
Abstract
Purpose:
To compare the safety and efficacy of hepatic arterial infusion chemotherapy followed by transarterial embolization (HAIC+TAE) to transarterial chemoembolization (TACE) for the treatment of unresectable hepatocellular carcinoma (uHCC).
Materials and methods:
The clinical data of patients who received HAIC+TAE or TACE between April 2020 and April 2022 was collected. Propensity score-matching was used to balance the baseline characteristics of the two groups. Tumor response according to mRECIST, median time to progression (TTP) and overall survival (OS) were investigated. ALBI score was applied to evaluate the changes of liver function and other relative adverse reactions were recorded.
Results:
A total of 98 patients with uHCC were enrolled in the study, including 71 in the TACE group and 27 in the HAIC+TAE group. After propensity score matching, 23 pairs of patients were investigated. The HAIC+TAE group showed a longer median TTP and OS than TACE group (mTTP 316 vs. 235 days, P=0.023; mOS 580 vs. 493 days, P=0.020). Objective response rates in HAIC+TAE group and TACE group were 65.2% and 47.8% (P=0.234). Disease-control rates were 87.0% and 82.6% (P=1.000). No significant difference was found in the incidence of adverse events between the two groups (P>0.05).
Conclusion:
The combination treatment strategy of HAIC+TAE in patients with uHCC appears to be a safe regimen, with the potential to prolong mTTP and mOS relative to TACE. The sequential application of this therapy merits consideration as an innovative treatment strategy for individuals with uHCC.
Keywords
Introduction
Hepatocellular carcinoma (HCC) remains a global problem and poses a serious threat to human health. 1 Due to the fact that most patients cannot accept radical treatment at diagnosis, the one-year survival rate of HCC patients is less than 50%. 2 Intra-arterial therapy is one of the main modalities for the treatment of unresectable HCC (uHCC), including transarterial chemoembolization (TACE), hepatic arterial infusion chemotherapy (HAIC), and transarterial radioembolization (TARE). 3 HAIC avoids the first-pass effect and increases the intra-tumoral drug concentration by delivering chemotherapy drugs directly into the tumor-supplying arteries. 4 FOHAIC-1 clinical trial 5 revealed that HAIC-FO (hepatic arterial infusion of fluorouracil, leucovorin and oxaliplatin) yielded a better median overall survival (OS) in patients with advanced-stage HCCs than sorafenib. This suggests that HAIC may be an alternative treatment option for partial patients with advanced-stage HCCs.
Recently, it has been found that transarterial embolization (TAE) followed by HAIC can prolong the progression-free survival of patients with uHCC. 6 However, chemotherapy drugs can hardly enter the blocked blood vessels after embolization, which may reduce the killing effect on the tumor. If HAIC is performed first, the chemotherapeutic agents can be fully applied to the tumor cells, and then TAE is performed to block the tumor supply artery. Theoretically, this may improve the treatment effect. On this basis, we established a propensity score-matching (PSM) study to investigate the safety and efficacy of HAIC followed by TAE for uHCC.
Methods
Patients
This retrospective study was approved by the Ethics Review Committee of our center. The clinical data of patients with uHCC treated with TACE or HAIC+TAE between April 2020 and April 2022 was reviewed. HCC was diagnosed in accordance with the American Association for the Study of Liver Diseases (AASLD) practice guidelines. 7 Those patients with Child-Pugh Class A or B liver function and a performance status of 0 or 1 were enrolled. The exclusion criteria were as follows: No measurable lesion on CT/MR images; previous local or systemic treatment; extrahepatic metastasis or concomitant malignancies other than HCC; lost to follow-up; and renal insufficiency. The requirement for informed consent was waived due to the retrospective nature of the study.
Procedures
All procedures were performed under local anesthesia by board-certified interventional radiologists with over five years’ experience. The patients underwent conventional TACE via the femoral artery. A 4-F catheter was inserted into the celiac and superior mesenteric artery, and then angiography was performed to find the tumor-supplying arteries. For patients with portal vein tumor thrombus, the hemodynamic of portal vein was evaluated during the portal phase of superior mesenteric arteriography. A 2.7-F coaxial microcatheter was selected and inserted into proper hepatic artery through the outer catheter. Chemotherapy drugs including doxorubicin (30-50mg) and oxaliplatin (100-200mg) were slowly injected into the hepatic artery (infusion time ⩾20min). After that, the tumor-supplying arteries were selected by the microcatheter and embolized using the emulsion of 10mg doxorubicin and 10-20ml lipiodol (Guerbet, Villepinte, France). In addition, gelatin sponge particles (Alicon, Hangzhou, China) were used for some large tumors.
For patients who were treated with HAIC+TAE, the procedures were performed via femoral artery or radial artery. HAIC was performed first in these cases. A microcatheter was used to skip the gastroduodenal artery and was inserted into the proper hepatic artery. Then the microcatheter was sealed with heparin dilution liquid and fixed in the groin. After patients returned to the ward, an automatic infusion pump was used to administer arterial infusion chemotherapy. The drug regimen applied was modified FOLFOX including oxaliplatin (85 mg/m² infusion for 2 hours), leucovorin (400 mg/m² infusion for 1 hour) and fluorouracil (400 mg/m² bolus injection for 15 minutes, 2400 mg/m² infusion for 46 hours). After that, TAE was performed to block the tumor supply artery by injecting iodized oil. Gelatin sponge particles were added if necessary.
All patients were administrated with liver-protecting drugs postoperatively. Patients were examined by enhanced MRI or CT 6-8 weeks after treatment. Procedure was repeated if there were residual lesions observed on follow-up imaging studies. However, the procedure would be discontinued when severe liver damage or unacceptable toxicity occurred. Systemic therapy was allowed for advanced HCCs and recommended for intermediate-stage HCC patients whose disease was still progressing after two courses of treatment.
Observed clinical date
Baseline laboratory indexes were obtained within one week before treatment. These laboratory data include alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum bilirubin (BIL), albumin, blood cell count. These laboratory examinations were performed one week after treatment and repeated every three months. Moreover, baseline and postprocedural ALBI grades were calculated according to the laboratory values. In addition, any development of fever, emesis, abdominal pain, diarrhea and debilitation was recorded. The safety and toxicity were evaluated by comparing the change of laboratory values, change of ALBI grades, and the incidence of other adverse events described above. Adverse events were graded based on the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE, Version 5.0).
Contrast enhanced MRI or CT examinations were performed every 6-8 weeks to evaluate the therapeutic effect according to the mRECIST criteria. Objective response rate (ORR) and disease-control rate (DCR) were calculated. ORR was defined as the percentage of patients with complete response (CR) and partial response (PR) which was maintained for at least four weeks. DCR was evaluated by ORR plus stable disease (SD). Overall survival (OS) was the duration from the commencement of treatment until death or the last follow-up. Time to progression (TTP) was defined as the time from the first treatment course to progression of disease. The rates of survival and disease progression at one year were also recorded. Collection of follow-up data was terminated on 31 May 2023.
Statistical analysis
Statistical analyses were performed by SPSS 26.0 software. Considering the differences in the baseline characteristics between the two cohorts. The PSM method was applied to remove the covariate imbalance. The variables used for matching included age, gender, hepatitis history, alpha fetal protein (AFP), tumor size, Child-Pugh class, ALBI grade and BCLC stage. The two groups were matched 1:1 according to the treatment regimen, with a caliper width equal to 0.2. A t-test was used to compare continuous variables, and a chi-square or Fisher exact test was used to compare categorical variables. TTP and OS were calculated using Kaplan-Meier analysis, and significance was evaluated with a log-rank test. P<0.05 was considered statistically significant.
Results
Patient characteristics
A total of 98 patients who met the inclusion and exclusion criteria were enrolled in the study, including 71 in the TACE group and 27 in the HAIC+TAE group. After 1:1 propensity score matching, a final analysis of 46 patients was conducted to this study. As shown in Table 1, the baseline clinical characteristics of the patients were summarized before and after PSM. Before PSM, the proportion of patients with intermediate stage HCC was higher in TACE group than that in HAIC+TAE group (83.1% vs. 63.0%, P=0.033). After matching, there were no significant differences in baseline characteristics between the two groups.
Baseline characteristics before and after propensity-score matching.

AFP: Alpha-fetoprotein; ALBI: Albumin-bilirubin; BCLC: Barcelona Clinical Liver Cancer.
P<0.05.
Efficacy
Tumor response rates of the two groups are shown in Table 2. There were three patients (13.0%) in the HAIC+TAE group and one patient (4.3%) in the TACE group who achieved a CR (P=0.601). No significant difference was detected in the ORR between the HAIC+TAE group and TACE group (65.2% vs 47.8%, P=0.234). Also, DCRs of the two groups were similar (87.0% vs 82.6%, P=1.000).
Tumor response rates of the two groups, n (%).

CR: Complete response; PR: Partial response; SD: Stable disease; PD: Progressive disease; ORR: Objective response rate; DCR: Disease control rate.
Patients in the HAIC+TAE group had a longer TTP than those in the TACE group (P=0.023), with a median TTP of 316 days (95% CI, 156.3-475.6) in the HAIC+TAE group and 235 days (95% CI, 102.0-368.0) in the TACE group (Figure 1). As shown in Figure 2, Patients treated with HAIC+TAE had a longer median OS compared with those treated with TACE (580 d vs 493 d, P=0.020). At one year, 12 patients (52.2%) in the HAIC+TAE group and 17 patients (73.9%) in the TACE group had disease progression on imaging findings (P=0.127). Death occurred within one year in four patients (17.4%) from the HAIC+TAE group and three patients (13.0%) from the TACE group (P=1.000).
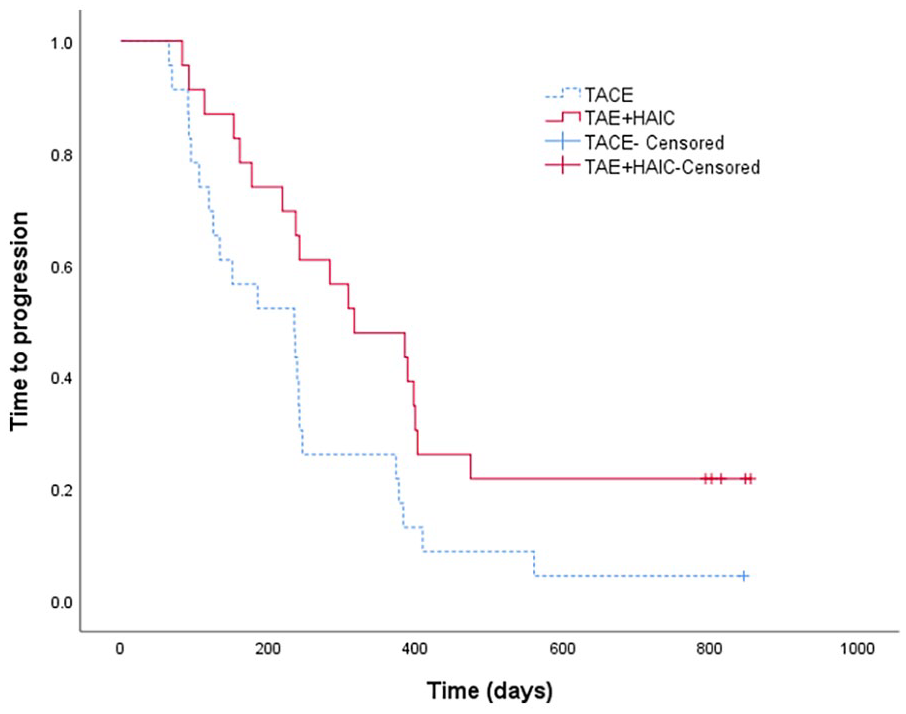
Time to progression analysis comparing HAIC+TAE and TACE patients.
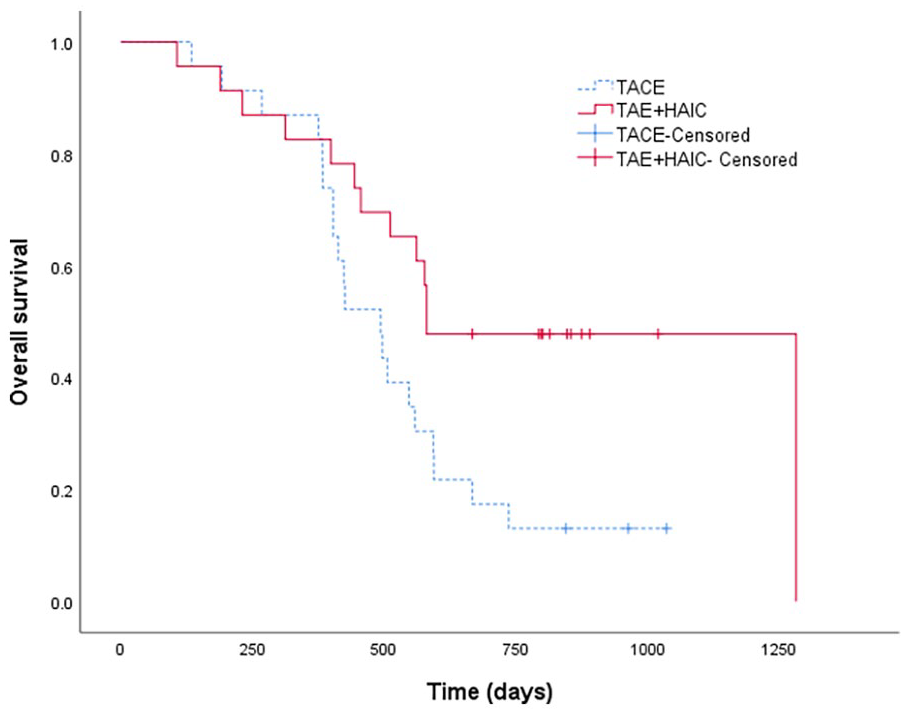
Overall survival analysis comparing HAIC+TAE and TACE patients.
Seventeen patients (six targeted therapy, 11 targeted therapy combined with immunotherapy) in the HAIC+TAE group and 15 patients (four targeted therapy, 11 targeted therapy combined with immunotherapy) in the TACE group received systemic therapy. And there was no significant difference between the two groups (P=0.522).
Safety and adverse events
Patients in the TACE group received a total of 76 treatments and patients in the HAIC+TAE group received a total of 69 treatments. No treatment-related mortality occurred in either group. In the TACE group, a total of six patients underwent ALBI grade changes, with three patients increasing from 1 to 2, one patient increasing from 2 to 3 and two patients reducing from 2 to 1. In the HAIC+TAE group, nine patients underwent ALBI grade changes, with two patients increasing from 1 to 2, two patients increasing from 2 to 3 and five patients reducing from 2 to 1. No significant difference was detected in the change of ALBI grade between the two groups (P=0.449).
As shown in Table 3, there was no significant difference in the incidence of adverse events between the two groups (P>0.05). One patient (4.3%) in the HAIC+TAE group developed grade 3 leukocytopenia and thrombocytopenia. Two patients (8.7%) in the TACE group and one patient (4.3%) in the HAIC+TAE group experienced grade 3 increase in alanine aminotransferase. The liver function of the three patients was improved after treatment with liver-protecting drugs. Other adverse events occurred in both groups including AST elevation, BIL elevation, fever, emesis, abdominal pain, diarrhea and debilitation were all non-severe adverse events (grade 1 or 2). And these reactions could be relieved with symptomatic treatment.
Adverse events after PSM, n (%).

ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; BIL: Serum bilirubin.
Discussion
Cytotoxic drugs commonly used in conventional TACE treatment include cisplatin, epirubicin, doxorubicin and idarubicin. 8 A recent study 9 has shown that intravenous chemotherapy with FOLFOX regimen can improve the ORR and prolong progression-free survival of advanced HCC compared to the widely used epirubicin. Another study 10 confirmed the feasibility of the FOLFOX regimen for hepatic arterial perfusion. It showed that HAIC can prolong survival time of the patients with advanced HCC compared with sorafenib, which is closely related to the appropriate pharmacokinetic and pharmacodynamic properties of the injected drugs. Guo et al 6 found that TAE followed by HAIC can prolong the progression-free survival of uHCC. However, cytotoxic drugs can hardly enter the blocked blood vessels after embolization. It is necessary to investigate the safety and efficacy of HAIC followed by TAE for uHCC, because chemotherapy drugs can seep out into the tumor unrestrictedly this way.
This retrospective study found that HAIC+TAE was as safe as TACE in treating uHCC, as the two groups had similar rates of adverse effects. In addition, ORRs were similar between the two groups (HAIC+TAE vs. TACE, 65.2% vs. 47.8%; P=0.234). Noteworthy, patients in the HAIC+TAE group had a longer median OS and TTP than those in the TACE group. Thus, this study supports the use of the sequential therapy in patients with uHCC.
In contrast to previous studies,6,11 we adjusted the treatment steps by administering HAIC first and then TAE. In this retrospective study, the ORR of the HAIC+TAE group was 65.2%, which was superior to the results of sorafenib/lenvatinib+TACE+HAIC reported in two previous studies (42.4% to 56.1%).12,13 A network meta-analysis 14 showed that the likelihood of maximal TTP was the highest with HAIC treatment. Consistent with the result of this study, patients in the HAIC+TAE group had a longer TTP than patients in the TACE group. In addition, median OS (580 days) in patients treated with HAIC+TAE in this study was equally higher than the findings from recent studies11,15,16 of TACE+HAIC (9.0 months to 10.0 months). The reasons for these results could be as follows: It has been proved that FOLFOX regimen can improve the ORR and prolong progression-free survival of advanced HCC compared to other chemotherapy drugs. 9 Furthermore, HAIC first can enable chemotherapy drugs to fully affect the tumor cells. And then TAE can block the blood vessels. This may decrease the possibility of chemotherapy drug reflux and reduce the side effects of chemotherapy drugs. Given the above, HAIC+TAE might be used as a new treatment strategy for patients with uHCC.
A systematic review 17 revealed that the overall mortality rate for patients treated with TACE was 0.6% and the most common cause of death was related to acute liver insufficiency. Previous studies18,19 have also shown that abnormal liver function was one of the most common adverse effects of TACE. In this study, 60.9% and 43.5% of patients in the TACE group experienced ALT and AST elevation after treatment. The incidence of elevated liver enzymes was close to that described in a previous review. 20 As no significant difference was detected in the incidence of elevated liver enzymes between the two groups. It suggested that the effect of HAIC+TAE on liver function was tolerable.
The incidence of myelosuppression was slightly higher in the HAIC+TAE group compared to that in the TACE group (leukocytopenia HAIC+TAE vs. TACE, 26.0% vs 13%; thrombocytopenia HAIC+TAE vs. TACE, 26.0% vs. 17.4%). However, there was no significant difference between the two groups (leukocytopenia, P=0.457; thrombocytopenia, P=0.475). Although one patient (4.3%) in the HAIC+TAE group met the criteria for a severe adverse event with a grade 3 leukocytopenia and thrombocytopenia, leukocytes and platelets of the patient recovered slowly after treatment discontinuation. A recent study 21 has demonstrated the safety of the TACE+HAIC therapy for HCC with portal vein tumor thrombus. The incidence of myelosuppression in the above study (leukocytopenia, 39.6%; thrombocytopenia, 38.8%) appeared to be higher than that in the HAIC+TAE group of this study. This may be related to the relatively high dose of chemotherapeutic drugs used in TACE+HAIC treatment. Overall, HAIC+TAE treatment was safe enough for uHCC.
Several limitations of this study should be noted. First, the small sample size of this study may cause information bias. Second, it is a pity that different treatment sequences of TAE and HAIC were not compared in this study, because fewer patients accepted HAIC after TAE in our center. Finally, part of the patients received systemic therapy, which would affect the outcomes of the TTP and OS. Therefore, prospective studies with a large sample size are required to verify the results of this study.
Conclusions
The sequential therapy of HAIC+TAE holds the promise of prolonging the median TTP and OS for patients with uHCC when compared to conventional TACE, while maintaining an acceptable safety profile. Consequently, HAIC+TAE could potentially emerge as a novel treatment option for individuals with uHCC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required. This article does not contain any studies with animals performed by any of the authors.
Informed consent
This study has obtained IRB approval from the first affiliated hospital of Soochow University and the need for informed consent was waived.
Consent for publication
Consent for publication was obtained for every individual person’s data included in the study.