
Abstract
Asian small-clawed otters (Aonyx cinereus, ASCOs) and North American river otters (Lontra canadensis, NAROs) are commonly housed at zoos and aquaria in the United States. The few reports of diseases in these species have mainly focused on free-ranging populations and do not represent otters in managed care. Necropsy reports from 93 individuals, 71 ASCO and 22 NARO, that died or were euthanized between 2000 and 2020 from 10 separate institutions were evaluated, including 47 females, 45 males, and 1 unreported sex. All otters with known ages ranged between 2 months and 21 years of age (median = 14 years). Otters were further divided into age classes according to known lifespan. ASCO age classes were juvenile (4; 6%), adult (26; 37%), older adult (9; 13%), and geriatric (32; 45%). NARO age classes were juveniles (0; 0%), adult (5; 23%), older adult (5; 23%), and geriatric (12; 55%). Common causes of death or euthanasia in both species included malignant neoplasia (29), chronic renal disease and/or urolithiasis (27), degenerative joint disease (13), and cardiovascular disease (10). Severe gastrointestinal hemorrhage caused mortality in 9 (13%) ASCOs. Common morbidities or comorbidities included periodontal disease (30) and degenerative joint disease (21). Consistent health and disease surveillance of these otter species in managed care will further elucidate mechanisms of disease, aid in the development of preventative and therapeutic strategies, and continue optimizing standards of care.
Keywords
Otters are semi-aquatic and aquatic members of the Mustelidae family and are commonly housed at zoological institutions and aquaria for their social and familial bonding, relative ease of husbandry, and charismatic behavior. Although some otter species are considered ubiquitous, population declines have been reported in 12 species, 7 species are vulnerable, and 5 are endangered, according to the International Union for Conservation of Nature. Asian small-clawed otters (ASCOs, Aonyx cinereus) are listed as vulnerable in their native ranges, although they are found in zoos and aquaria around the world and kept as pets in Japan.30,54 Other otter species managed at zoos and aquaria include North American river otters (NARO, Lontra canadensis), spotted-necked otters (Hydrictis maculicollis), Eurasian river otters (Lutra lutra), and sea otters (Enhydra lutris).
Much of the available literature focuses on disease epidemiology of free-ranging individuals, particularly sea otters, or specific disease processes.1–13,17–20,23,24,35,38,45,46 Husbandry protocols and medical guidelines are available for otter species; however, there are limited case reports and case series involving otters in managed care, and comprehensive retrospective studies are lacking. 26
Gross necropsy and histology reports from ASCO and NARO housed at United States zoos and aquaria were reviewed to investigate major causes of death and concurrent disease processes. This pathology data will be valuable to optimize husbandry, nutrition, and management, as well as to develop new and improve current preventative and therapeutic strategies for these and similar otter species.
Material and Methods
Necropsy reports from ASCO and NARO housed at 10 different Association of Zoos and Aquariums-accredited institutions within the United States that died or were euthanized between 2000 and 2020 were evaluated for signalment, gross and histologic lesions, cause of mortality, and comorbidities. Cases without histology data (eg, gross examinations only) and neonates less than 1 month of age were excluded. Necropsy findings were classified by etiology (infectious, neoplastic, degenerative, inflammatory, toxic, environmental, and traumatic) and further categorized by body system (cardiovascular, respiratory, urinary, reproductive, gastrointestinal, endocrine/exocrine, hemic-lymphatic, musculoskeletal, nervous, and integumentary). For euthanized individuals, the primary disease process that led to euthanasia was listed as the cause of mortality. Lesions or diseases that were not considered a direct cause of death were noted as comorbidities.
Signalment (species, age at time of death, and sex) and method of death (euthanasia vs natural death) were noted. The ages of both species were categorized according to life stages.26,39 For ASCO, age categories included juvenile (<1 years), sexual maturity/adult (1–8 years), older adult (life expectancy in the wild is 8–12 years), and geriatric (>12 years). For NARO, age categories included juvenile (<2 years), sexual maturity/adult (2–10 years), older adult (life expectancy in the wild is 10–15 years), and geriatric (>15 years). Fisher’s exact tests were used to identify age category and sex associations with causes of mortality for both species. Analyses were conducted using QuickCalcs software (GraphPad Software Inc., San Diego, California).
Immunohistochemistry was completed at the University of Illinois Veterinary Diagnostic Laboratory per the manufacturers’ instructions: CD3 polyclonal (Biocare, Concord, California; 901-215-110912); CD79a monoclonal (Biocare 901-067-091917), and myoglobin (BioGenex, San Ramon, California; 932-012P-EN).
Results
Asian Small-Clawed Otters
Necropsy reports from 71 ASCOs were included in the study. Sex was identified in all ASCO and included 33 (46%) intact males, 1 (1%) neutered males, 36 (51%) intact females, and 1 (1%) spayed female. Age at the time of death was reported for 56 individuals and ranged from 2 months to 20 years (median = 14 years). The exact age was not reported for 15 individuals (listed as adult or geriatric), and those were included within the associated age-class categories. Age-class distribution was as follows: 4 juveniles (6%), 26 adults (37%), 9 older adults (13%), and 32 geriatrics (45%). Thirty-nine (55%) individuals were euthanized, and 31 (44%) died naturally. The method of death for 1 individual was not listed. Lesions are listed in Table 1 and reviewed by categories below. No statistically significant association was identified between sex and age categories with causes of mortality.
Non-neoplastic lesions of Asian small-clawed and North American river otters.
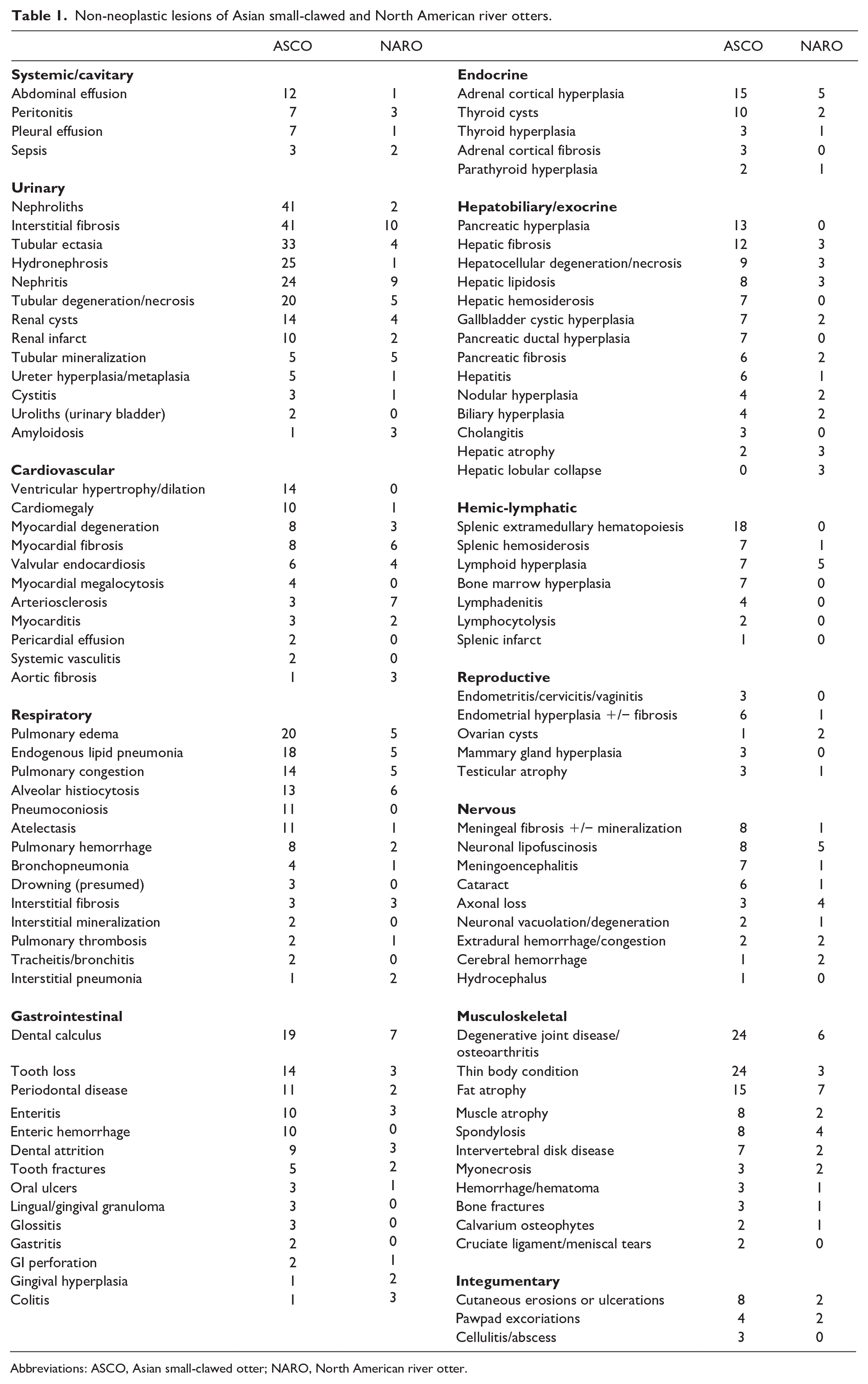
Abbreviations: ASCO, Asian small-clawed otter; NARO, North American river otter.
Degenerative
Degenerative diseases directly contributing to mortality involved the urinary (24 cases, 34%), musculoskeletal (9 cases, 13%), and cardiovascular (4 cases, 6%) systems. Chronic renal disease (CRD) was the most common cause of mortality in this species. Common associated lesions included nephrolithiasis (21 cases) (Fig. 1a), interstitial fibrosis (21 cases), hydronephrosis (17 cases), tubular dilation (16 cases), nephritis (11 cases), tubular degeneration and/or necrosis (10 cases), tubular cysts (8 cases), and chronic infarction (5 cases) (Fig. 1b). Interestingly, only 3 ASCO with CRD had uroliths or ureteroliths, and 2 had associated urinary bladder cystitis. One of these otters had bacterial pyelonephritis, and the other had urinary bladder herniation through the inguinal canal with subsequent strangulation. In 1 otter with CRD and lymphoma, no nephroliths were identified; however, a severe membranous glomerulopathy was detected histologically.

(a) Asian small-clawed otter, kidney, nephrolithiasis. The renal pelvis is dilated with large golden yellow to brown calculi. The surrounding parenchyma is pale and firm with loss of corticomedullary distinction. (b) Asian small-clawed otter, kidney, nephrolithiasis. Histologically, the renal parenchyma is distorted with extensive loss and atrophy of tubules and increased interstitial collagenous tissue (fibrosis), in which there are low numbers of lymphocytes, plasma cells, and macrophages. Remnant tubules are ectatic, degenerate, or lined by enlarged, basophilic, crowded cells with vesicular nuclei (hyperplasia, regeneration). Hematoxylin and eosin (HE). (c) Asian small-clawed otter, stifle joint, degenerative joint disease. The menisci and the joint capsule are thickened (fibrosis). The articular cartilages are dull, gray, and granular with partial to complete loss and exposure of the subchondral bone (eburnation). (d) Asian small-clawed otter, thoracic cavity, congestive heart failure. The heart is enlarged, and the thoracic cavity is filled with hazy, watery, yellow-tinged fluid (effusion). (e) Asian small-clawed otter, liver, congestive heart failure. Hepatic lobules are collapsed, and centrilobular cords are narrow and discontinuous. Intervening sinusoids are multifocally dilated and contain Kupffer cells with brown granular cytoplasmic pigments (hemosiderin), indicative of chronic passive congestion. HE. (f) Asian small-clawed otter, heart, pulmonary arterial thrombosis. The right ventricle (incised) is dilated, and the pulmonary artery contains an elongated, cylindrical, pink, tan, and dark red mass (thrombus).
While CRD was the direct cause of death in 24 ASCO, 40 (56%) individuals had nephroliths identified on gross examination. Nephrolith composition was evaluated at the Minnesota Urolith Center (University of Minnesota) for 12 ASCO (Table 2). Nine had stones composed of >80% calcium oxalate monohydrate, 2 had stones composed of 100% uric acid, and 1 had a stone composed primarily of ammonium urate.
Urolith composition of Asian small-clawed otters.
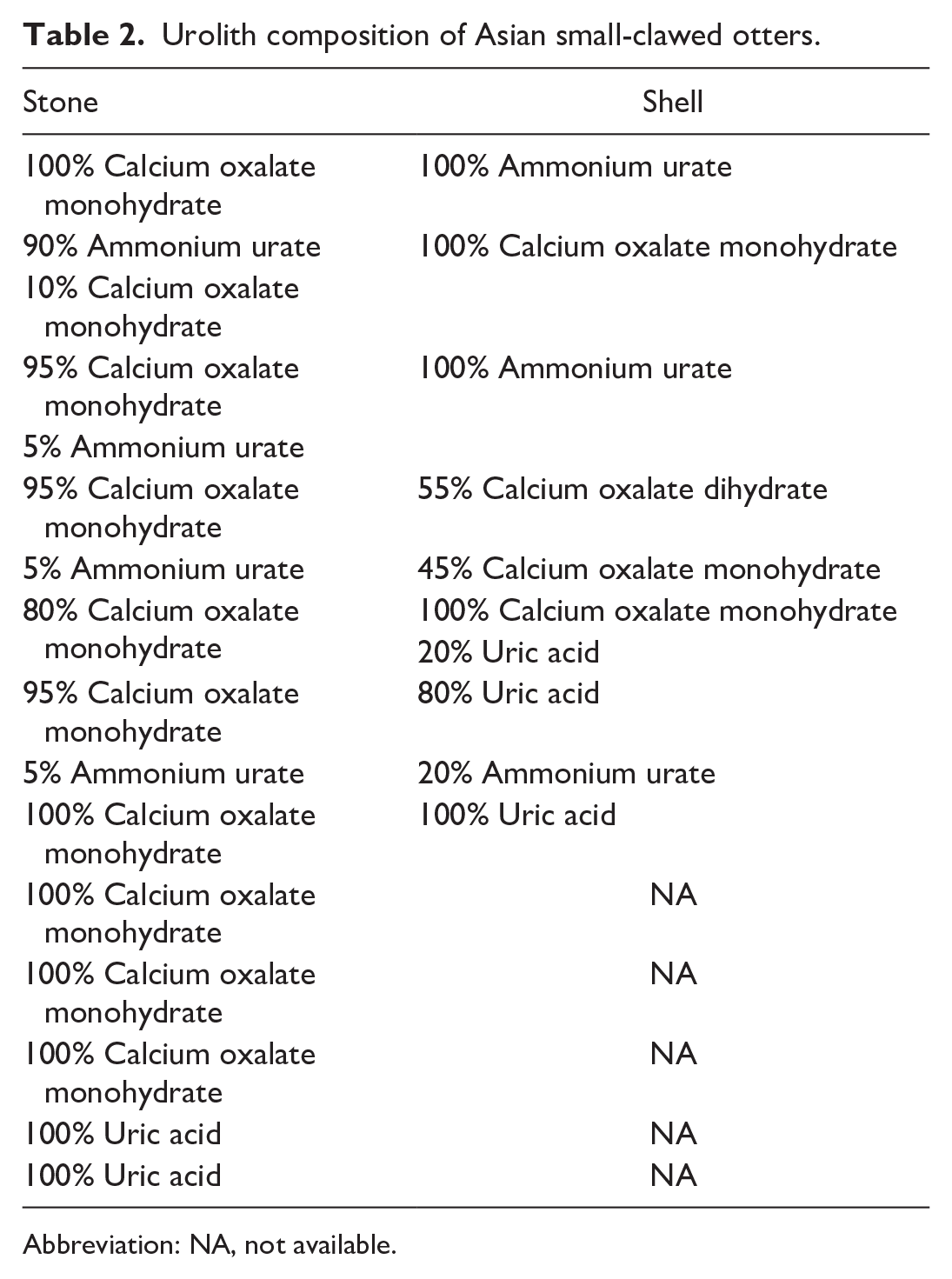
Abbreviation: NA, not available.
Degenerative joint disease (DJD; osteoarthritis) was a primary cause of death (euthanasia) in 9 (13%) ASCOs. Two otters had unknown ages and were listed as adults, and the 7 otters with known ages ranged from 14 to 20 years (median = 16). Joints most affected included the stifles (6 cases) (Fig. 1c), elbow (2 cases), coxofemoral (1 case), lumbar (L) vertebrae (5 cases), and thoracic (T) vertebrae (3 cases). Common gross lesions associated with DJD included joint capsule fibrosis, osteophyte formation, cruciate ligament tear (stifle), meniscus degeneration (stifle), and eburnation. One otter had substantial intervertebral disk disease (IVDD) involving T8–9 and T11-L1 with osteolysis, fibrosis, and nucleus pulposus degeneration. Two ASCOs with arthritis had acute traumatic fractures at the time of euthanasia—1 of the femur and 1 of the tibia/fibula. Fractures were not associated with affected joints directly and were considered independent from arthritis. Common extraskeletal lesions in cases euthanized for DJD included alopecia and/or excessive barbering, foot pad ulceration, and hindlimb muscle wasting. Six of the 9 (67%) ASCOs euthanized due to DJD also had concurrent primary CRD identified as a cause of death.
Four (6%) ASCO died (3 cases) or were euthanized (1 case) due to primary cardiovascular disease, with 3 cases of congestive heart failure and 1 case of pulmonary thromboembolism. All 3 individuals with cardiovascular disease had evidence of both left and right-sided failure with bicavitary effusions (Fig. 1d), chronic passive hepatic congestion (Fig. 1e), and alveolar histiocytosis. Hemosiderin-laden macrophages interpreted as “heart-failure cells” were identified in pulmonary alveoli in 1 case. Aside from grossly dilated right (2 cases) or left (1 case) ventricles, only 1 case had histologic lesions in the heart that included endocardial fibrosis and aortic valvular endocardiosis. In the otter with pulmonary thromboembolism, the thrombus was present at the hilus of the left middle lung lobe and extended along the main pulmonary artery into the right ventricular outflow tract (Fig. 1f). The right ventricle had focal myocardial fibrosis, which was considered related. A few additional smaller thrombi were also identified in arteries within the left caudal lung lobe, and there was evidence of chronic thrombosis of the hepatic artery (severe bridging to massive hilar fibrosis).
Neoplastic
Malignant neoplasia (19 cases, 27%) was the second most common cause of mortality in ASCO. Systems affected included digestive, reproductive, hemic-lymphatic, integumentary, endocrine, urinary, and respiratory (Table 3). Digestive tract neoplasms resulting in mortality were restricted to the oral cavity, with 2 cases of squamous cell carcinoma involving the tongue that, in 1 individual, extended into the pharyngeal tissue. No evidence of regional or distant metastasis was identified in either case. Mammary gland neoplasia resulting in euthanasia was identified in 4 ASCOs. Three masses were the characteristic of mammary adenocarcinomas. The fourth mass had a predominantly spindloid morphology with differential diagnoses including spindle cell carcinoma, soft tissue sarcoma, or malignant myoepithelioma. No further diagnostics were completed to differentiate these possible diagnoses. All 4 mammary gland neoplasms had evidence of regional or distant metastasis with the lungs (Fig. 2a), liver, and lymph nodes being the most common sites of metastasis.
Neoplasms of Asian small-clawed otters.
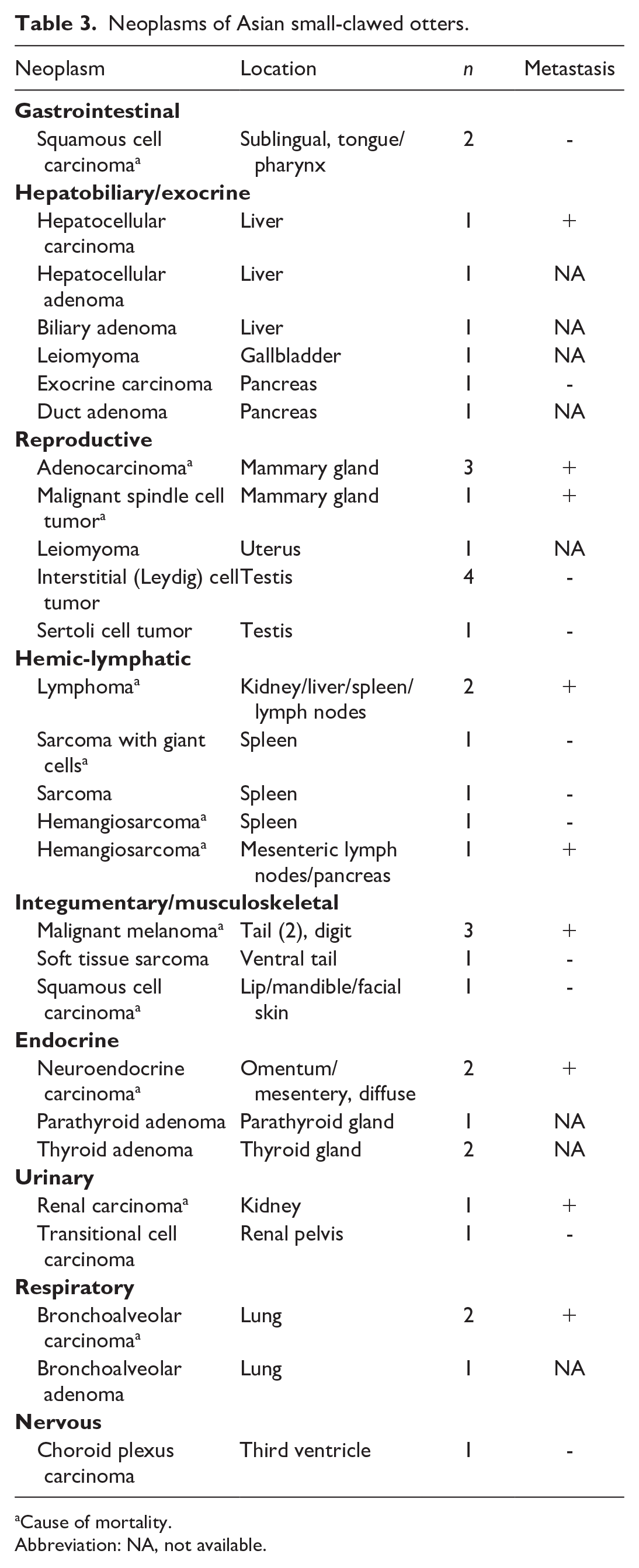
Cause of mortality.
Abbreviation: NA, not available.

(a) Asian small-clawed otter, heart and lungs, metastatic mammary gland carcinoma. The lungs and mediastinum have multiple, variably sized, tan to pale yellow neoplastic nodules. The tracheobronchial lymph node is also severely enlarged and expanded by neoplastic tissue. This otter had a large mammary mass. (b) Asian small-clawed otter, spleen, hemangiosarcoma. The spleen is expanded and effaced by several coalescing cystic, blood-filled masses. (c) Asian small-clawed otter, lung, bronchoalveolar carcinoma. Pulmonary parenchyma is replaced by densely arranged and anastomosing tubular and papillary neoplastic structures, recapitulating bronchioles and alveoli among a variably dense fibrous stroma. Hematoxylin and eosin (HE). (d) North American river otter, small intestine, small T-cell lymphoma. Intestinal villi are thickened with numerous small neoplastic lymphocytes along and among the surface enterocytes (epitheliotropism). HE. (e) North American river otter, small intestine, small T-cell lymphoma. Neoplastic lymphocytes have positive immunolabeling using antibodies targeting CD3, indicative of a T-cell lineage. (f) North American river otter, urinary bladder, transitional cell carcinoma. At the trigone, bladder mucosa has closely clustered, irregular, raised masses. (g) North American river otter, kidney, myoglobinuric nephrosis. Some renal tubules are slightly dilated, lined by attenuated epithelium, and contain luminal clumped granular to smudged, eosinophilic material. HE. (h) North American river otter, kidney, myoglobinuric nephrosis. In affected renal tubules, the luminal material has positive immunolabeling using antibodies targeting myoglobin.
Four of the 5 neoplasms originating in the hemic-lymphatic system involved the spleen, and the fifth was limited to visceral lymph nodes. Lymphoma and splenic sarcomas, including hemangiosarcoma (Fig. 2b), were identified, and, aside from lymphoma, dissemination (metastasis) was rare.
Malignant melanoma (3 cases) was the most common integumentary neoplasm associated with mortality. The tail was the primary site of origin for 2 individuals and a hindlimb digit for the third. All 3 otters had their primary neoplasms completely excised; however, widespread metastases involving the liver, spleen, and lymph nodes occurred, resulting in euthanasia. The second type of integumentary neoplasm that was a primary cause of death was a regionally invasive squamous cell carcinoma involving the facial skin and the labial mucocutaneous margin. Like the oral squamous cell carcinomas, no evidence of metastasis was identified.
The 2 fatal endocrine neoplasms included abdominal and/or widespread disseminated neuroendocrine carcinomas. No primary neoplasm was identified in either of these otters, although adrenal medulla (pheochromocytoma) was considered a possible origin in 1 case.
Two cases of bronchoalveolar carcinoma (Fig. 2c) were identified. It was the primary cause of death in 1 individual with pleural carcinomatosis and a single metastasis in the pancreas. Renal carcinoma was the only fatal urinary system neoplasm and was associated with peritoneal carcinomatosis, pleural effusion, and splenic metastasis. Interestingly, this individual also had concurrent chronic nephrolithiasis and hydronephrosis.
Infectious
Infectious causes of death (14; 20%) were limited to bacterial infections affecting the skeletal muscle/soft tissues and urinary, digestive, respiratory, reproductive, and nervous systems. Of these, 3 otters had fulminant septicemia, 3 had myositis/cellulitis, 4 had pyelonephritis, 3 had bronchopneumonia, and 2 otters had clostridial enteritis. There were individual cases of rhinitis, pyometra, and meningitis.
All 4 cases of pyelonephritis were in individuals with concurrent CRD and nephrolithiasis; thus, they were considered to be related to mechanical damage in the urinary tract and ascending bacterial infection. Bacteria cultured at necropsy from cases of pyelonephritis included Staphylococcus pseudintermedius, Escherichia coli, and hemolytic E. coli. Three of these otters had evidence of septicemia, which was the major cause of death, and included 2 otters with CRD and nephrolithiasis and the single case of rhinitis. Septic lesions included meningoencephalitis, myocarditis, vasculitis, lymphadenitis, enteritis, and/or peritonitis. In most cases, at least 3 bacterial organisms were identified on postmortem culture. In a few cases, no bacteria were identified, presumably due to long-term antibiotic treatment. Bronchopneumonia was secondary to aspiration in 1 case and was an extension of inflammation or aspiration of bacteria from a chronic cheek abscess in the second.
Soft tissue bacterial infections included necrotizing masseter muscle myositis, axillary cellulitis, and retrobulbar abscess in 1 case each. Mixed bacterial populations, including gram-positive cocci, were identified within the masseter muscle myositis and retrobulbar abscess. An atypical Mycobacterium sp. was identified in the case of axillary cellulitis. The retrobulbar abscess extended into the orbital bone and meninges, resulting in severe osteomyelitis and meningitis.
Clostridium sp
Infection was associated with a necrotizing ileitis in 1 individual, and Clostridium difficile enteritis was confirmed in the other. Rhinitis was associated with lymphadenitis and pulmonary congestion with mixed bacteria on postmortem culture. One case of fatal pyometra, caused by Pseudomonas aeruginosa, was identified in an otter with concurrent CRD and osteoarthritis. Finally, 1 case of meningitis was identified in an individual with concurrent CRD and osteoarthritis. The cause of meningitis was not investigated further (suspected viral etiology).
Inflammatory
Two ASCOs (3%) died from sequelae of gastrointestinal perforation (1 gastric and 1 duodenal). In both cases, perforation by a foreign body (fish bone) was suspected, as there was no significant concurrent gastrointestinal disease. Sequelae included severe suppurative peritonitis, lymphadenitis (1 case), and pneumoabdomen with pulmonary atelectasis (1 case). In the individual with duodenal perforation, there was an associated region of chronic peritonitis indicative of previous perforation.
Toxic/metabolic
Two (3%) cases of suspected 1–4 phenylenediamine toxicity occurred simultaneously at 1 institution. These otters had Nyanzol-D (Albinal Dyestuff Inc., Jersey City, New Jersey) fur dye placed for identification at the time of their quarantine examination and died within hours after application. Ingestion of the hair dye (self and conspecific grooming) was the presumed route of intoxication, as both otters had black discolored tongues at the time of death. Gross lesions included hydropericardium with orange to brown fluid, scleral and mucosal pink to orange discoloration, hepatomegaly, and failure of lungs to collapse upon opening the thoracic cavity, suggestive of acute respiratory distress and failure. Histologically, the lungs had bronchoconstriction with luminal mucus and proteinaceous fluid and extensive edema; acute myocardial and skeletal muscle degeneration; peribiliary, mesenteric, and glossal edema; and marked multicentric congestion.
Environmental and idiopathic
Nine (13%) otters died (6 cases) or were euthanized (3 cases) with moderate-to-severe luminal gastrointestinal hemorrhage. Luminal hemorrhage was present throughout the stomach, intestine, and colon (2 cases) or in the intestine and colon only (7 cases). Coprimary causes of death included CRD, lymphoma, metastatic melanoma, hemangiosarcoma, bacterial septicemia, and congestive heart failure. Two otters did not have any other significant lesions and died solely due to severe gastrointestinal hemorrhage. Five (56%) of these ASCO had undergone an anesthetic procedure within 5 days of death, 3 within 1 day.
There were 3 (4%) cases of suspected drowning. Aside from evidence of potential trauma in 1, no other contributory diseases or lesions were identified.
One (1%) juvenile ASCO with no significant lesions aside from complete depletion of fat reserves died 4 days after vaccination. One (1.4%) adult ASCO died while under anesthesia for an ovariohysterectomy for in utero fetal death and maceration. Bacterial culture of the uterine contents yielded no growth, and there was no evidence of concurrent systemic disease to attribute to anesthetic death. The cause of death in 1 older adult ASCO was unknown, with no significant gross or histologic lesions.
Comorbidities
Renal lesions were the most common comorbidity and were identified in 32 ASCO that did not die or were euthanized due to primary CRD-related disease. Lesions included urolithiasis (10 cases), interstitial fibrosis (20 cases), tubular dilation (16 cases), nephritis (11 cases), tubular degeneration (10 cases), renal cysts (6 cases), ureter hyperplasia (5 cases), and infarction (5 cases).
DJD was also a significant comorbidity. Sixteen (23%) ASCOs that did not die and were not euthanized for DJD-related disease had evidence of osteoarthritis, IVDD, and/or spondylosis. Common joints affected were the stifle (10 cases), elbow (4 cases), shoulder (2 cases), and tarsal (2 cases). Spondylosis and/or IVDD involved the cervical (4 cases), thoracic (4 cases), and lumbar (2 cases) vertebrae.
Degenerative cardiac comorbidities included 11 (15%) cases of cardiac ventricular dilation and 7 (10%) cases of myocardial fibrosis. Periodontal diseases including missing or broken teeth, dental attrition, dental calculus, and/or gingival hyperplasia were identified in 23 (32%) otters. Six ASCOs (8%) had lenticular cataracts.
Multiple benign neoplasms (Table 3) and hyperplastic lesions (Table 1) were identified including gallbladder cystic hyperplasia (7 cases), biliary hyperplasia (4 cases), hepatic nodular hyperplasia (4 cases), nodular exocrine pancreatic hyperplasia (13 cases), pancreatic ductal hyperplasia (7 cases), parathyroid hyperplasia (2 cases), thyroid hyperplasia or cysts (10 cases), adrenal cortical nodular hyperplasia (15 cases), endometrial hyperplasia (6 cases), and mammary gland hyperplasia (3 cases).
Thin body condition was commonly reported (24; 24%). Fat (15 cases, 21%) and muscle (8 cases, 11%) atrophy were generally noted in ASCO with one or more significant disease processes (CRD, neoplasia, etc).
North American River Otters
Necropsy reports from 22 NARO met the inclusion criteria. Of these, sex was identified in all but 1 individual and included 9 (41%) intact males, 2 (9%) neutered males, and 10 (32%) intact females. Age at the time of death was reported for 17 individuals and ranged from 2 to 21 years (median = 16 years). The exact age was not reported for 5 individuals (listed as adult or geriatric), and those were included within the associated age-class categories. The age-class distribution was as follows: no juveniles (0; 0%), 5 adults (23%), 5 older adults (23%), and 12 geriatric (54%). Thirteen (59%) otters were euthanized, 8 (36%) otters died spontaneously, and the cause of death for 1 (5%) otter was not reported. Lesions are listed in Table 1 and reviewed by categories below. Neoplasia was the most common cause of mortality (10 cases, 45%), followed by degenerative disease (9 cases, 41%), inflammatory disease (2 cases, 9%), and trauma (1 case, 5%). No statistically significant association was identified between sex and age categories with causes of mortality.
Neoplastic
Gastrointestinal neoplasms were the most common, with 3 cases of small intestinal lymphoma and 1 case of suspected enteric-origin adenocarcinoma (Table 4). Two cases of intestinal lymphoma had some degree of epitheliotropism, with 1 confirmed to be T-cell origin on immunohistochemistry (CD3 positive, CD79 negative) (Fig. 2d, e). Metastasis to the mesenteric lymph nodes was present in 2 cases, and hepatic metastasis was identified in 1 case. Although the primary neoplasm was not identified, the presumed enteric-origin adenocarcinoma was diagnosed based on the presence of metastatic carcinoma with goblet cell differentiation in a mesenteric lymph node.
Neoplasms of North American river otters.
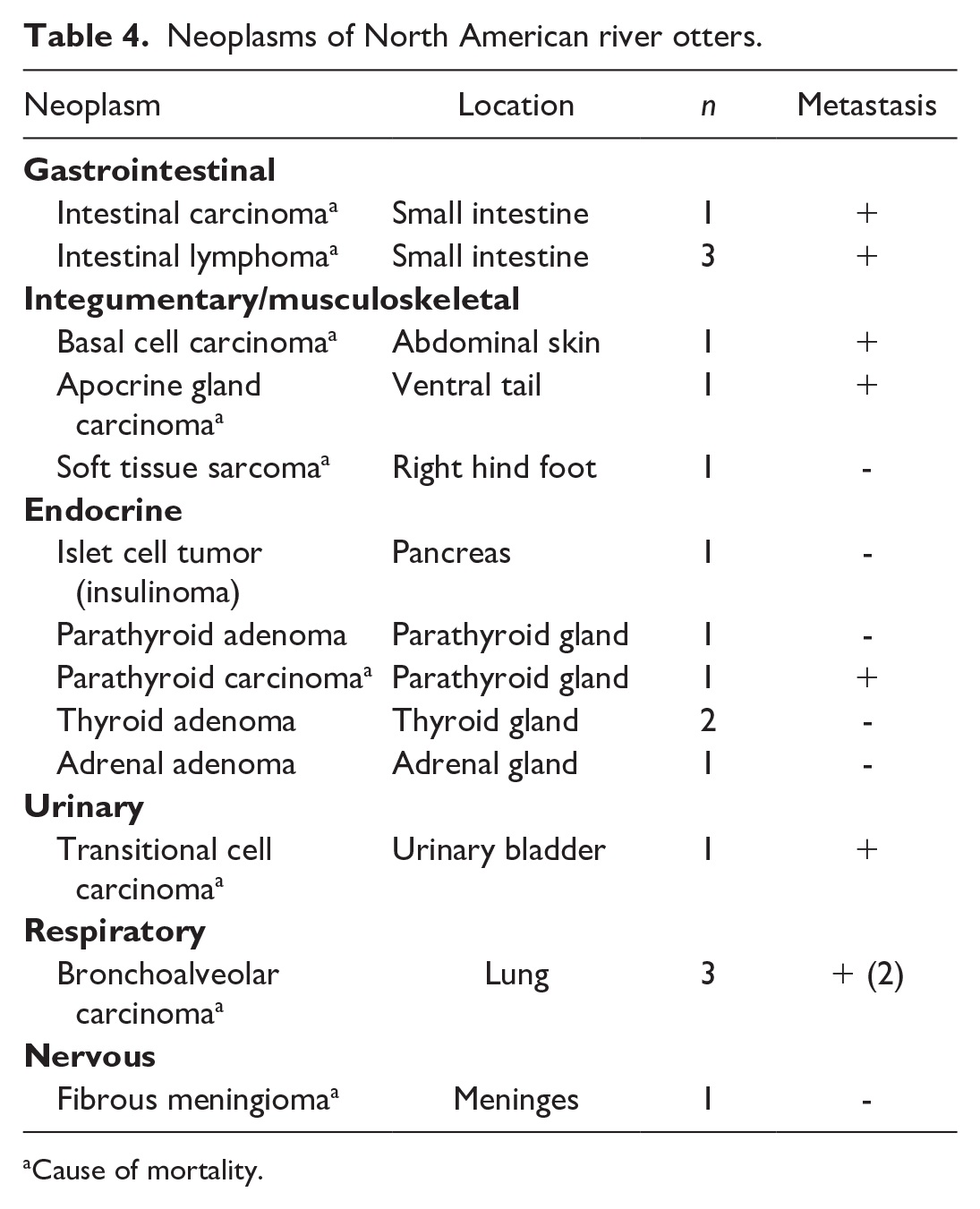
Cause of mortality.
Integumentary neoplasms were the second most common neoplastic cause of mortality, with 1 case each: fibrosarcoma (dorsal aspect of right hind foot), basal cell carcinoma (abdominal skin), and apocrine ductular carcinoma (ventral tail). The basal cell carcinoma and apocrine ductular carcinoma were both present in the same individual. Both had evidence of metastasis to the inguinal lymph nodes, and the basal cell carcinoma also metastasized to the lungs. No evidence of metastasis was identified for the fibrosarcoma.
Endocrine neoplasms resulting in euthanasia or that contributed to death included a parathyroid carcinoma and an insulinoma (individual had antemortem hypoglycemia) and were present in the same individual. This individual also had a bronchoalveolar carcinoma that was presumed incidental at the time of death. There were 2 additional individuals with bronchoalveolar carcinomas associated with regional lymph node or widespread metastases, including metastasis to the central nervous system.
Transitional cell carcinoma of the urinary bladder (Fig. 2f) associated with widespread visceral, muscular, and lymph node metastasis was the only neoplasm of the urinary tract identified in this species that resulted in death. Finally, there was 1 case of intracranial fibrous meningioma that led to cerebellar herniation and euthanasia.
Degenerative
Degenerative diseases (9 cases, 41%) directly associated with mortality affected the cardiovascular, musculoskeletal, and urinary systems.
Six (27%) otters died or were euthanized due to cardiac disease, all of which had evidence of myocardial, endocardial, and/or aortic fibrosis. Other cardiac lesions were arteriosclerosis (4 cases), valvular endocardiosis (2 cases), lymphoplasmacytic myocarditis (2 cases), and cardiac amyloid deposition (1 case). Interestingly, no NARO had cardiomegaly noted on gross examination. Two individuals had evidence of left-sided heart failure with pulmonary edema, pulmonary congestion, alveolar (interstitial) fibrosis, and intra-alveolar hemosiderin-laden macrophages (“heart-failure cells”). Lesions suggestive of right-sided congestive heart failure were seen in one of these otters and included pleural effusion, abdominal effusion, and chronic passive hepatic congestion.
Osteoarthritis or DJD was a primary cause of death in 4 (18%) otters: 1 with IVDD and 3 with DJD of appendicular joints. Specific joints were not described in 1 case. Vertebral (2 cases), stifle (2 cases), and tibiotarsal (1 case) joints were grossly affected with a spectrum of changes including patellar tendon mineralization, cartilage erosion or eburnation, joint capsule thickening, torn meniscus, and/or osteophyte formation. Moderate to severe, ventral, bridging bony proliferations consistent with spondylosis were described in thoracic (T9–15), lumbar (L1–3, L5–6), and lumbosacral joints (L7–S1). In the case of IVDD, there was disk degeneration with chronic herniations present between T1/T2, T2/T3, and T3/T4. Extra-articular lesions and clinical signs associated with DJD and IVDD included paw pad hyperkeratosis or erosion, ventral alopecia, hindlimb muscle atrophy, and unstable gait prior to euthanasia.
Three (14%) NARO died from CRD. One had evidence of nephrolithiasis; the stone was not submitted for composition analysis. The other 2 NARO had substantial glomerular and medullary interstitial amyloid deposition. The 2 NARO with renal amyloidosis also had amyloid in the heart, liver, mesenteric blood vessels, mesenteric lymph node, skeletal muscle, and esophageal lamina propria. Aside from kidney disease, no other areas of chronic inflammation or infection were identified in these individuals to account for secondary amyloidosis. Other observed urinary tract lesions were tubular degeneration and necrosis, tubular mineralization, tubular ectasia, interstitial fibrosis, mild neutrophilic tubulitis, and lymphocytic cystitis. Lesions attributed to terminal uremia included ulcerative esophagitis and myonecrosis with mineralization.
Inflammatory
Inflammatory diseases (2 cases, 9%) directly associated with mortality included 1 case of colonic perforation and 1 case of myocarditis with pulmonary vasculitis. Foreign body perforation was considered most plausible in the otter with the colonic perforation, as it was not associated with a primary infectious or inflammatory colitis. Bacterial peritonitis with heavy growth of Klebsiella pneumoniae and septicemia were sequelae to the perforation. In the case of myocarditis, regionally severe lymphoplasmacytic inflammation and necrosis were superimposed on chronic lesions such as myocardial fibrosis, valvular endocardiosis, and arteriosclerosis. Marked neutrophilic and lymphoplasmacytic panarteritis was associated with fibrinoid vascular necrosis and perivascular hemorrhage and edema. No infectious organisms were detected in these lesions. Differential diagnoses included terminal septicemia or immune-mediated disease such as polyarteritis nodosa.
Trauma and other causes of mortality
One case of exertional myopathy was identified. It occurred following immobilization for removal of a skin mass. There was myonecrosis in skeletal and cardiac muscles and associated myoglobin-induced nephropathy (Fig. 2g, h). Presumed breeding trauma with subsequent drowning resulted in the death of 1 female NARO. This individual had cutaneous puncture wounds on the head, lip lacerations, and hyperemic vulvar tissue.
Comorbidities
Comorbidities included CRD (16 cases), cardiovascular (12 cases) and pulmonary (12 cases) diseases, periodontal disease (7 cases), DJD (5 cases), and multiple benign hyperplastic (10 cases) or neoplastic (4 cases) processes. There was a high incidence of renal lesions in NARO that were not euthanized due to CRD, including renal fibrosis (9 cases), nephritis (8 cases), renal cysts (3 cases), tubular dilation (3 cases), tubular degeneration and necrosis (3 cases), amyloidosis (1 case), and nephrolithiasis (1 case). Similarly, NARO that died or were euthanized for other reasons had evidence of DJD (3 cases), cartilage erosion or eburnation (2 cases), spondylosis (2 cases), and IVDD (1 case). Joints affected included stifles, tibiotarsal, and elbow, and IVDD affected T13/14. Periodontal diseases were also identified as common comorbidities and included dental calculus (7 cases), dental attrition (3 cases), missing teeth (3 cases), gingival hyperplasia (2 cases), and tooth fractures (2 cases). Cardiovascular and pulmonary changes included arteriosclerosis +/− atherosclerosis (3 cases), endocardiosis (3 cases), pulmonary alveolar histiocytosis (3 cases), endogenous lipid pneumonia (5 cases), pulmonary edema (2 cases), myocardial degeneration (1 case), and myocardial fibrosis (1 case).
Multiple, presumed subclinical hyperplastic (Table 1) and benign neoplastic (Table 4) lesions were identified. Endocrine lesions were most common and included adrenal gland cortical nodular hyperplasia (5 cases) and adenoma (1 case), thyroid gland hyperplasia (1 case) and adenoma (2 cases), parathyroid gland hyperplasia (1 case), and adenoma (1 case). Other incidental hyperplastic changes were hepatic nodular hyperplasia/regeneration (2 cases), gallbladder cystic mucosal hyperplasia (2 cases), biliary hyperplasia (2 cases), and endometrial cystic hyperplasia (1 case).
Finally, thin body condition (3 cases), fat atrophy (7 cases), and muscle atrophy (2 cases) were noted in individuals with other concurrent disease processes and considered direct sequelae.
Discussion
This retrospective study identified causes of death and comorbidities in ASCOs and NAROs housed in multiple zoos and aquaria across the United States over a 20-year period. Notably, 41 of 71 (58%) ASCOs and 17 of 22 (77%) NAROs in this study were identified as older adults or geriatric, indicative of relatively long lifespans in managed care. Degenerative and neoplastic diseases were over-represented in both species, which was attributed to the older age of the study population. Thin body conditions, evidenced by fat and muscle atrophy, were likely sequelae to the myriad chronic, degenerative diseases related to advanced age.
In agreement with previous reports, urolithiasis, specifically nephrolithiasis, was common in ASCO (41 of 71; 58%) and a major cause of morbidity and mortality in 21 of 71 (30%) ASCOs in this study. Interestingly, uroliths were found in only 2 NAROs, highlighting ASCO’s predisposition to this disease. From 2000 to 2010, 28 ASCOs were confirmed with nephrolithiasis compared to 13 during 2011 to 2020, which suggests a decreased incidence over the study period. Of the 13 ASCOs in this later time period, 2 additionally had uroliths in the bladder, while no uroliths were documented from 2000 to 2010. Together these findings indicate a potential shift in nephrolithiasis epidemiology among ASCO in managed care, likely associated with diet changes to increase natural prey items such as crustaceans and fish, and decrease consumption of meat, eggs, and other animal proteins (personal communication, J. N. Langan). Nephrolithiasis has been long established in both male and female otters in managed care, particularly ASCO and Eurasian otters, and is thought to be multifactorial including nutritional, metabolic, and genetic factors.6,8,33,55 In 1 study, ASCO housed in North American zoos had the highest incidence of nephrolithiasis with over 62% affected, followed by European zoos (~13%) and Asian institutions (<10%). Age and dietary calcium were considered risk factors, while crude protein and sodium correlated with decreased stone formation. 55 Notably, ASCO fed a naturalistic crustacean-based diet for 2 years showed no progression of uroliths. 7 In ASCO, nephroliths are typically found bilaterally and are composed of calcium oxalate or urate.6,8,55 Of the 12 nephroliths analyzed in this study, most were composed of calcium oxalate monohydrate +/− ammonium urate, although a few had uric acid as a component, and 2 stones were 100% uric acid (Table 3). Uric acid stones occur in animals and humans eating a diet high in animal proteins; thus, dietary restriction of purines is recommended. 52 In addition to high protein intake, there are typically either concurrent bacterial urinary infections resulting in increased urease-splitting or due to mutations in the hypoxanthine-guanine-phosphoribosyltransferase pathway, causing excess degradation of purines. 52 It is unclear why some ASCO in this study developed uric acid instead of calcium oxalate nephrolithiasis, although differences in water sources and water quality have been speculated. Bilateral uric acid nephrolithiasis with associated ureteral hypertrophy was described in 1 free-ranging NARO without a known predisposing cause. 14 Analysis of stones in additional otter cases is important to determine potential causes. Further research with continued focus on nutrition and dietary components, and optimization to mimic diets of free-ranging populations, is required to fully elucidate mechanisms of nephrolithiasis in ASCO and other prone otter species. 37
In addition to nephrolithiasis, CRD was reported as a cause of mortality and a common comorbidity in both species. In ASCO, many of the tubular and interstitial lesions were secondary to chronic nephrolithiasis; however, in NARO, nephrolithiasis was found in only 2 individuals. Unlike ASCOs, NAROs had lesions centered on tubules and glomeruli, and 3 individuals had evidence of renal amyloidosis; thus, CRD pathogenesis in NARO appears distinct from that of ASCO. Interestingly, NARO had amyloid deposition in other organs, which suggests a predisposition to multisystemic amyloidosis, similar to the amyloid A amyloidosis described in martens. 1 Like many non-domestic species in managed care, the underlying pathogenesis of renal disease in ASCO and NARO is not fully understood. Advanced ages of zoo-housed individuals compared to free-ranging individuals, and concurrent comorbidities (nephrolithiasis and cardiovascular disease) that may exacerbate CRD, are likely major influences given the lack of degenerative renal lesions documented in wild animals.
DJD (osteoarthritis) was a significant cause of morbidity and often a factor for euthanasia in ASCO (13%) and NARO (18%). Stifle joints were commonly affected in both species, and IVDD of the caudal thoracic and lumbar regions negatively impacted the quality of life, based on clinical reports of pain and decreased mobility. These lesions were seen in older adult and geriatric otters, and many individuals had one or more comorbidities, also contributing to end-of-life decisions. 10 Osteoarthritis has previously been reported in a group of ASCO, sea otters, and NARO.2,10,20,40 Although the literature is sparse regarding this disease process in otter species, DJD is generally considered progressive, requiring medical, husbandry, and habitat management as the animal ages, as in many other veterinary patients. 26
Cardiovascular lesions were frequently reported in ASCO and NARO, and in total, 10 of 93 (11%) otters died or were euthanized due to cardiac insufficiency and failure. Gross and histologic lesions were varied, although cardiomegaly and ventricular hypertrophy and dilatation were only noted in ASCO, and arteriosclerosis and aortic fibrosis were more common in NARO. All ASCOs with cardiac disease as a primary cause of death had biventricular heart failure, whereas NAROs with cardiac disease had right- (2 cases) or left-sided (1 case) congestive heart failure. Cardiomyopathy has been reported in these species; however, the overall prevalence is unknown. 3 In previous studies, cardiomyopathy was reported to be the third most common cause of death in free-ranging Southern sea otters (Enhydra lutris nereis) with documented contributory protozoal (Toxoplasma gondii, Sarcocystis neurona), toxic (domoic acid), and to a lesser extent nutritional etiologies. 24 A diagnosis of dilatative cardiomyopathy usually indicates end-stage disease. Thiamine deficiency, as documented in cats, has been purported as a possible factor, particularly in otters fed diets composed exclusively of fish species (eg, carp, roach, herring, mackerel, and smelt) with higher thiaminase activity. 3 Other Musteloidea superfamily members, eg, domestic ferrets (Mustela putorius furo) and striped skunks (Mephitis mephitis), under human care also have a predilection for primary cardiac disease, with obesity, genetics, and/or advanced age all speculated as contributing factors.5,53 As for prevention of nephrolithiasis, diets of otters in managed care should incorporate varied prey items, like those encountered in natural settings, in order to optimize cardiovascular health. Furthermore, routine cardiac evaluations would be beneficial to better understand cardiovascular disease in both species and possibly improve current therapeutic strategies to delay heart-failure symptoms and sequelae.
Neoplasia was the cause of death or euthanasia in 19 (47%) ASCOs and 10 (45%) NAROs. Notably, not all histologically malignant neoplasms were the primary cause of death. For example, hepatocellular carcinoma, exocrine carcinoma, transitional cell carcinoma, and splenic sarcoma were diagnosed and considered comorbidities in ASCO (Table 3). In ASCO, malignant neoplasms that were linked to mortality were found in every organ system, although integumentary, mammary, gastrointestinal, endocrine, and hemic-lymphatic systems were most common. There were 16 cases of metastatic or disseminated diseases in ASCO and 10 neoplasms with metastatic disease in NARO. The median ages of ASCO and NARO with disseminated neoplastic diseases were 17 and 14, respectively, indicating advanced age as a factor in its development.
Integumentary neoplasms included 3 malignant melanomas (all ASCO), 2 soft tissue sarcomas, and 1 each of squamous cell carcinoma, apocrine gland carcinoma, and basal cell carcinoma. One NARO had both apocrine gland and basal cell carcinomas with concurrent metastases. A malignant integumentary basal cell tumor with apocrine differentiation and metastasis was recently reported in a zoo-housed cape clawless otter (Aonyx capensis). 28 All 4 cases of malignant mammary gland neoplasia were in ASCO and were associated with metastatic disease at the time of euthanasia, consistent with previous reports. 25 Interestingly, NARO had 3 cases of intestinal lymphoma, including 2 suspected and 1 confirmed small T-cell lymphoma, which has been recently reported in an ASCO and an Eurasian otter.4,34 Splenic lymphoma was found in 2 ASCOs, adding to previous reports.22,42
Undifferentiated neuroendocrine neoplasms were found in the abdominal cavity of 2 ASCO; both were malignant and disseminated throughout. Disseminated pheochromocytoma has been described in a zoo-housed NARO and was suspected, although not confirmed, in 1 ASCO from the current study population. 38 Benign or subclinical neoplastic disease was most often of endocrine origin, likely representing a spectrum of endocrinopathies. Hyperplasia of thyroid, parathyroid, and adrenal glands was common in both species. Clinicopathologic correlations were not investigated in most cases, although there was 1 case of hypoglycemia in an otter with an insulinoma.
Interestingly, 3 ASCOs and 3 NAROs had bronchoalveolar neoplasms, 5 of which were malignant, and 3 of which were metastatic. Bronchoalveolar carcinomas, like all primary lung tumors, are generally rare in animals compared to humans. One case of primary pulmonary bronchoalveolar carcinoma in a zoo-housed NARO was associated with pulmonary silicosis; no evidence of silicosis or concurrent pulmonary disease was seen in the otters with bronchoalveolar neoplasms from this study cohort. 43 Risk factors found in dogs include advanced age and breed; environmental factors such as air pollution have not been linked with increased incidence of lung neoplasia as seen in humans. 36 In dogs, longer survival times have been reported in cases of primary pulmonary neoplasia with intrathoracic nodal metastases compared to distant metastatic disease, particularly with surgical interventions. 36 An adult free-ranging NARO was diagnosed with a primary pleural squamous cell carcinoma using immunohistochemical markers; thus, primary lung tumors may be specific to this species. 49
Although there were several soft tissue neoplasms, primary bone malignancies were not reported in either species of this study group. One ASCO had a digit with a regionally invasive melanoma, and an NARO had a soft tissue sarcoma affecting the right hind foot. There has been a single case of lymphangiosarcoma invading lumbar vertebral bones and nerve roots, resulting in osteolysis and paresis in a 10-year-old ASCO. 44
Several ASCOs died due to acute gastrointestinal hemorrhage, and the underlying cause was not confirmed in any of the cases, as no primary areas of inflammation, ulceration, or ruptured vessels to account for the luminal hemorrhages were identified grossly or histologically. Hemorrhagic enteropathies are reported in both river otters and sea otters. These are characterized by mucosal, submucosal, and luminal hemorrhage in the intestinal tract and can progress to fatalities resulting from shock, stress, hypovolemia, or insufficient cardiac function. Interestingly, most of the affected otters from this study had concurrent primary causes of death or comorbidities including CRD, malignant neoplasia, bacterial infection, congestive heart failure, and/or had been anesthetized the day of or within a few days of death. Two individuals had no primary cause of death other than the hemorrhage. There was a reported outbreak of canine parvovirus-2b and C. difficile in a group of juvenile (6- to 24-month-old) ASCO, which died of severe gastrointestinal disease. 50 Although intestinal contents in these juvenile otters included some hemorrhage, parvovirus and C. difficile were not considered as causes of hemorrhagic disease in this study given the lack of supportive histologic findings and detection of organisms and the age of affected individuals. However, hemorrhagic enteropathies may be associated with dysbiosis and increased clostridial-like spore-forming bacilli on fecal cytology. 19 Further evaluation of cases of massive luminal gastrointestinal hemorrhage in ASCO including potential risk factors, signalment, concurrent disease, age, sex, diet, potential toxin exposures, antemortem blood parameters, and anesthetic protocols is warranted to better understand or elucidate potential contributing etiologies.
One NARO had capture (exertional) myopathy with confirmed myoglobin casts in renal tubules. Capture myopathy has been documented in free-ranging and managed otters and is a stress response from handling, transport, and capture.15,18 Serum biochemistry will show elevations in enzymes such as creatine kinase, aspartate aminotransferase, and lactate dehydrogenase, which can cause muscle necrosis both at a gross and cellular level. Toxic causes of death in this study group were limited to ingestion of 1 to 4 phenylenediamine through self- and conspecific grooming in 2 ASCOs that ingested Nyanzol-D hair dye, which was used for identification purposes. Other cases of toxicity in ASCO and NARO under human care that have been previously published include melarsomine dihydrochloride toxicity in an otter under heartworm treatment and cyanide toxicity from loquat (Eriobotrya japonica) seed ingestion.29,51
Overall, inflammatory and infectious diseases were not a predominant cause of mortality in the study population, although there were several cases of bacterial pneumonia, pyelonephritis, or septicemia secondary to wounds, gastrointestinal or reproductive compromise/infection, or soft tissue infections. Bacterial etiologies were mostly limited to enteric or opportunistic pathogens, although species identification through culture or molecular analyses was not completed for all cases. Some fatal bacterial infections were seen in older otters with 2 or more other disease processes. Fatal peritonitis and necrotizing hepatitis due to Pasteurella multocida were recently reported in a 12-year-old female ASCO with nephrolithiasis and pyometra. 27 Thus, otters of advanced age with comorbidities may be predisposed to potentially fatal bacterial infections.
Not surprisingly, no mortalities or significant morbidity due to endoparasitism or confirmed viral disease were identified in this study group. This is presumably due to structured prophylactic vaccination and anthelmintic treatment protocols as well as known health and environmental parameters (healthy enclosure mates, minimal native wildlife interactions, food safety, and preventative medical exams) in otters under managed care. There are, however, a few published cases of fatal or clinically significant parasitism in these otter species under human care including severe visceral pentastomiasis in a geriatric ASCO with concurrent thyroid neoplasia and cystoisosporiasis (Cystoisospora sp.) associated with diarrhea in juvenile ASCO.16,47 While there have been reports of patent infections of Dirofilaria immitis in European otters, only nonpatent, single-sex cases of dirofilariasis have been described in NARO and ASCO.21,32,41,48 Multiple viral diseases have been described affecting free-ranging and captively held NARO and ASCO. 50 Aside from 1 NARO with CRD, osteoarthritis, and suspected concurrent viral meningitis, viral-associated disease was not found in necropsies for animals from institutions in this study. In 2020, the SARS-CoV-2 global pandemic changed husbandry and medical protocols for otters and like species due to their relative susceptibility to SARS-CoV-2 infection and evidence of spillover from humans to managed and free-ranging otters.9,31 Thus, despite the findings in this 20-year review, viral diseases will continue to be investigated in ASCO, NARO, and other otter species.
This comprehensive review of gross and histologic lesions of ASCO and NARO from several US institutions provides a broad foundation of pathology data, from which additional or improved husbandry, nutritional, diagnostic, and treatment protocols may be developed and implemented. In addition, further surveillance and investigations to better elucidate pathogeneses of common diseases will be beneficial for management of ASCO, NARO, and related species in managed care and free-ranging populations.
Footnotes
Acknowledgements
We thank the husbandry and veterinary staff at the contributing institutions for their optimal care of the otters in this study. We thank the pathologists and diagnosticians for the initial case workup and the histology laboratory technicians and diagnostic lab personnel for their assistance and technical expertise.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.