
Abstract
Introduction:
Cachexia is a multifactorial syndrome prevalent in advanced illness. Guidelines rarely integrate the relational, multidimensional perspective of palliative care (PC). Addressing this gap is essential to optimize care. To achieve this, national consensus among PC physicians and nurses on principles and priorities for managing cachexia within PC settings is necessary.
Methods:
A two-round Delphi study was conducted with 43 Italian PC experts (29 physicians, 14 nurses) meeting ⩾10 years’ experience criteria. In Round 1, participants answered open-ended questions informed by literature and a prior exploratory study. Qualitative Framework Method analysis generated 28 statements. In Round 2, statements were rated on a 5-point Likert scale; consensus was defined as ⩾90% agreement (scores 4 or 5).
Results:
Response rates were 82.2% (Round 1) and 95.5% (Round 2). High consensus (⩾90%) from both physicians and nurses was reached for 14 of 28 statements. Unanimous agreement (100%) supported the need for multiprofessional management, assessment of symptom clusters, and reframing the meaning of food in relation to illness stage. Strong agreement was found for dyadic care planning (97.7%), oral care (97.7%), and body image assessment (95.3%). Lower consensus occurred for prioritizing nutritional deficits (55.8%) and routine CRP/prealbumin testing (34.5%), reflecting contextual and prognostic considerations.
Conclusions:
This study defines core PC-oriented principles for cachexia management: interprofessional collaboration, dyadic engagement, early holistic assessment, and goal-concordant interventions. Findings can inform future clinical guidelines, training, and policy development to address cachexia in advanced illness.
Introduction
Patients in palliative care (PC) often face high symptom burdens, notably cachexia, which severely impairs quality of life (QoL). 1 Cachexia is a multifactorial metabolic syndrome linked to chronic illnesses such as cancer, HIV/AIDS, heart failure, Chronic Obstructive Pulmonary Disease (COPD), 2 and chronic kidney disease (CKD). 3
In this study, we used the international consensus definition of cancer cachexia by Fearon et al. 4 : a multifactorial syndrome characterized by ongoing loss of skeletal muscle mass (with or without fat loss) that cannot be fully reversed by conventional nutritional support and causes progressive functional decline. Cachexia is distinct from malnutrition. While the latter may be reversed through adequate nutritional support, cachexia is resistant to nutritional interventions alone.
We acknowledge that definitions of cachexia vary across national and international bodies. The 2008 consensus 5 characterizes cachexia as a complex metabolic syndrome marked by involuntary weight and muscle loss, often accompanied by anorexia, inflammation, and metabolic dysfunction. Major guidelines reflect these elements with different emphases: American Society of Clinical Oncology (ASCO), 6 describes cachexia as a multifactorial syndrome affecting appetite, weight, muscle mass, treatment tolerance, function, and survival; the European Society for Medical Oncology (ESMO) 7 frames it as a condition with both objective (weight and muscle loss, metabolic changes) and subjective (anorexia, early satiety, distress) components; and the European Society for Clinical Nutrition and Metabolism (ESPEN) 8 guideline highlights early nutritional risk screening and multimodal interventions without mandating a single diagnostic threshold.
Outside oncology, terminology diverges further. In CKD, for example, the International Society of Renal Nutrition and Metabolism promotes the concept of protein-energy wasting (PEW). 9
Given the uncertainties in treating cachexia, prevention in high-risk groups is promoted as a practical strategy. Guidelines emphasize early screening, nutritional counselling, and symptom management as key to prevention.6–8 Evidence shows early multimodal interventions—dietary counselling, supplements, exercise, anti-inflammatory methods—can stabilize weight and function when initiated early.10,11 Prevention is especially vital for patients with cancers prone to cachexia, those beginning intensive therapies, and those with chronic inflammatory or catabolic conditions like heart failure, COPD, or CKD. 7 Measures include routine nutrition screening, early dietitian referral, individualized nutrition plans, 12 tailored resistance exercise where feasible, and multiprofessional support to address barriers.
Evidence underscores the necessity of early, multimodal interventions13–16 that are multi-professional17,18 and centered on both patients and care partners (e.g., family caregiver or other primary carer). 19
The palliative care gap
Despite the profound impact of cachexia, current international guidelines 20 largely overlook the syndrome from a PC perspective, 21 omitting principles such as relationality, contextual appropriateness, and person-centered decision-making. 19
To address the limited integration of PC in cachexia management across disease trajectories, we conducted an exploratory study with 39 physicians from PC, oncology, internal medicine, and community health. 22 Participants completed a pre-course survey before a cancer anorexia-cachexia session. Responses revealed four complexities: intervention timing amid uncertainty, adherence and family expectations, assessing multifactorial symptoms, and need for interprofessional care.13,18,23
This Delphi study aims to integrate PC into cachexia guidelines by building consensus among PC experts, defining key components of a context-sensitive, interprofessional approach—based on evidence and experience—to inform future recommendations across cancer and other conditions.
Methods
This study used the Delphi method 24 to achieve consensus on managing patients with cachexia in PC. Whereas surveys in this field have mapped attitudes, knowledge gaps, and interprofessional barriers via large cross-sectional designs,25,26 the Delphi method is expressly designed to iteratively converge expert judgment and prioritize actionable recommendations. 27
The Delphi process for this study included two rounds of feedback.
Composition of the expert panel
A panel of 65 experts, including physicians and nurses from Italy's public health system's specialist PC service, was invited to participate. Experts had ⩾10 years of clinical PC experience, managed advanced illness, including cachexia, and were identified via rosters, networks, and an open call by SICP. The panel comprised specialist PC physicians (excluding non-certified oncologists or internists) and trained nurses, many with extra qualifications. Exclusions included dietitians, physical therapists, pharmacists, and social workers. Invitations detailed study aims, participation procedures, and privacy, with willing participants providing consent. Data was anonymized with unique ID codes for confidentiality.
First Delphi round
In the first Delphi round, tailored open-ended questions were developed for physicians and nurses. An interdisciplinary team—including PC physicians, a nurse, and a qualitative methodologist—created questions using a qualitative approach based on a literature review, guidelines, and a survey with Italian clinicians. 22 A pilot with nine experts tested clarity and relevance, leading to improved wording, removal of redundancies, and added prompts for psychosocial aspects. The final set included 10 questions for nurses and 14 for physicians (see supplemental material). Participants provided open-text responses, analyzed using qualitative content analysis via the framework method. Themes were coded into higher-order categories. The frequency and relevance of themes helped develop 28 statements for the second Delphi round, based on clinical practice and professional experience.
Second Delphi round
In the second pilot phase, 10 experts reviewed the Delphi statements, reorganized statements for coherence, clarified ambiguous terms, and adjusted Likert scale anchors for better interpretability. These refinements ensured the final questionnaires reflected clinical accuracy and practicality, with 28 items for physicians and 20 for nurses (see Table 1). Statements were uploaded to an online platform for anonymous voting on a 5-point Likert scale, with space for comments. A 90% agreement threshold (scores of 4 or 5) was set to ensure strong consensus, reflecting collaborative PC practice.
Statements and consensus reached in the second Delphi round.
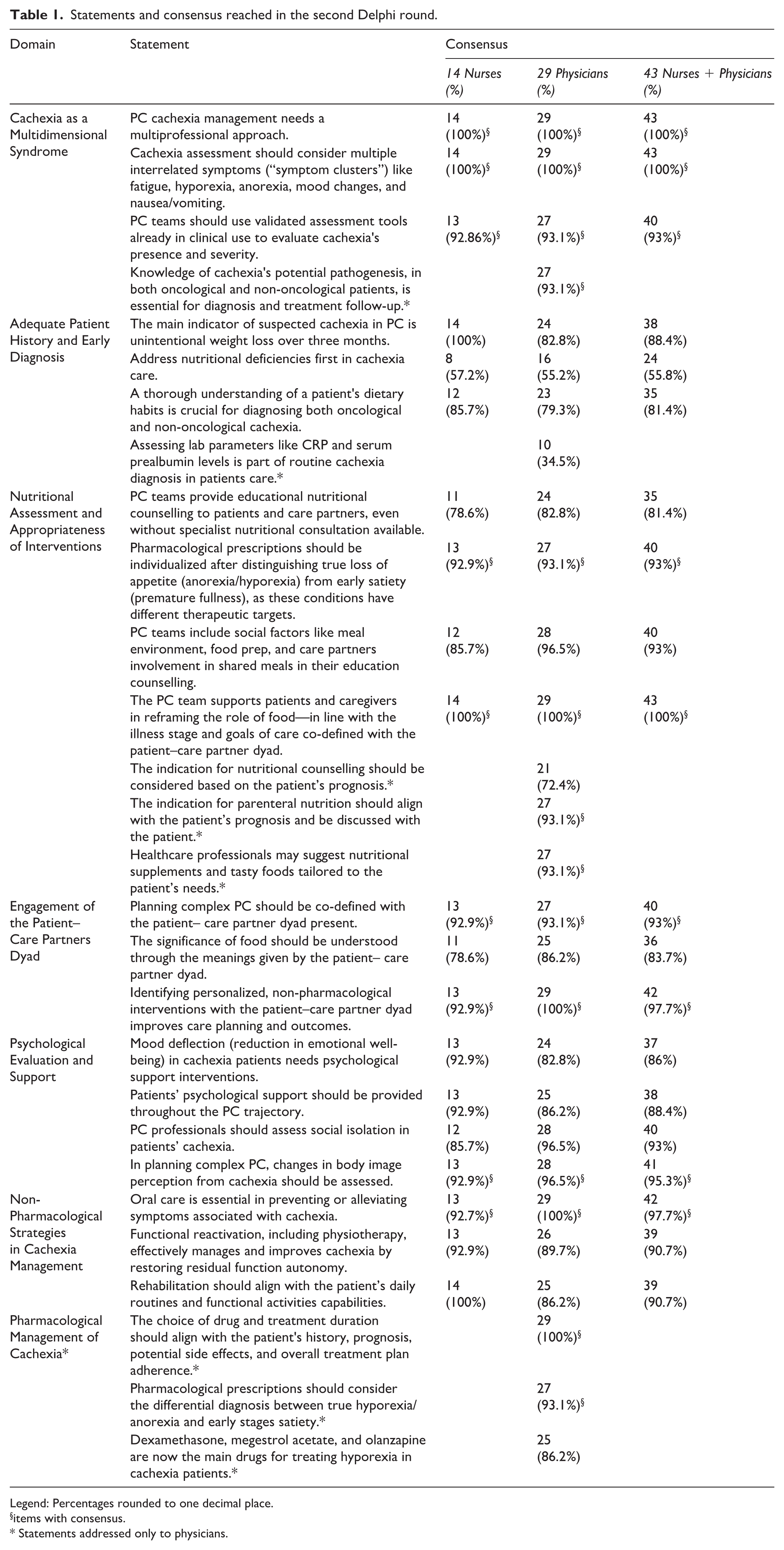
Legend: Percentages rounded to one decimal place.
items with consensus.
Statements addressed only to physicians.
Results
First Delphi round results
Open-ended responses from the first Delphi round produced 36 codes from nurses and 57 from physicians. Key themes included bodily changes, nutritional deficits, and the patient–care partner dyad. Physicians cited weight and muscle loss, while nurses noted symptoms like nausea and anorexia. These findings led to six core themes and 28 statements for the second round.
These themes, refined through team discussion and grounded in the panel’s insights, included: Cachexia as a multidimensional syndrome, adequate patient history and early diagnosis, nutritional assessment and intervention, engagement of patient-care partner dyad (when applicable), psychological evaluation and support, non-pharmacological strategies, and pharmacological management of cachexia. These themes shaped the content and structure of the statements submitted for the second Delphi round.
Second Delphi round results
Most statements achieved over 90% consensus among physicians and nurses. There was high agreement on relational, team-based, and patient-centered approaches, while consensus was lower on operational and prognostic aspects, affected by clinical context and resources.
Multiprofessionalism and symptom clusters
Unanimous agreement (100%) was reached on the statement: “PC cachexia management needs a multiprofessional approach.”
The statement on recognizing symptom clusters, including fatigue, anorexia, and mood deflection (reduction in emotional well-being), received full consensus. Participants agreed cachexia is a multidimensional syndrome—biological, functional, psychological, social—not just nutritional loss.
Reframing food and engaging the patient–care partner dyad
Statements on food's symbolic and relational role, and the importance of the patient–care partners’ dyad, showed high agreement. All respondents (100%) endorsed the concept that “The PC team supports patients and caregivers in reframing the role of food—in line with the illness stage and goals of care co‑defined with the patient–care partner dyad.”
Co-definition of care plans with the dyad received strong support, with comments highlighting cachexia as a key condition needing dyadic approaches—interventions co-delivered to the patient and their primary care partner, whether family or not.
Broad support for non-pharmacological and psychosocial interventions
There was high consensus for non-pharmacological strategies, especially oral care (97.7%). Statements on psychological support also received broad agreement—88.4% favored continuous support—though slightly lower (<90%), possibly because it is seen as part of routine PC. Assessment of body image (95.3%) was supported.
Conditional agreement: Nutritional interventions and appropriateness
Statements concerning nutritional counselling and interventions based on prognosis received variable responses. 93.1% agreed that “The indication for parenteral nutrition should align with the patient’s prognosis and be discussed with the patient.”
Low consensus: Nutritional prioritization and routine lab testing
Three statements failed to reach consensus:
- “Address nutritional deficiencies first in cachexia care.” (55.8%)
- “Routine assessment of CRP and prealbumin levels” (34.5%, physicians only)
- “Unintentional weight loss as the primary indicator for diagnosis” (88.4%)
Diagnostic tools and the need for training
The use of validated tools to assess cachexia received high support (93%), yet many highlighted gaps in awareness and training.
Discussion
This Delphi achieved high consensus on many PC dimensions: relationality, contextual appropriateness, symptom complexity, and person-centeredness. Lower consensus highlights ongoing tensions in diagnostics, prognostic tailoring, and intervention thresholds.6,7,28–31
The highest consensus areas reveal widely accepted aspects of care aligned with PC ethos: relationality, proportionality, interprofessional collaboration, and focus on subjective and social dimensions illness.17,19
Echoing Amano et al., 23 we advocate context-sensitive, co-planned care with patients and care partners—beyond biomedical correction—to preserve dignity, comfort, and QoL.
As to body image assessment, our participants referred to the need to explore perceived changes in appearance, self-consciousness, and loss of bodily integrity, and recommended using validated instruments such as the Body Image Scale (BIS)32,33 and the EORTC QLQ-CAX24 34 (used with QLQ-C30) to capture cachexia-related body-image concerns.
Importantly, this study seeks to enrich guidelines by integrating the lived experience of PC teams who manage cachexia in complex, often non-curative settings. At the same time, in areas where priorities align—such as the need for early identification and multimodal, pharmacological interventions35,36—our findings reinforce the validity of current guidelines.
Consensus statements complement existing guidelines by focusing on biomedical and nutritional interventions, while our findings highlight PC principles—relationality, context, and shared goals with patients and care partners. Incorporating these could foster holistic recommendations that prioritize QoL and outcomes. Future updates should include dyadic care, psychosocial support, and non-drug strategies, addressing physical and emotional aspects of advanced illness. Expanding Delphi processes internationally can validate and adapt these principles across diverse settings.
Strengths and limitations
This study's strengths include using the Delphi method for structured, iterative expert reflection, minimizing bias through online rounds and supporting rigor. The high response rate and low attrition indicated participant engagement. Insights from nurses and physicians, core Italian PC team members, focused on cachexia in PC. A key limitation is the absence of dietitians and social workers, which could have enriched perspectives on nutrition and family dynamics. Italy's PC team varies; this study followed a common model of physicians and nurses, ensuring representativeness but limiting transferability. Future research should include more professionals for stronger interprofessional insights. Qualitative analysis of open responses involved interpretive decisions, making findings Italy-specific and less broadly applicable.
Conclusions
This study advocates person-centered, context-aware care for cachexia in palliative settings. It recommends interdisciplinary management, thorough symptom assessment with validated tools, and low-burden nutritional strategies that consider social and emotional factors. Prioritizing early risk detection and multimodal support aligns cachexia care with palliative goals: enhancing QoL, preserving function, and potentially slowing progression from pre-cachexia to refractory stages through psychological and non-drug approaches.
Supplemental Material
sj-docx-1-tmj-10.1177_03008916261418900 – Supplemental material for Attitudes and beliefs of Italian palliative care experts regarding cachexia: A Delphi study
Supplemental material, sj-docx-1-tmj-10.1177_03008916261418900 for Attitudes and beliefs of Italian palliative care experts regarding cachexia: A Delphi study by Matteo Moroni, Eduardo Bruera, Luca Ghirotto, Gianmarco Priori and Simone Veronese in Tumori Journal
Footnotes
Acknowledgements
The authors wish to express their sincere gratitude to the Italian Society for Palliative Care (SICP) members for their invaluable support throughout the study. We also extend our heartfelt thanks to all the experts—physicians and nurses—who generously contributed their time, insights, and clinical experience to the Delphi process. Their commitment and thoughtful participation were essential to the success of this research.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the Italian Ministry of Health – Ricerca Corrente Annual Program 2027.
Ethical approval and informed consent statements
Before starting, the research team checked with the Ethics Committee to see if approval was needed. Italian laws state that studies involving healthcare professionals without sensitive patient data do not require ethical review. This study used anonymous responses from clinicians to practice questions, with no patient data collected. Procedures followed GDPR, and participants received detailed information about the study’s purpose, methods, and data use.
Consent to participate
Consent was obtained via affirmative email response, and all data were anonymized and stored securely using coded identifiers to ensure confidentiality.
Consent for publication
All participants gave informed consent via email after being explained the study's aims and procedures. No identifiable data is included, and participants know their anonymized data may be used for scientific publications.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.