
Abstract
For decades, the surgical management of non-small cell lung cancer (NSCLC) has been predominantly guided by anatomical staging. However, this traditional approach often overlooks the “fourth dimension” of cancer biology: time. This narrative review explores how circadian and circannual rhythms act as silent drivers of oncological prognosis, deeply influencing the interaction between host immunity and tumor behavior. Evidence suggests that the integrity of the molecular clock, regulated by genes such as TIMELESS and RORA, is not merely a biochemical detail but a critical determinant of survival and metastatic potential. Furthermore, environmental cues like Vitamin D synthesis and photoperiodism introduce seasonal fluctuations in patient resilience, creating specific “windows of vulnerability” during surgical stress. Moving toward a “time-aware” oncology opens the possibility of synchronizing clinical interventions—from the hour/season of surgery to immunotherapy scheduling—with the patient’s biological rhythms. Such an approach represents a promising, cost-effective frontier to further personalize the therapeutic journey and optimize long-term outcomes in resectable NSCLC
Introduction
For decades, surgical management of non-small cell lung cancer (NSCLC) has been guided by a spatial–anatomical–paradigm, the TNM staging system, which assesses tumor size, nodal involvement, and metastatic spread, and still remains the gold standard for prognostic stratification. 1 However, this static approach neglects the “fourth dimension” of cancer biology: time. Evolution, under the influence of day-night cycles, has resulted in the development of highly conserved internal “oscillators” known as circadian clocks.2,3 These rhythms regulate nearly all physiological processes, including metabolic flux, DNA repair, and immune cell trafficking.2,4 In oncology, disruption of these rhythms, termed chronodisruption, is now recognized as a fundamental driver of malignant transformation and therapeutic resistance, rather than a secondary consequence of systemic illness.4,5
Resectable NSCLC presents a clinical context in which the timing of host-tumor interactions is critical. Surgical resection triggers a substantial neuroendocrine and inflammatory stress response. 6 Recent epidemiological studies have identified an association between the season of surgery and long-term survival outcomes.7,8 This observed seasonality is unlikely to be attributable solely to a statistical artifact. Instead, it may reflect fluctuations in the patient’s biological state, influenced by photoperiod and Vitamin D synthesis. 9 In certain cohorts, differences in mortality hazard ratios of up to 20–25% have been reported across seasonal windows of intervention.7,9
Within this seasonal context, the host's systemic fitness at the time of surgery is a key determinant of oncological outcomes. Markers from routine blood tests (RBT), such as C-reactive protein (CRP), serve as important surrogates for the patient's immune-inflammatory set-point. 10 An elevated perioperative inflammatory state indicates a compromised biological environment, which may impair immunosurveillance and promote early recurrence. 6 Elucidating the interaction between internal inflammatory markers and external temporal cues is essential for developing a comprehensive, multi-dimensional prognostic model.
This narrative review explores available evidence linking chronobiological factors to clinical outcomes in NSCLC, with particular attention to the role of circadian clock genes and to seasonal patterns. By reporting discordant evidence from different latitudes, we seek to highlight that the calendar serves as a biological surrogate for a complex network of temporal drivers that may be integrated into modern precision oncology.
Methods
This narrative review draws on a structured, non-systematic search on PubMed, Scopus, and Web of Science for literature published between 1995 and December 2025. Search terms included “circadian rhythm,” “seasonality,” “lung cancer,” “immunotherapy,” “perioperative inflammation,” and “clock genes.” Priority was given to peer-reviewed English-language original studies, meta-analyses, and authoritative reviews on thoracic oncology. Study selection was guided by relevance to the review topic, methodological robustness, and conceptual alignment with the scope of the manuscript. No formal risk-of-bias assessment was performed.
We included original research articles, large-scale retrospective cohort studies, and seminal reviews that offered mechanistic insights into the temporal regulation of NSCLC. This review integrates three different issues: (1) molecular data on circadian gene expression and prognostic value in lung tissue; (2) clinico-epidemiological data on seasonal survival fluctuations after curative-intent surgery; and (3) chrono-immunological evidence on the rhythmic nature of the tumor microenvironment and systemic inflammation. The numerical sequence of references reflects the integration of multidisciplinary sources to construct a cohesive argument for time-aware management of NSCLC patients.
The molecular clockwork in lung cancer
The biological orchestration of the cell cycle, DNA repair, and apoptosis is governed by a sophisticated hierarchical network of genes known as the core clockmachinery. In healthy pulmonary tissue, these oscillators maintain homeostasis. On the contrary, in NSCLC, this machinery is frequently hijacked or silenced, leading to a state of internal temporal chaos. 11 The fundamental molecular oscillator consists of an autoregulatory transcription-translation feedback loop. At its core, the heterodimer complex formed by CLOCK and BMAL1 (ARNTL) binds to E-box promoter elements to drive the expression of Period (PER1, PER2, PER3) and Cryptochrome (CRY1, CRY2) genes. Once translated, PER and CRY proteins translocate back into the nucleus to inhibit the activity of CLOCK-BMAL1, completing a cycle of approximately 24 hours.11,12
A crucial second loop involves the nuclear receptors RORA (RAR-related orphan receptor A) and REV-ERBα, which compete for binding sites on the BMAL1 promoter. RORA acts as a positive regulator and has recently emerged as a significant tumor suppressor in lung adenocarcinoma. 13 Compared to adjacent normal mucosa, data indicate that RORA expression is frequently downregulated in NSCLC tissues. Some authors have reported that patients with high RORA expression levels exhibit significantly improved overall survival (OS) and disease-free survival (DFS), as this gene suppresses tumor cell proliferation and invasion by modulating the epithelial-mesenchymal transition (EMT). 13
Conversely, the overexpression of TIMELESS, a gene originally identified for its role in circadian rhythm and DNA replication fork stabilization, is associated with a poor prognosis.13,14 TIMELESS appears to function as a pro-tumorigenic factor in NSCLC; its upregulation is correlated with advanced TNM stages, larger tumor sizes, and a higher propensity for lymph node metastasis. In clinical cohorts, TIMELESS expression has been associated with increased mortality, making it a robust, independent prognostic biomarker. 14
The relationship between the tumor and the host's systemic rhythms is further complicated by “humoral chronodisruption.” Recent evidence suggests that adenocarcinoma cells do not merely possess a broken clock but can actively desynchronize the host's peripheral rhythms. Serum factors from NSCLC patients, particularly those with advanced adenocarcinoma, contain pro-inflammatory cytokines and metabolic byproducts that alter the rhythmic expression of clock genes in distal healthy cells. 15 This systemic disruption of circadian signaling has been associated with cancer-associated fatigue as well as metabolic derangements observed in advanced disease. Furthermore, the molecular clock intersects with key oncogenic pathways. For instance, p53, the “guardian of the genome,” is both a regulator and a target of the circadian machinery.12,16 Similarly, the c-MYC oncogene is directly repressed by the CLOCK-BMAL1 complex; thus, when the circadian clock is disrupted in NSCLC, c-MYC becomes constitutively active, driving uncontrolled cellular growth and metabolic reprogramming toward glycolysis (the Warburg effect) (Table 1).12,14,16
Core clock genes and their prognostic significance in NSCLC.
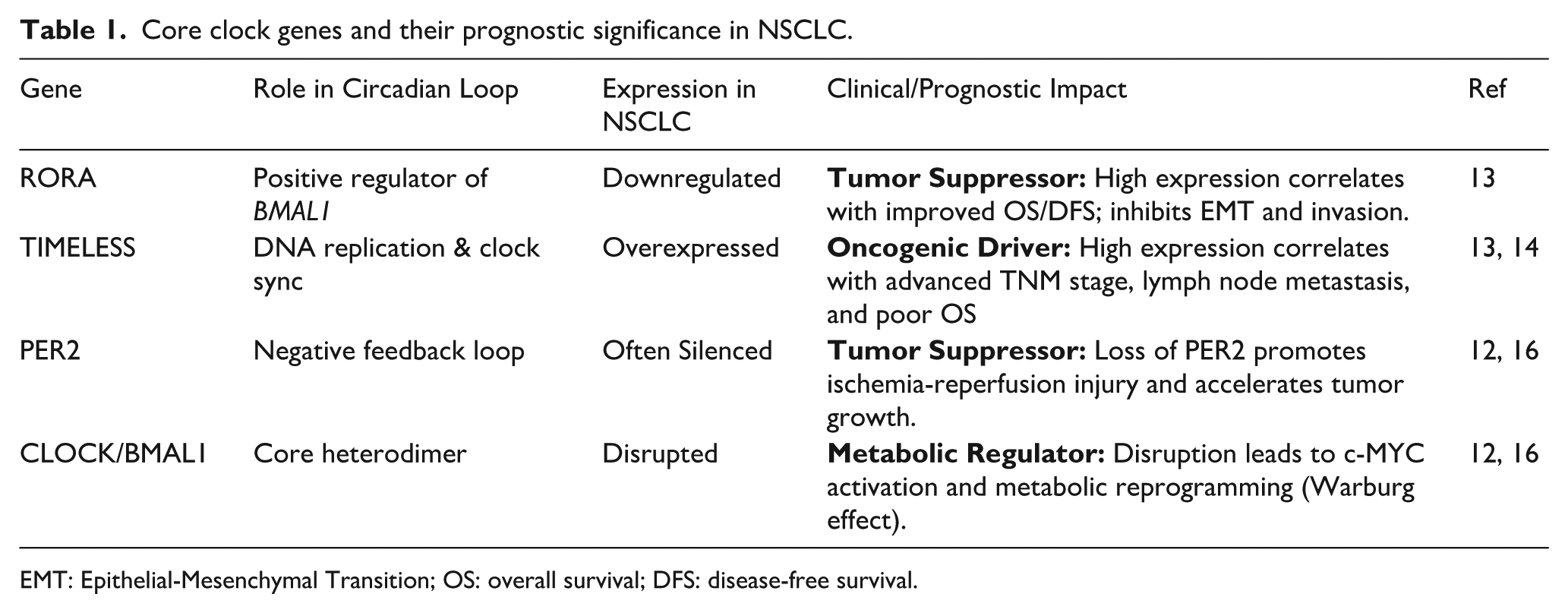
EMT: Epithelial-Mesenchymal Transition; OS: overall survival; DFS: disease-free survival.
Immunity’s fourth dimension and the seasonal environment
The “host resistance” to cancer is related to the temporal organization of the immune system. The immune landscape is no longer considered a static shield, as it undergoes strong oscillations across both circadian and circannual scales. In the context of NSCLC, these rhythms dictate the patient's “immunosurveillance fitness” during surgical stress.
Seasonal vulnerability and the Lewis lung model
The impact of seasonality on NSCLC progression has been demonstrated in prior experimental oncology studies. Specifically, studies on Lewis lung carcinoma model have revealed a significant circannual rhythm in metastatic potential.5,15,16 The formation of pulmonary metastases exhibits a clear acrophase, or peak activity, coinciding with the summer solstice. While derived from experimental models, these findings are conceptually consistent with clinical observations suggesting a period of increased biological vulnerability during the warmer months. 16
This “seasonal window” of aggressiveness may be closely associated with fluctuations in immune cell populations. In fact, some experimental data have reported that T-cell subsets (specifically CD3+ and CD4+ lymphocytes) undergo a dramatic reduction during the spring-summer period. 17 Conversely, a significant increase in CD3+ populations is observed during the winter months. This seasonal effect on CD4 (and inversion of the CD4/CD8 ratio) suggests a state of “relative immunodeficiency” during the summer. 17 These observations suggest that immune competence may vary across the year, potentially contributing to temporal heterogeneity in host–tumor interactions.
Immune cell trafficking and the pulmonary microenvironment
On a circadian scale, leukocyte trafficking between the bone marrow, blood, and peripheral tissues is regulated by the rhythmic expression of adhesion molecules and chemokines.2,18-20 The cytolytic activity of Natural Killer (NK) cells and the proliferative response of T-lymphocytes follow a precise 24-hour cycle, modulated by the autonomic nervous system and glucocorticoid signaling.2,17 In the lung, which serves as a major reservoir for marginated granulocytes and lymphocytes, the timing of surgery may coincide with either a “pro-inflammatory” or “immunosuppressive” phase of this cycle, a balance further modulated by seasonal and environmental factors that influence systemic immune tone.21,22 Chronic chronodisruption leads to a “flat” immune rhythm, characterized by diminished NK cell infiltration and an accumulation of myeloid-derived suppressor cells (MDSCs) within the tumor microenvironment.5,23
The sun-Vitamin D-VDR axis
The most potent environmental Zeitgeber (time-giver) for circannual rhythms is solar radiation, which governs the systemic levels of Vitamin D. Beyond its role in bone homeostasis, 25-hydroxyvitamin D [25(OH)D] acts as a critical immunomodulator in NSCLC.9,18,19,24 The Vitamin D receptor (VDR) is widely expressed in both bronchial epithelial cells and tumor-infiltrating lymphocytes. This evidence suggests a possible bridge between the environment and the tumor microenvironment. In the literature, some authors reported that patients with higher circulating Vitamin D levels before surgery had significantly improved recurrence-free survival (RFS), with a reduction in recurrence risk of approximately 18-20% compared with deficient cohorts.9,18,19,21
This protective effect is further modulated by genetic polymorphisms in the VDR gene, such as the FokI and BsmI variants, which can either enhance or impair anti-proliferative signaling.18,19 Furthermore, the “Lag-Phase” theory suggests that the peak in Vitamin D synthesis during late summer may provide a protective immunological “buffer,” manifesting as improved outcomes for patients treated in the subsequent autumn months.9,21,25
The seasonal paradox: Reconciling discordant evidence
The impact of seasonality on NSCLC prognosis presents a fascinating geographical dichotomy. While the existence of a “seasonal prognostic window” is widely accepted, the specific months associated with optimal survival vary significantly across different latitudes, creating what researchers define as a seasonal paradox.
The northern latitude model: The summer benefit
Data from high-latitude regions consistently point toward a survival advantage for patients undergoing surgery during the summer months.7,9 In these territories, extreme fluctuations in the solar photoperiod mean that the “biological summer” provides the only window of sufficient ultraviolet B (UVB) exposure for adequate Vitamin D synthesis.9,17 Some authors thought this oscillation in 25(OH)D levels during June and July may prime the immune system, enhancing the anti-tumor response at the critical moment of surgical tumor shedding.2,19 Furthermore, in these cold climates, the summer season represents a period of minimal thermal stress, favoring homeostatic stability and reducing perioperative complication rates.8,21
The Mediterranean perspective: Heat stress and autumnal advantage
On the contrary, other evidence from Mediterranean and southern regions suggests a different trend, reporting a survival peak in autumn or winter. 22 This discrepancy can be explained through the lens of environmental stress and chronodisruption. In southern countries, summer is often characterized by extreme heat, which can cause physiological stress.22,24,26 As a result, high temperatures have been shown to disrupt the circadian rhythm of core body temperature, which serves as a fundamental coordinator of systemic rhythms.4,5
As previously noted, the stability of these internal oscillators is a prerequisite for favorable host recovery.5,26 In these contexts, the excessive thermal load of summer may act as a “pro-inflammatory” stimulus, counteracting the benefits of solar exposure and potentially leading to the relative immunodeficiency observed in experimental models during the warmer months.15,17,27
The lag-phase and the “biological buffer”
To reconcile these findings, the “Lag-Phase” hypothesis suggests that the prognostic benefit of a season is not instantaneous but delayed. The cumulative effect of summer solar radiation on the immune system may reach its peak efficacy several weeks or months later. 9 This suggests that the high Vitamin D levels synthesized in summer could provide a protective “biological buffer” for patients treated in subsequent months.19,25 Ultimately, the “optimal month” for NSCLC surgery is context-dependent, representing the point of intersection between maximum “positive drivers” (solar exposure, Vitamin D reserves) against minimum negative stressors (heat stress, healthcare delays).22,27
Chronotherapy and clinical management: Optimizing the surgical and adjuvant window
The circadian timing of surgery: Morning vs. afternoon outcomes
The “time-of-day” effect in thoracic surgery is an emerging field of investigation. Retrospective analyses have suggested that the timing of pulmonary resection or radiotherapy can influence immediate post-operative outcomes and long-term survival.28,29 Some authors postulated that patients undergoing elective surgery in the afternoon/night may experience a higher incidence of postop complication rates or mortality in specific cohorts.29,30 Mechanistically, this has been linked to the circadian variation in pulmonary compliance and the rhythmic activity of alveolar macrophages, which exhibit a peak in phagocytic and inflammatory capacity during the early morning hours in humans.2,31 Furthermore, anesthesia itself is a potent chronodisruptor; the interaction between volatile anesthetics and molecular clock genes (such as PER2) can either aggravate or mitigate ischemia-reperfusion injury during lung manipulation, depending on the circadian phase of the intervention.32,33
Lessons from chronomodulated systemic therapy
The pioneering work in this field has established that the efficacy and toxicity of pharmacological agents are not constant but fluctuate according to the patient's internal clock. 34 In lung cancer, chronomodulated chemotherapy—specifically the infusion of cisplatin or gemcitabine at specific circadian windows—has demonstrated a reduction in hematological toxicity by up to 30-40% compared to flat-rate infusions, while maintaining or even enhancing the objective response rate.35,36 These findings have profound implications for the adjuvant setting in resectable NSCLC. If the “host soil” is more resilient at certain hours, the administration of adjuvant chemotherapy or immunotherapy (checkpoint inhibitors) should be synchronized with the acrophase of immune cell infiltration.37,38 For instance, recent data on PD-L1 inhibitors suggest that infusions before 14:00 are associated with significantly better overall survival than late-afternoon infusions, a finding hypothesized to be related to circadian variation in T-cell activation.37,38
Seasonal vaccination and immunological priming
In this context, an interesting and debated issue is the timing of seasonal influenza vaccination, especially considering that chronodisruption can significantly impair host immune surveillance. 39 Beyond preventing respiratory infections, vaccination serves as an immunological “boost” that can modulate the host's systemic inflammation. Studies have shown that flu vaccination in cancer patients is not only safe but may provide an unintended survival benefit through a process of “trained immunity”.40,41 In resectable patients, administering the vaccine in the weeks preceding surgery (during the autumn months) may prime the innate immune system, potentially reducing the risk of post-operative pneumonia and altering (or improving) the inflammatory response to surgical stress.41,42
Towards a “time-aware” oncology
The evidence reported in this review underscores a new paradigm shift: the prognosis of resectable NSCLC is not determined solely by the anatomical extent of the disease and the type of medical therapy, but can also be modulated by the temporal coordination between host and tumor biology (Figure 1). As we have explored, the “when” of surgery emerges as a potentially relevant biological variable alongside the “where” and the “how”.1,3,7,8 However, translating these chronobiological insights into routine clinical practice requires a critical appraisal of the current literature and the resolution of several methodological challenges (Table 2).4,43
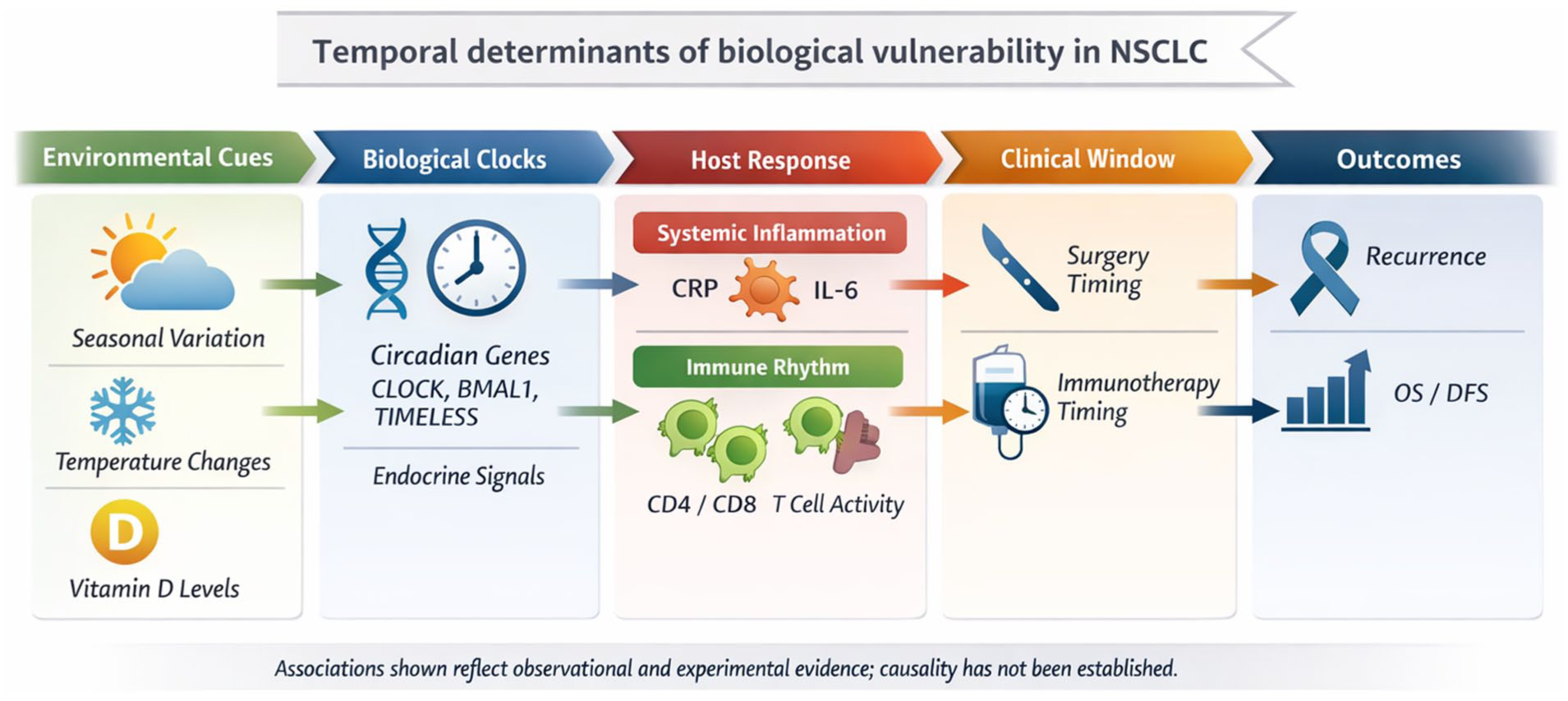
Integrative model of temporal determinants in NSCLC.
Multilevel evidence supporting temporal modulation of outcomes in NSCLC.
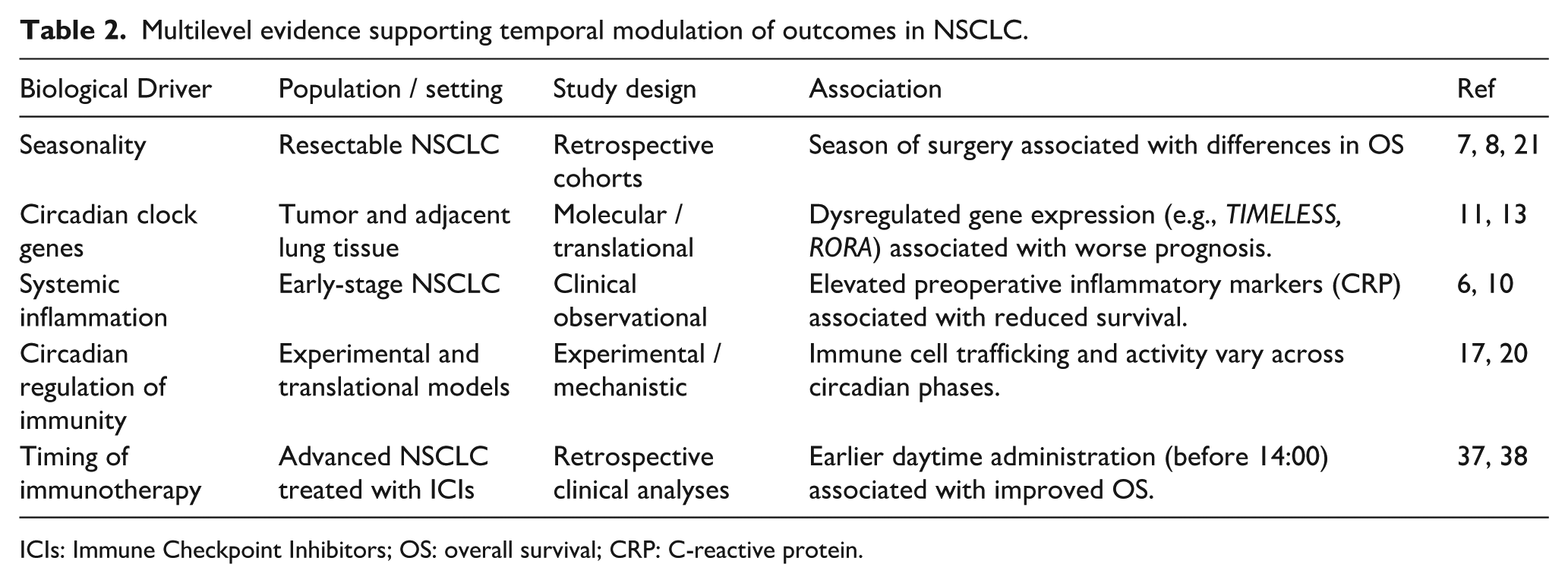
ICIs: Immune Checkpoint Inhibitors; OS: overall survival; CRP: C-reactive protein.
Critical analysis and current limitations
A significant bias for the adoption of specific chronobiological models stems from the heterogeneity of existing data. Specifically, most studies on seasonality in NSCLC analyzed retrospective registry data that often lack standardization for key confounding variables. 22 For instance, while Vitamin D levels are frequently cited as a primary driver of the “seasonal window,” few surgical cohorts include prospective, longitudinal measurements of 25(OH)D or VDR polymorphisms.18,19,44
The molecular characterization of the “tumor clock” also faces challenges. Although the prognostic value of TIMELESS and RORA has been validated in large datasets, their clinical application is hindered by the lack of standardized immunohistochemical assays that can be performed on surgical specimens cost-effectively.11,13,14,45 Moreover, the systemic impact of “humoral chronodisruption” means that the tumor’s clock cannot be viewed in isolation from the host's central oscillators.15,43
The chrono-surgical protocol: A speculative framework
Despite these limitations, the synthesis of these data points toward the necessity of a “time-aware” oncological framework. A proactive surgical strategy for NSCLC should move beyond the static “waiting list” approach. As proposed by the emerging evidence, a future Chrono-Surgical Protocol would involve a multi-dimensional assessment 46 :
Dynamic Pre-operative Stratification: Utilizing RBT and inflammatory markers (i.e., CRP) as indicators of the patient's systemic “immune-inflammatory set-point”.6,10 Identifying patients with a “flat” or disrupted rhythm through these surrogates could allow for pre-operative “chrono-rehabilitation” to restore circadian amplitude before the surgical hit.46,47
Chronobiological Scheduling: Prioritizing complex resections for the morning hours to align with the peak of pulmonary compliance and immune resilience.29,30 This scheduling must also account for the individual's chronotype to minimize the “circadian misalignment” induced by early-morning hospital routines. 48
Adjuvant Synchronization: Transitioning from fixed-rate adjuvant chemotherapy to chronomodulated delivery systems to maximize the therapeutic index and minimize toxicity.36,49
Chronotherapeutic Stabilization: In this framework, as reported in studies on the implementation of Vitamin D in NSCLC patients, 18 the adjuvant use of melatonin emerges as a pivotal strategy to counteract perioperative chronodisruption. By acting as a systemic “zeitgeber”, melatonin supplementation may not only improve sleep-wake cycles but also directly inhibit tumor cell proliferation and DNA repair mechanisms, potentially serving as a non-toxic bridge to stabilize the molecular clock following surgical stress. 50
Conclusions
The concept “beyond the calendar” suggests that the date of a surgical intervention is not merely an administrative detail but a biological marker of a complex internal state. In resectable NSCLC, the association of molecular clock genes (CLOCK/BMAL1,TIMELESS, RORA), seasonal environmental cues (Vitamin D, photoperiod), and host immune fitness can interact with the success of curative-intent surgery. Additionally, by acknowledging and harnessing these chronobiological drivers, thoracic oncology can overcome the inherent limitations of the TNM anatomical paradigm. In the near future, chronotherapy may become a further central pillar for precision medicine in early-stage NSCLC. The concept of a “temporal window” for both surgery and adjuvant therapy may be employed to offer a non-invasive, cost-effective strategy to improve survival. In this scenario, preop administration of a systemic zeitgeber (e.g., melatonin) to counteract peri and postoperative chronodisruption, along with a deeper understanding of VDR gene polymorphisms, may represent a promising strategy for preventing NSCLC relapse and personalizing the oncological journey.
Footnotes
Author contributions
Conception and design: GL.
Collection and assembly of data: All authors.
Interpretation: All authors.
Manuscript writing: All authors.
Final approval of manuscript: All authors.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GLR declares Advisory boards, consultancies, travel accommodations, speaker fees, writing fees, pi role in profit trials: MSD, Regeneron, Roche, Lilly, BMS, Amgen, AstraZeneca, Johnson And Johnson, Merck, Novartis, Pierre Fabre, Bayer, Beigene, Pfizer, Takeda, GSK, Daiichi, Sanofi, Gilead. CP declares Advisory boards, consultancies, travel accommodations, speaker fees, writing fees, pi role in profit trials: Pfizer, Roche, AstraZeneca, Daiichi Sankyo, MSD, Spectrum Pharmaceuticals, Janssen, Lilly, BMSI. AP declares Advisory boards, consultancies, travel accommodations, speaker fees, writing fees, pi role in profit trials: Janssen, Bayer, MSD, Lilly, BMS, AstraZeneca. All other authors have nothing to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.