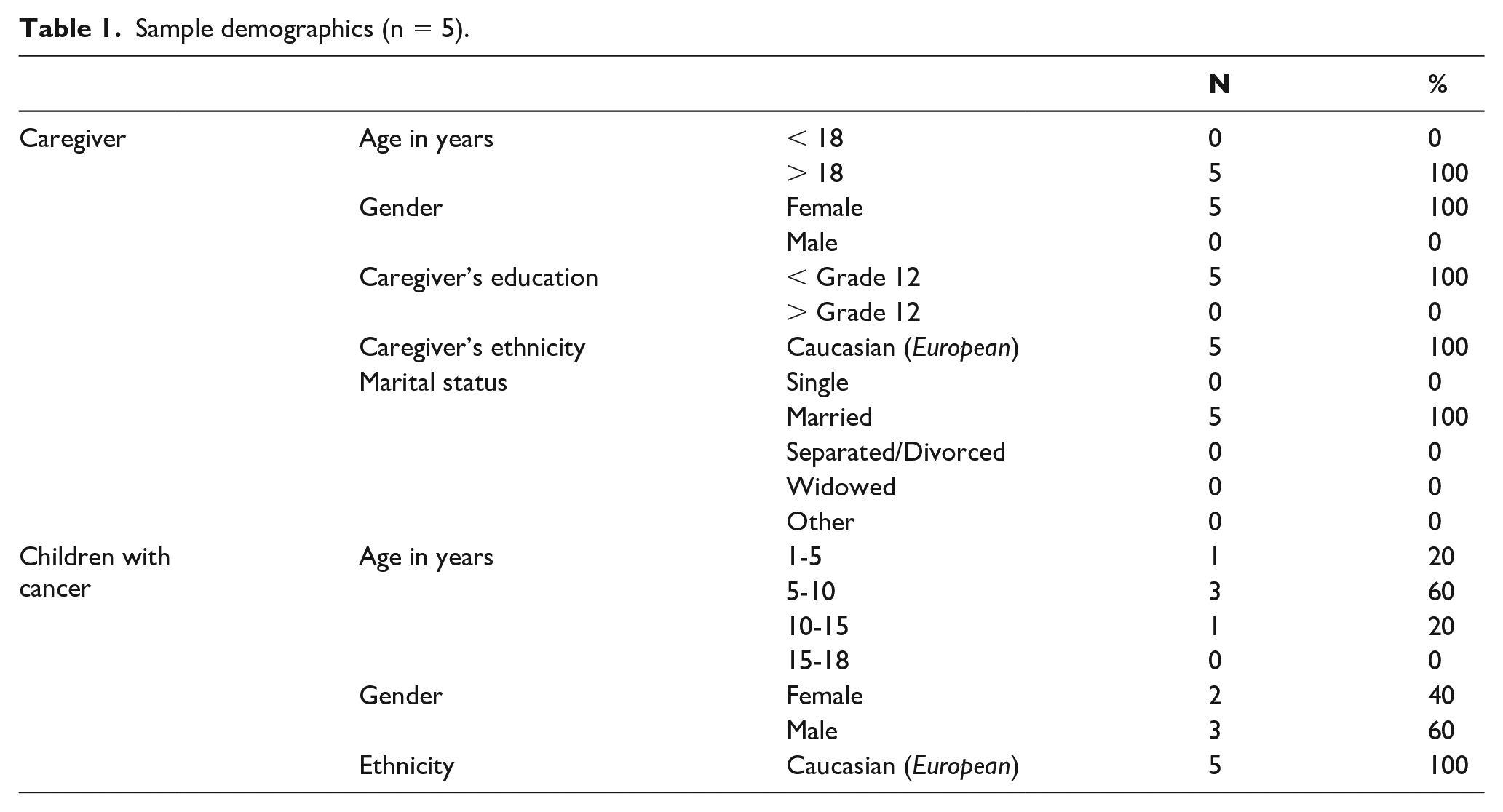
Five caregivers participated in the pre-test phase, all of whom were older than 18 years and had an education level above 12th grade (corresponding to the high school graduation in Italy). All five caregivers were of Caucasian-European ethnicity and were currently married. The demographic characteristics of the pediatric patients are also presented in Table 1. The sample consisted of five children: one child in the 1-5 age group (but over two years old), three children in the 5-10 age group, and one child in the 10-15 age group. Of the five children: two were female, three were male, and all were of Caucasian-European ethnicity. Only one subject reported the presence of siblings.
As Table 2 illustrates, the results present a picture in which the families do not seem to manifest fragility either in Family Structure/Resources or in Social Support. On the other hand, slight criticalities emerge in the areas of Child Problems, Stress Reactions, and Family Beliefs.
Pilot testing.
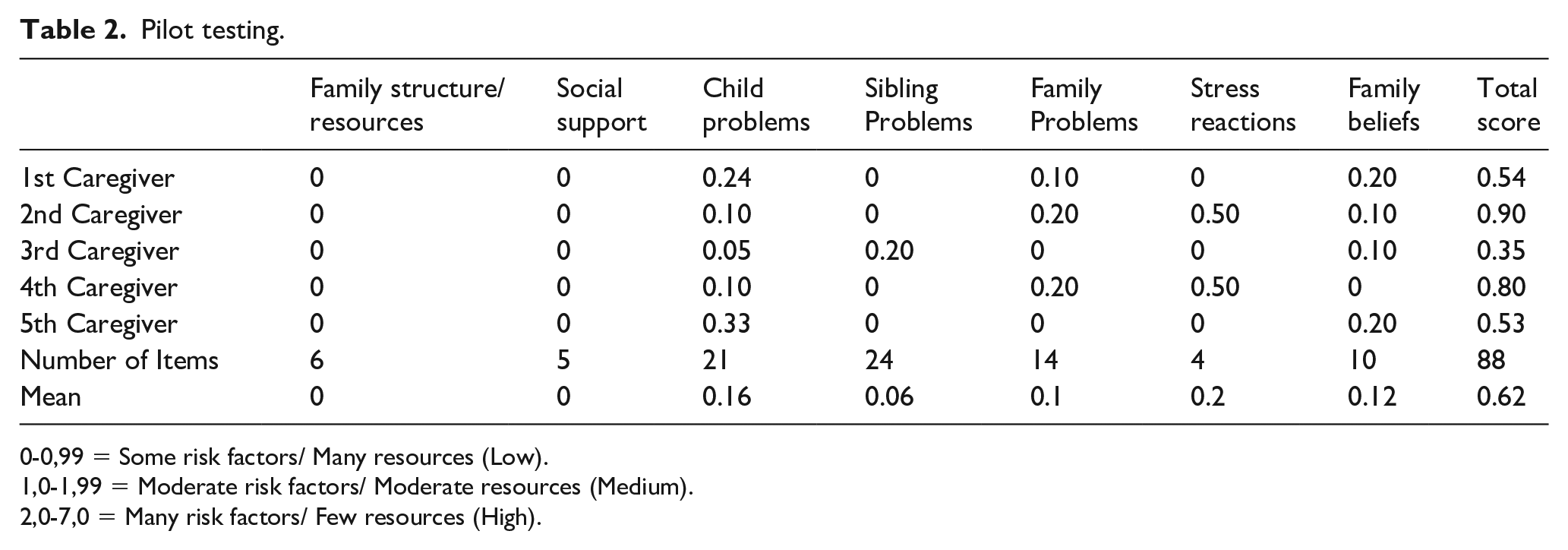
The only family with siblings in the sample reports a slight criticality in the subscale Sibling Problems.
The last line presents the total score, which allows the overall risk level (Universal, Targeted, Clinical) to be defined according to the PPPHM model integrated into PAT 3.1.
Comparing the values obtained with the normative ranges reported in the legend, it is possible to observe how all the subjects involved present low-risk criticalities and, according to the PPPHM model, fall within the Universal area. This, therefore, highlights the presence of distress in the family and child but, simultaneously, the existence of essential resources that promote resilience.
Finally, data are presented on the number of items for each subscale, the mean, the range, and the α obtained from the sample as a whole.
Discussion and conclusion
Screening the psychosocial needs of families is an important component of care not only in pediatric oncology but in the whole pediatric setting. For this reason, it is important to implement instruments capable of assessing the psychosocial needs of young people in care, in order to monitor how each family's needs and resources vary.
The PAT 3.1 translation process undertaken by our center started precisely with the aim of being able to better identify the frailties and resources of the various families in question, at an early stage.
In this assignment the pyramid structure of the PPPHM implemented in the PAT 3.1 allows for an essential subdivision of families into three different risk levels, permitting identification of the most appropriate clinical interventions for the specific psychosocial needs of families.
Thus, PAT 3.1 allows identification and differentiation of the specific level of risk manifested by the patient, caregiver, and siblings; such categorization, in a heterogeneous and broad context such as pediatric oncology, is critical in activating the most appropriate care possible.
In the analyses conducted, all patients fell within the Universal range, which does not require specific clinical interventions as families reveal significant resources, proving competent, and adaptive to the stressors of the disease. At this stage of the spectrum, the interventions to be activated range from psycho-education to psychological support and monitoring of more serious risk factors that may develop. Although the sample in this translation phase was small, from the comments of the clinicians in charge of the participating subjects, PAT 3.1 seems to prove itself as a tool capable of providing a valid insight into the level of psychosocial distress in pediatric patients and caregivers. The main limitations of this paper are due to its nature as a work related to the translation phase of the original version of PAT 3.1 and to the narrowness of the sample examined, which does not allow for statistically significant inferences. Obviously, this phase of work is limited by an approach more focused on preliminary work, which needs to be considered in a preparatory perspective to what could be a validation study of the tool using an Italian sample.
PAT 3.1 is a tool that is widely used abroad, and one which can contribute to creating a standard for assessment in the psychosocial field so as to allow for studies and clinical comparisons with other countries. Psychosocial screening through PAT 3.1 represents a significant possibility of implementation in clinical work in pediatric age. This leads to supporting the validation project of the translated tool in order to obtain data that support clinical intervention in pediatric oncology and other pediatric core health settings.
Footnotes
Acknowledgements
The authors would like to acknowledge UGI OdV, ADISCO Sezione Piemonte and Fondazione Maria Teresa Lavazza, who helped make this initiative possible.
Author contributions
CB: wrote the first draft; MG: wrote the first draft; PQ: contributed additional edits to the text and comments; NB: contributed additional edits to the text and comments; GZ: contributed additional edits to the text and comments; FF: contributed additional edits to the text and comments.
Data availability statement
The raw data supporting the conclusions of this article are fully presented in the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.