
Abstract
Introduction
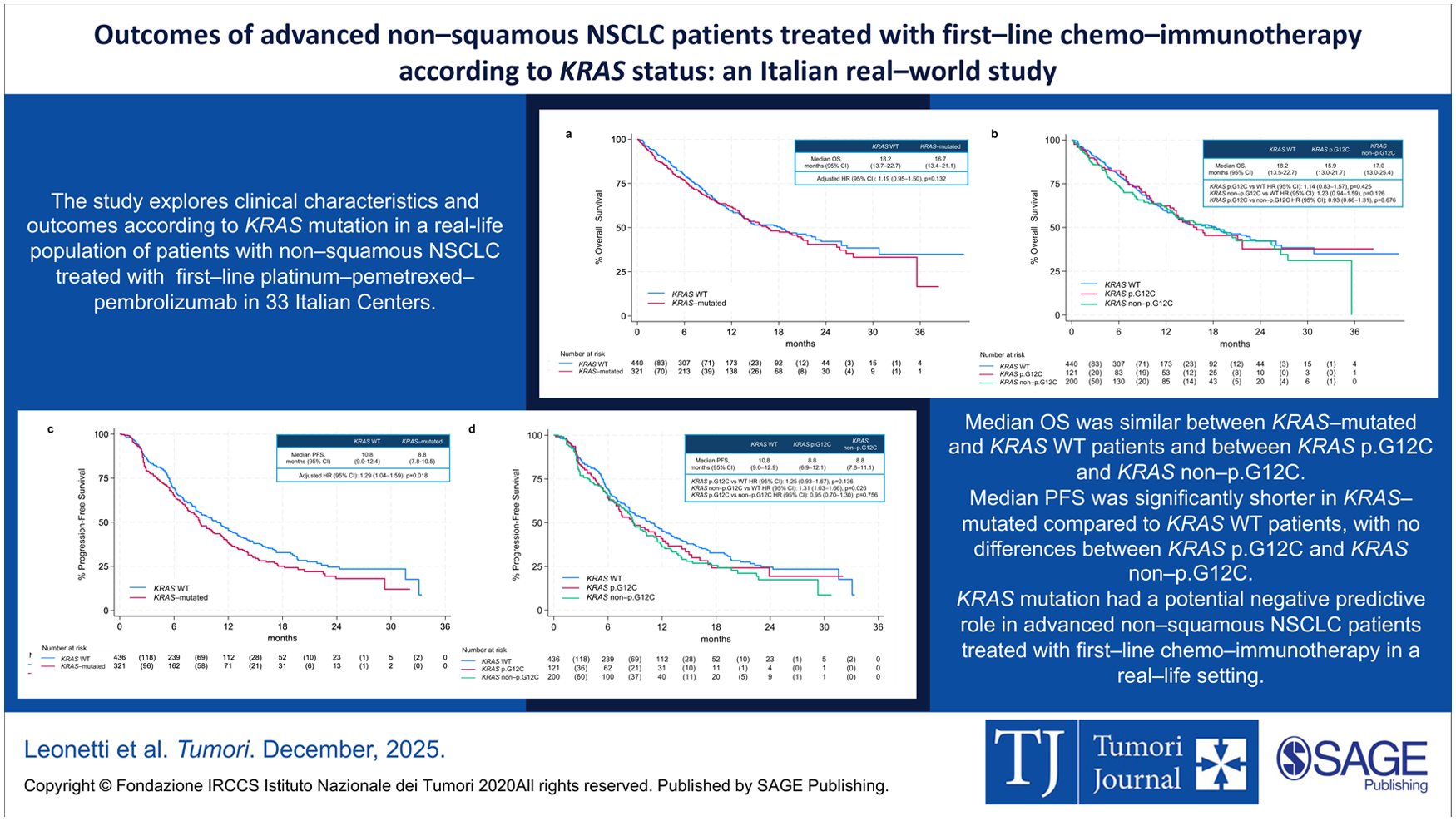
Chemo–immunotherapy is the standard frontline treatment of advanced non–squamous non–small cell lung cancer (nsq–NSCLC). Among oncogenic drivers, KRAS mutation accounts for approximately 25% of lung adenocarcinomas, with p.G12C being the most common variant. This study assessed clinical features and survival outcomes according to KRAS mutation in a real–life population of nsq–NSCLC patients treated with first–line platinum–pemetrexed–pembrolizumab.
Methods
This is a retrospective–prospective study including patients with nsq–NSCLC who received first–line platinum–pemetrexed–pembrolizumab from 4 September 2018 in 33 Italian Centers.
Results
Among the 765 patients included in this analysis, 121 (15.8%) had KRAS p.G12C mutation, 201 (26.3%) KRAS non–p.G12C mutation and 443 (57.9%) KRAS WT. KRAS–mutated patients had more frequently a history of smoking (90.6% vs 84.1%, p=0.012) and bone metastases (44.1% vs 35.9%; p=0.022) compared to KRAS WT.
Median Overall Survival (OS) was similar between KRAS–mutated and KRAS WT patients (16.7 vs 18.2 months; adjusted Hazard Ratio [HR] 1.19, 95% Confidence Interval [CI] 0.95–1.50, p=0.132). No difference in OS was found between KRAS p.G12C and KRAS non–p.G12C (15.9 vs 17.0 months, HR 0.93, 95% CI: 0.66–1.31, p=0.676).
Median progression–free survival was significantly shorter in KRAS–mutated compared to KRAS WT patients (8.8 vs 10.8 months; adjusted HR 1.29, 95% CI 1.04–1.59, p=0.018), with no differences between KRAS p.G12C and KRAS non–p.G12C (8.8 vs 8.8 months, HR 0.95, 95% CI: 0.70–1.30, p=0.756).
Conclusions
KRAS mutation showed a potential negative predictive role in advanced nsq–NSCLC treated with first–line chemo–immunotherapy. The impact of co–mutations and post–progression outcomes warrants further investigation.
Introduction
Chemo–immunotherapy represents a cornerstone in the treatment of metastatic non–small cell lung cancer (NSCLC). The choice of first–line therapy is guided by multiple factors, including histology, tumour genotype, PD–L1 expression, Eastern Cooperative Oncology Group Performance Status (ECOG PS) and comorbidities. 1 In the absence of actionable mutations, the combination of immunotherapy and chemotherapy represents the standard first–line approach, irrespective of PD–L1 expression.1,2
KRAS mutations are the most frequently detected genetic alterations in NSCLC, occurring in approximately 31–35% of cases. Among them, KRAS p.G12C is the most prevalent variant, accounting for 30–40% of KRAS–mutated cases.3-5 KRAS p.G12C frequently co–occurs with mutations in STK11 (10–28%), KEAP1 (6–23%), and TP53 (18–50%), which may influence disease progression and treatment response. 5
The prognostic and predictive role of KRAS mutations remains controversial. A meta–analysis of 43 studies found no significant correlation between KRAS mutations and progression–free survival (PFS) or overall survival (OS) in randomized controlled trials. However, multiple observational studies suggest a negative prognostic role, with poorer response to treatments and an increased likelihood of liver and brain metastases.3,6
KRAS mutations also have predictive value. Indeed, some studies suggest that KRAS mutations may enhance response to anti–PD–(L)1 therapy in combination with chemotherapy.7,8 Conversely, an exploratory analysis of the KEYNOTE–189 and KEYNOTE–407 trials found no significant correlation between KRAS status and the efficacy of pembrolizumab in combination with chemotherapy. 7
Co–occurring mutations further modulate treatment efficacy and prognosis. While STK11 and KEAP1 mutations have been associated with reduced benefit from chemo–immunotherapy,7,9 TP53 co–mutations may enhance responsiveness. 9 The heterogeneity introduced by co–mutations complicates the clinical interpretation of KRAS status, highlighting the need for further investigation.
In this context, we conducted a sub–analysis of a real–world retrospective–prospective study 10 to assess the impact of KRAS mutations on clinical outcomes in advanced non–squamous NSCLC patients treated with first–line chemo–immunotherapy according to the KEYNOTE–189 regimen.
Material and methods
This is a multicentre, retrospective–prospective, observational study involving 33 Italian centres. Patients with advanced non–squamous NSCLC who received first–line treatment with platinum–pemetrexed–pembrolizumab from the date of EMA approval (4 September 2018), were included. Only patients with assessable KRAS status were included in this analysis. Data collection was conducted prospectively from 31 January 2021 for a period of 12 months. Patients were followed up for at least 12 months or until death, last treatment dose, or study cut–off (31 January 2023).
KRAS status was assessed locally using either PCR or next–generation sequencing (NGS) on histological samples. Based on KRAS status, patients were categorized into three groups: KRAS p.G12C mutation, KRAS non–p.G12C mutation and KRAS wild–type (KRAS WT). Computed Tomography (CT)–scan assessment was conducted according to local clinical practice every three–four months. Blinded Independent Central Review (BICR) for radiological imaging was not performed.
The study was approved by the Ethics Committee of the coordinating center (University Hospital of Parma) on 22 September 2020 (protocol number 35333, issued on 17 September 2020), and subsequently by the Ethics Committees of all participating centers. The study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines.
Statistical analysis
Baseline demographic and clinical characteristics were summarized using descriptive statistics. Categorical variables were reported as frequencies and percentages and compared using the χ² test or Fisher’s exact test, as appropriate. Continuous variables were reported as medians with ranges or interquartile ranges (IQR) and compared using non–parametric tests.
Overall survival (OS) and progression–free survival (PFS) were estimated using the Kaplan–Meier method and compared using the log–rank test. Hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated using Cox proportional hazards models, adjusted for clinically relevant covariates (cohort, age, gender, smoking status, bone and liver metastasis, diabetes and PD–L1 value).
Objective response rate (ORR) and duration of response (DoR) were defined according to RECIST version 1.1. All tests were two–sided, and a p–value < 0.05 was considered statistically significant. Statistical analyses were performed using Stata software, version 18.
Clinical data were collected using REDCap, a secure web–based electronic data capture system, installed and managed at the University Hospital of Parma.
Results
A total of 1068 patients were enrolled in the study. Of these, 109 were oncogene–addicted and 194 had missing KRAS status and were excluded from the analysis. The final study population consisted of 765 patients, among whom 322 (42.1%) harboured a KRAS mutation. Specifically, 121 patients (15.8%) had a KRAS p.G12C mutation, while 201 (26.3%) had KRAS non–p.G12C mutations.
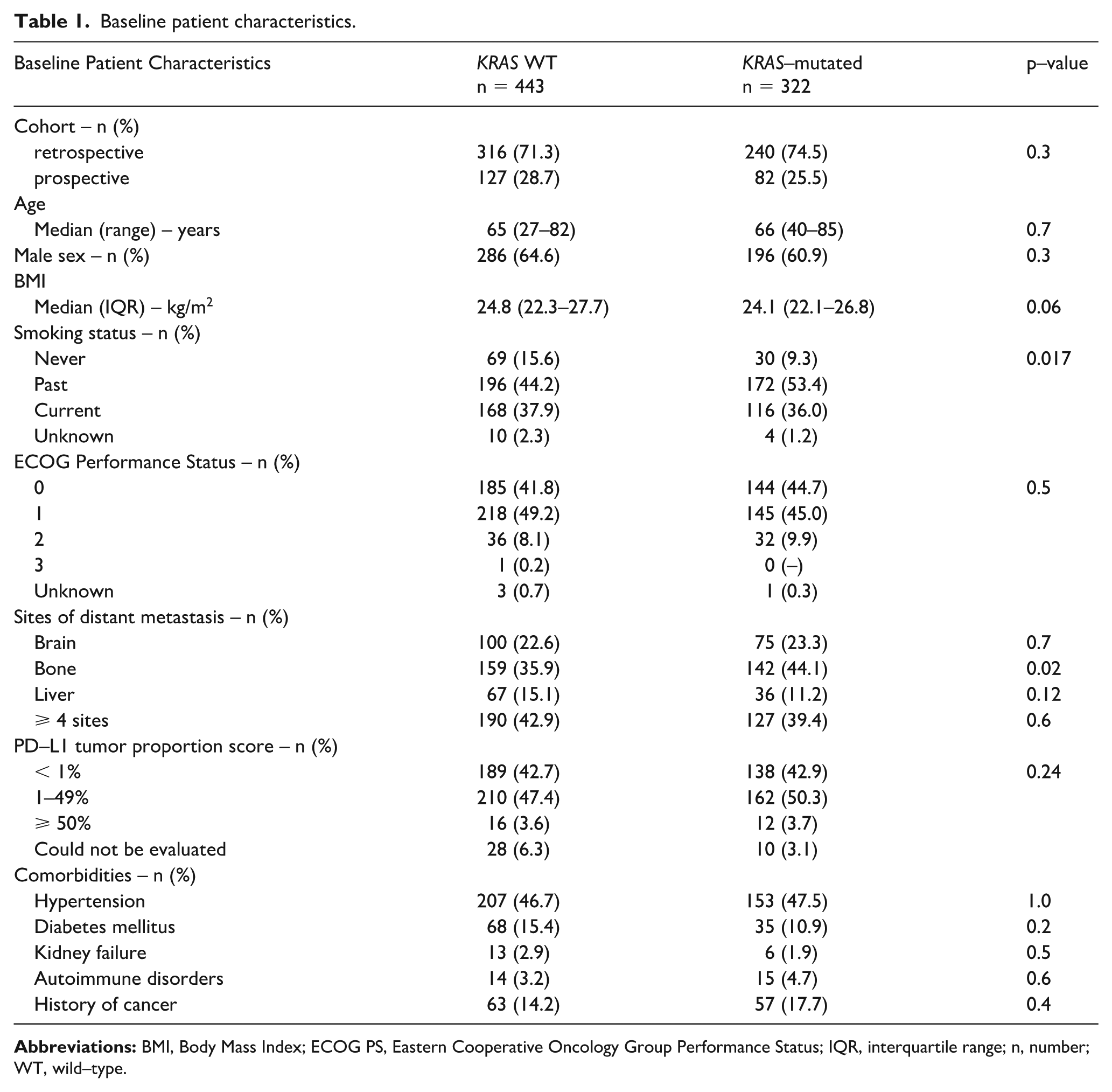
Baseline characteristics of patients are summarized in Table 1 and Online Supplementary Table A1. Differences in patients’ characteristics included a higher prevalence of past/current smoking in KRAS–mutated patients (90.6% in KRAS–mutated vs 84.1% in KRAS WT, p=0.012) and a greater frequency of bone metastases in KRAS–mutated compared to KRAS WT patients (44.1% vs 35.9%, p=0.022).
Baseline patient characteristics.
Median OS was similar between KRAS–mutated and KRAS WT (16.7 vs 18.2 months; adjusted HR 1.19, 95% CI 0.95–1.50, p=0.132; Figure 1a). Within subgroups, median OS tended to be shorter for KRAS p.G12C (15.9 months) compared with KRAS non–p.G12C (17.0 months) and KRAS WT patients (18.2 months), but these differences were not statistically significant (Figure 1b).
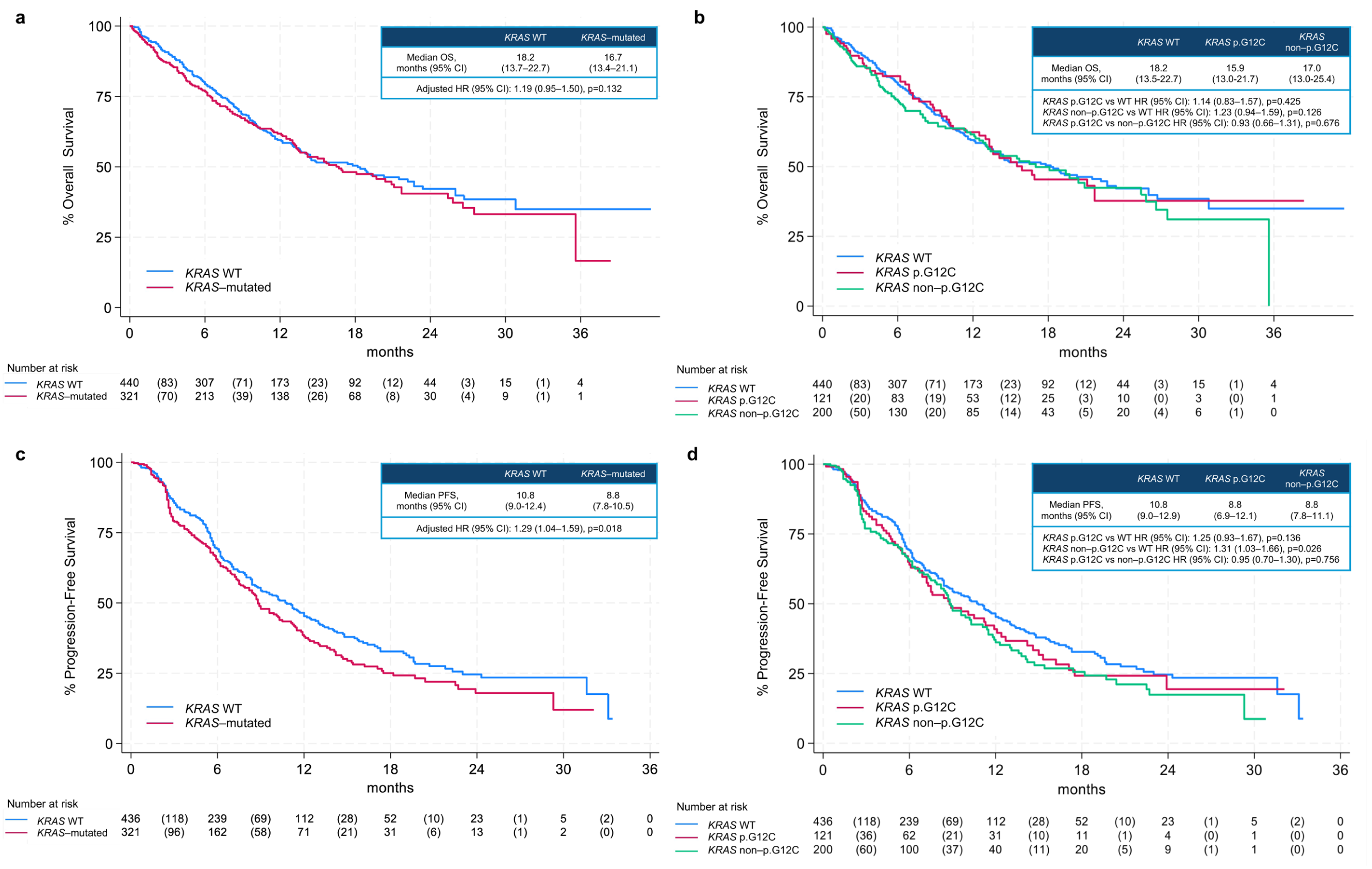
Overall Survival (OS) and Progression–Free Survival (PFS) according to KRAS mutation status: (a) Kaplan Meier curves for OS stratified by KRAS status (mutated vs wild type); (b) Kaplan Meier curves for OS stratified by KRAS subtype (p.G12C, non–p.G12C, and wild type); (c) Kaplan Meier curves for PFS stratified by KRAS status (mutated vs wild type); (d) Kaplan Meier curves for PFS stratified by KRAS subtype (p.G12C, non–p.G12C, and wild type).
Median PFS was significantly shorter in KRAS–mutated patients than in KRAS WT (8.8 vs 10.8 months; adjusted HR 1.29, 95% CI 1.04–1.59, p=0.018; Figure 1c). Within subgroups, KRAS non–p.G12C mutations were associated with shorter PFS than KRAS WT (8.8 vs 10.8 months; HR 1.31, 95% CI 1.03–1.66, p=0.026), while KRAS p.G12C mutations showed no significant difference versus KRAS WT (HR 1.25, 95% CI 0.93–1.67, p=0.136; Figure 1d). No significant PFS difference was observed between KRAS p.G12C and KRAS non–p.G12C (HR 0.95, 95% CI 0.70–1.30, p=0.756).
Objective response rate (ORR) and median duration of response (DoR) did not significantly differ between KRAS–mutated and KRAS WT patients (ORR 41.6% vs 47.6%, p=0.106; DoR 13.8 vs 14.8 months, p=0.606), nor between KRAS p.G12C and KRAS non–p.G12C subgroups (ORR 44.6% vs 39.8%, p=0.179; DoR 16.2 vs 13.6 months, p=0.498). Partial response was the most common best overall response across all the subgroups: KRAS WT (45.2%), KRAS p.G12C (42.2%) and KRAS non–p.G12C (37.8%). Lung was the most common site of progression: KRAS WT (33.4%), KRAS p.G12C (32.2%) and KRAS non–p.G12C (36.8%) (Table 2 and Online Supplementary Table A2).
Treatment outcomes in KRAS WT and KRAS–mutated patients.
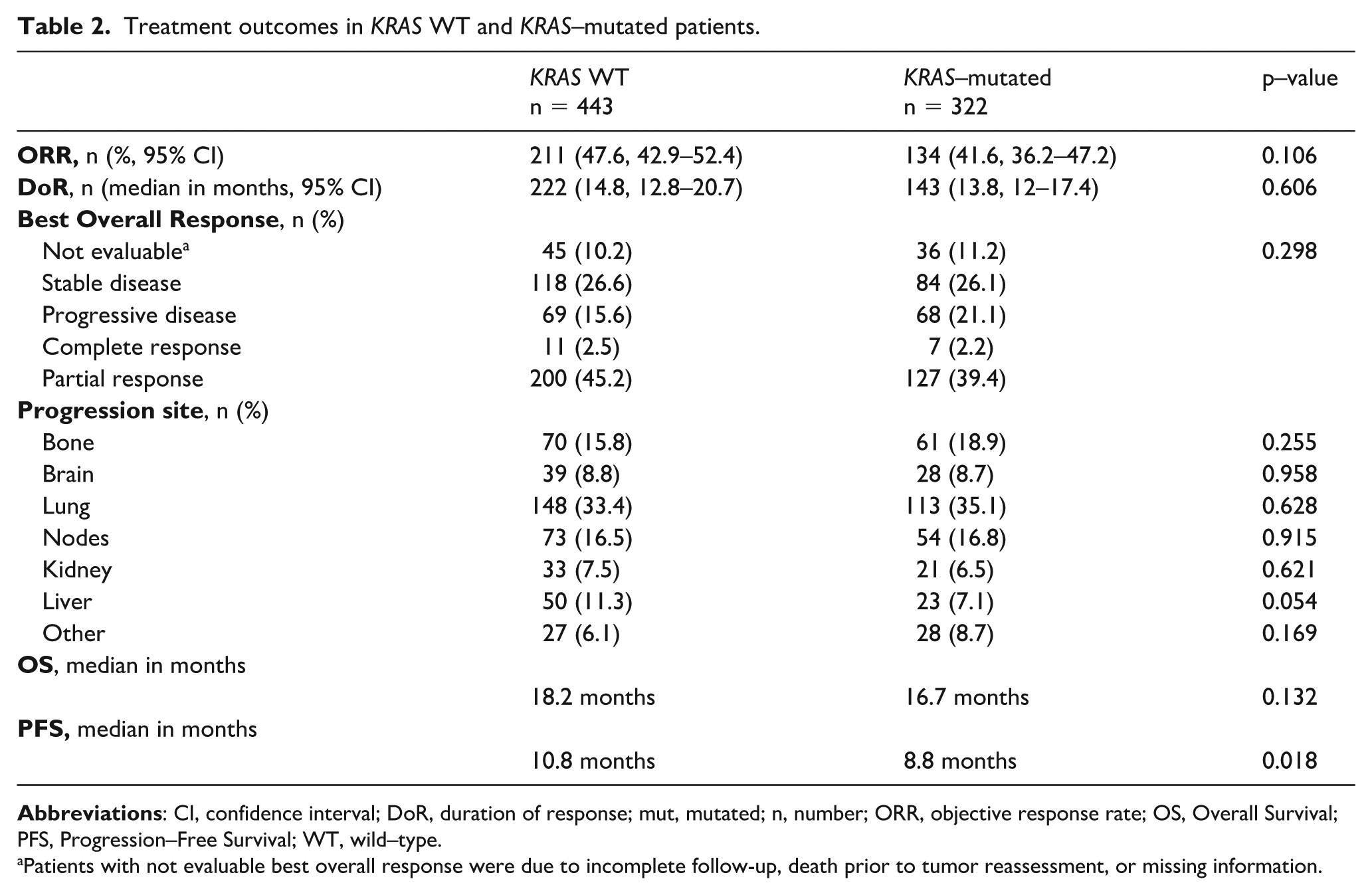
Patients with not evaluable best overall response were due to incomplete follow-up, death prior to tumor reassessment, or missing information.
Among patients progressing after first–line chemo–immunotherapy, 30.0% of KRAS WT and 34.5% of KRAS–mutated patients received a second–line therapy (p=0.184; Table 2 and Online Supplementary Table A3). The KRAS G12C inhibitor sotorasib was administered exclusively to KRAS–mutated patients (5.0%, p<0.001), and participation in clinical trials was more frequent in this group compared to KRAS WT patients (3.7% vs 1.6%, p=0.002).
Discussion
In this large multicentric real–world study, we evaluated the prognostic and predictive role of KRAS mutations in advanced non–squamous NSCLC patients treated with first–line chemo–immunotherapy according to the KEYNOTE–189 regimen. The prevalence of KRAS mutations (42.1%), and particularly of the p.G12C variant (15.8%), was consistent with previous epidemiological reports, confirming the high frequency of KRAS alterations in lung adenocarcinoma. 11
Our analysis showed that KRAS–mutated patients more frequently had a smoking history, in line with previous observations linking KRAS mutations with smoking–related carcinogenesis.12-15 Interestingly, non–p.G12C mutations were more prevalent among former smokers, supporting the heterogeneity of environmental and biological drivers behind specific KRAS variants. The presence of bone metastases was more frequent in KRAS–mutated patients compared to KRAS WT. Although bone involvement is recognized as a negative prognostic factor in NSCLC, literature data on its association with KRAS status are conflicting.16,17 Notably, we did not find significant correlations between KRAS status and PD–L1 levels, in contrast with available literature suggesting that KRAS mutation is associated with higher level of PD–L1.18,19 This result could have been influenced by the low proportion of PD–L1 ⩾ 50% patients included in our study, due to the Italian Regulatory Authority restrictions for the combination only in patients with tumor expressing PD–L1 < 50%, negative or not evaluable.
Median OS did not significantly differ between KRAS–mutated and KRAS WT patients, although a trend toward inferior survival among KRAS–mutated was observed. On the other hand, we observed a significantly shorter median PFS in KRAS–mutated patients, irrespective of the mutation subtype, compared to KRAS WT. This suggests that KRAS mutations may confer reduced benefit from the combination of chemotherapy and immunotherapy in the first–line setting. This result is partially concordant with previous real–world analyses reporting that KRAS status does not impact negatively on OS, even though available literature is contrasting.20-22 A possible explanation is the availability of subsequent treatment lines, including KRAS–targeted therapies or alternative systemic approaches, which may mitigate the initial disadvantage conferred by KRAS mutations on long–term survival. Consistently, in our study, second–line treatments, particularly the KRAS G12C inhibitor sotorasib and participation in clinical trials, were more frequent among KRAS–mutated patients, potentially contributing to the similar OS despite shorter PFS. In addition, the biological heterogeneity of KRAS–mutated NSCLC, driven by co–occurring genomic alterations and different PD–L1 expression levels, may substantially influence treatment response and clinical outcomes. 21 In particular, the co–occurring mutations in STK11 and KEAP1 have been consistently associated with resistance to PD–1/PD–L1 inhibitors and worse clinical outcomes among KRAS–mutated patients.23-25 Conversely, KRAS/TP53 co–mutated tumors display a more “hot” immune profile, with increased interferon–γ signaling and higher PD–L1 expression, translating into better sensitivity to immunotherapy.26,27 The absence of co–mutation data represents a limitation of our study, as it prevented the evaluation of clinically relevant KRAS subgroups with distinct sensitivity to immunotherapy. Indeed, STK11 and KEAP1 co–mutations may have contributed to the shorter PFS observed in KRAS–mutated compared with KRAS WT patients.
Notably, we did not observe significant differences in ORR or DoR between KRAS–mutated and KRAS WT patients, nor between KRAS p.G12C and non–p.G12C subgroups. This finding indicates that KRAS status does not influence the likelihood of achieving an initial radiological response, but rather affects the duration of disease control. This aligns with prior studies reporting no clear impact of KRAS mutations on response rates to immunotherapy.22,28 Of note, the presence of TP53 co–mutation may have mitigated the impact of other negative co–mutations such as STK11 or KEAP1 within the KRAS–mutated group, contributing to the similar ORR and DoR observed in our cohort.
The therapeutic landscape of KRAS–mutated NSCLC is rapidly evolving. While sotorasib and adagrasib, KRAS p.G12C inhibitors, are currently approved in the post–platinum setting, emerging evidence suggests that their integration in earlier lines may improve outcomes.29-31 Combinations with chemotherapy, immunotherapy, or other targeted agents (e.g., SHP2, EGFR, MET inhibitors) are being explored to overcome resistance mechanisms and enhance durability of response. Our results showing limited benefit of chemo–immunotherapy in KRAS–mutated patients, especially in terms of PFS, reinforce the need to tailor treatment strategies for this subgroup.
Limitations of our study include the retrospective component of data collection, lack of BICR and the absence of molecular data on co–mutations, which may have confounded outcomes. Additionally, the absence of information on the proportion of KRAS testing performed by PCR versus NGS across centers may have introduced potential detection bias.
Conclusions
Our study confirmed the potential negative predictive role of KRAS mutation in advanced non–squamous NSCLC patients treated with first–line chemo–immunotherapy, without significant differences in OS, ORR and DoR. The development and integration of novel KRAS–targeted therapies will likely reshape treatment algorithms and further refine the prognostic and predictive role of KRAS status.
Supplemental Material
sj-docx-1-tmj-10.1177_03008916261443123 – Supplemental material for Outcomes of first-line chemo-immunotherapy in advanced non-squamous NSCLC according to KRAS status: An Italian real-world study
Supplemental material, sj-docx-1-tmj-10.1177_03008916261443123 for Outcomes of first-line chemo-immunotherapy in advanced non-squamous NSCLC according to KRAS status: An Italian real-world study by Alessandro Leonetti, Vanessa Callegari, Fabiana Perrone, Giuseppe Maglietta, Paola Bordi, Emilio Bria, Emanuele Vita, Francesco Gelsomino, Andrea De Giglio, Alain Gelibter, Marco Siringo, Francesca Mazzoni, Enrico Caliman, Carlo Genova, Giulia Barletta, Federica Bertolini, Giorgia Guaitoli, Francesco Passiglia, Marco Donatello Delcuratolo, Michele Montrone, Sara Oresti, Giulia Pasello, Elisa Roca, Lorenzo Belluomini, Fabiana Letizia Cecere, Annalisa Guida, Anna Manzo, Alessandro Russo, Francesca Rastelli, Alessandra Bulotta, Fabrizio Citarella, Luca Toschi, Federica Zoratto, Diego Luigi Cortinovis, Francesco Paoloni, Alessandro Follador, Annamaria Carta, Andrea Camerini, Flavio Salerno, Rosa Rita Silva, Editta Baldini, Corrado Ficorella, Matteo Brighenti, Matteo Santoni, Francesco Malorgio, Caterina Caminiti, Matteo Puntoni and Marcello Tiseo in Tumori Journal
Supplemental Material
sj-docx-2-tmj-10.1177_03008916261443123 – Supplemental material for Outcomes of first-line chemo-immunotherapy in advanced non-squamous NSCLC according to KRAS status: An Italian real-world study
Supplemental material, sj-docx-2-tmj-10.1177_03008916261443123 for Outcomes of first-line chemo-immunotherapy in advanced non-squamous NSCLC according to KRAS status: An Italian real-world study by Alessandro Leonetti, Vanessa Callegari, Fabiana Perrone, Giuseppe Maglietta, Paola Bordi, Emilio Bria, Emanuele Vita, Francesco Gelsomino, Andrea De Giglio, Alain Gelibter, Marco Siringo, Francesca Mazzoni, Enrico Caliman, Carlo Genova, Giulia Barletta, Federica Bertolini, Giorgia Guaitoli, Francesco Passiglia, Marco Donatello Delcuratolo, Michele Montrone, Sara Oresti, Giulia Pasello, Elisa Roca, Lorenzo Belluomini, Fabiana Letizia Cecere, Annalisa Guida, Anna Manzo, Alessandro Russo, Francesca Rastelli, Alessandra Bulotta, Fabrizio Citarella, Luca Toschi, Federica Zoratto, Diego Luigi Cortinovis, Francesco Paoloni, Alessandro Follador, Annamaria Carta, Andrea Camerini, Flavio Salerno, Rosa Rita Silva, Editta Baldini, Corrado Ficorella, Matteo Brighenti, Matteo Santoni, Francesco Malorgio, Caterina Caminiti, Matteo Puntoni and Marcello Tiseo in Tumori Journal
Supplemental Material
sj-docx-3-tmj-10.1177_03008916261443123 – Supplemental material for Outcomes of first-line chemo-immunotherapy in advanced non-squamous NSCLC according to KRAS status: An Italian real-world study
Supplemental material, sj-docx-3-tmj-10.1177_03008916261443123 for Outcomes of first-line chemo-immunotherapy in advanced non-squamous NSCLC according to KRAS status: An Italian real-world study by Alessandro Leonetti, Vanessa Callegari, Fabiana Perrone, Giuseppe Maglietta, Paola Bordi, Emilio Bria, Emanuele Vita, Francesco Gelsomino, Andrea De Giglio, Alain Gelibter, Marco Siringo, Francesca Mazzoni, Enrico Caliman, Carlo Genova, Giulia Barletta, Federica Bertolini, Giorgia Guaitoli, Francesco Passiglia, Marco Donatello Delcuratolo, Michele Montrone, Sara Oresti, Giulia Pasello, Elisa Roca, Lorenzo Belluomini, Fabiana Letizia Cecere, Annalisa Guida, Anna Manzo, Alessandro Russo, Francesca Rastelli, Alessandra Bulotta, Fabrizio Citarella, Luca Toschi, Federica Zoratto, Diego Luigi Cortinovis, Francesco Paoloni, Alessandro Follador, Annamaria Carta, Andrea Camerini, Flavio Salerno, Rosa Rita Silva, Editta Baldini, Corrado Ficorella, Matteo Brighenti, Matteo Santoni, Francesco Malorgio, Caterina Caminiti, Matteo Puntoni and Marcello Tiseo in Tumori Journal
Footnotes
Acknowledgements
We wish to thank all the patients, family members and staff from all the units that participated in the study.
Data availability
The datasets analyzed in this study are available from the corresponding author with reasonable instrumental restrictions and upon motivated request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lorenzo Belluomini received speakers’ fees from Astra-Zeneca, MSD, Roche, BMS, Amgen, Takeda. Federica Bertolini declares grants for advisory boards from BMS, MSD, Roche, AMGEN, Novartis, and Regeneron, speaker’s fee from Astra Zeneca, travel grant from MSD and Roche. Emilio Bria has received grants or contracts from Astra-Zeneca, Roche and honoraria for lectures from Merck-Sharp & Dome, Astra-Zeneca, Pfizer, Eli-Lilly, Bristol-Myers Squibb, Novartis, Takeda and Roche. Emilio Bria has been member of Data Safety Monitoring Board or Advisory Board of Merck-Sharp & Dome, Pfizer, Novartis, Bristol-Myers Squibb, Astra-Zeneca, and Roche. Fabrizio Citarella received speakers’ fees from Astra-Zeneca and Novartis. Fabrizio Citarella has received writing support fee from BMS. Alessio Cortellini declares grants for consultancies/advisory boards from MSD, OncoC4, IQVIA, AstraZeneca, Access Infinity, Ardelis Health Alpha Sight; speaker fees from Astra Zeneca, Eisai, Pierre-Fabre, MSD, Sanofi/REGENERON; writing/editorial activity from BMS and MSD; travel support from Sanofi and MSD. Diego Luigi Cortinovis received speakers’ and scientific advisors’ fees from Astra-Zeneca, Boehringer Ingelheim, Roche, Pfizer, Daiichi Sankyo, Amgen, Sanofi/Regeneron, BeOne, BMS, MSD, Eli-Lilly, Catalym. Andrea De Giglio received travel support by Daiichi Sankyo. Alain Gelibter has been on advisory board for Astra-Zeneca, MSD, Roche, BMS, Takeda. Francesco Gelsomino declares grants for consultancies/advisory boards from Pfizer, BMS, Regeneron, Eli-Lilly, Novartis. Giorgia Guaitoli declares grants for advisory boards from Roche and AMGEN, speaker’s fees from Roche, Pfizer and Regeneron, editorial projects from Novartis, travel and accommodation support from MSD, Roche and Astrazeneca. Alessandro Leonetti has received speaker’s fee for AstraZeneca, BMS, MSD, Regeneron, Sanofi and Takeda. Alessandro Leonetti has been on advisory board for Amgen, AstraZeneca, BeOne, Novartis and Sanofi. Alessandro Leonetti has received consultant’s fee for Amgen. Alessandro Leonetti has attended editorial activities sponsored by Eli Lilly, Novartis and Roche. Alessandro Leonetti has received travel support from MSD, Novartis, Roche and Takeda. Francesca Mazzoni declares grants for advisory boards or speaker fees from Roche, MSD, BMS, Astra Zeneca, Regeneron, Amgen, J&J. Francesco Passiglia received advisory/consultant fee from Astrazeneca, J&J, Amgem, BeOne, Pfizer, Roche, BMS, MSD, Daichii Sankyo, Gilead, Pharmamar, Thermofisher Scientific.
Alessandro Russo has received advisory board or consultancy from AstraZeneca, MSD, Novartis, Pfizer, BMS, Takeda, Amgen, Regeneron, Daiichi Sankyo, Merck, Johnson & Johnson, Abbvie, Roche, Boehringer Ingelheim and BeOne. Marcello Tiseo received speakers’ and consultants’ fee from Astra- Zeneca, Pfizer, Eli-Lilly, BMS, Novartis, Roche, MSD, Boehringer Ingelheim, Otsuka, Takeda, Pierre Fabre, Amgen, Merck, Sanofi. Marcello Tiseo received institutional research grants from Astra-Zeneca and Boehringer Ingelheim. Luca Toschi declares grants for consultancies/advisory boards from BeOne, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Sanofi, Takeda; speaker’s fees from Amgen, AstraZeneca, Roche, Johnson & Johnson, Bristol Myers Squibb, Novartis; institutional research grant from Pfizer
All remaining authors have declared no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of the coordinating center (University Hospital of Parma) on 22 September 2020 (protocol number 35333, issued on 17 September 2020), and subsequently by the Ethics Committees of all participating centers. The study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. All alive patients gave written consent to use their data for the study.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.