
Abstract
Hereditary cancer genetics is increasingly recognized as an integral component of cancer care, contributing to treatment, early detection, and risk reduction strategies for patients and their relatives. In this context, several hereditary cancer programs, databases, recommendations, and guidelines have been implemented within the Italian National Health System and at hospital level. However, independent and specific quality indicators for hereditary tumor management are still lacking, limiting the ability to evaluate activities across individual centers. To address this gap, AIFET (Associazione Italiana Familiarità ed Ereditarietà Tumori) has established a dedicated scientific committee for the development of such quality indicators. Here, for the first time to our knowledge, we present a set of 37 quality indicators derived from a national Italian survey. The indicators were organised into four sections: General indicators (applicable to all syndromes), specific to hereditary breast and ovarian cancer, specific to colorectal cancer and polyposis, specific to melanoma predisposition. By promoting consistency across centres, this model may not only enhance the quality of care nationally but also foster collaboration with European institutions toward shared standards in hereditary cancer management.
Introduction
The genetics of hereditary tumors are increasingly recognized as an integral component of cancer care, playing a fundamental role in treatment, early detection, and risk reduction for patients and their families. Identifying hereditary cancer predisposition can provide substantial benefits for the community by detecting individuals at increased risk. Specifically, such benefits include reducing the likelihood of cancer development, diagnosing tumors at an earlier and more treatable stage, informing the optimal choice of targeted therapies when cancer develops, and guiding reproductive decisions.
Genetic testing of probands—usually individuals already affected by cancer—together with cascade testing of relatives and the provision of comprehensive downstream services, can effectively reduce both cancer incidence and mortality in the population. Achieving this goal requires the establishment of dedicated services that are adequately resourced and subject to regular quality monitoring.
In Italy, many centers currently identify genetic cancer predisposition, but some have expertise limited to specific syndromes depending on hospital activity (e.g., breast/ovarian or colorectal cancer). In such a fragmented scenario, certain steps in the diagnostic–therapeutic pathway for inherited tumor identification and carrier management are often outsourced or lacking. This heterogeneity is generally due to two main reasons:
The highly specialized role of certain centers acting as tertiary referral hospitals (e.g., Breast, Prostate, or Lung Units).
The management of tumors requiring less specialized or more widespread care (e.g., cutaneous tumors or intestinal adenomas).
Currently, most centers operate independently, without a coordinated national framework. There is no standardized model of care for patients with hereditary cancer predisposition in Italy, nor are there multidisciplinary national guidelines for genetic assessment, testing, or management. For this reason, the definition of quality indicators (QIs) specific to hereditary cancers is essential to evaluate both the quality and the completeness of each step in the care pathway, from diagnosis to the management of at-risk relatives.
In November 2021, the Italian Association for Familial and Hereditary Tumours (AIFET, Associazione Italiana Familiarità ed Ereditarietà Tumori) was founded, building on the Italian Association for Familial and Hereditary Gastrointestinal Cancers (AIFEG), established in 2002. 1 AIFET is a multidisciplinary national society with the mission of improving the identification and management of hereditary tumors in Italy. To coordinate and strengthen familial cancer services across the country, AIFET has developed a set of specific QIs designed to measure adherence of clinical practice in this field to international standards.
The proposed QIs focus on hereditary syndromes involving breast cancer, colorectal cancer, and melanoma. These areas were selected by AIFET expert sub-panels because they are potentially relevant in every hospital, regardless of the level of specialization, and are therefore considered “Universal.”
To test the proposed QI set, all Italian institutions affiliated with AIFET were invited to participate in a survey assessing adherence to these indicators. This pilot study aims to provide the foundation for developing a robust set of indicators for future accreditation programs, designed to measure and monitor the quality of care pathways for individuals with hereditary cancer predisposition.
Methods
To identify appropriate indicators for hereditary cancers, the AIFET Committee conducted a literature review of evidence-based recommendations. Specifically, guidelines from NCCN,2–3 ERN Genturis, 4 NICE, 5 and recommendations from the Italian Societies of Medical Oncology (AIOM), Pathology (SIAPEC), 6 and Human Genetics (SIGU) 7 were considered. However, no publications directly addressing this specific topic were identified. All documents were shared with experts invited to contribute to this consensus paper. The indicators identified were derived using national and international guidelines, shared by all commission members and are in agreement with therapeutic diagnostic pathways for hereditary tumors published by the Italian Ministry of Health (AGENAS). 8
The AIFET Committee, which includes specialists in genetics, oncology, surgery, gastroenterology, pathology, and psychology, met in 2023 and agreed to develop a set of quality indicators for the following cancer predisposition syndromes 9 :
Lynch syndrome (ORPHA 144)
Familial polyposis syndromes (ORPHA 733, 247798)
Hereditary breast and ovarian cancer syndrome (ORPHA 145)
Melanoma predisposition syndrome (ORPHA 618)
According to the Agency for Healthcare Research and Quality (AHRQ) Evidence Report No. 105 (04-E030-2, 2004), the key properties of a quality measure are reliability and validity. Validity means that the indicator truly measures what it is intended to, while reliability implies that the observation is consistently reproducible—either by the same observer over time or by different observers.
Two additional properties are also relevant:
Usability, meaning the results generated are easy to interpret and can inform actions to improve healthcare delivery.
Feasibility, meaning data collection should be straightforward during routine clinical practice, with limited costs.
The expert panel was therefore asked, whenever possible, to select indicators that were simple, clearly defined, and covered both process and outcome measures. In the context of certification, the number of QIs was deliberately kept to a minimum, with the goal of reflecting the entire diagnostic and therapeutic process while relying on readily available, systematically collected variables.
For each indicator, both its definition and assigned numerical values were reported. These values were determined based on the clinical relevance of the recommendation. The sum of all values produced a score for each participating institution.
The indicators were organized into four sections:
General indicators (applicable to all syndromes)
Indicators specific to hereditary breast and ovarian cancer
Indicators specific to colorectal cancer and polyposis
Indicators specific to melanoma predisposition
These indicators are qualitative, systemic, and syndrome-oriented. No quantitative indicators were included.
The indicators were tested across Italian centers affiliated with AIFET. To this end, each center completed a structured questionnaire, which was subsequently approved by the competent administrative authority of the respective healthcare provider.
The study was conducted in accordance with the procedures for observational studies and in compliance with the ethical principles of the Declaration of Helsinki (59th WMA General Assembly, Seoul, Korea, October 2008). The study protocol was submitted to the Ethics Committee of Verona (CESC).
Results
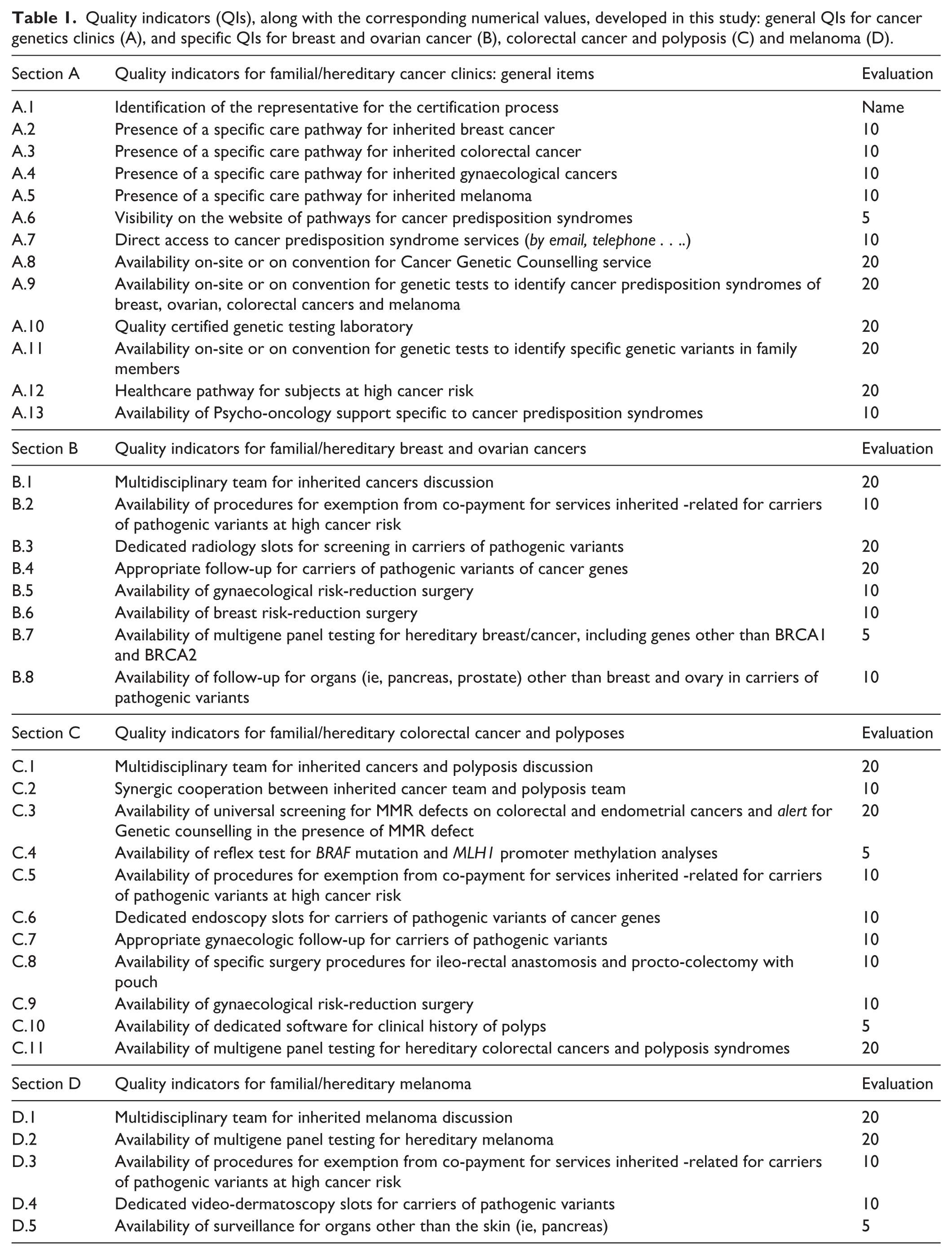
A total of 37 benchmark QIs that could be adopted by Italian hereditary cancer services were identified. Table 1 shows the general QIs (A) and the syndrome-specific QIs for breast and ovarian cancer (B), colorectal cancers and polyposis (C), and melanoma (D), along with the assigned values.
Quality indicators (QIs), along with the corresponding numerical values, developed in this study: general QIs for cancer genetics clinics (A), and specific QIs for breast and ovarian cancer (B), colorectal cancer and polyposis (C) and melanoma (D).
All Italian centers affiliated with AIFET were included in the survey through a questionnaire requiring adherence to the identified indicator. Twenty-two centers (Figure 1) submitted the completed questionnaire along with a self-declaration from the applicant. These included academic institutions, cancer care and research centres (IRCCS, Istituti di Ricovero e Cura a Carattere Scientifico), and hospitals organized within the Hub-and-Spoke model. The 37 indicators and their corresponding scores, as defined by the AIFET Committee, are listed in Table 1. Thirty-one indicators related to the identification and management of patients and their relatives affected by hereditary cancer, while six indicators focused on aspects such as exemption from co-payment (“ticket”) and access to clinical cancer genetic services (Figure 2).

Geographical location of the 22 centers participating in the survey.
Definition of “ticket” within Italian National Health system (SSN).
Among syndrome-specific indicators, eight referred to HBOC (ORPHA 145), 11 to inherited colorectal cancers and polyposis (ORPHA 144, 733, 247798), and five to familial melanoma (ORPHA 618). For each QI, the degree of implementation of specific activities was linked to assigned scores. The sum of these scores generated a final value indicative of the quality of cancer genetic services, including diagnosis, treatment, and follow-up for both affected individuals and their healthy relatives.
The survey was conducted as a self-assessment exercise (each center evaluating itself). No external verification was performed, and the results were analyzed anonymously.
Figure 3 illustrates the national survey results. These reveal a stronger focus on breast cancer predisposition syndromes, and comparatively less attention to familial melanoma (see QIs A2, A3, A4, A5). We found that multidisciplinary disease-related groups, where care strategies for patients are discussed, are quite widespread (95%, 72%, 41% for QIs B1, C1, and D1, respectively). However, this activity was not consistently associated with the existence of specific care pathways for the three familial cancer categories (77%, 50%, 54%, 32% for QIs A2, A3, A4, A5). This finding highlights the limited advocacy among Italian healthcare providers in making hereditary pathways visible and accessible (QIs A2–A5; A11, A12), likely reflecting difficulties in managing these patients—especially unaffected relatives—outside the immediate cancer treatment pathway (QIs B3, C6, D4).
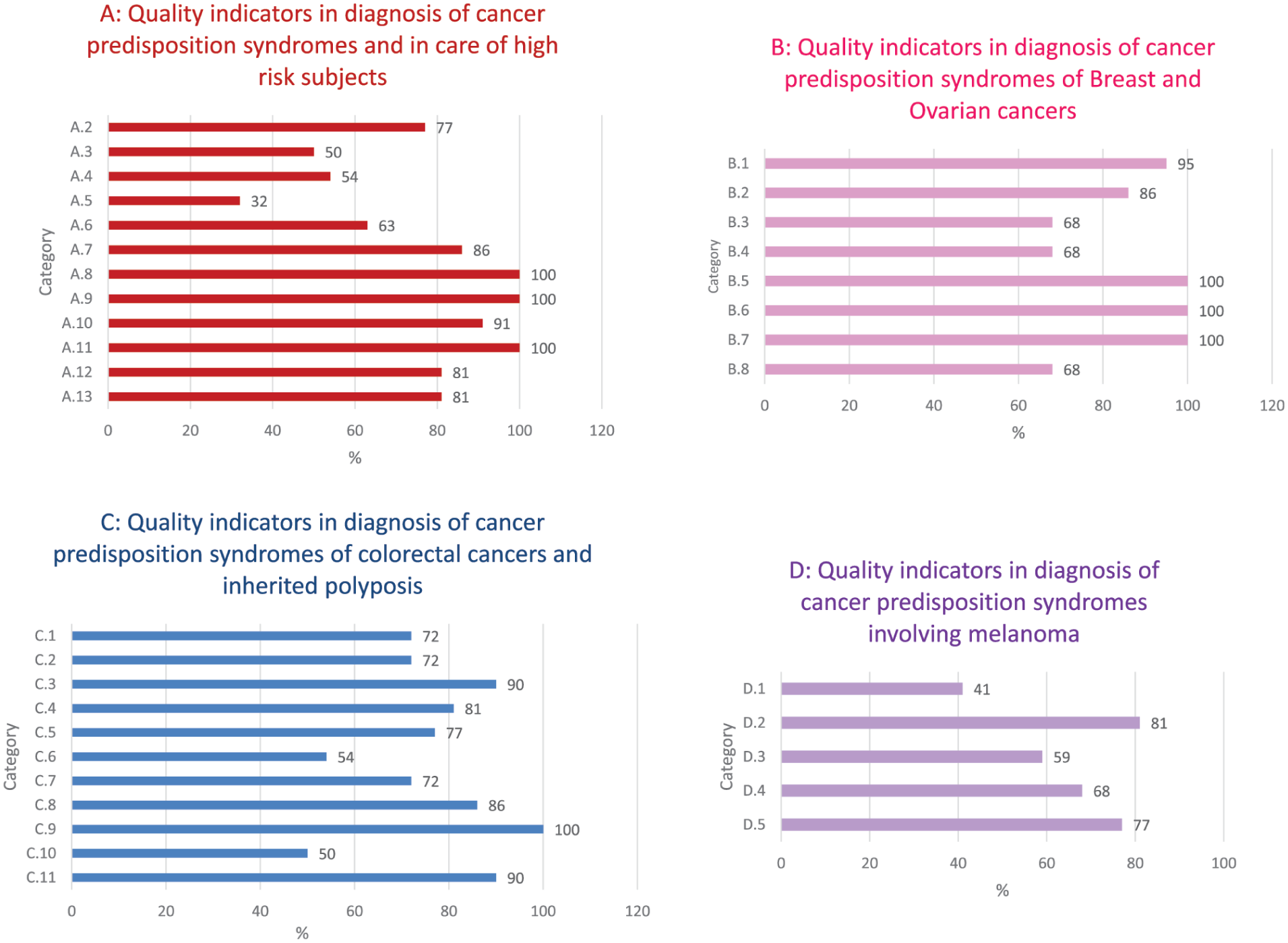
Results of the survey on the 37 QIs shown in Table 1 across national hereditary cancer centers.
Nevertheless, prophylactic surgery was available in all centers (100%; QIs B5, B6, C9), regardless of the type or level of the institution.
The availability of genetic testing was also very high (100%; QI A11), suggesting particular attention is paid to the diagnosis of inherited cancers. Multigene panel tests were widely used for all cancer types considered, although they were slightly less common for familial melanoma (QI B7, C11, D2: 100%, 90%, and 81%, respectively).
Interestingly, Universal Screening for MMR defects 10 was more frequently available than reflex testing for BRAF mutations and MLH1 hypermethylation (90% vs 81%, QIs C3 and C4). This gap indicates that in some cases the hereditary diagnostic pathway remains incomplete, as MMR deficiency (MLH1/PMS2 loss) requires reflex testing (C4) to exclude sporadic carcinoma. This finding underlines the need for a new indicator to capture the rate of incomplete Lynch syndrome screening. As with other screening programs (e.g., breast cancer), detection rates are proportional to patient adherence; incomplete pathways decrease the identification rate of Lynch syndrome.
The survey also revealed limited availability of dedicated software for evaluating polyp history (QI C10; 50%) and, notably, underutilization of pathology department software that could track cumulative polyp counts (>10), which is essential for polyposis identification.
Care pathways for high-risk individuals were present in 81% of centers (QI A12). Risk-reducing surgery was available for breast and ovarian cancer in most centers, and to a lesser extent for colorectal cancer (QIs B5, B6, C8, C9). Psychological support was available in 81% of centers (QI A13). However, dedicated clinical appointment slots were available in only 54–68% of centers, depending on the cancer type and procedure (QIs B3, C6, D4).
Regarding patient accessibility to specialized centers and exemption from co-payments for genetic services, these features were consistently present across AIFET centers—an expected finding given their institutional role.
In 2024, the AIFET Steering Committee analyzed the data from the 21 centers and calculated overall scores. The mean institutional score was 362.0, ranging from 130 to 460.
Conclusions
This AIFET initiative represents the first national effort to define quality indicators (QIs) for hereditary cancer services in Italy. The proposed QIs provide a practical framework to assess and improve diagnostic and care pathways, ensuring that genetic testing, surveillance, and risk-reducing strategies are systematically implemented. By promoting consistency across centers, this model may not only enhance the quality of care nationally but also foster collaboration with European institutions toward shared standards in hereditary cancer management.
Footnotes
Members of Associazione Italiana Familiarità ed Ereditarietà Tumori (AIFET) partecipating at this survey
Genuardi M., Grillo F., Ghiorzo P., Peccatori F., Urso EDL., Puccini A., Panfili A., Turchetti D., Caligo F., Terribile D., Vitellaro M., Lucci-Cordisco E., Roncucci L., Ghiorzo P., Barana D., Romeo S., Mammi I., Adami F., Viel A., Rizzo A., Zampiga V., Cavestro M., Bonanni B., Sessa F., Russo A., Greco F., Morabito A., Stigliano V., Zovato S. Giacchè M., D’Angelo V.
Contributions
A.R. and M.G.T. conceptualized, wrote, reviewed and edited the manuscript.
G.B.R., I.C. and C.O. wrote and reviewed the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.