
Abstract
Our study evaluated the desire to procreate of 96 mothers of children treated for cancer at the Pediatric Oncology Unit of Istituto Nazionale Tumori of Milan in 2021. Even at a time during which they fear losing the child they already have, nearly one in four mothers expressed their desire to have another child.
This wish emerged within a complex interplay of individual, relational, and sociocultural factors. Notably, cultural expectations surrounding motherhood, self-sacrifice, and the ideal of the “good mother” appeared to intensify feelings of guilt associated with procreative desire in the context of anticipatory grief. Future cross-cultural investigations could clarify how norms regarding motherhood and reproductive choices differ across societies and influence this phenomenon.
Our results also showed a relation between mother’s age, children’s age, stage of disease and presence of siblings: procreative desire was mainly expressed by younger mothers with only one child, in preschool age and with a bad prognosis.
Introduction
In the pediatric oncology setting, the stability of families is often undermined when a child is diagnosed with cancer. Although such an event represents an enormous and complex trauma for the parents, it is not uncommon to meet mothers of patients who are pregnant. Since we frequently work with parents of childbearing age, this may be a simple coincidence of timing. However, clinical experience suggests that parents often choose, even amid a child's complicated and prolonged illness, to give birth to another child.
One may be led to think that during or after an experience of such extreme suffering, it is difficult for a parent to choose to undertake the path of parenthood again. It is known that the more aversive an experience is, the more the individual tends to develop avoidance of what may cause similar pain.1-5 While this is true for most traumatic experiences, it does not seem to apply in the same way to motherhood, whether the trauma involves prenatal or perinatal bereavement or an illness that threatens or leads to the death of a child.6-11
To investigate this fact, we evaluated the desire to procreate of our patients’ mothers, as expressed by them during psychological support interviews.
Beyond individual psychological factors, broader sociocultural expectations appear to shape how mothers experience and interpret this desire. In particular, the pervasive cultural ideal of the “good mother” — selfless, self-sacrificing, and fully devoted to the sick child — may render any wish for another pregnancy morally problematic in the mothers’ own eyes, heightening feelings of guilt and ambivalence. Moreover, notions of motherhood, reproductive choice, and parental duty vary across societies; therefore, future cross-cultural studies may deepen our understanding of how cultural stereotypes around motherhood influence parents’ procreative motivations in the face of a life-threatening pediatric illness.
Furthermore, little is known about whether the motivations for seeking a new pregnancy in this anticipatory grief context overlap with or differ from those observed after a child’s death, as described in post-bereavement literature. Contrasting these two conditions may clarify whether the desire to have another child serves similar psychological functions — such as restoring a sense of purpose, hope, or continuity — or whether it reflects distinct adaptive mechanisms when the child is still alive but gravely ill.
Methods
This study outlines the psychological support given to parents of children and adolescents treated at the Pediatric Oncology Unit of the Istituto Nazionale Tumori of Milan, from 1 January 2021 to 31 December 2021. Due to the pandemic, only one parent had access to the ward, in almost all cases and for most of the time the mother was the parent present. Therefore, our study considers only the mothers who received psychological support.
All psychological evaluations and interviews were conducted by licensed clinical psychologists with expertise in pediatric oncology. The interviews were semi-structured and took place either at the bedside or in a dedicated counseling room, depending on the clinical condition of the child and the mother’s preference.
The semi-structured interview guide explored several domains: emotional responses to the child’s diagnosis, coping strategies, representation of motherhood, perceptions of parental role during the child’s illness, and—when spontaneously expressed by the mother—any reflections on the desire to have another child. Although the procreative desire was not directly solicited, psychologists recorded it when mothers verbalized it spontaneously or in connection with discussions on family planning, fears of loss, or future projections. Notes were taken immediately after each session in the psychological report form, following institutional clinical documentation standards.
The clinical cases were assessed considering maternal age and child age, prognosis (classified for the purpose of this analysis in localized, locally-advanced, metastatic and relapsed) and presence of siblings. For the purpose of this study, “poor prognosis” referred to metastatic or relapsed disease.
Statistical analysis (descriptive analysis and X-Squared Test) was performed using R Statistical Software. 12 Yates’ continuity correction was applied in 2x2 tables.
Given the qualitative nature of the mothers’ statements, the psychologists’ written notes were reviewed to extract all expressions of procreative desire. These were coded as present or absent. No audio recordings were made due to clinical constraints and privacy rules, but written documentation followed a standardized format used in routine clinical activity, allowing consistent extraction of data. The study is based exclusively on anonymized clinical records and did not require ethics committee approval, according to institutional guidelines.
Results
During 2021, 228 new solid tumor diagnoses were made in our Pediatric Oncology Unit. All young patients and their mothers underwent initial psychological evaluation; among these, 87 mothers received ongoing psychological support. In addition, nine mothers of relapsed patients were taken into care during the same period.
The mean age of the mothers of the study was 41.8 years and of the children 10.9 years. On the basis of the data collected during the interviews (Table 1), 22 mothers (23% of cases) verbalized to the psychologist their desire to procreate. In three of these cases a pregnancy had been already achieved during 2021.
Procreative desire and associated variables.
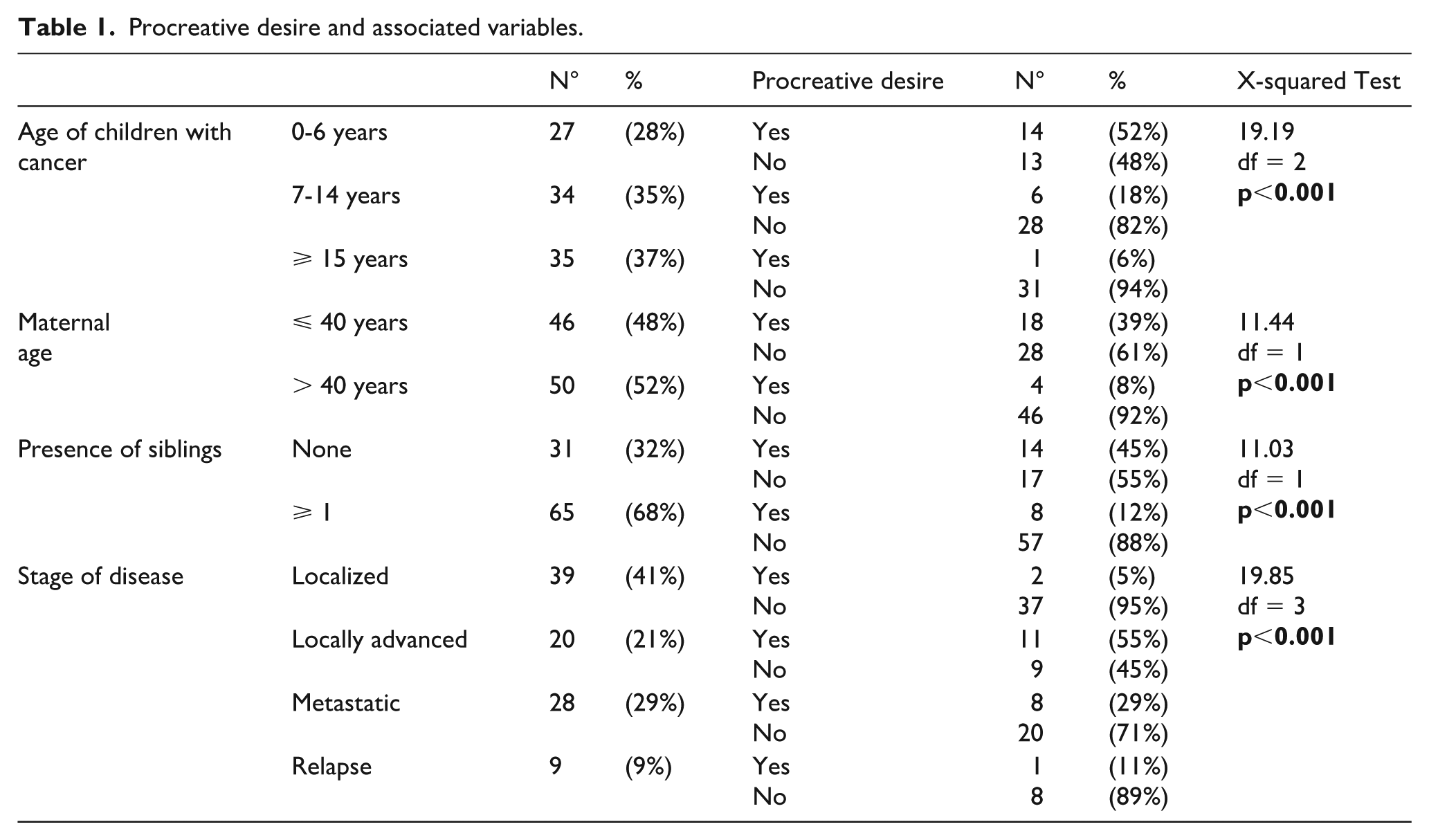
The expression of procreative desire showed significant associations with specific maternal and clinical characteristics. Mothers who verbalized this desire were generally younger than those who did not. Most were mothers of an only child, and the procreative wish was particularly frequent when the child was in preschool age.
Regarding clinical variables, procreative desire emerged more often among mothers of children with a poor prognosis (metastatic or relapsed disease). The association between prognosis and desire to procreate reached statistical significance, suggesting that the perception of high risk for the sick child may play a role in triggering or amplifying this wish.
No significant associations were found between procreative desire and the child’s sex, type of tumor, or time elapsed since diagnosis, although the limited sample size may have reduced the power to detect such effects.
Qualitative review of the clinical notes revealed that the procreative desire was often described as spontaneous, emotionally charged, and accompanied by ambivalence or guilt. Mothers frequently contrasted their longing for another child with a sense of moral conflict regarding their role as caregivers to the sick child.
Discussion
This brief study aims at describing the desire to procreate of the mothers of pediatric cancer patients treated in our center during one calendar year. A relatively large number of mothers communicated their desire to have another child, even while expressing fear for the life of the child currently in treatment.
Interestingly, most mothers subsequently censored or questioned this desire, perceiving it as morally inadmissible or incompatible with the stereotype of a “good mother,” who—according to their internalized expectations—should be entirely devoted to the sick child and willing to sacrifice herself for him or her.
This moral tension reflects deeply rooted cultural narratives about motherhood. Across many societies, mothers are expected to embody selflessness, unconditional availability, emotional containment, and unwavering focus on the child’s well-being. In such a framework, the idea of desiring another pregnancy while one child is gravely ill may be interpreted by mothers as a betrayal of this ideal. These cultural expectations amplify the sense of guilt, contributing to the emotional conflict observed in our interviews.
These feelings of guilt were present in almost all mothers who expressed the desire for another child. Some feared that this wish was a sign of attempting to “replace” the sick child; others believed that another pregnancy would drain time and energy from the child currently fighting for life. The following statements - taken from clinical interviews - illustrate this tension: “I am a bad mother: while my son is fighting for his life, I am already thinking of another child, even though I know he can never be replaced.” Said one mother. Another mother said: “My husband and I confessed that we want another child, but we think it is reckless and may take energy away from our sick daughter.”
No parent is expected to survive his or her children; the sheer unnaturalness of this possibility may partly explain the intensity of parental anguish. Most languages lack a specific term to describe a bereaved parent, suggesting the magnitude of the experience. Despite the gravity of the threat they face, many mothers narrated a desire for life and motherhood, even in the midst of the oncology setting.
Literature on procreative desire after the death of a child mainly concerns prenatal or perinatal bereavement.6,7,9–11,13 It shows that most couples attempt to conceive again shortly after the loss, and that emotional disturbances during the subsequent pregnancy are common.14–19 Some authors suggest that a new pregnancy may serve as a way to fill the emotional void left by the deceased child.15,19,20
Our findings suggest that, although the child in our context is alive, certain psychological mechanisms resemble those described in post-bereavement literature. For some mothers, the desire for another child appears linked to the anticipation of loss, functioning as a coping strategy to counter the existential threat and maintain a sense of future continuity. However, unlike post-bereavement pregnancies, the desire expressed in anticipatory grief is accompanied by stronger guilt, due to the coexistence of care for the sick child and thoughts about a future child. This duality makes the anticipatory context unique and deserving of dedicated research.
The meanings attributed to motherhood, grief, and reproductive choices differ substantially across cultural contexts. The moral judgment mothers expressed around their desire to procreate likely reflects Western ideals of intensive mothering and individual responsibility. In societies where fertility is culturally valorized, or where the maternal role is differently constructed, the emotional experience associated with procreative desire during a child's illness may differ significantly. Future cross-cultural studies could illuminate how social norms, gender roles, and religious or familial expectations shape reproductive motivations during pediatric illness.
In the context of pediatric oncology, the presence of siblings has been reported as a protective factor for both patients and parents.21–24 Some authors suggest that parents may wish to give birth to another child as a potential resource for the sick child, though this remains understudied.
The desire for another child may also have an evolutionary interpretation. Facing the concrete possibility that their child may not survive, parents may experience an instinctive drive to ensure genetic continuity. From an evolutionary standpoint, procreative desire in this context may represent a normative adaptive response rather than a pathological one, counteracting the existential threat posed by the illness. Importantly, this interpretation does not diminish the emotional complexity of the phenomenon but offers an additional layer of understanding that may help clinicians reduce parental guilt. 25-29
Our clinical experience also suggests that giving birth to another child may provide parents with a renewed sense of purpose and a reason to continue living in the face of anticipated grief. Some mothers expressed that imagining a future child helped them endure the psychological burden of their current situation.
Parents frequently stated that they believed it impossible to survive the sorrow of losing a child: “I could not live thinking that I am alive and he is dead”; “I will die with him”.
For clinicians and psychologists, acknowledging the legitimacy of these emotions and recognizing procreative desire as a potential coping mechanism—rather than a sign of denial or selfishness—may be crucial in supporting families. Providing a culturally sensitive, non-judgmental space for discussing these desires may help reduce guilt and promote psychological adaptation.
Our study presents several limitations, including the absence of a control group, which would clarify whether parents of oncology patients differ from their peers in procreative desire. Furthermore, the phenomenon was assessed through spontaneous verbalization during clinical interviews rather than through a dedicated standardized measure.
Future research should aim to systematically investigate the psychological and sociocultural factors underlying procreative desire in this context, compare anticipatory grief–related motivations with post-bereavement pregnancies, and design cross-cultural studies to explore how varying conceptions of motherhood and sacrifice influence this experience.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.