
Abstract
Feline fibrocystic hepatobiliary lesions (FHLs) and extrahepatic biliary malformations (EBMs) are supposedly common, but prevalence studies and detailed gross and histologic descriptions within a large cohort are lacking. Our aims were to identify the prevalence of FHLs and EBMs within a large feline population, characterize gross and histologic features, and report comorbidities. Of 140 cats, 20 (14.3%) had either FHLs and/or EBMs. FHLs were most common (15/20, 75%) and included cystic biliary lesions (CBLs, 14/20, 70%) and congenital hepatic fibrosis (CHF, 1/20, 5%). CBLs had gross variability but histologically comprised multiloculated cysts lined by biliary epithelium overlying variably hyalinized collagenous trabeculae. Gross features of CHF included severe hepatic fibrosis with embedded biliary cysts, parenchymal collapse, and nodular regeneration. Histologically, there was loss of lobular architecture, proliferation of small irregular to cystic bile ducts, bridging fibrosis, inapparent portal veins, and scattered hepatocellular necrosis. Gallbladder malformations were present in 5/20 cats (25%) and were classified as duplex (2/5) or bilobed (3/5). Two of 20 cats (10%) had anomalous, blind-ended, extrahepatic bile ducts extending from the gallbladder into the pancreas/peripancreatic mesentery. FHLs and EBMs were rarely concurrent (1/20 cats, 5%). CHF contributed to significant morbidity, but other FHLs/EBMs were incidental. Concurrent pancreatic/renal cysts were uncommon (2/20, 10%) and were seen in association with a CBL and CHF. Common comorbidities included cardiovascular and/or renal disease and neoplasia. We provide evidence that the majority of feline FHLs represent ductal plate malformations, with CBLs having morphologic features compatible with von Meyenburg complexes (VMCs)/biliary hamartomas.
Fibrocystic hepatobiliary lesions (FHLs) and extrahepatic biliary malformations (EBMs) are anecdotally considered relatively common in cats compared with other species.12,28 The majority of FHLs are classified as ductal plate malformations (DPMs). DPMs are congenital biliary tree malformations that arise secondary to aberrant development of the embryonic ductal plate, the precursor tissue of intrahepatic bile ducts. DPMs can affect different segments of the intrahepatic biliary tree, resulting in a variety of malformations that have been reported across several species, including cats.3,8,18,26,30,34,53,58,59 In animals, DPMs can be grouped in 3 descriptive/morphologic categories that have been adapted from human terminology: (1) adult-type polycystic liver disease (PCLD; in humans, often but not always associated with autosomal dominant polycystic kidney disease [PKD]), (2) juvenile-type PCLD (in humans, often associated with autosomal recessive PKD), and (3) congenital dilation of hepatic and large intrahepatic bile ducts (resembling Caroli disease, as described in humans).12,49 Several variants on this terminology are presented and often confused across different literature sources and when comparing the lesions in humans vs animals; for consistency, the proposed veterinary-specific terminology above will be utilized throughout this article.
Subtypes of DPMs reported in cats include congenital hepatic fibrosis (CHF), von Meyenburg complexes (VMCs)/biliary hamartomas, PCLD, and Caroli disease.10,12,19,49,59 CHF is classified as a juvenile-type PCLD, and in cats is characterized by portal-portal bridging fibrosis accompanied by proliferation of irregular, often dilated bile ducts.5,49 Adult-type PCLD encompass a spectrum of lesions that includes PCLD and VMCs. While specific diseases within this group with identified genetic phenotypes and inheritance patterns have been defined in humans, in cats, these terms have often been used interchangeably in the literature, resulting in confusion in lesion and/or disease definition. PCLD is defined by the presence of multiple (in humans, > 20), unilocular or multilocular, noncommunicating cysts that are 1 mm to 12 cm in diameter, lined by biliary epithelium, and contain clear colorless fluid.49,60 In humans, PCLD is described as having “scanty” supportive connective tissue, unless there are concurrent VMCs. 31 VMCs consist of discrete, often periportal and subcapsular foci comprised variably hyalinized fibrotic stroma with admixed irregular bile ducts.5,33,49 VMCs are most often reported as “small” (reported size ranges in humans of 0.5–1 cm in diameter),31,42 but in both animals and humans can have progressive, gradual dilation over years that results in larger cyst formation.5,31,32,49 In both humans and cats, adult-type PCLD and juvenile-type PCLD manifestations are often reported in conjunction with PKD.5,47,49,60 In humans, further identification of genetic mutations and inheritance patterns in conjunction with these lesions defines specific diseases such as autosomal dominant PKD, autosomal recessive PKD, and isolated/autosomal dominant PCLD. 25 However, this depth of genetic evaluation has not been performed for similar lesions in cats; to date, only PKD1 mutations have been associated with either adult or juvenile-type PCLD in cats.5,12,59 Congenital dilation of hepatic and large intrahepatic bile ducts (Caroli disease or Caroli-like disease) has been reported in a few cats and is characterized by dilation of medium to larger caliber intrahepatic ducts with variable extension and involvement of proximal extrahepatic ducts.10,17,34
In addition to DPMs, other FHLs described in cats include solitary biliary cysts and multiloculated biliary cystic masses, the latter of which have historically been referred to as biliary cystadenomas.1,28 These lesions are often incidental findings during postmortem examination of older cats.1,28 Currently, the true pathogenesis of these lesions and relationship to DPMs is unknown, although it is possible that a subset of biliary cystadenomas may represent VMCs that have undergone the aforementioned dilation or may have a different genetic predisposition other than that previously documented in cats (ie, PKD1 mutation).12,31,32,49 However, additional characterization of these lesions is required to build further support for this theory.
EBMs affect the extrahepatic biliary tree (cystic, hepatic, or common bile ducts) or the gallbladder. Malformations characterized by dilation and/or presence of diverticula of extrahepatic biliary ducts (primarily the common bile ducts) are known as choledochal cysts and have also been reported in cats.2,18,41,46 However, it is unclear if these lesions represent congenital dilations or changes secondary to alterations in bile flow.23,43,44,46,48,52 In addition, gallbladder malformations, variably termed accessory, bilobed, or duplex gallbladders, are historically the most commonly reported malformations in cats, with incidence rates ranging from 12% to 24%.7,28,45
Despite observations indicating that FHLs and EBMs are common in domestic cats,7,12,28,45 a study characterizing the prevalence and detailed features of these lesions in a large cohort of cats is lacking. In this study, our aim was to identify the prevalence of FHLs and EBMs in a cohort of cats presented for autopsy examination and describe the gross and histologic features of different subtypes of lesions. For FHLs, we hypothesized that these lesions represented DPMs and sought to compare observed histologic features with reported features of DPMs. Concurrently, we report comorbidities identified in cats.
Materials and Methods
Cats in this study presented for postmortem examination at North Carolina State University College of Veterinary Medicine between August 2017 and March 2020. Cats included in this cohort were those recruited for opportunistic and prospective sampling for inclusion in a separate study investigating histomorphology of the major duodenal papilla and feline “triaditis.” 39 Ethical approval was given for use of tissues for teaching and research for patients upon submission for autopsy. Gross and histologic reports of cats within this cohort were reviewed to identify cats with FHLs or EBMs for inclusion in the study. When available, gross images and/or histologic slides of lesions were additionally reviewed to further refine classification of lesions. Gross images were available for review for 13/22 identified lesions (6 FHLs and 7 EBMs), and histologic slides were available for review for 15/22 identified lesions (12 FHLs and 3 EBMs). Further details on gross appearance of lesions, including lesions for which gross images were not available, were summarized based on review of pathology reports. Autopsy reports, gross images, and histologic slides were also evaluated for identification of comorbidities in cats. All tissues examined histologically were fixed in 10% neutral-buffered formalin and were routinely trimmed, processed, and stained with hematoxylin and eosin for microscopic examination. All reports, images, and slides were evaluated by one pathologist (MES). Gross and/or histologic features of cases were further evaluated by a second pathologist (JMC) for confirmation of findings as warranted; 13/20 cases were dual-reviewed (Table 1). Data were collected from medical records for each cat, including signalment (age, sex, and breed) and significant findings from the postmortem examination (eg, significant lesions identified, cause of clinical decline, and other significant comorbidities). Cats were classified as kitten (birth to 1 year), young adult (1–6 years), mature adults (7–10 years), or senior (> 10 years) based on the 2021 American Animal Hospital Association/American Academy of Feline Practitioners Feline Life Stage Guidelines (https://www.aaha.org/).
Clinical information for cats with fibrocystic hepatobiliary lesions and extrahepatic biliary malformations.
Gross and/or histologic features were reviewed by both MES and JCM for 13/20 cats.
For 3 cats, cystic biliary lesions were not evaluated histologically, but given consistent gross features were presumptively classified as such.
For 2 cats, cystic biliary lesions were not identified grossly but were found incidentally on routine histologic liver evaluation.
Abbreviations: FS, female spayed; MC, male castrated; DSH, domestic short hair; DMH, domestic medium hair; DLH, domestic long hair; CNS, central nervous system; DCM, dilated cardiomyopathy; CBD, common bile duct; IMHA, immune-mediated hemolytic anemia.
Associations between numerical variables (ages of cats) were analyzed using a Mann-Whitney rank sum test (Statistics Kingdom, https://www.statskingdom.com/170median_mann_whitney.html).
Results
Case Demographics of Cats With Fibrocystic Hepatobiliary Lesions and Extrahepatic Biliary Malformations
Data from a total of 140 cats were reviewed. The average age across all 140 cats was 10.3 years old, and the cohort included 9 kittens, 30 young adults, 29 mature adults, 69 seniors, and 3 cats of unknown age. From this cohort, 20 cats (14.3%) had FHLs or EBMs (Table 1). Cats with FHLs or EBMs (mean, 13.7 years; median, 14 years; range, 1–21 years) were significantly older (P < .05) than cats without (mean, 9.7 years; median, 10 years; range, 1 month–20 years). Cats with FHLs or EBMs included domestic mixed breed cats (n = 17) and 1 Himalayan, Siamese, and ragdoll cat each. Among cats with FHLs or EBMs, castrated male cats (n = 13) were overrepresented compared with spayed female cats (n = 7).
Overview and Subtypes of Fibrocystic Hepatobiliary Lesions and Extrahepatic Biliary Malformations
Lesions were broadly classified into 3 categories: FHLs (ie, intrahepatic lesions), gallbladder malformations, and anomalous extrahepatic bile ducts. Two cats had 2 distinct types of lesions, while the remaining cats had a single lesion type, resulting in a total of 22 lesions identified (Table 1).
FHLs were identified in 15 cats and were the most common lesion identified on either gross or histologic examination. Of these cats, the majority (14/15, 93%) had FHLs classified grossly and/or histologically as a cystic biliary lesion (CBLs, Table 2), while 1 cat was diagnosed with CHF. Gallbladder malformations were the second most common biliary malformation identified (n = 5). Finally, 2 cats had anomalous, blind-ended, extrahepatic bile ducts extending from the gallbladder into the pancreas or surrounding mesentery.
Gross features of feline cystic biliary lesions (putative von Meyenburg complexes).
For 2 cats, cystic biliary lesions were not identified grossly but were found incidentally on routine histologic evaluation of the liver, and so gross features were not described and are marked as “N/A”
Abbreviations: CBL, cystic biliary lesion; FS, female spayed; MC, male castrated; DSH, domestic short hair; DMH, domestic medium hair; DLH, domestic long hair; L, left; R, right.
Gross and Histologic Features of Feline Fibrocystic Hepatobiliary Lesions
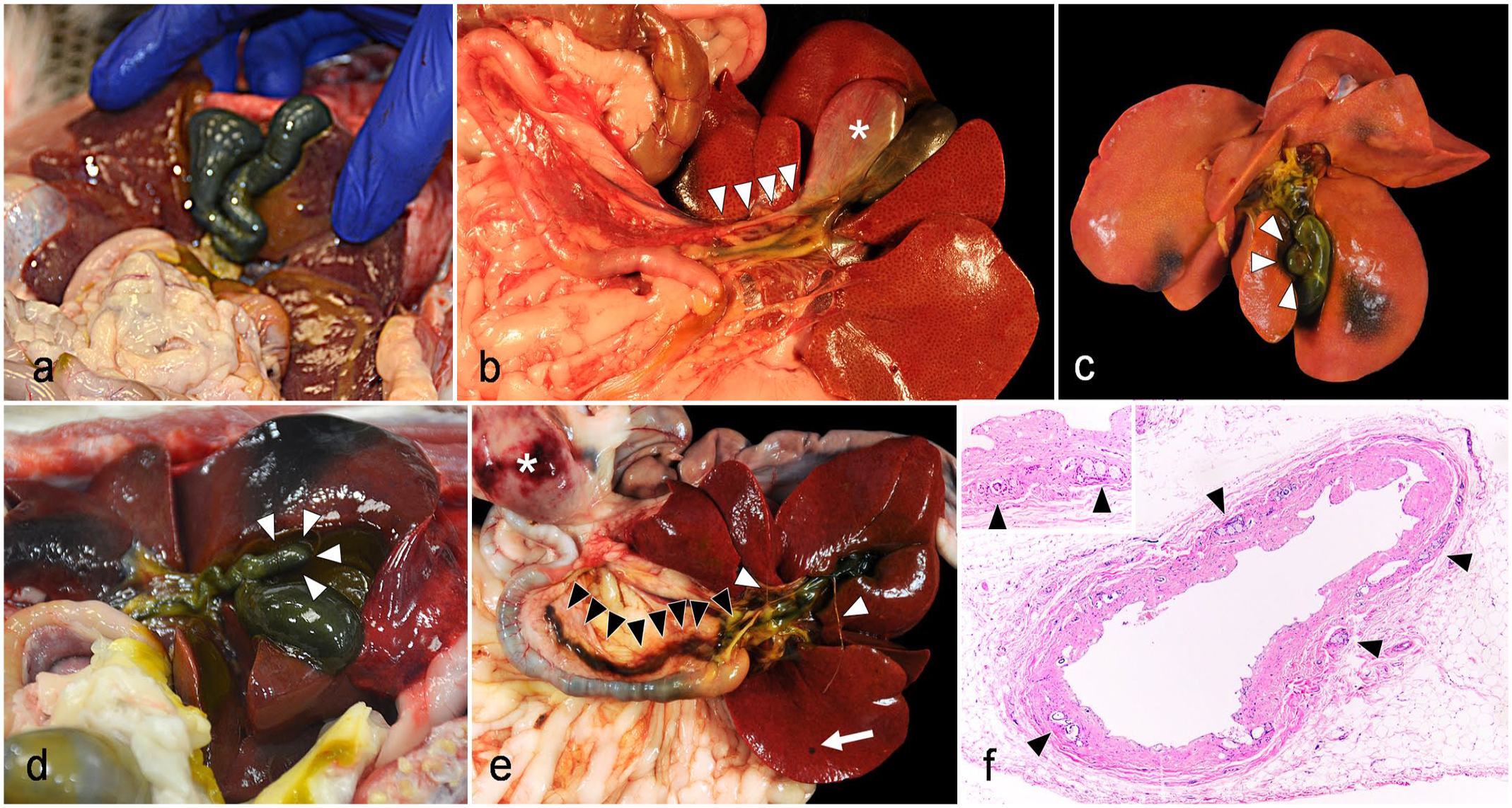
Gross descriptions were available for 12/14 cats with CBLs, while focal CBLs were identified incidentally in 2 cats on histologic examination of the liver. Of the 14 cats with CBLs, 7 had focal (single) CBLs and 7 had multifocal CBLs. The number of identified CBLs in each cat liver ranged from 1 to 10, and there was no apparent lobe predisposition, although the left lateral was the most frequently affected (5/14 cats). CBLs ranged in size from 1 mm to 3.5 × 3.0 × 4 cm in diameter. The majority of CBLs (11/14, 79%) were < 2 cm in diameter or grossly inapparent. Gross features of CBLs were highly variable (Table 2, Fig. 1). Most often, the lesions were described as flat or depressed, dark green to clear, cystic foci within the hepatic parenchyma (Fig. 1a–c), but larger CBLs tended to be described as multilocular (Fig. 1c) and raised nodules or masses (Fig. 1d). Regardless of their depressed, flat, or raised nature, they were frequently described as being thin-walled and containing watery, clear to green-tinged fluid. One CBL was grossly misdiagnosed as telangiectasia due to the presence of dark red, opaque fluid (blood) within the cystic space (case 10, Fig. 1e), and for 3 additional cats with CBLs, telangiectasia was either identified concurrent to CBLs (Fig. 1b, d) or listed as a clinical differential for CBL.
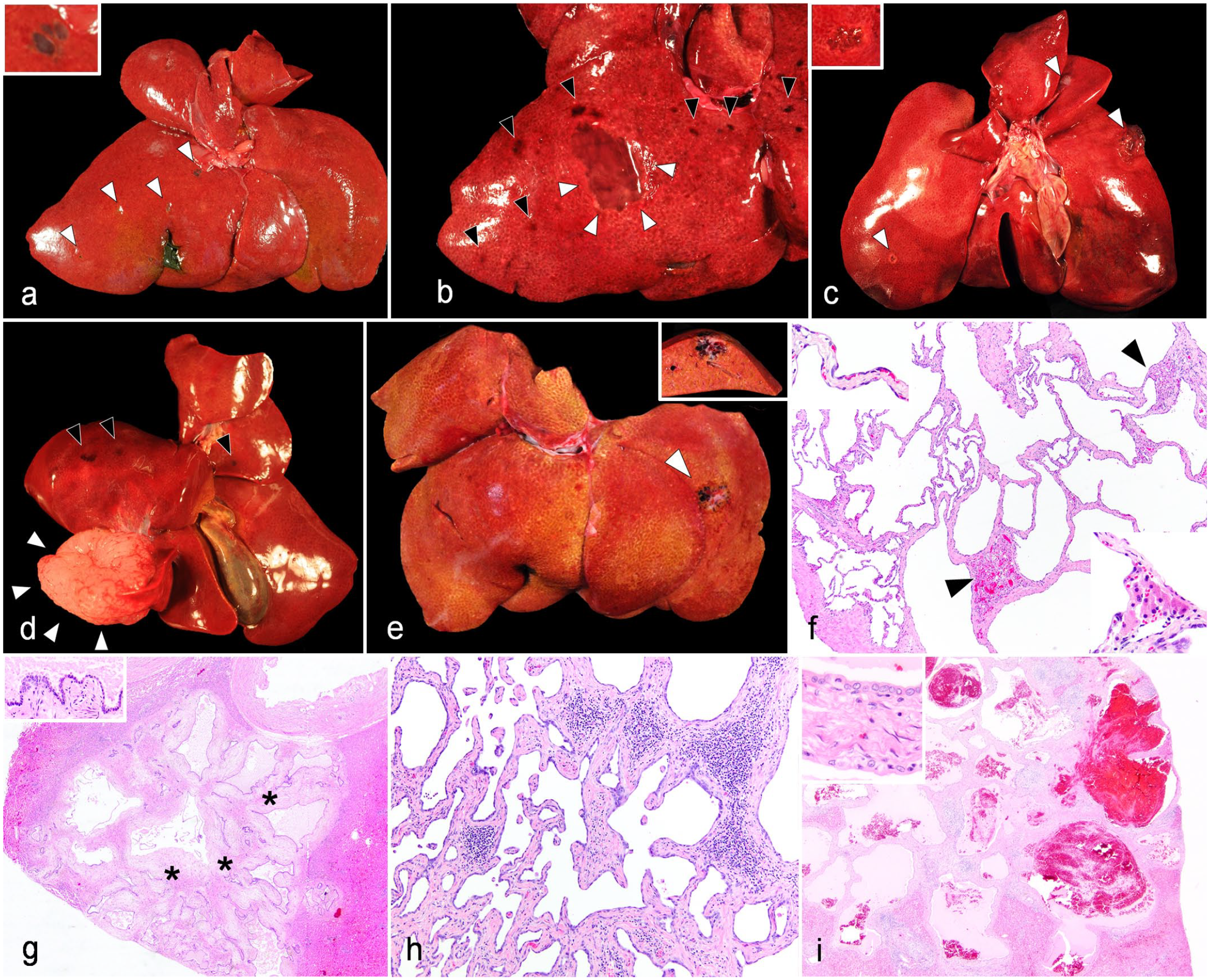
Gross and histologic features of cystic biliary lesions (CBLs) in cats. (a) Multifocal CBLs, liver, 10-year-old, spayed female domestic shorthair (DSH) cat. Case 2. Several small, flat-to-depressed, green cysts (arrowheads) are scattered throughout the liver. Inset: higher magnification of cyst. (b) Focal CBL, liver, 14-year-old, spayed female DSH cat. Case 8. Within the right medial lobe is a focal, flat to depressed, clear, cyst (white arrowheads). Note multifocal telangiectasia present elsewhere in the liver (black arrowheads). (c) Multifocal CBLs, liver, 8-year-old, spayed female DSH cat. Case 5. Three small to medium-sized, flat to raised, clear to white, multilocular cysts (white arrowheads) are scattered throughout the liver. Inset: higher magnification of an additional CBL. Photo courtesy of Amy Flis. (d) Focal CBL, liver, 18-year-old, castrated male Himalayan cat. Case 1. Arising from the left medial lobe is a focal, raised, white to pale pink, well-demarcated, multiloculated nodule comprised a myriad of cysts (white arrowheads). Smaller CBLs (not pictured) and foci of telangiectasia (black arrowheads) were present throughout the liver. (e) Focal CBL, liver, 12-year-old, castrated male DSH cat. Case 10. Within the left lateral lobe is a focal, slightly raised, multiloculated cystic nodule that is mottled white to dark red (arrowhead). On cut surface (inset), dark red opaque fluid is present within the cyst. Because of this finding, telangiectasia was also considered as a differential diagnosis at the time of gross examination. Photo courtesy of Elizabeth Alloway. (f–i) Histologic features of CBLs. Hematoxylin and eosin. (f) Focal CBL, liver, 18-year-old, castrated male Himalayan cat. Case 1. The CBL comprised multiloculated cystic structures lined by an attenuated biliary epithelium (upper left inset) with intervening thin, hyalinized collagenous trabeculae that contain few, small caliber blood vessels and entrapped islands of unremarkable hepatocytes (arrowheads, lower right inset). (g) Focal CBL, liver, 17-year-old, castrated male domestic longhair cat. Case 11. The CBL comprised multiloculated cystic structures lined by a cuboidal biliary epithelium (upper left inset) supported by thicker hyalinized beams of edematous collagenous stroma (asterisks). Note the scant eosinophilic fluid present in cyst lumina. (h) Focal CBL with lymphoplasmacytic inflammation, liver, 14-year-old, castrated male DSH cat. Case 14. Hyalinized to fibrillary collagenous trabeculae are multifocally expanded by moderate numbers of lymphocytes and plasma cells. (i) Focal CBL with intracystic hemorrhage, liver, 12-year-old, castrated male DSH cat. Case 10. Cysts within the CBL are multifocally filled with free erythrocytes (hemorrhage) admixed with fibrin and pale eosinophilic fluid. Telangiectasia is ruled out for this lesion based on the cuboidal epithelium lining cystic structures (upper left inset), consistent with biliary epithelium.
Of the 14 cases of CBL, 11 were evaluated histologically (Fig. 1f–i). and were consistently described as expansile, relatively well-demarcated, unencapsulated masses comprised a network of cystic structures lined by a variably attenuated, simple cuboidal biliary epithelium overlying trabeculae of collagenous stroma (Fig. 1f–g). Cuboidal epithelium was well-differentiated with minimal atypia and no apparent mitotic activity. Collagenous supporting trabeculae were variably thin (Fig. 1f) to thick (Fig. 1g), with somewhat hyalinized collagenous stroma and often had entrapped islands of hepatocytes. The majority (9/11, 82%) of CBLs were confirmed to be subcapsular. These features are compatible with those reported for VMCs/ biliary hamartomas, a variant of adult-type PCLD.5,33,49 In addition, infiltration of trabeculae by leukocytes was common (9/11, 82%) and was most often dominated by lymphocytes with fewer descriptions of plasma cells, pigment-laden macrophages, and neutrophils (Fig. 1h). Other features occasionally noted included presence of eosinophilic amorphous fluid within cystic spaces (4/11, 36%) and compression/atrophy of adjacent parenchyma (2/11, 18%). Two cats (2/11, 18%) had hemorrhage identified within cystic spaces of the CBL (Fig. 1i), including the cat with gross identification of dark red, opaque fluid within cysts.
For the remaining 3 cats with intrahepatic biliary cysts, lesions were not evaluated histologically; however, the cysts had gross features consistent with CBLs as described in other cases and were presumptively categorized as such.
Of the cats with FHLs, only a single cat (1/15, 7%), an 18-year-old, castrated male domestic shorthair, was diagnosed with CHF (case 15, Fig. 2). On gross examination, the cat had a body condition score of 1/9 with severe, diffuse atrophy of the skeletal muscles and adipose tissues. The cat had approximately 160 ml of red, watery fluid within the abdominal cavity admixed with white, friable, fibrin strands (Fig. 2a). The cat’s liver was mottled red to tan with an undulating surface. The majority (approximately 50%–75%) of the liver was tan and firm with loss of normal parenchyma (fibrosis), while the remaining intact parenchyma was red and comprised numerous, < 1 cm diameter, coalescing nodules (nodular regeneration, Fig. 2b). Multifocally throughout the tan tissue, there were too numerous to count, thin-walled, pinpoint to few mm in diameter, translucent, fluid-filled cysts.
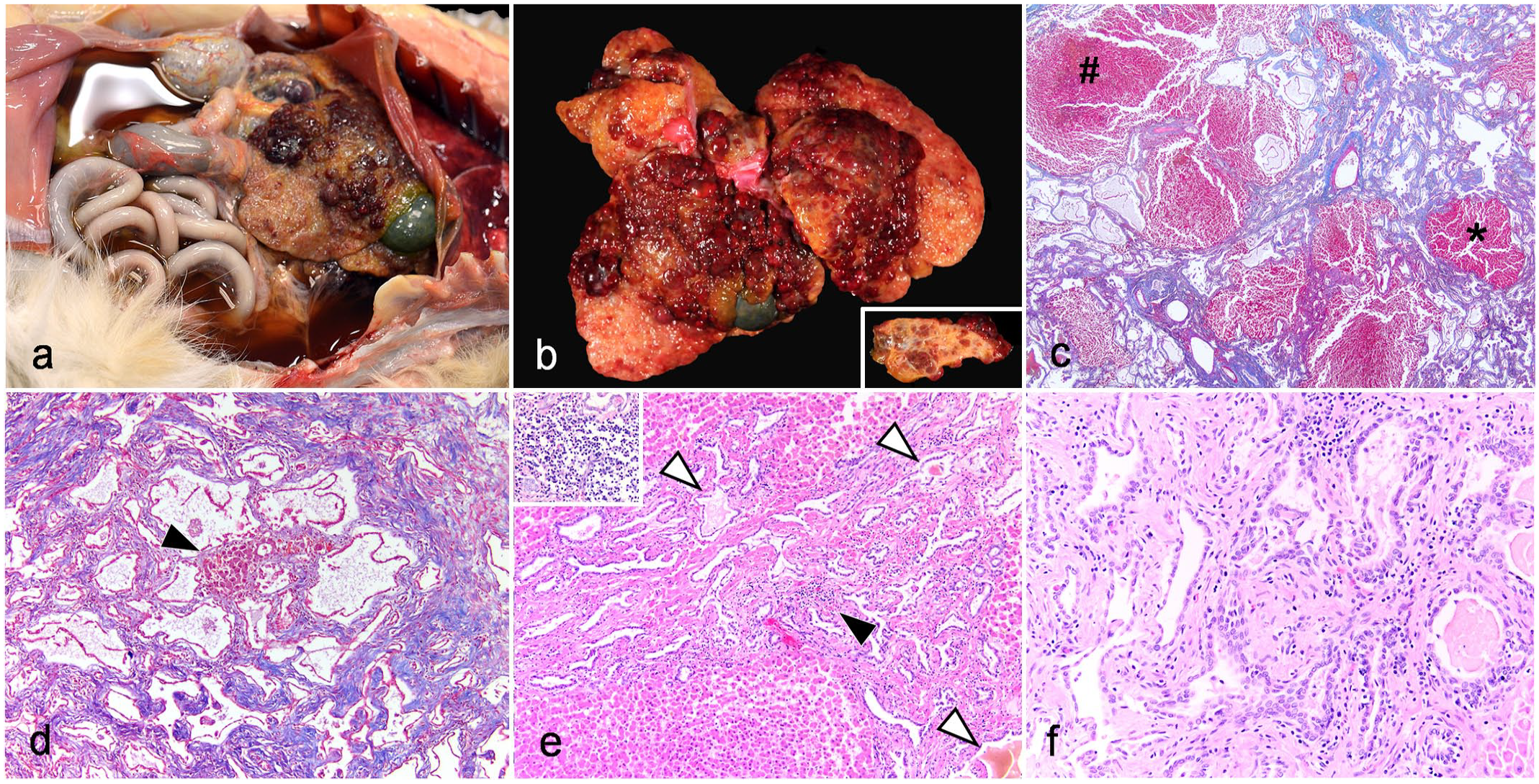
Gross and histologic features of congenital hepatic fibrosis (CHF) in a cat. CHF, 18-year-old, castrated male domestic shorthair cat. Case 15. (a) Abdominal cavity. Abundant dark orange-red, transparent, watery fluid fills the abdominal cavity with scattered admixed fibrin strands loosely adherent to several visceral organs. The liver is small with undulating margins and pale tan to dark red mottling throughout. Photo courtesy of Olivia Patania. (b) Liver. The majority of the liver is tan, collapsed, firm, and slightly undulating (fibrosis), while the remaining parenchyma is dark red and comprised numerous coalescing raised nodules (nodular regeneration). Regenerative nodules surrounded by dissecting, yellow-tan, fibrosis are apparent on cut surface (inset). Photo courtesy of Olivia Patania. (c–f) Histologic features of CHF. (c, d) Masson’s trichrome. (c) Numerous biliary cysts of variable shape and size are supported by fibrous connective tissue, which dissects through the hepatic parenchyma. Nodular regeneration (asterisk) as well as hepatocellular necrosis and hemorrhage within regenerative nodules (#) are apparent. (d) Tortuous and occasionally cystically dilated biliary profiles are embedded in fibrous connective tissue and surround isolated islands of hypertrophied, regenerative hepatocytes (black arrowhead). (e, f) Hematoxylin and eosin. (e) Proliferative, tortuous bile ducts that occasionally contain luminal green-brown fluid (bile; white arrowheads) track between portal tracts; portal veins are often inapparent. Scattered (black arrowhead) to occasionally more dense (inset) aggregates of lymphocytes, plasma cells, and macrophages accompany fibrosis and proliferative ducts. (f) Bile ducts are lined by a variably attenuated simple cuboidal epithelium and contain luminal bile or eosinophilic fluid. Scattered lymphocytes, plasma cells, and macrophages are present in fibrous connective tissue.
On histologic evaluation, the capsular surface of the liver was undulating with marked parenchymal collapse and loss of normal lobular architecture (Fig. 2c). Approximately, 50% to 75% of the hepatic parenchyma comprised bile ducts embedded in dense fibrous connective tissue that dissected throughout the tissue in a vague portal to portal distribution. Bile ducts were variably small to large, tortuous to cystically dilated, or had an irregular profile that sometimes forms short papillary projections (Fig. 2c, d). Bile ducts were lined by a simple, variably attenuated, cuboidal epithelium, and occasionally contained intraluminal orange-green fluid (interpreted as bile). Bile ducts and fibrosis occasionally surrounded ill-defined spherical nodules comprised hypertrophied hepatocytes that lacked lobular architecture (nodular regeneration, Fig. 2c, d). Within the adjacent parenchyma unaffected by fibrosis and biliary proliferation, there were multifocal to coalescing, centrilobular to random, variably sized foci of hepatocellular coagulative necrosis; red blood cells often accumulated in areas of necrosis and hepatocellular loss (Fig. 2c). Within portal areas and throughout tracts of fibrosis, portal veins were often inapparent (Fig. 2e). Multifocally, fibrosis and bile ducts were admixed with mild to moderate numbers of lymphocytes, plasma cells, and fewer neutrophils (Figs. 2e, f). Collectively, these gross and histologic findings were consistent with a diagnosis of CHF.
Gross and Histologic Features of Gallbladder Malformations
Gallbladder malformations were the second most common lesion identified (n = 5, Fig. 3). Using a recently proposed schema for gallbladder malformation classification in cats, 45 these were further subclassified as either duplex or bilobed gallbladders (Table 1). Duplex gallbladders consisted of 2 gallbladders of similar size with separate cystic ducts (n = 2, Fig. 3a, b), while bilobed gallbladders were defined by the presence of sacculated outpouchings of the gallbladder that were smaller than the primary gallbladder and joined with the primary gallbladder prior to formation of a single cystic duct (n = 3, Fig. 3c, d).
Gross and histologic features of extrahepatic biliary malformations in cats. (a–d) Gallbladder malformations. (a) Duplex gallbladder, 17-year-old, castrated male domestic shorthair (DSH) cat. Case 17. Two full-sized gallbladders with separate cystic ducts that conjoin prior to entry into the common bile duct are present. (b) Duplex gallbladder, 15-year-old, castrated male DSH cat. Case 16. Two full-sized gallbladders with separate cystic ducts are present. The “accessory” gallbladder (asterisk) is diffusely gray with a thin wall and a non-patent, blind-ended, anomalous cystic duct that tracks into the right lobe of the pancreas (arrowheads). (c) Bilobed gallbladder, 1-year-old, castrated male DSH cat. Case 18. Protruding from the midbody of the gallbladder with minimal clefting/separation from the gallbladder is a spherical out-pouching that is contiguous with the gallbladder (arrowheads). (d) Bilobed gallbladder, 13-year-old, spayed female, Siamese cat. Case 19. Extending from the neck of the gallbladder and completely separated from the gallbladder body is an ovoid out-pouching that is contiguous with the gallbladder neck (arrowheads). (e–f) Anomalous extrahepatic bile ducts. (e) Anomalous extrahepatic bile duct, 10-year-old, spayed female domestic medium hair cat. Case 2. An anomalous bile duct (black arrowheads) extends from the common bile duct into the right lobe of the pancreas and is patent with the gallbladder upon gallbladder expression (note green color of the anomalous duct). Concurrent mesenteric lymphoma (asterisk), fibrinous hepatic capsulitis (white arrowheads), and a focal von Meyenburg complex (white arrow) are also apparent. (f) Blind-ended anomalous cystic duct associated with duplex gallbladder, 15-year-old, castrated male DSH cat. Case 16. Hematoxylin and eosin. Cross-section of the duct indicated with white arrowheads in panel (b). The duct traverses through peripancreatic adipose and has a wall comprised an inner mucosa (predominantly sloughed due to autolysis), submucosal glands (arrowheads), a mixture of smooth muscle and connective tissue, and an outer adventitia. Submucosal glands (arrowheads, inset) are consistent with extrahepatic bile duct architecture.
Of the 2 cats with duplex gallbladders, 1 had 2 gallbladders that each had patent cystic ducts that joined together at the entry into the common bile duct; aside from the duplication of the organ, the gallbladders were grossly unremarkable (Fig. 3a). For the other cat with a duplex gallbladder, the secondary/accessory gallbladder was diffusely gray with mural thinning (Fig. 3b). This accessory gallbladder had a blind-ended cystic duct that did not connect to the common bile duct but instead tracked into the pancreatic parenchyma. Upon accessory gallbladder expression, light yellow to clear fluid flowed into the ectopic cystic duct into the parenchyma of the right lobe of the pancreas, with no apparent connection to the duodenum (Fig. 3b). A thin, approximately 1 to 2 mm diameter, band of tissue with a duct-like appearance connected the accessory gallbladder to the primary gallbladder, but there was not a patent lumen between the 2 gallbladders. Upon opening of the accessory gallbladder, similar yellow-clear fluid was present in the lumen along with gritty, pinpoint yellow debris and 2, approximately 5 mm diameter, discrete yellow cystoliths.
For the 3 cats with bilobed gallbladders, all malformations were described as dilated diverticula or outpouchings of tissue protruding from the wall of the gallbladder. One was noted to be arising from the midbody of the gallbladder and was spherical and 1 cm in diameter (Fig. 3c). The other 2 were described as arising from the neck of the gallbladder and were either spherical (2 mm in diameter) or ovoid/oblong (2 × 2 × 6 mm in diameter; Fig. 3d).
Histologic evaluations of the gallbladder malformations were only performed in 2/5 cats, including 1 cat with a bilobed gallbladder (case 18) and the cat with duplex gallbladders and concurrent cystolithiasis in the accessory gallbladder (case 16). Autolysis of the gallbladders precluded extensive histologic evaluation in both cases. For the bilobed gallbladder, there were no overt histologic abnormalities. For the duplex gallbladder, in both the accessory and the primary gallbladders, there was mild multifocal ectasia of submucosal glands, which were filled with a mixture of mucin and bile. Otherwise, the tissue was histologically unremarkable.
Gross and Histologic Features of Anomalous Extrahepatic Bile Ducts
Two cats had anomalous, blind-ended, extrahepatic bile ducts that extended from the gallbladder and into the parenchyma of the right lobe of the pancreas and had no apparent connections to the pancreatic ducts or duodenum. One of these anomalous bile ducts was previously described in association with an accessory gallbladder (Fig. 3b). For the second cat, an anomalous 6.5 cm duct extended from the common bile duct into the mesentery and ultimately the right lobe of the pancreas, running parallel with the duodenum (Fig. 3e). Upon expression of the gallbladder, the duct filled slowly with dark green to brown bile but appeared blind-ended and nonpatent with the duodenum. Notably, this cat also had concurrent multifocal VMCs. Histologic evaluations of anomalous bile ducts were performed for both cats. Autolysis of tissue precluded extensive evaluation, but both ducts comprised a wall consistent with a bile duct, including simple columnar epithelium overlying a submucosa with submucosal glands, and an outer wall comprised collagenous stroma with intermixed smooth muscle fibers (Fig. 3f).
Causes of Clinical Decline and Notable Comorbidities in Cats With Fibrocystic Hepatobiliary Lesions or Extrahepatic Biliary Malformations
All 20 cats with FHLs or EBMs were euthanized. Causes of clinical decline/euthanasia were variable, and the cause of decline for the majority of cats (17/20, 85%) was attributed to nonbiliary lesions. Renal or cardiovascular disease, including changes secondary to hyperthyroidism, were the most common primary lesions and contributed to the death of 8 cats (Table 1). Neoplasia was considered the primary cause of decline in 7 cats, and included lymphoma (3/7, 43%), pituitary neoplasia (2/7, 29%), ureteral carcinoma (1/7, 14%), and common bile duct carcinoid (1/7, 14%, Fig. 4a, b). An additional cat with a CBL had a biliary adenoma that was distinct from the concurrent CBL (Fig. 4c), as well as multifocal pulmonary adenomas, but these neoplasms were not considered the primary cause of morbidity, as this cat also had evidence of concurrent heartworm disease. The biliary adenoma was grossly a solid tan mass and was histologically comprised densely arranged tubules lined by plump, well-differentiated, cuboidal epithelium (Fig. 4d); notably, the margins of the neoplasm were relatively poorly demarcated, so a well-differentiated carcinoma was also considered. This mass was differentiated from a CBL by the lack of hyalinized collagenous trabecula and large cystic spaces as well as the more hypertrophied/plump character of the epithelial cells. Additional primary contributors to death included chronic bronchitis (feline asthma, n = 1), musculoskeletal trauma (n = 1), and immune-mediated hemolytic anemia (n = 1).
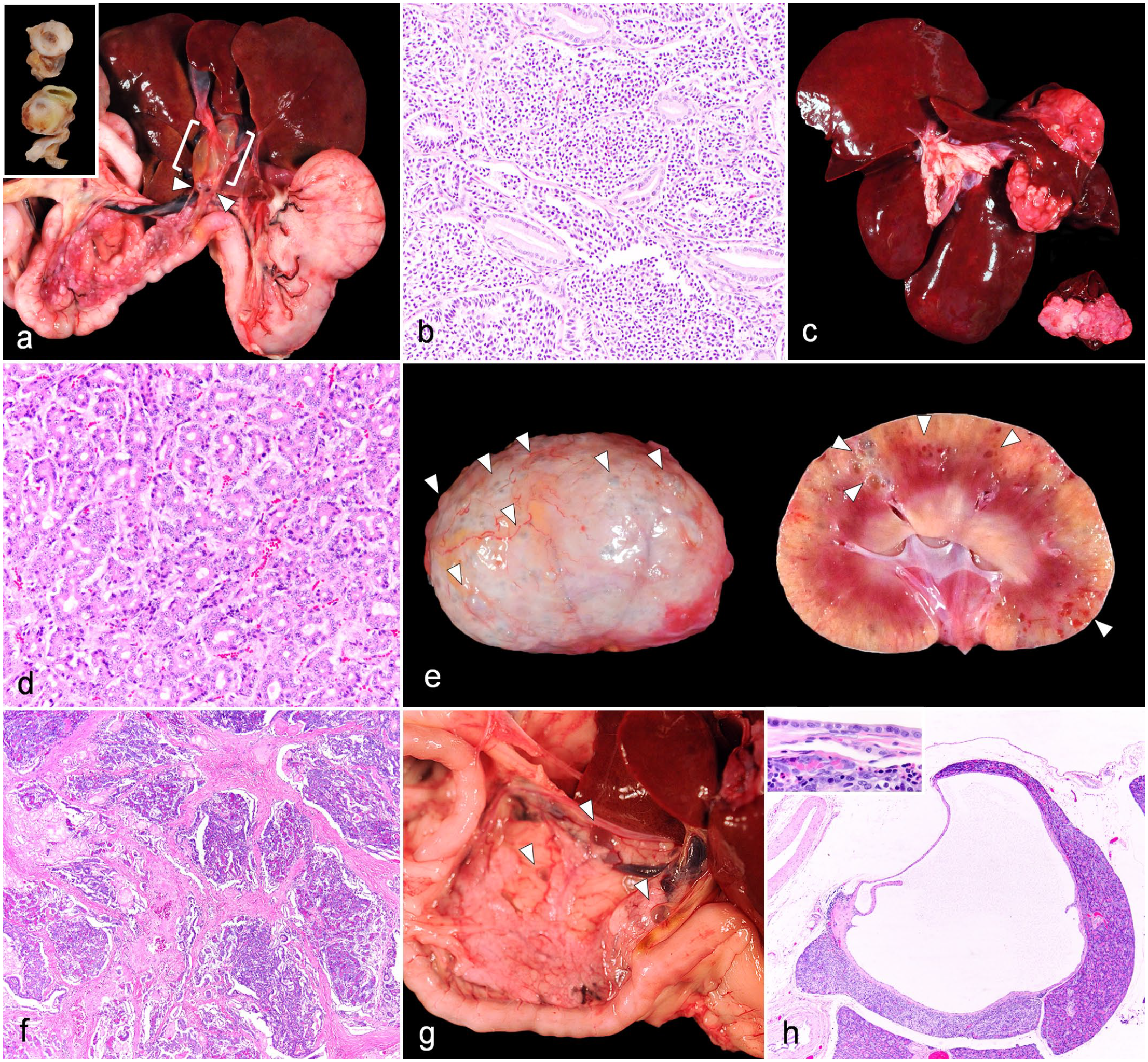
Gross and histologic features of pertinent comorbidities in cats with fibrocystic hepatobiliary lesions and extrahepatic biliary malformations. (a, b) Focal carcinoid, common bile duct, 17-year-old, castrated male domestic longhair (DLH) cat. Case 11. (a) Arising from the common bile duct proximal to entry at the major duodenal papilla is a focal, white-pink, spherical, soft mass (arrowheads). Inset: 2 cross-sections of the mass. The extrahepatic biliary tree proximal to this mass, including the common bile duct and hepatic duct, are segmentally distended (white brackets). (b) Common bile duct mass. Histologic evaluation reveals a mass comprised numerous packets of polygonal cells supported by a fine fibrovascular stroma, consistent with a carcinoid. Hematoxylin and eosin (HE). Adopted from Schreeg et al. 39 (c, d) Focal biliary adenoma, liver, 12-year-old, castrated male DLH cat. Case 2. (c) Arising from the caudate lobe is a well-demarcated, multilobulated, homogenously light pink to tan, slightly firm mass. On cut surface, the mass is mottled tan to pink and is solid with no apparent cystic spaces. (d) The mass comprised tightly packed tubular/ductal structures supported by minimal fibrovascular stroma. Note the lack of atypia as well as the lack of cystic spaces supported by collagenous trabeculae. HE. (e, f) Renal cysts and pancreatic fibrosis and atrophy associated with congenital hepatic fibrosis, 18-year-old, castrated male domestic shorthair cat. Case 15. (e) Numerous small cysts (white arrowheads) are apparent on the capsular (left) and cut (right) surfaces of the kidney. Photo courtesy of Olivia Patania. (f) Pancreas. Thick beams of collagenous stroma dissect through the pancreas, isolating lobules of acinar cells with few embedded dilated ducts. HE. (g, h) Multifocal pancreatic cysts, pancreas, 18-year-old, castrated male Himalayan cat. Case 1. (g) Within the pancreas, there are 3 thin-walled, clear, spherical cysts (white arrowheads). (h) Pancreas. Disrupting the pancreas is a focal, thin-walled cyst that has few internal papillary projections of collagenous stroma. Inset: A simple cuboidal epithelium and low numbers of associated lymphocytes, plasma cells, and eosinophils are apparent. HE.
Three of the cats with FHLs or EBMs had significant lesions affecting the biliary tree. However, FHL was considered the primary contributor to clinical decline/euthanasia in only the 1 cat (5%) that was diagnosed with CHF. In addition to CHF, this cat had numerous, bilateral, multifocal, variably sized renal cortical cysts (Fig. 4e). Histologic evaluation of the kidneys additionally identified mild chronic lymphoplasmacytic interstitial nephritis with moderate interstitial fibrosis. Given the relatively mild interstitial nephritis combined with numerous cysts, PKD was favored for this lesion. However, given that the cysts were small and affected a relatively small proportion of the renal parenchyma, cystic dilation of tubules secondary to chronic renal disease was also considered as a differential diagnosis. In addition, this cat had concurrent severe pancreatic fibrosis/atrophy and pancreatitis (case 15, Fig. 4f). Morbidity in this cat was ultimately attributed to a combination of all 3 of these lesions. In addition, the cat had several other neoplastic comorbidities that were considered non-primary contributors to decline, including a meningioma, thyroid adenomas, enteropathy-associated T-cell lymphoma type 2, and a pulmonary adenoma. Two of 20 (10%) of cats with FHLs or EBMs had concurrent, separate biliary diseases that were considered primary contributors to clinical decline/euthanasia. This included one cat with extrahepatic obstruction secondary to a carcinoid within the common bile duct (case 11, concurrent CBL); extrahepatic biliary obstruction and subsequent dilation was so severe in this case that choledochal cyst was initially considered for the extrahepatic biliary dilation (Fig. 4a). The other cat had significant triaditis (concurrent cholangitis, pancreatitis, and enteritis) secondary to microscopic pancreatolithiasis within the pancreatic ducts and common bile duct (case 10, concurrent CBL). In addition, 2/20 (10%) cats had histologic evidence of triaditis that were noted to be possible contributors to morbidity; however, both of these cats had concurrent renal/cardiovascular disease that were considered primary causes of clinical decline.
In addition to the concurrent renal cysts and pancreatic fibrosis seen in the cat with CHF, a Himalayan cat with a CBL (case 1) had concurrent pancreatic cysts (Fig. 4g, h). Grossly, within the body and along the periphery of the pancreas were 3, thin-walled, clear, cystic nodules that were 2 to 5 mm in diameter (Fig. 4g). Histologically, cysts were lined by an attenuated cuboidal epithelium and had mild numbers of lymphocytes, plasma cells, and eosinophils expanding the immediately adjacent parenchyma (Fig. 4h).
Discussion
To our knowledge, this is the first study documenting the prevalence and describing detailed gross and histologic features of FHLs and EBMs in a cohort of cats identified on autopsy in a single academic institute. In this study, FHLs were the most common lesion identified, and FHLs identified in this study had multiple histologic features compatible with those described for DPMs.
DPMs can affect different levels of the biliary tree, resulting in grossly and clinically distinct disease manifestations that are broadly referred to as congenital hepatic fibrocystic diseases. 52 In humans, congenital hepatic fibrocystic diseases have historically been grouped into 3 separate descriptive categories, and similar classification has been proposed for animals as well.12,49 These groups include (1) adult-type PCLD, (2) juvenile-type PCLD, and (3) congenital dilation of hepatic and large intrahepatic bile ducts (resembling Caroli disease).12,13,49 These groups are distinguished by the size of the bile duct affected by the malformation, and can be further subdivided by the presence of either ectasia or involution of the malformed ducts. 13
The grouping referred to as adult-type PCLD is characterized by unilocular to multilocular biliary cysts that lack a connection to the biliary tree; these lesions are thought to arise from the most peripheral/small bile ducts, and are therefore often subcapsular.5,49 Currently, both PCLD and VMCs are considered to be classified in this group.5,25,49 PCLD is thought to occur due to malformation and subsequent ectasia of peripheral bile ducts 49 and is characterized by accumulation of multiple 1 to 12 cm cysts within the liver parenchyma in small animals. 5 In humans, PCLD is further classified as occurring in conjunction with PCKD, or in isolation (ie, affecting only the liver); 25 to our knowledge, this distinction has not been made in small animals. Historically in humans, VMCs were thought to be lesions secondary to ischemia; however, they are currently thought to occur due to malformation and initial involution of peripheral bile ducts with accompanying deposition of variably hyalinized fibrous connective tissue.13,49 Given their association with other congenital hepatic fibrocystic diseases, as well as their morphologic overlap with other manifestations of adult-type PCLDs, they are currently accepted as a DPM variant.5,25,31,33,49 Juvenile-type PCLD, which includes CHF, is characterized by malformations affecting interlobular ducts, and result in accumulation of numerous abnormal bile ducts accompanied by abnormal portal veins and bridging fibrosis.12,13,49 Congenital dilation of hepatic and large intrahepatic bile ducts, as the name suggests, is characterized by abnormal dilation of medium to large caliber intrahepatic bile ducts that are contiguous with the rest of the biliary tree.12,13,49
In this study, CBLs were the most common FHL identified, and were present in 10% of cats. These CBLs uniformly had histologic features compatible with those of VMCs, as described in both cats and humans, which consisted of well-demarcated, predominantly subcapsular foci comprised multiple, irregular, biliary epithelium-lined, cystic duct structures that were embedded in trabeculae of hyalinized collagenous stroma.5,13,33,49 Furthermore, while not specific for VMCs, CBLs were also considered unrelated to clinical decline in all cases, which is consistent to findings with VMCs in humans where the majority of individuals with VMCs are asymptomatic. 42 Given these findings, we propose that the histologic features seen with CBLs in this study are supportive of a diagnosis of VMC, and that these lesions represent congenital biliary malformations, or DPMs. Henceforth, we will refer to these lesions as putative VMCs.
CBLs in this study had variable gross manifestations, presenting as either flat cysts in the parenchyma or raised mass-like lesions. This variation in gross appearance and size, as well as presence of these lesions in aged cats, likely has contributed to the previous classification of some of these lesions as biliary cystadenomas.1,12,28,49 In humans, benign biliary neoplasms, including serous cystadenomas and biliary fibroadenomas, have been described that have some morphologic overlap with the CBLs described in cats in this study, 15 and so we cannot completely rule out this possibility. However, in addition to the supportive histologic features of VMCs already outlined, we identified novel histologic features in described feline CBLs that we believe further support their classification as VMCs. In multiple cases, we identified islands of entrapped yet unremarkable (presumably preexisting) hepatocytes. While this finding is not a definitive diagnostic feature of VMCs, it has been described in putative VMCs in animals previously. 50 Furthermore, descriptions of VMCs in humans have noted that VMCs may be present multifocally in close proximity to one another, 49 and may cystically dilate and enlarge over time.5,13,31,32,49 Given this fact, we speculate that the CBLs described in this study may be capturing the dilation, interdigitation, and coalescing of multiple VMCs in cats, resulting in entrapment of preexisting hepatocytes within a larger multiloculated mass. Therefore, this phenomenon described in VMCs could explain both the entrapped hepatocytes and occasional large size of CBLs seen in cats. While dilation of other benign, static biliary masses (eg, an adenoma) could have a similar progressive enlargement, we postulate that a clonal proliferation of biliary epithelium effacing/compressing adjacent hepatocytes (as in a malignant neoplasm) would not entrap unremarkable hepatocytes. Evaluation of a larger cohort of putative feline VMCs is needed to further investigate the significance of this histologic feature. Furthermore, additional investigation into genetic associations (ie, PKD1 mutations), proliferative indices (eg, Ki-67 immunolabeling), and serial advanced imaging of cats with CBLs is warranted to provide further support that these lesions are representative of VMCs rather than adenomas.
To this point, in this study, there was one cat diagnosed with a concurrent putative VMC and biliary adenoma that allowed for direct comparison. While the putative VMC had consistent features as those described in this study, the biliary adenoma instead comprised densely arranged tubules lined by plump cuboidal epithelium and lacked collagenous trabeculae or central entrapment of hepatocytes. Despite the histologic differences described, in our experience, true biliary adenomas are exceedingly rare, and therefore, we cannot rule out that the diagnosed biliary adenoma either (1) arose from biliary epithelium originating from the putative VMC, (2) represents an uncommon manifestation of a DPM, or (3) represents a well-differentiated carcinoma. In humans, similar so-called biliary or bile duct adenomas have been described, although there is active debate over whether these are best termed adenomas or peribiliary hamartomas.16,22,55 Further evaluation of biliary masses that are not easily classified is warranted.
Similarly, VMCs can be readily differentiated from biliary adenocarcinomas (also called cholangiocarcinomas) due to the lack of associated clinical signs as well as the absence of gross and histologic features of malignancy. However, as alluded to with the biliary adenoma, care should be taken in histologic evaluation of CBLs suspected to represent VMCs, as malignant biliary neoplasia can arise from biliary epithelium within a VMC, as demonstrated in cats and other animals.4,51,54
The other FHL identified in this study was CHF, a DPM classified within juvenile PCLD in humans. Notably, this was the only FHL identified that was considered to be the primary cause of clinical decline in a cat in this study. CHF commonly leads to clinical signs of liver failure with development of portal hypertension, ascites, and acquired portosystemic shunts in dogs, horses, cattle, rats, and non-human primates as well as humans.6,8,19,20,26,36,58,59 Interestingly, the cat in this study with CHF was 18 years old when it succumbed to this congenital disease, while the majority of other animals reported with CHF became symptomatic at a much younger age.6,8,19,20,26,36,58 Previous reports of CHF in cats concurs with this finding, with CHF not identified in several cats until their teens. 5 In humans with CHF, there can be variation in the extent of the liver affected, the time of onset of clinical signs, and even increased fibrosis over time, as well as complication of lesions by superimposed bouts of cholangitis. 13 Given this variation in human CHF, we suspect that feline CHF may have similar slowly progressive changes (eg, progressive fibrosis and/or concurrent cholangitis), and may not become clinically relevant until advanced age.
Within the entire cohort, cats with FHL and EBM were significantly older than those cats without. The identification of these lesions, specifically CBLs, in aged cats has been a major factor in their classification as biliary cystadenomas. 1 While neoplasia is more common with age, in humans, multiple studies have shown that the incidence of VMCs also increases with age,33,42 with one study reporting an average age of detection of 55 years old. 42 In humans and animals, it has been reported that cysts in VMCs may dilate and become larger and more apparent with age,5,13,31,32,33,42,49 presumably due to filling of cysts with fluid and/or weaking of connective tissue surrounding cysts. Such “growth” of the lesions with advanced age could be compatible with classifying larger CBLs in this study as VMCs and could be one explanation for why the lesions were identified in older cats in this study. It may also be more challenging to identify early, small VMCs in young cats, both grossly and clinically. However, in the current study, the vast majority (98/140, 70%) of cats were > 7 years old, and so proportionally few young cats were evaluated. Further studies elucidating why these lesions suspected to be DPMs become grossly apparent/clinically relevant in aged cats are warranted.
Historically, DPMs, including both VMCs and CHF, have been highly associated with the presence of renal cysts, and in humans, these diseases are included in the spectrum of fibrocystic hepatorenal syndromes.11,33,35,47,56 Specifically in cats, there is a demonstrated association between PKD and DPMs.5,59 PKD1 mutations causing PKD in Persians, exotic shorthaired, and related breeds are associated with both biliary cysts similar to CBLs described in this study and CHF.5,12,59 In one study, 68% of cats with PKD had concurrent DPM in the liver. 5 Occasionally, cysts in the kidneys and liver may also be associated with cysts in the pancreas.5,11,14 In the current study, only 2 cats of 15 with FHLs (13%) had either renal or pancreatic cysts. One cat had concurrent CHF and renal cysts, and although it is unclear if the renal cysts truly represent PKD or a change secondary to chronic renal disease, both were considered significant contributors to morbidity. Notably, this cat also had severe pancreatic fibrosis with concurrent pancreatitis; it is unclear if this fibrosis represented a similar pancreatic congenital malformation or was a change secondary to CHF or other comorbidities. However, fibrocystic pancreatic dysplasia has been reported in humans concurrent to DPM and PKD and has been referred to as renal-hepatic-pancreatic dysplasia. 56 In addition, one cat had a putative VMC concurrent to pancreatic cysts. This cat was Himalayan, and so an associated PKD1 mutation may be possible, but was not investigated further. Notably, there were no Persian cats with biliary malformations identified in this study, which might explain the low prevalence of concurrent cysts in kidney or liver. However, the low prevalence of concurrent renal and pancreatic cysts in this population of cats with putative DPMs may also suggest that some DPMs may be present outside of the context of concurrent renal cysts and PKD1 mutations. As previously alluded to, further genetic evaluation of cats with CBLs is warranted to either bolster or refute the proposed congenital nature of these lesions.
Gallbladder malformations were the second most common biliary lesion found in this study. Gallbladder malformations in cats can be broadly divided into 2 categories, known as vesica fellea divisa and vesica fellea duplex. Vesica fellea divisa refers to a bi- or multilobulated gallbladder that still maintains a single cystic duct.7,9,24,45 These so-called “bilobed” gallbladders develop due to abnormal division of the primordial gallbladder and can have variable clefting, septation, and/or asymmetry. In contrast, vesica fellea duplex refers to a true duplication of the gallbladder, which occurs due to an embryologically redundant duplication of the primordial gallbladder. These duplex gallbladders have separate cystic ducts. In this study, both bilobed and duplex gallbladders were identified, and there was marked variability in the gross appearance of malformations, which is consistent with previous observations in feline gallbladder malformations.7,45 Interestingly, the overall incidence of gallbladder malformations found in the cohort of cats in this study (4%) is lower than those reported in other studies, which range from 12% to 24%.7,28,45 Previous studies in cats have described several (at least 23 in one study 7 ) anatomic variants of gallbladders, many of which are relatively subtle malformations, including so-called septated gallbladders that result from embryologic errors in gallbladder recanalization.9,24,45 Therefore, given the wide range and subtle nature of these malformations, it is possible that some subtler gallbladder malformations could have been overlooked in this cohort.
All gallbladder malformations in this study were considered unassociated with the primary causes of clinical decline; the incidental nature of this finding is consistent with the majority of previous reports of gallbladder malformations.7,28 One cat in this study with a duplex gallbladder had concurrent cholecystolithiasis but was asymptomatic, which may be associated with the non-patency of the associated cystic duct of the affected gallbladder. In contrast to the current cases, previous reports of concurrent feline duplex gallbladder and cholelithiasis were associated gallbladder rupture, cholestasis, and/or gallbladder mucocele formation.27,57 Therefore, it may be prudent to monitor cats with duplex gallbladder for cholelithiasis and other complications.
Two cats in this study had anomalous, blind-ended, extrahepatic bile ducts that traversed from the common bile ducts into the peripancreatic mesentery. One of these ducts was a nonpatent cystic duct associated with a duplex gallbladder, while the other was associated with a grossly unremarkable gallbladder and appeared to terminate within the right lobe of the pancreas parallel to the duodenum. To our knowledge, this type of biliary malformation has not been previously described in cats, although we have also anecdotally seen similar, suspected malformations in other cats outside of this cohort (personal experience of the authors). Grossly, these malformations bear some resemblance to subvesical bile ducts (supravesicular ducts or “Ducts of Luschka”) reported in humans, which are described as anomalous extrahepatic bile ducts that often connect from the gallbladder to either intrahepatic or extrahepatic bile ducts.29,38,41 However, in the 2 current cats, the ducts appeared to traverse from the extrahepatic biliary tree (either duplex cystic duct or common bile duct) directly into the pancreas/peripancreatic tissue, which is different from that described in humans. Meaningful histologic characterization of these ducts, unfortunately, was limited by postmortem autolysis that obscured mucosal evaluation. One possible alternative diagnosis for the presumed anomalous duct arising from the common bile duct is that the duct in fact represented a pancreatic duct that contained refluxed bile from the major duodenal papilla; however, based on the limited histology of the duct (size, suspect submucosal glands) and gross location of the duct, this hypothesis is less favored.
Multiple other intrahepatic biliary malformations and EBMs that have been described in cats, and seen outside of this cohort by the authors, were not identified within this cohort, including true PCLD,5,21,28 Caroli disease,10,34 and choledochal cysts.2,18,40,46 We suspect this is due to an overall lower prevalence of these conditions in cats. Interestingly, one study reported a very high incidence (44%) of these biliary malformations in cats specifically with suppurative cholangitis/cholangiohepatitis, with Caroli disease and choledochal cysts predominating. 10 Notably, these conditions were diagnosed primarily by abdominal ultrasound. In contrast, in the current study, significant biliary disease was only rarely identified in cats with biliary malformations, which may be due to the differences in types of malformations examined (ie, intrahepatic vs extrahepatic). Ultimately, the reason for these discrepancies between cohorts is unclear, but we suspect that some of these reported EBMs, which are characterized by dilation of ducts, may in fact be secondary changes to extrahepatic obstruction. In the authors’ personal experience, we have seen cats with extrahepatic biliary dilation mimicking Caroli disease and/or choledochal cyst (including case 11 with an extrahepatic biliary carcinoid) that were definitively concluded by serial diagnostic imaging and histology to be secondary to extrahepatic obstruction rather than congenital defects. Ultimately, further investigation and multimodal (ie, imaging, gross, and histologic) classification of extrahepatic bile duct dilation syndromes in cats is warranted.
Interestingly, FHLs and EBMs in this population of cats were nearly always mutually exclusive, with only a single domestic medium hair cat (case 2) having a concurrent DPM and anomalous extrahepatic bile duct. This is in contrast to dogs, where DPM have been reported in conjunction with gallbladder malformations, most notably gallbladder atresia.30,37 Future observational studies will benefit from further examination of whether these malformations can occur concurrently in cats.
There are multiple limitations to the current study. First, there was a lack of uniform histologic evaluation of tissues performed across cats, including a lack of consistent examination of liver tissue and histologic examination of CBLs in 3 cases. These limitations prevented definitive identification of links between FHLs/EBMs and concurrent hepatobiliary inflammation, as has been demonstrated in other studies. 10 Furthermore, it is possible that the 3 grossly diagnosed CBLs did not have features supportive of VMCs, and in fact represented different cystic lesions. Second, the extent of autolysis present in gallbladder and anomalous bile duct cases prevented meaningful histologic evaluation of these malformations, which ultimately limits our overall understanding and/or definitive confirmation of the lesions present. Third, mature adult and senior cats were overrepresented in the study population, making associations and observations in regard to the age and lesion presence challenging to assess. Finally, while the population size was relatively robust, the relatively limited number of FHLs and EBMs identified precludes meaningful conclusions on several facets of the malformations, including the extent of variability of gallbladder malformations, variability in features of CHF, as well as features of malformations not identified (eg, choledochal cyst, Caroli disease, PCLD).
In conclusion, FHLs and EBMs appear to be relatively common in cats, with CBLs being the most common malformation identified in this cohort. Despite having a variable gross presentation, CBLs had histologic and clinical features compatible with those described for VMCs, and we propose that the majority of these lesions represent this subtype of DPM. In this cohort, most FHLs and EBMs were incidental, with the exception of CHF being a significant contributor to morbidity. Further studies are warranted detailing subtle gallbladder anatomic malformations in cats, investigating the overall prevalence and breadth of FHLs and EBMs in a larger population of cats, and investigating possible contributions of these lesions to concurrent feline hepatobiliary disease.
Footnotes
Acknowledgements
We would like to acknowledge the expertise and contribution of the staff of Ms. Laura Miller and the NCSU CVM Histology Laboratory. We would also like to thank the numerous NCSU CVM pathology faculty, residents, staff, and students that aided in tissue collection; without this team effort this study would not have been possible. Specifically, we would like to thank Drs. Elizabeth Alloway, Amy Flis, and Olivia Patania for providing excellent gross images and descriptions of featured malformations, and Dr. Mandy Womble for aid in retrieval of gross images, histologic slides, and autopsy reports. Finally, we would like to thank Dr. Jody Gookin for her guidance and oversight in the initial project that led to collection of tissues for characterization in this study.
Author Contributions
MES and JMC designed and performed the experiments, performed histologic evaluations, and wrote the manuscript. MES performed statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.