
Abstract
Fibromatous epulis of periodontal ligament origin (FEPLO), also known as peripheral odontogenic fibroma (POF), is a benign gingival lesion that occurs frequently in dogs. Common use of both names is cumbersome and confusing yet persists due to disagreement regarding pathogenesis. With the objective of clarifying the histogenesis and pathogenesis, 100 canine FEPLO/POF lesions that had been surgically excised en bloc were evaluated histologically to characterize the lesion’s relationship to surrounding anatomic structures and to document concurrent pathologies in those tissues. No lesions involved the periodontal ligament space, although 88/100 (88%) lesions attached to alveolar bone, similar to the normal anatomy of the gingival ligament. The lesions consist of fibrous tissue with osteogenic potential, and 54/100 (54%) lesions had bone or cemento-osseous matrix. Odontogenic epithelium was evident in 63/100 (63%) lesions, and the paradental location of the epithelium suggests that the origin of most odontogenic epithelium in FEPLO/POF lesions is a result of hyperplastic junctional epithelium extending into the lesion. Hypercellularity was interpreted as a feature of reactive lesions since 15/17 (88%) hypercellular lesions were ulcerated and 15/17 (88%) were inflamed. Frequent concurrent histologic findings included hypercementosis at the cementoenamel junction of the adjacent tooth (79/89, 89%), reactive alveolar bone (90/100, 90%), and inflammation of alveolar bone (67/100, 67%). While the pathogenesis cannot be determined with absolute certainty, available evidence supports a reactive, hyperplastic process rather than neoplastic. The authors believe that fibromatous hyperplasia of the gingival ligament is an anatomically correct name that accurately reflects the likely etiopathogenesis.
Keywords
Fibromatous epulis of periodontal ligament origin (FEPLO) in dogs was described in the late 1950s as a tumor-like fibrous gingival mass.10,11 The early literature is often unclear about “epulides” in dogs, providing confusing or contradictory features for lesions that included fibrous epulis, ossifying epulis, giant cell epulis, acanthomatous epulis, and focal fibrous hyperplasia. It was not until 1979 that FEPLO, including those with ossification, was clearly differentiated from canine acanthomatous ameloblastoma. 6 In this article, Dubielzig et al 6 described FEPLO as “a fibrous lesion derived from the periodontal ligament (PDL) that does not invade bone.” This definition, and the lesion name itself, represents an inherent contradiction since a lesion that does not exist within bone cannot arise from the PDL. This contradiction was largely ignored because the histology of the lesion is characteristic of PDL and because the lesion typically has continuity with the coronal edge of the PDL. Although seldom identified as a distinct anatomic structure, the gingival ligament is specialized fibrous tissue with osteogenic potential that is histologically identical to the PDL yet exists peripheral to alveolar bone. 21 The gingival ligament serves to attach gingiva to bone of the alveolar margin and attaches gingiva to the tooth near the cementoenamel junction (CEJ). 21
Like the PDL, the gingival ligament is derived from odontogenic ectomesenchyme of the dental follicle. During the process of tooth eruption, a portion of both the odontogenic ectomesenchyme and the reduced enamel epithelium contribute to the inner portion of the gingiva, forming the gingival ligament and the junctional epithelium, respectively (Fig. 1). 21 Thus, both the gingival ligament and the junctional epithelium are of odontogenic tissue origin and part of the periodontal apparatus even though, following complete eruption of a tooth, these tissues are components of the gingiva and entirely peripheral to alveolar bone. 20
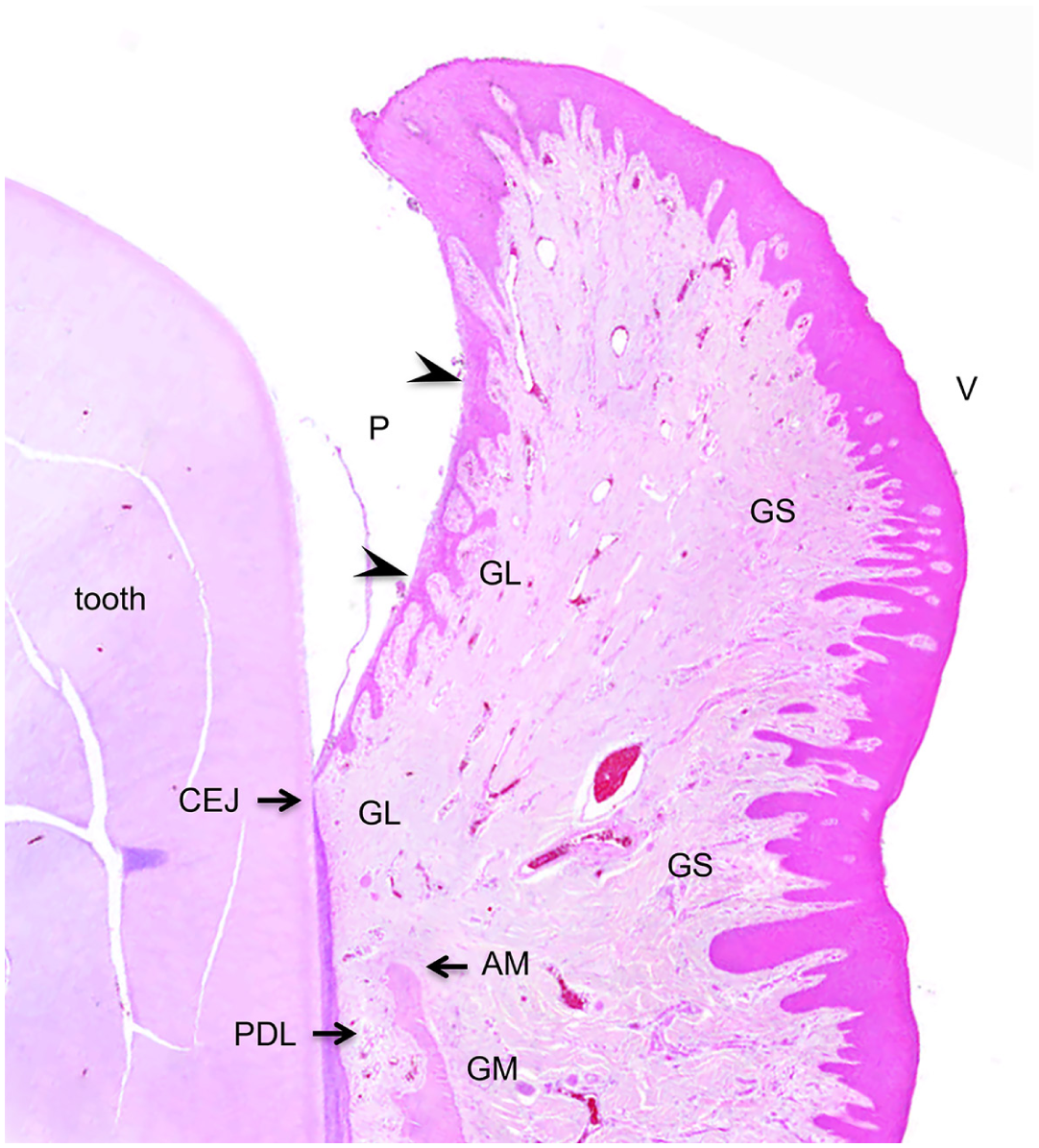
Normal gingiva, dog. Junctional epithelium (arrowheads) lines the paradental (P) surface while typical gingival epithelium covers the vestibular (V) surface. The gingival ligament (GL) attaches gingiva to bone at the alveolar margin (AM) and gingiva to tooth at the cementoenamel junction (CEJ). The gingival mucoperiosteum (GM) attaches the dense fibrous gingival stroma (GS) to the vestibular surface of alveolar bone. The periodontal ligament (PDL) occupies a narrow space between alveolar bone and cementum on the tooth root surface. Hematoxylin and eosin.
During the late 1980s and early 1990s, studies argued that FEPLO in dogs was analogous to peripheral odontogenic fibroma (POF), which is an uncommon odontogenic tumor of humans.5,9 However, this proposal was not without opposition. For example, Reichart et al 22 stated, “. . . the canine lesion is a form of hyperplasia that seems to have no human counterpart” and “reclassification [as POF] adds to nomenclatural chaos.” Nevertheless, use of POF instead of FEPLO in an influential 1992 study of canine epulides has had lasting effects, particularly within the veterinary dental community. 28 These authors reclassified all “fibromatous and ossifying epulides” as either “focal fibrous hyperplasia” or “peripheral odontogenic fibroma (WHO type).” 28 Although a goal of the publication was to eliminate use of FEPLO, this terminology persists and is favored by some pathologists who reject POF. Many pathologists continue to use both names, referring to the lesions as FEPLO/POF. Since that time, POF has been used for lesions in other veterinary species, including cats and horses.14,27
FEPLO/POF is remarkably common in dogs and therefore a clinically and economically important lesion despite its benignity and limited impact on patient morbidity. Studies have characterized lesion location and patient signalment.2,8,23 Histomorphologic studies of FEPLO/POF in dogs have characterized typical and hypercellular lesions.5,6,12,15,28 However, no previous study has specifically evaluated the relationship of the lesion to the surrounding anatomic structures. The study described here was designed to evaluate 100 FEPLO/POF lesions that had been excised en bloc. Investigators hypothesized that characterization of the lesion’s anatomic relationship to adjacent tissues and documentation of concurrent pathologies would inform the histogenesis and pathogenesis of FEPLO/POF.
Materials and Methods
Sample Collection
A retrospective case series utilized 100 oral lesions from client-owned dogs that had been diagnosed as FEPLO/POF and excised en bloc. Cases that met these criteria were selected sequentially from the database of Specialty Oral Pathology for Animals between May 2023 and February 2024. Written or verbal consent from the dog owners was not required for inclusion in the study. For the purpose of the study, en bloc excision was necessary so that histologic sections available for evaluation had spatially preserved architecture of surrounding tissue (gingiva, PDL, and alveolar bone). This study did not attempt to determine the reason for en bloc excision or whether lesions had been previously diagnosed by incisional biopsy; these details were considered to be beyond the focus of the study, which was to evaluate histologic morphology of lesions. An additional 300 lesions from dogs with the diagnosis of FEPLO/POF, including both incisional and excisional biopsy samples from the same time period, were evaluated only for lesion location.
Clinical information collected from the selected cases included demographic data (breed, age, and sex), lesion location, lesion size, presence of tooth displacement, and presence of multifocal/generalized gingival hyperplasia. Lesion size was taken from the pathology report since mass lesions were routinely measured in 3 dimensions during gross evaluation of specimens. Evaluation of gingival hyperplasia was aided by clinical photographs. Evaluation of tooth displacement was aided by clinical photographs and/or diagnostic imaging (intraoral radiographs or cone beam computed tomography). However, clinical photographs and diagnostic imaging were not available for all cases. Lesion location was recorded by quadrant and as either rostral (mass centered on a canine or incisor tooth) or caudal (mass centered on a premolar or molar tooth).
Follow-up information was limited to whether or not the lesion had recurred and the most recent date that lack of recurrence was determined. This outcome information was sought by contacting each veterinary practice that had submitted a lesion included in the study. Confirmation of recurrence or lack of recurrence was based on either a veterinarian’s oral exam or information conveyed by the dog’s owner.
Histomorphologic Evaluation
Tissues were received in 10% neutral-buffered formalin and decalcified by immersion in 10% hydrochloric acid solution for a minimum of 4 hours and maximum of 36 hours, depending on the amount of bone and tooth material present in sampled sections. Tissues were processed routinely, embedded in paraffin, sectioned at 5 µm, and stained with hematoxylin and eosin. A single tissue section was evaluated unless multiple sections were necessary for margin evaluation. Recut sections were prepared if necessary to ensure adequate slide quality. Recorded histologic findings included the following: location of the base of the lesion relative to the CEJ, contact of the base of the mass with the alveolar bone margin (yes/no), extension of the lesion to the mucogingival junction (yes/no), presence of odontogenic epithelium (yes/no), distribution of odontogenic epithelium (diffuse, vestibular, and paradental), certain distinctive features of odontogenic epithelium (cyst formation, keratinization, and pigmentation), inflammation within the mass (yes/no), presence of bone or cemento-osseous matrix (yes/no), continuity of bone within the mass with bone of the alveolar margin (yes/no), hypercellularity of the lesion, ulceration of the mass, invasion of the PDL space (yes/no), specific changes within the PDL space (normal, disrupted by periodontal inflammation, effaced by cemento-osseous remodeling), evidence of alveolar osteoproliferation/hyperostosis (yes/no), evidence of alveolar osteolysis/bone loss (yes/no), evidence of reactive alveolar bone (yes/no), invasion of alveolar bone (yes/no), presence of inflammation within alveolar bone (yes/no), presence of hypercementosis at the CEJ (yes/no), and evidence of adjacent tooth resorption (yes/no). When available, intraoral radiographs were also used to evaluate for tooth resorption.
The presence of odontogenic epithelium was defined as isolated islands or cords of epithelium within the fibrous tissue of the mass. Hypercellularity was judged subjectively based on increased density of mesenchymal cells and decreased abundance of collagen matrix.12,15 Inflammation within the mass was considered to be positive if inflammatory cells, typically lymphocytes and plasma cells, were distributed throughout at least 40% of the mass. Lesions that had inflammatory cells limited to the paradental/sulcular surface were recorded as negative. Lesional fibrous tissue causing widening or effacement of tissue between alveolar bone and the adjacent tooth root was considered to be positive evidence of PDL space invasion. Evidence of alveolar osteoproliferation was defined as increased amount of bone resulting in either increased thickness of bone at the alveolar margin or increased height of the alveolar margin. Evidence of alveolar osteolysis/bone loss was defined as absence of bone or decreased height of the alveolar margin. Evidence of reactive alveolar bone included alteration of trabecular organization resulting in increased density of bone (osteosclerosis), intermingling of woven bone with lamellar bone, and/or bone having irregular reversal lines. Positive evidence of alveolar bone invasion required the presence of lesional fibrous tissue between bony trabeculae of preexisting bone or replacement of bone deep to the alveolar margin. The presence of lesional fibrous tissue between bony trabeculae superficial to the alveolar margin was not interpreted as alveolar bone invasion regardless of the maturity of bone. All slides were evaluated by the same board-certified veterinary pathologist (CB). Tabulated data analyzed in this study are available in the Supplemental Materials (Supplemental Table S1).
Statistical Analysis
The associations between continuous variables (lesion size) and categorical variables (involvement of the mucogingival junction, hypercellularity, intralesional bone, and tooth displacement) were evaluated using binary logistic regression models, with categorical variables as the outcome variable. Lesion size (cm3) was treated as a continuous predictor and log-transformed prior to analysis, due to a right skewed distribution pattern. Results were reported as odds ratios with 95% confidence intervals (CIs). Model performance was assessed using receiver operating characteristic curve analysis and the Hosmer-Lemeshow goodness-of-fit test. The associations between lesion ulceration and lesion hypercellularity as well as between lesion inflammation and lesion hypercellularity were evaluated using two-sided Fisher’s exact test. All variables were analyzed as binary categorical outcomes and contingency tables were constructed for each comparison. All analyses were performed in GraphPad Prism version 10.6.1, and statistical significance was set at P < .05.
Results
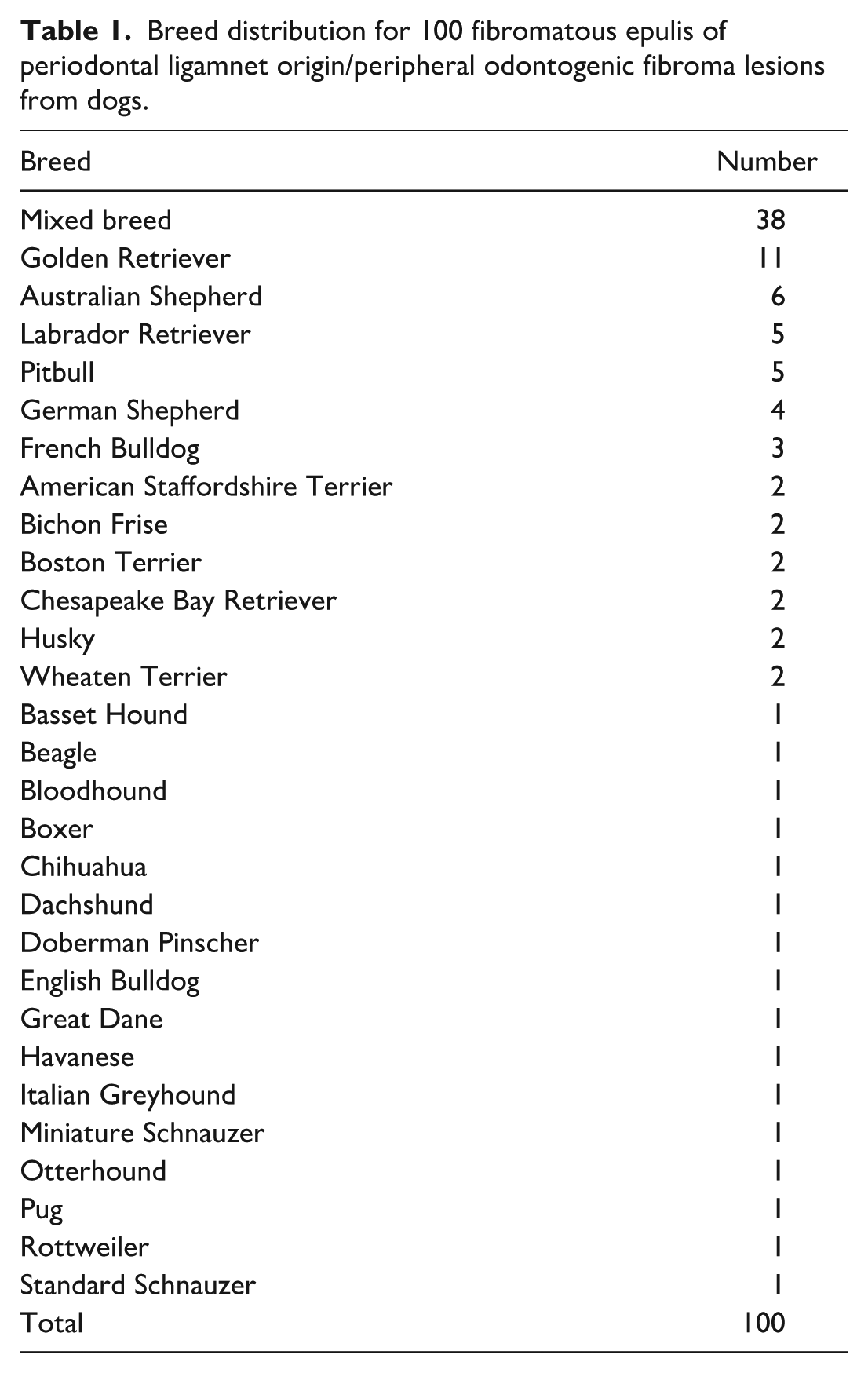
The age range of dogs in the study population was 2 to 13.5 years with an average of 7.3 years and median of 7 years. There were 57 neutered males, 39 neutered females, 2 intact males, and 2 intact females. Mixed breed was most common breed (38%) followed by Golden Retriever (11%). All breeds and respective numbers are provided in Table 1, and the presence or absence of many morphologic parameters are summarized in Table 2.
Breed distribution for 100 fibromatous epulis of periodontal ligamnet origin/peripheral odontogenic fibroma lesions from dogs.
Histomorphologic findings of 100 fibromatous epulis of periodontal ligament origin/peripheral odontogenic fibroma lesions from dogs.
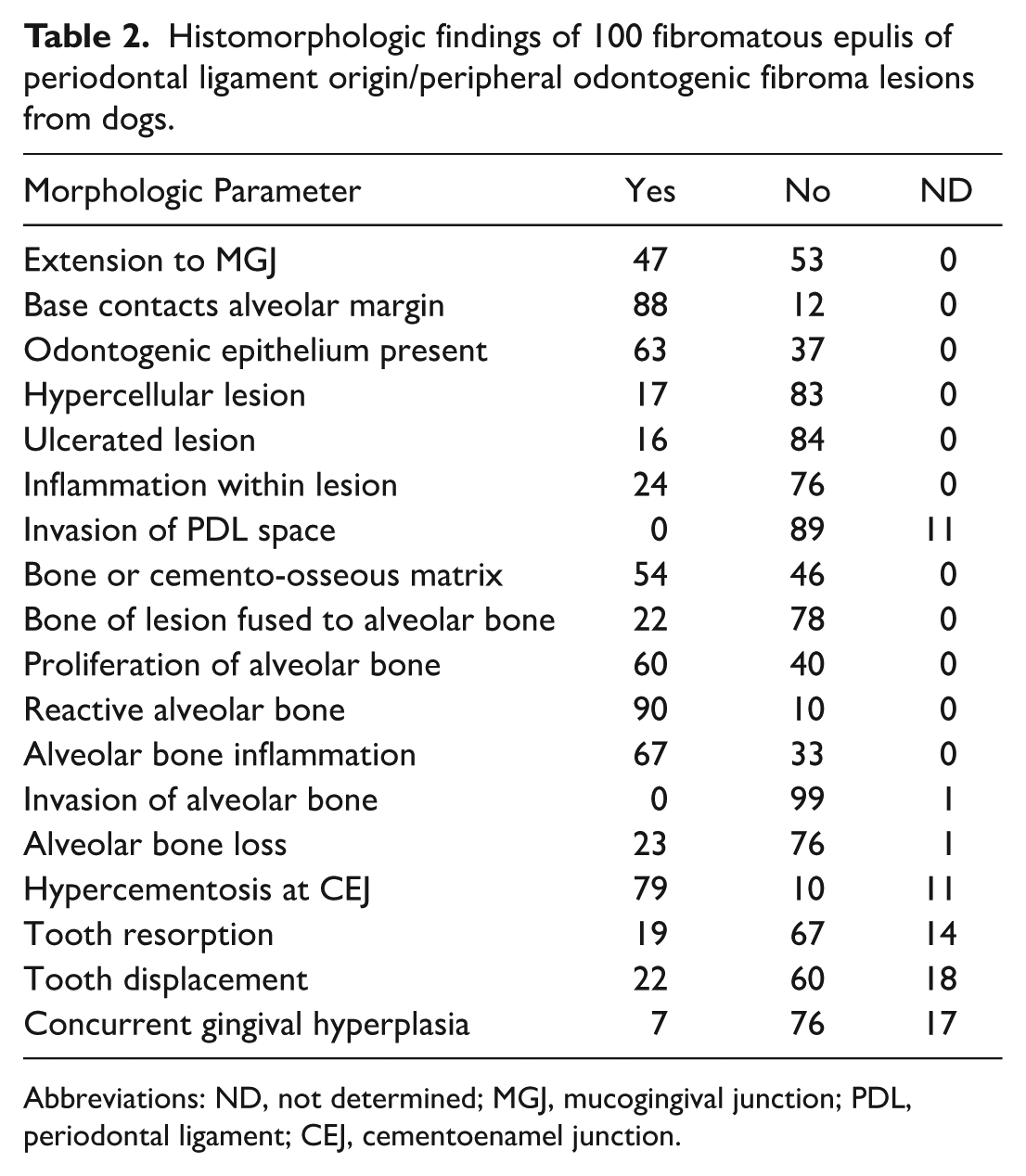
Abbreviations: ND, not determined; MGJ, mucogingival junction; PDL, periodontal ligament; CEJ, cementoenamel junction.
The distribution of lesions was nearly equal between the maxilla and mandible. For the 100 lesions that were excised en bloc, more were rostral (61%) and fewer were caudal (39%). However, data from 400 cases showed nearly equal distribution between rostral and caudal lesions with a distribution of 26.5% in the rostral maxilla (105/400), 20.0% in the rostral mandible (80/400), 27.25% in the caudal maxilla (109/400), and 26.25% in the caudal mandible (106/400) (Fig. 2). Thirty (30%) of the en bloc lesions involved a canine tooth, and 8 of the 10 largest lesions occurred at a canine tooth. The size of lesions ranged from 0.036 to 19.4 cm3 with an average of 2.94 cm3 and median of 1.32 cm3. All lesions were confined to the gingiva; 88% of lesions extended to the alveolar bone margin and 47% extended to the mucogingival junction (Fig. 3a, b). For those that did not extend to the alveolar bone margin, the base of the lesion was more superficial, within the gingiva. The average size of lesions that extended to the mucogingival junction was 4.32 cm3 (range 0.056–19.4 cm3) versus 1.72 cm3 (range 0.036–17.9 cm3) for those that did not extend to the mucogingival junction. Logistic regression demonstrated a significant positive association between lesion size and extension to the mucogingival junction. After log transformation of lesion size, increasing lesion size was associated with markedly increased odds of mucogingival involvement (β = 1.646, 95% CI 0.842–2.572), corresponding to an odds ratio of 5.19 (95% CI 2.32–13.10, P < .0001).
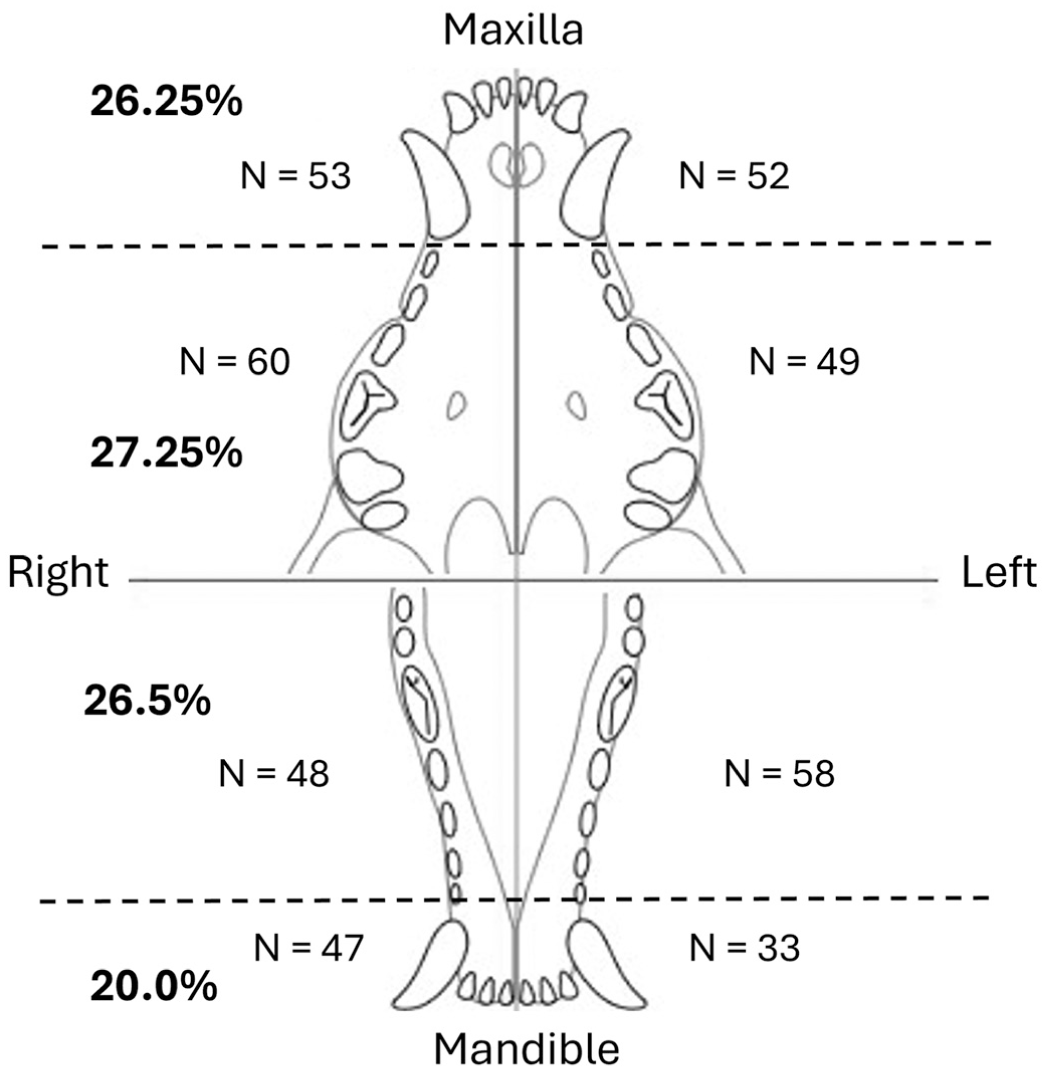
Distribution of 400 fibromatous epulis of periodontal ligament origin (FEPLO)/peripheral odontogenic fibroma (POF) lesions from dogs.
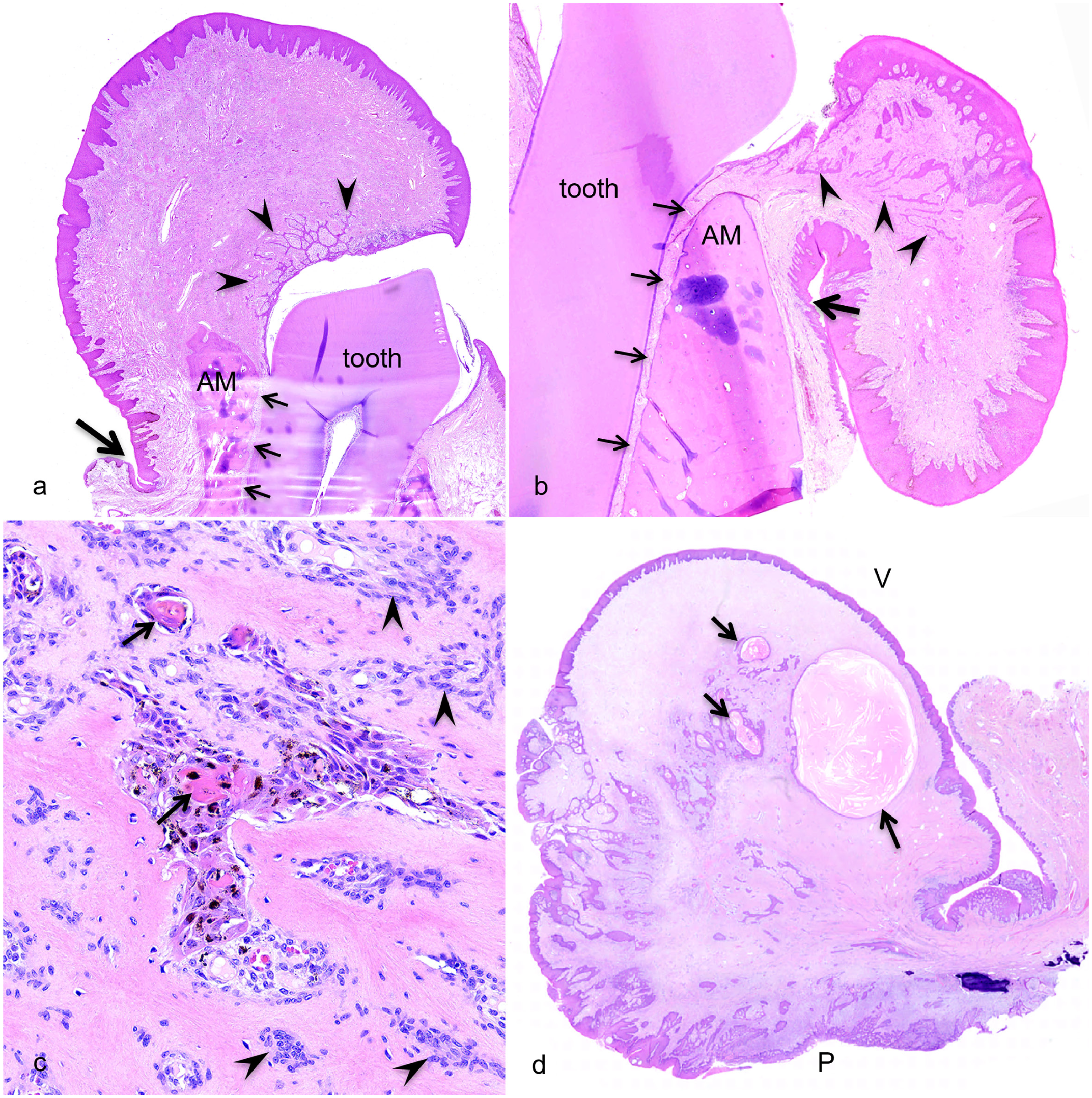
Fibromatous epulis of periodontal ligament origin (FEPLO)/peripheral odontogenic fibroma (POF) lesions from the gingiva of dogs. Hematoxylin and eosin. (a, b) Each lesion has fibrous tissue of the mass attaching to the alveolar bone margin (AM) and neither extends to the mucogingival junction (large arrow) or invades the periodontal ligament space (small arrows). The distribution of odontogenic epithelium (arrowheads) is paradental. (c) Islands of odontogenic epithelium have small foci of keratinized squamous cells (arrows) and black melanin pigment within the cytoplasm of some epithelial cells. Note the uneven spacing of mesenchymal cells (arrowheads) in this hypercellular lesion. (d) A lesion with multiple cysts (arrows) that are lined by odontogenic epithelium. Odontogenic epithelium is diffusely distributed throughout the mass yet more closely associated with hyperplastic rete pegs of junctional epithelium on the paradental side of the mass (P). The vestibular surface of the mass (V) has smooth gingival epithelium that does not anastomose with odontogenic epithelium.
Odontogenic epithelium was confirmed to be present in 63% of the lesions and was not identified in histologic sections for 37% of the lesions. For lesions with odontogenic epithelium, the distribution was determined to be diffuse in 29/63 lesions (46%) and paradental in 34/63 lesions (54%) (Fig. 3a, b). None of the lesions had a vestibular distribution of epithelium. Five lesions had keratinization of odontogenic epithelium, and two of these also had melanin pigment within the cytoplasm of epithelial cells (Fig. 3c). One lesion had cysts lined by odontogenic epithelium (Fig. 3d).
Hypercellularity was a feature of 17 lesions (17%) (Supplemental Figure S1), ulceration was noted for 16 lesions (16%), and inflammation was recorded for 24 lesions. Of the hypercellular lesions, 15/17 (88%) were ulcerated, and 15/17 (88%) had inflammation. A significant association was identified between lesion ulceration and lesion hypercellularity (P < .0001). Using ulceration as a predictor of hypercellularity, sensitivity was 88%, and the specificity was 99%, with a positive predictive value of 94% and a negative predictive value of 98%. A significant association was also observed between lesion inflammation and lesion hypercellularity (P < .0001). When inflammation was used as a predictor of hypercellularity, the sensitivity was 88% and specificity was 89%, with a positive predictive value of 63% and a negative predictive value of 97%.
An average lesion size of 7.06 cm3 (range 0.96–19.4 cm3) was recorded for hypercellular lesions and average size of 2.10 cm3 (range 0.036–15.0 cm3) was recorded for lesions that were not hypercellular. Logistic regression demonstrated a strong positive association between lesion size and hypercellularity. After log transformation of the lesion size, increasing lesion size was associated with markedly increased odds of hypercellularity (β = 2.679, 95% CI 1.408–4.246), corresponding to an odds ratio of 14.6 (95% CI 4.09–69.82, P < .0001). Although the pattern of mesenchymal cell organization was not recorded for each case, a subjective observation was that areas of hypercellularity tended to occur in proximity to ulcerated surfaces and to have streaming spindle cells rather than uniformly spaced cells with stellate morphology (Fig. 4).
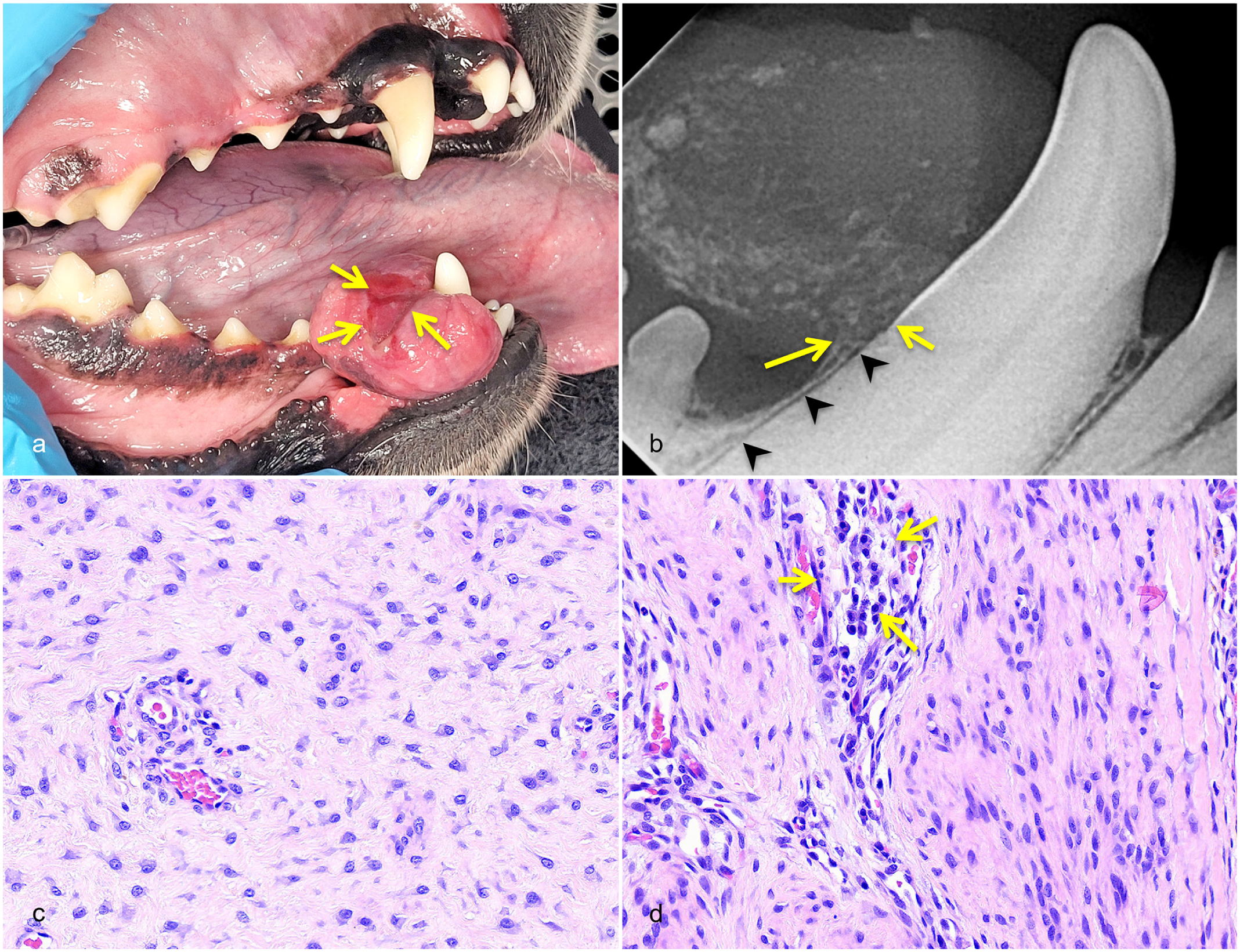
Fibromatous epulis of periodontal ligament origin (FEPLO)/peripheral odontogenic fibroma (POF), gingiva, dog. (a) Grossly, the mass is distal to the right mandibular canine tooth (404) and has an area of ulceration (arrows) that correspond to the site of occlusion by the right maxillary canine tooth. (b) An intraoral radiograph of the lesion shows small mineral opacities throughout the mass, which has a narrow base at the cementoenamel junction (short arrow) and alveolar bone margin (long arrow). The periodontal ligament space (arrowheads) is normally uniform and narrow. (c) An area of the lesion with stellate cells evenly spaced among fine collagen fibers. Hematoxylin and eosin (HE). (d) A more cellular and inflamed area of the lesion, near the ulcerated surface, has more closely spaced spindle cells that stream along collagen fibers and greater numbers of perivascular lymphocytes and plasma cells (arrows). HE.
Cemento-osseous matrix or bone, including both woven and lamellar bone, was present in 54 of 100 lesions. Bone within the lesion was continuous with (fused to) subjacent alveolar bone in 22/54 (41%) of those that had bone. Lesions with bone had an average size of 4.16 cm3 (range 0.16–19.4 cm3) and lesions without bone or cemento-osseous matrix had an average size of 1.50 cm3 (range 0.036–15.0 cm3). Logistic regression demonstrated a significant positive association between lesion size and the presence of bone within the lesion. After log transformation of the lesion size, increasing lesion size was associated with substantially increased odds of bone involvement (β = 1.642, 95% CI 0.843–2.563), corresponding to an odds ratio of 5.16 (95% CI 2.32–12.97, P < .0001). This indicates that for each 1-unit increase in the natural logarithm of lesion size, the odds of identifying bone within the mass increased by approximately 416%.
Proliferation of alveolar bone at the base of the mass was seen in 60% of the lesions, and evidence of reactive alveolar bone was seen in 90% of the lesions. Inflammatory cells were present within alveolar bone at the base of the mass in 67% of the lesions. Alveolar bone loss could not be evaluated for 1 lesion and was noted in 23 lesions (23/99, 23%). Most cases with alveolar bone loss also had alveolar bone inflammation (18/23, 78%), a history of previous mass debulking (5/23, 22%), or previous extraction of the associated tooth (2/23, 9%). For one lesion with alveolar bone loss, the associated tooth had a root fracture (1/23, 4%). Only one case (1/23, 4%) had no apparent concurrent pathology or history that provided a plausible explanation for alveolar bone loss. Invasion of alveolar bone was not observed in 99% of lesions and alveolar bone invasion could not be evaluated in one lesion due to suboptimal orientation of the histologic section and paucity of marginal bone.
Increased thickness of cementum (hypercementosis) at the CEJ was seen in 79 of 89 lesions (89%) for which this feature could be evaluated. Tooth resorption was seen in 19 of 86 lesions (22%) for which this feature could be evaluated.
The location of the base of the mass was at the CEJ for 80% of the lesions and below the CEJ for 18% of the lesions, and 2 lesions were confined to the attached gingiva and therefore did not approach the CEJ. Extension of lesion tissue below the CEJ was unexpected; therefore, for these 18 cases, clinical records were examined in closer detail for a potential explanation. It was found that 3 lesions occurred at a site of previous tooth extraction, 5 lesions occurred in conjunction with periodontal disease, 7 lesions had been previously excised, and 7 lesions had been previously excised and occurred in conjunction with periodontal disease.
The PDL of the adjacent tooth was present for evaluation in histological sections for 89 of 100 lesions including 73 (82%) with normal PDL, 12 (14%) with PDL disrupted by periodontal inflammation (Fig. 5), and 4 (5%) with PDL effaced by cemento-osseous remodeling concurrent with tooth resorption. None of the lesions were observed to invade the PDL space.
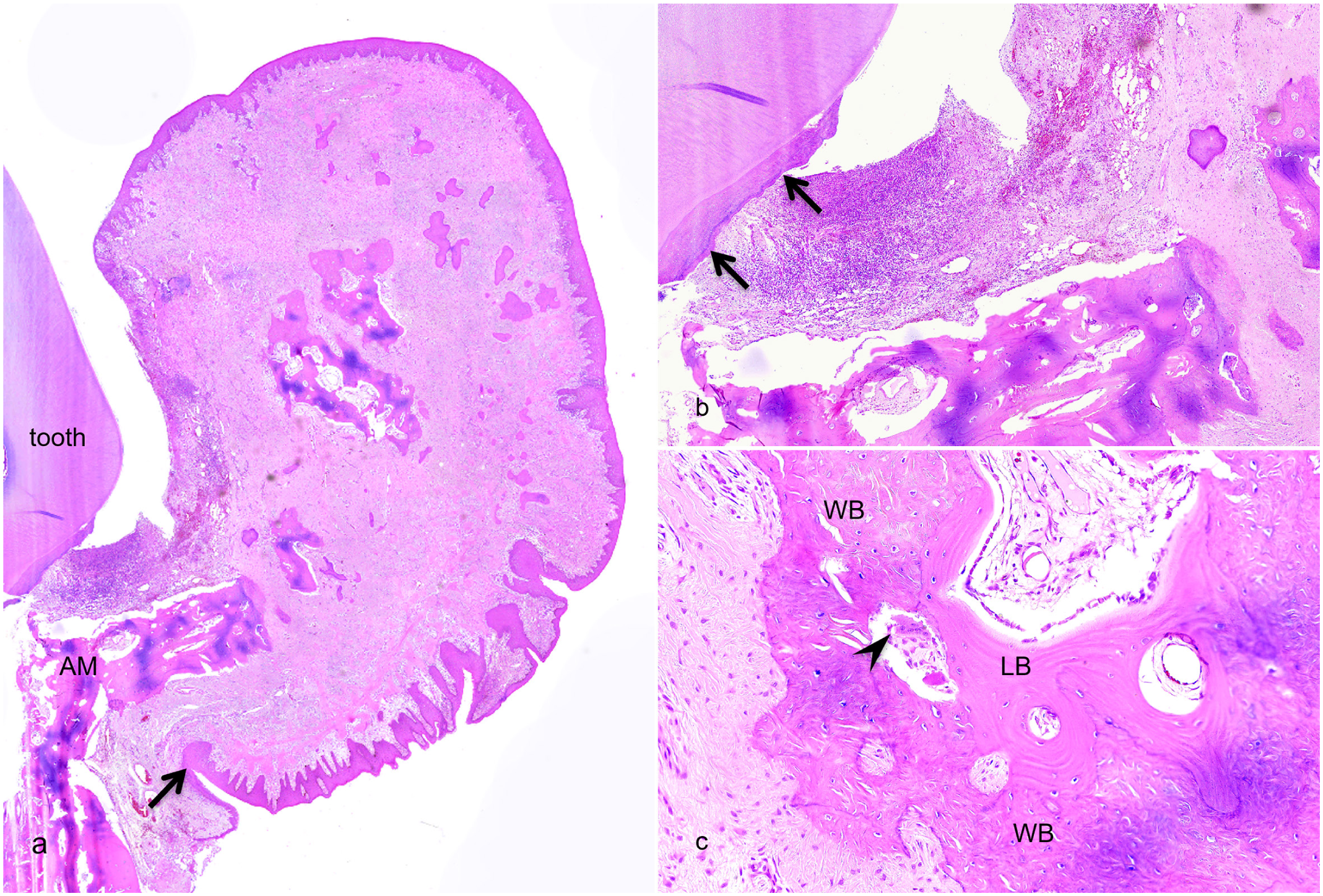
Fibromatous epulis of periodontal ligament origin (FEPLO)/peripheral odontogenic fibroma (POF), gingiva, dog. Hematoxylin and eosin. (a) The mass extends to the mucogingival junction (arrow) and has variably-sized islands of bone. Bone at the alveolar margin (AM) is proliferative and extends up into the base of the mass. The tooth associated with this mass has periodontitis with loss of periodontal tissue attachment and inflammation at the base of the tooth crown. (b) The inflamed tissue effaces the periodontal ligament that should attach to cementum (arrows). (c) Ossification within the mass is predominantly woven bone (WB), although osteoclasts are present (arrowhead) and some bone has matured to lamellar bone (LB).
Tooth displacement was noted in 22 of 82 lesions (27%) for which this feature could be evaluated. Teeth displaced included maxillary incisors (15/22, 68%), mandibular incisors (4/22, 18%), mandibular second premolars (2/22, 9%), and a maxillary second premolar (1/22, 5%). Logistic regression did not demonstrate a statistically significant association between lesion size and tooth displacement. After log transformation of the lesion size, the regression coefficient for lesion size was β = −0.489 (95% CI −1.337 to 0.333), corresponding to an odds ratio of 0.61 (95% CI 0.26–1.39, P = .24). Overall, these findings suggest that lesion size alone is not a reliable predictor of tooth displacement in this model.
Multifocal/generalized gingival hyperplasia was apparent in 7 of 83 dogs (8%) for which this feature could be evaluated. Breeds represented in this group include 2 mixed breed dogs and one each of the following: English Bulldog, Boston Terrier, Golden Retriever, Boxer, and French Bulldog.
Follow-up was received for 77% of lesions, none of which had recurred following en bloc excision. The time between surgery and follow-up ranged from 0.25 to 31.25 months with a mean of 17.5 months and median of 22 months. Greater than half of the lesions (61%) had follow-up of at least 3 months.
Discussion
Results of this study are congruent with previous studies of FEPLO/POF in dogs regarding over-representation of castrated males.2,8 Mean age of this study population (7.3 years) was slightly less than previous studies of 8.1 and 8.5 years.2,8,23 Golden Retriever was the most common pure breed although it is not clear if this breed was overrepresented for the entire database population. In a previous study, a greater than expected number of Golden Retrievers were found among dogs with FEPLO/POF. 8 Boxer dogs have also been reported to be at increased risk of FEPLO/POF; therefore, it was surprising that only one Boxer was in this study population. 2 Boxer dogs may have FEPLO/POF lesions in conjunction with gingival hyperplasia and marginal excision may be elected for treatment when a dog has multiple gingival enlargements. If this is true, then selection of cases treated by en bloc excision could have resulted in a negative bias for Boxer dogs in this study.
The rostral maxilla has been reported as the most common site with 40% to 47% of FEPLO/POF lesions described in this location.2,8 A rostral location was also most common for the 100 lesions in this study that were excised en bloc, although rostral maxillary and rostral mandibular lesions were present in approximately equal numbers. However, there was little difference in distribution when a larger number (400) of both incisional and excisional biopsy cases was evaluated. It may be that FEPLO/POF lesions in dogs occur more uniformly throughout the gingiva than previously believed and prior studies may have had too few cases or other sources of bias. A significant source of bias may be ease of lesion recognition by owners and by veterinarians performing an awake physical exam. A mass located near an incisor or canine tooth is more likely to be noticed than a caudal mass. The 400 lesions that were obtained by either incisional or excisional biopsy include more masses that were found incidentally during anesthetized oral exam and dental procedure; therefore, these represent a less biased sample.
This is the first study to report lesion size and to attempt to correlate lesion size with other histomorphologic features. Larger lesions were more likely to extend to the mucogingival junction, and the average size of ossified lesions was greater than lesions without bone or osteoid. It is probable that larger lesions are chronic, although a longitudinal study would be necessary to determine if ossification correlates with lesion duration or rate of growth. Lesion size did not appear to correlate with tooth displacement; instead, the size of the tooth seemed to be more significant since the only teeth noted to be displaced were incisors and, less often, second premolars. The roots of incisors possess a lower PDL surface area compared with the roots of premolars and molars. As such, they are more prone to displacement from low-level forces.
Anatomic boundaries of FEPLO/POF lesions span the entire gingiva, extending to the mucogingival junction, to the CEJ, and to the alveolar bone margin. For most lesions (80%), the deep border of the mass corresponded with the level of the CEJ and 88% of lesions contacted the alveolar bone margin. These data demonstrate that lesions do not invade alveolar bone and do not involve the PDL proper. The lesions do not originate from the PDL yet invariably involve the gingival ligament. Sharpey’s fibers are noted, attaching the fibrous tissue to bone of the alveolar margin and to cementum near the CEJ. This histomorphologic relationship is characteristic of the gingival ligament.
The histologic organization of FEPLO/POF lesions has been thoroughly described by Dubielzig and others.5,6,13 The proliferative lesions are composed of fibrous tissue with spindle to stellate mesenchymal cells that are evenly spaced within abundant collagenous matrix. The collagen fibers are fine and randomly interwoven rather than arranged in dense linear bundles. These features are characteristic of odontogenic mesenchymal tissue that normally forms the periodontal and gingival ligaments. In contrast, fibrous connective tissue of the gingival stroma is poorly cellular with spindle cells between coarse collagen fibers that often form intersecting bundles. Localized hyperplasia of fibrous gingival stroma, focal fibrous gingival hyperplasia, is often clinically indistinguishable from FEPLO/POF. Histomorphology of the fibrous tissue is the essential difference between fibrous gingival hyperplasia and FEPLO/POF, not the presence or absence of odontogenic epithelium.
More recent studies have described hypercellular variants of FEPLO/POF.12,15 These lesions are described as having increased cellularity, a lower proportion of fibrous matrix, pleomorphism, and mitotic activity.12,15 A quantitative means to evaluate lesion cellularity is not available to pathologists and lack of uniform cellularity within a single lesion would complicate validation of such a metric. Compared with “typical” FEPLO/POF lesions, the hypercellular lesions do not have a more negative prognosis, higher incidence of recurrence, or requirement for more aggressive treatment.12,15 Rather than considering cellularity as a singular parameter of significance, it may be more relevant for pathologists to recognize hypercellularity as a feature that warrants explanation. Seventeen percent of lesions in this study were hypercellular; of those, 15 (88%) were ulcerated and 15 (88%) had inflammation. A previous study of hypercellular FEPLO/POF lesions reported that 41% (22/54) were ulcerated and 76% (41/54) had lymphocytes and plasma cells. 16 Hypercellularity was often nonuniform within a lesion with ulcerated areas having greater cellularity than areas remote to ulceration in the same mass. Additionally, areas of hypercellularity differed morphologically from typical areas by having closely spaced, streaming spindle cells. Mitotic counts were not recorded for each lesion; therefore, no conclusion can be made regarding the relationship of mitotic activity to lesion cellularity.
Trauma is a common reason for oral tumors to be ulcerated, and the physical forces associated with traumatic occlusion can significantly alter tissue histomorphology. Increased cellularity, pleomorphism, and mitotic activity are likely reactive features of FEPLO/POF lesions that are traumatized or otherwise perturbed. Hypercellularity of a lesion appears to be the effect of extrinsic factors rather than an intrinsic difference. As such, the relevance of recognizing “hypercellular” lesions as a distinct histologic subtype is questionable. Increased cellularity and pleomorphism are nonetheless important since a reactive FEPLO/POF lesion can be histologically indistinguishable from a malignant spindle cell neoplasm. When noted by a pathologist, increased cellularity or atypia should be reported and interpreted in the context of other findings (eg, ulceration and inflammation). A differential diagnosis that includes spindle cell neoplasms may be most appropriate if there is no clear explanation for reactive changes or if the pathologist is not given sufficient history to make a clinical correlation.
Intralesional bone formation was seen in 54% of cases, and new woven bone that arose within the lesion was able to model into mature lamellar bone. Occasionally, bone within a lesion was fused with bone of the alveolar margin, although this was not seen in most cases with ossification. As such, data from this study support a remark by Bostock and White that, “bone [in the canine epulis] was not derived from the underlying periosteum, but occurred in isolated islands, within the fibrous tissue stroma.” 5 This finding suggests that the osteogenic potential is intrinsic to fibrous connective tissue of the lesion. Recent studies in periodontology have shown that PDL stroma has osteogenic potential and expresses osteogenic proteins, including SATB2.1,24 Since the periodontal and gingival ligaments arise from the same odontogenic mesenchyme of the dental follicle, osteogenic potential is also intrinsic to the gingival ligament stroma.
Odontogenic epithelium was present in most lesions (63%), and the distribution was either diffuse or paradental. The origin of this epithelium has not been satisfactorily explained. It is likely incorrect to assume that this epithelium is derived from rests of Malassez since these foci of odontogenic epithelium are derived from Hertwig’s epithelial root sheath, distributed throughout the PDL, and therefore located between the tooth root surface and alveolar bone. 21 A mass arising in this location would expand alveolar bone. Odontogenic rests of Serres are a more likely source since these are derived from the dental lamina, which is an embryologic epithelial structure that extends from epithelium lining the oral cavity to the enamel organ of a developing tooth. Breakdown of the dental lamina could theoretically leave rests of Serres within the fibrous gingival stroma. However, it is notable that odontogenic epithelial rests are not evident within normal gingiva in the same manner that they can be readily found throughout the PDL. This fact makes it difficult to accept the theory that odontogenic epithelium within FEPLO/POF lesions arises exclusively from rests of Serres.
Reichart et al 22 postulated that epithelium within FEPLO/POF lesions is explained by down-growth and entrapment of hyperplastic surface epithelium. This theory is compelling if further modified to specify junctional epithelium rather than all surface epithelium. This is an important distinction because gingival epithelium that covers the vestibular surface and most of the gingival free margin is not odontogenic. 21 Junctional epithelium, which lines only the paradental surface of the gingiva, is derived from the reduced enamel epithelium and is therefore odontogenic. 21 This difference is morphologically evident in sections of normal gingiva where the vestibular epithelium is robust and lightly keratinized with broad, short rete pegs. In contrast, the junctional epithelium is attenuated and nonkeratinized with plexiform branching of long, thin rete pegs. During development and growth of FEPLO/POF lesions, we believe that rete pegs of hyperplastic junctional epithelium extend into and become embedded within proliferative tissue of the gingival ligament. This explanation is compatible with both embryogenesis and our findings that odontogenic epithelium within FEPLO/POF lesions is either diffuse or paradental, but not vestibular.
The odontogenic epithelium within lesions of this study occasionally had uncommon morphologic features including keratinization, melanin pigment, and cyst formation. To the best of our knowledge, these were incidental features that are unlikely to relate to the pathogenesis or to impact biologic behavior, treatment recommendations, or prognosis. In this study, lesions with keratinized epithelium had multiple, small foci of keratinized squamous cells within islands and cords that were usually near the junctional epithelium. Lesions that have prominent epithelium, particularly with keratinizing squamous cells and/or cyst formation, may be difficult to differentiate from canine acanthomatous ameloblastoma or conventional ameloblastoma. Two of the four lesions with keratinization also had melanization of epithelial cells. Both dogs had heavily pigmented gingiva and oral mucosa.
Concurrence of other pathologic changes within or near FEPLO/POF lesions in dogs has not been previously investigated. These changes are potentially important since active processes within subjacent alveolar bone could promote initiation, growth, or recurrence of FEPLO/POF lesions. The most common changes were hypercementosis at the CEJ (89% of lesions) and evidence of reactive alveolar bone (90% of lesions). Factors that trigger remodeling of alveolar bone and hypercementosis (eg, dentoalveolar trauma) may also stimulate hyperplasia of the gingival ligament. Inflammatory cells infiltrated alveolar bone in 67% of lesions. Subjectively, most instances of alveolar osteitis were mild, although the high proportion of lesions with osteitis was surprisingly high since only 24% of lesions had inflammation within the mass and 13.5% of lesions had periodontal inflammation effacing the PDL. It is likely that many more lesions would have had inflammation within the mass had we not excluded those with only paradental inflammation. Lymphoplasmacytic inflammation along the paradental surface of any type of gingival mass is very common because this surface directly contacts plaque biofilm on the adjacent tooth crown. Therefore, for this study, lesions that had only paradental inflammation were not considered to have inflammation within the mass. Nevertheless, paradental inflammation can extend into subjacent alveolar bone, and this might explain the high proportion of lesions that had mild alveolar osteitis. Tooth resorption was noted in 22% of lesions, and 8% of lesions occurred in dogs with multifocal/generalized gingival hyperplasia. Dentoalveolar trauma, alveolar osteitis, and other processes within alveolar and periodontal tissues are likely to contribute to FEPLO/POF lesions in dogs, which supports a hyperplastic rather than neoplastic pathogenesis.
Evaluation of the deep border of the lesion with respect to the CEJ and alveolar bone was important to determine lesion invasiveness. In 2024, Kim et al 15 described “locally invasive hypercellular” FEPLO/POF lesions, stating, “In rare instances, invasion of the alveolar bone is present, suggesting potential for locally invasive behavior.” This conclusion was based on 5 of 20 lesions that had “evidence of bone invasion merging with the alveolar bone and PDL region.” 15 In the present study, 18 of 100 of lesions extended below (apical to) the CEJ. In other words, the base of these lesions was anatomically in an area that should have been occupied by alveolar bone. However, each of these lesions had one or more of the following reasons for distorted anatomy: previous tooth extraction, previous excision of the mass, and local periodontal disease. In these cases, involvement of periodontal tissues, including alveolar bone, was attributed to another process rather than taken as evidence of invasive behavior by the FEPLO/POF lesion.
Apparent invasiveness might also be explained by erroneous diagnosis. Both canine acanthomatous ameloblastoma and the desmoplastic variant of conventional ameloblastoma have the potential to histologically mimic an invasive FEPLO/POF. 7 Furthermore, osteosarcoma or other sarcomas may be misdiagnosed as an “invasive hypercellular POF.” We have found that FEPLO/POF lesions do not extend beyond the anatomic boundaries of the gingiva, although occasional lesions may extend beyond the CEJ if tissue anatomy has been compromised by another process. We believe that FEPLO/POF is not a rational differential diagnosis for a lesion that demonstrates conclusive histologic evidence of infiltrative growth or any mass that directly causes bone expansion or osteolysis.
Of 61 cases with follow-up of at least 3 months, none had reported recurrence following en bloc excision. Nevertheless, FEPLO/POF lesions may recur following debulking or marginal excision. In a recent study, recurrence was reported for 5% (1/24) of cases. 23 An older study from 1987 reported a higher recurrence rate of 18% (3/17). 5 This difference might reflect a bias for conservative surgical treatment in past decades compared with more contemporary recommendations for excision to the level of alveolar bone. 25 A study of hypercellular FEPLO/POF lesions reported no recurrence (0/20) during the follow-up timeframe (minimum 6 months) irrespective of excisional margins. 15 A subsequent study of hypercellular lesions had 14% (4/29) recurrence. 12
When lesions do recur, the stimulus for regrowth is likely to occur at the base of the mass, involving the CEJ and/or alveolar bone margin. Because the gingival ligament fibers anchor to the cervical region of the tooth and to the superficial alveolar bone margin, superficial alveolectomy or alveoloplasty (bone recontouring) may be required to prevent recurrence.19,25 Our selection of lesions that had been excised en bloc should not be taken as recommendation of this surgical technique for all cases. We believe that histomorphologic data from this study support a conservative approach to surgical management of FEPLO/POF.
A two-step approach may be considered for surgical management: marginal excision of the mass followed by periodontal management of the adjacent tooth. Since the lesion is confined to the gingival ligament and overlying gingiva, marginal mass excision may include only the visibly affected gingiva with an incision to the alveolar margin, which will in effect include the gingival ligament. Periodontal management considerations may or may not require extraction of the adjacent tooth/teeth. Extraction may be prudent if the degree to which gingiva has been excised will compromise the long-term periodontal health of the tooth. The tooth can be spared if a healthy gingival collar can be maintained or restored with gingival surgery. While en bloc excision is typically more aggressive than necessary, it may have the benefit of surgical efficiency for large or extensively ossified lesions.
Inclusion of only lesions that had been excised en bloc is an important source of bias in this study. This may have selected for larger, chronic lesions. Clinical features of an aggressive process (rapid growth, recurrence, trauma, ulceration, and inflammation) could also influence the choice of en bloc excision. This may explain the number of reactive, hypercellular lesions in this study. No previous studies have established the frequency of hypercellularity for canine FEPLO/POF lesions, although 17% is greater than the authors would have predicted based on experience.
In human medicine, official bodies such as the World Health Organization publish reference volumes for tumors that are periodically updated and these represent a benchmark for nomenclature. 29 In veterinary medicine, there is no singular governing body that is comparable with the World Health Organization, although various types of benchmark publications often exist within veterinary specialties. Pertinent to this discussion, the American Veterinary Dental College maintains an online nomenclature page, which presently refers to this lesion as POF. 3 It is not clear when or by what process the terms fibromatous epulis and ossifying epulis were abandoned, although it is likely that use of the word “epulis” alone was objectionable to most American Veterinary Dental College members. In veterinary pathology, the Davis-Thompson foundation publishes tumor fascicles that are similar to World Health Organization publications. While the content of the fascicles is at the discretion of editors, each issue has multiple editors that are regarded as expert in their field. Both the most recent issue from 2020 and its predecessor from 2003 use the name FEPLO.13,16 Thus, to the extent that there is an official name, veterinary dentists recognize POF and veterinary pathologists recognize FEPLO. Reconciliation of this discrepancy is one of the main objectives of this study.
The name FEPLO is unacceptable for multiple reasons, including use of the antiquated and vague term “epulis” and the assertion that the lesion is “of periodontal ligament origin.” This study demonstrates that lesions have no such direct relationship to the PDL. Regarding POF, we reject the assertion, made almost exclusively by nonveterinary researchers, that the lesion of dogs is analogous to a mixed odontogenic neoplasm of the same name in humans. In fact, the lesion in dogs has more in common, both clinically and histologically, with peripheral ossifying fibroma of humans. 29 This name is also imperfect since lesions in dogs do not always ossify and the multifocal nature of the lesion is incompatible with neoplasia.
It is our position that the nomenclature for oral lesions in humans was applied inappropriately to dogs and has been extrapolated to use for benign hyperplastic gingival lesions in cats, horses, and other veterinary species. Between 1992 and 2014, veterinary pathologists contributed remarkably little to publications that advocated for replacement of FEPLO by POF. Among veterinary dentists, an impetus for replacement of FEPLO by POF was a 2011 Journal of the American Veterinary Medical Association publication in which FEPLO were reclassified as either focal fibrous hyperplasia or POF. 8 In 2014, publications in the Journal of Veterinary Dentistry by Bell and Soukup conformed with use of POF and eschewed FEPLO, representing the first publication on the topic by a veterinary pathologist since Dubielzig.4,26 In retrospect, these authors openly acknowledge that this endorsement was misguided and adoption of terminology that is acceptable to both veterinary pathologists and veterinary dentists is long overdue.
Fibromatous hyperplasia of the gingival ligament (FHGL) is put forth as an anatomically correct, biologically accurate, and unifying name for this lesion. Based on currently available evidence, the growth pattern and biological behavior of the lesion are more characteristic of a hyperplastic process rather than a mixed odontogenic neoplasm. While “gingival ligament” is not currently in common parlance, it is defined in the most authoritative text on oral histology and deserves widespread recognition. 21 An authoritative text in veterinary dentistry fails to name the gingival ligament but does describe the precise gingival fibers of this anatomic structure. 17 An updated text by the authors of this study explicitly defines the gingival ligament. 20 This text also uses FHGL to name the lesion as does a forthcoming new edition of Tumors in Domestic Animals, which is scheduled for publication in 2026.18,19
The histomorphology of FHGL is consistent most with a hyperplastic lesion that arises within and is anatomically confined to the gingiva. The pathoetiology of FHGL may involve various mechanical and inflammatory stressors that impact tissues of the gingival ligament as well as the adjacent tooth and subjacent alveolar bone. Odontogenic epithelium within FHGL lesions represents proliferative junctional epithelium that becomes incorporated into hyperplastic fibrous tissue of the gingival ligament. Hypercellularity is a reactive change that commonly occurs in conjunction with ulceration, inflammation, and lesional trauma. Bone within FHGL lesions represents osteogenic potential of odontogenic mesenchyme, which forms the gingival ligament. Separate names for lesions with and without bone are unnecessary and terminology such as ossified FHGL or FHGL with ossification is recommended. Understanding the gingival ligament and its relationship to periodontal anatomy will help clinicians to provide effective surgical treatment while minimizing patient morbidity.
Supplemental Material
sj-xlsx-1-vet-10.1177_03009858261457960 – Supplemental material for Histomorphologic evidence supports a hyperplastic pathogenesis of fibromatous epulis of periodontal ligament origin/peripheral odontogenic fibroma and proposal of fibromatous hyperplasia of the gingival ligament as unifying nomenclature
Supplemental material, sj-xlsx-1-vet-10.1177_03009858261457960 for Histomorphologic evidence supports a hyperplastic pathogenesis of fibromatous epulis of periodontal ligament origin/peripheral odontogenic fibroma and proposal of fibromatous hyperplasia of the gingival ligament as unifying nomenclature by Cynthia M. Bell, Brian G. Murphy and Jason W. Soukup in Veterinary Pathology
Supplemental Material
sj-pdf-1-vet-10.1177_03009858261457960 – Supplemental material for Histomorphologic evidence supports a hyperplastic pathogenesis of fibromatous epulis of periodontal ligament origin/peripheral odontogenic fibroma and proposal of fibromatous hyperplasia of the gingival ligament as unifying nomenclature
Supplemental material, sj-pdf-1-vet-10.1177_03009858261457960 for Histomorphologic evidence supports a hyperplastic pathogenesis of fibromatous epulis of periodontal ligament origin/peripheral odontogenic fibroma and proposal of fibromatous hyperplasia of the gingival ligament as unifying nomenclature by Cynthia M. Bell, Brian G. Murphy and Jason W. Soukup in Veterinary Pathology
Footnotes
Acknowledgements
We would like to thank the many veterinary dentists, clinicians, and our staff for providing follow-up information regarding lesion recurrence. We are specifically grateful to Dr Jamie Berning for granting permission to use Fig. 4a and b.
Supplemental material for this article is available online.
Author Contributions
CMB designed the study with contributions from BGM. CMB performed histologic evaluation and curated data. JWS performed statistical analysis. The manuscript was written by CMB with contribution from BMG and JWS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.