
Abstract
Objectives
To compare and assess hearing capacity between children with maxillary constriction and those with normal maxillary width. To evaluate the correlation between arch width and hearing capacity.
Materials and Methods
In this cross‑sectional study, 70 orthodontic patients in the late mixed dentition stage were divided into two groups. The experimental group (n = 35) included individuals with maxillary constriction, defined by an interpalatal molar width (IPMW) smaller than 34.92 mm and an IPMW-to-intercanine width (ICW) ratio around 1.15-1. The control group (n = 35) had normal maxillary dimensions and well‑aligned arches with no crowding or spacing, and with IPMW greater than 37.45 mm and an IPMW-to-ICW ratio near 1:1 ± 0.05. Maxillary arch width was measured on dental casts using a vernier caliper, and hearing thresholds were assessed using pure-tone audiometry in a sound-isolated chamber, and pure-tone air conduction averages were taken. Statistical tests were analyzed using unpaired t-tests and Pearson’s correlation.
Results
The experimental group showed significantly higher mean hearing thresholds (~28 dB) bilaterally compared to controls (~15 dB) (P < .0001). A strong negative correlation was observed between maxillary arch width and hearing threshold in the constricted group (r ≈ −0.49 left, r ≈ −0.44 right), indicating that narrower arches were associated with poorer hearing. No significant correlation was found in the control group.
Conclusions
Children with a constricted maxillary arch width demonstrated mild but significant bilateral conductive hearing loss. The findings support a strong relationship between transverse maxillary deficiency and auditory function, emphasizing the importance of interdisciplinary evaluation in orthodontic patients.
Introduction
Maxillary constriction, a transverse deficiency of the maxilla, is a common orthodontic condition characterized by a narrow, V-shaped arch with a high palatal vault, crowding, and a posterior crossbite. Although primarily an occlusal problem, maxillary constriction may have broader effects, potentially impacting auditory function. It has been reported that transverse craniofacial discrepancies affect approximately 8%-15% of adolescents.1, 2
In children, the Eustachian tube (ET) is anatomically shorter and more horizontally oriented than in adults, which predisposes children to inefficient middle-ear ventilation and otitis media. For example, the pediatric ET typically forms only a ~10° angle relative to the horizontal plane, compared to ~30°-45° in adults.3-6 A constricted maxillary arch or high palatal vault may accentuate this horizontal orientation of the ET, further impairing middle-ear drainage and contributing to conductive hearing loss.
Rapid maxillary expansion (RME) has been associated with decreased nasal mucosal hypertrophy, improved nasal airflow, and a reduced incidence of recurrent otitis media, suggesting potential auditory benefits.7-11 This further supports the hypothesis that maxillary constriction may have implications beyond dental and skeletal structures, affecting auditory health.
Previous studies have largely investigated hearing outcomes following RME in children selected because they already had otitis media with effusion or an established conductive hearing loss. Systematic reviews confirm that RME can improve conductive hearing thresholds in such patients, but also highlight substantial heterogeneity and a lack of data on unselected orthodontic populations. In contrast, there is limited evidence on the baseline hearing status of non‑syndromic children with transverse maxillary deficiency who present to orthodontic clinics and are otherwise free from diagnosed ear disease.
The age group of 8-12 years is a period of active craniofacial growth and is also the common time when orthodontic treatments such as RME are carried out. At the same time, this age is very important for hearing and speech development. Proper functioning of the hearing system and adequate sound stimulation are essential for the development of verbal language.
Therefore, the aim and objectives of this cross-sectional study were to compare the pure-tone air-conduction hearing thresholds between children with maxillary constriction and those with normal maxillary arch width. Additionally, to evaluate the correlation between arch width and hearing capacity.
By clarifying the relationship between craniofacial morphology and auditory function, our findings may contribute to interdisciplinary care involving orthodontists and otolaryngologists.
Materials and Methods
Study Design
This observational cross-sectional study was conducted on children with the late mixed dentition stage. Data were collected between May 15, 2024, and May 15, 2025. The participants in the sample were divided into two groups: the experimental group (n = 35): individuals in late mixed dentition with maxillary constriction, defined as an interpalatal molar width (IPMW) <34.92 mm and an IPMW-to-intercanine width ratio (IPMW:ICW) ≥1.15:1 ± 0.05. 12 Inclusion criteria were maxillary arch width deficiency, a V-shaped palate with a deep vault, unilateral or bilateral posterior crossbite, no clinically evident caries, and children who need maxillary expansion as part of their orthodontic treatment plan. Exclusion criteria included a history of cleft lip, cleft palate, or craniofacial syndromes, as well as prior orthodontic or otolaryngologic treatment. Control group (n = 35): individuals in late mixed dentition with normal maxillary arch dimensions, defined as IPMW >37.45 mm and an IPMW:ICW ratio of 1:1 ± 0.05. 12 Inclusion criteria were well-aligned arches with no crowding or spacing and no clinically evident caries. Exclusion criteria included a history of orthodontic, prosthodontic, or otolaryngologic treatment.
Sample Size Calculation
Sample size estimation was performed using G*Power software version 23.0, based on a power of 80%, and a significance level of 0.05. A minimum of 35 participants per group was determined to detect clinically relevant differences.
Blinding
To mitigate selection bias, three senior orthodontists independently evaluated maxillary dental models of participants who fulfilled the inclusion and exclusion criteria by unanimous consensus. Models were anonymized using a coded labeling system, randomized via a computer-generated sequence, and evaluated by a blinded examiner. Audiometric and maxillary arch measurements were conducted by blinded operators to prevent observer bias.
Variables and Measurements
We measured maxillary arch dimensions (ICW, IPMW) and pure-tone audiometric thresholds. Alginate impressions of the upper arch were taken and disinfected by glutaraldehyde 2% for 10 min, and hard stone plaster was poured within 10 min to obtain accurate stone casts.13, 14 Arch width measurements were taken on casts using a digital vernier caliper (±0.1 mm accuracy). IPMW was measured between the central fossae of the first permanent molars. ICW was measured between the cusp tips of the upper canines. The IPMW/ICW ratio was calculated.
Pure-tone audiometry was conducted in a sound-isolated chamber using an audiometer calibrated according to the American National Standards Institute standards. Hearing thresholds were measured across a range of standard frequencies (typically 250-8,000 Hz) and averaged to compute the pure-tone average of air conduction for each ear. Hearing capacity was classified as follows: 0-25 dB: normal hearing (with 16-26 dB sometimes considered as very slight deafness); 26-40 dB: mild hearing loss, 41-55 dB: moderate hearing loss, 56-70 dB: severe hearing loss, 71-90 dB: very severe hearing loss; and >90 dB: profound hearing loss.15, 16
Reliability Assessment
Intra-examiner and inter-examiner reliability for arch width measurements were evaluated using the intraclass correlation coefficient. Discrepancies between measurements were resolved by consensus.
Statistical Analysis
All statistical analyzes were conducted using Statistical Package for the Social Sciences software (version 23.0, IBM Corp, Armonk, NY, USA). The distribution of continuous variables, including hearing thresholds and maxillary arch width ratios, was evaluated for normality using the Shapiro–Wilk test. As the data met the assumptions of normality, group comparisons were performed using independent (unpaired) two-tailed t-tests. These were applied to compare the mean age, air-conduction hearing thresholds (in decibels) for both left and right ears, and the IPMW:ICW ratio between the experimental and control groups. The chi-square (χ2) test was used to compare gender distribution. To assess the relationship between maxillary arch width and hearing thresholds, Pearson’s correlation coefficient (r) was calculated separately for the left and right ears within each group. Correlation strength was interpreted as follows: values of |r| between 0.1 and 0.3 were considered weak, 0.3-0.5 moderate, and >0.5 strong. All statistical tests were two-tailed, and a P value < .05 was considered statistically significant.
Results
Participant characteristics are summarized in Tables 1 and 2. The mean age of participants in the experimental group was 9.82 ± 1.15 years, and 10.20 ± 1.10 years in the control group. The difference in mean age between the groups was not statistically significant (t = 1.377, P = .17; Table 1). The experimental group included 14 males (40%) and 21 females (60%), while the control group included 15 males (42.9%) and 20 females (57.1%). No significant difference in gender distribution was found between the groups (P = .998; Table 2).
Comparison of Age Between Study Groups Using the Unpaired t-test.

Comparison of Gender Distribution Between Study Groups Using the Chi-square Test.

Air-conduction hearing thresholds for both ears are presented in Table 3. In the left ear, the experimental group showed a mean threshold of 27.68 ± 6.77 dB, compared to 11.85 ± 4.95 dB in the control group (t = −11.55, P < .0001). In the right ear, the experimental group showed a mean threshold of 27.94 ± 6.89 dB, and the control group 12.97 ± 4.34 dB (t = −10.87, P < .0001).
Comparison of Hearing Thresholds Between Groups for Left and Right Ears Using Unpaired t-test.

Arch dimension measurements are presented in Table 4. The IPMW:ICW ratio was 1.162 ± 0.015 in the experimental group and 1.138 ± 0.030 in the control group. The difference was statistically significant (t = −3.42, P = .001).
Comparison of Interpalatal Molar Width:Intercanine Width (IPMW:ICW) Ratio Between Study Groups Using Unpaired t-test.

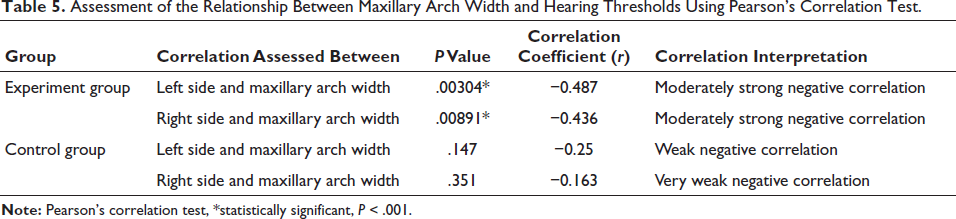
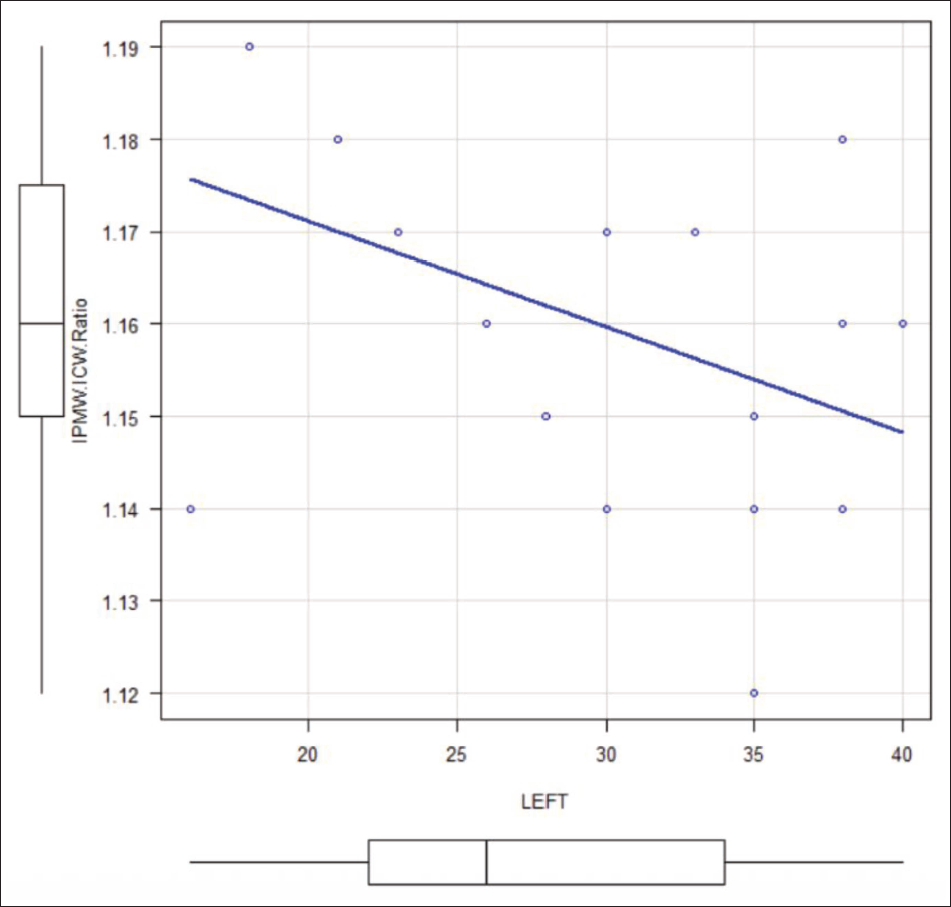
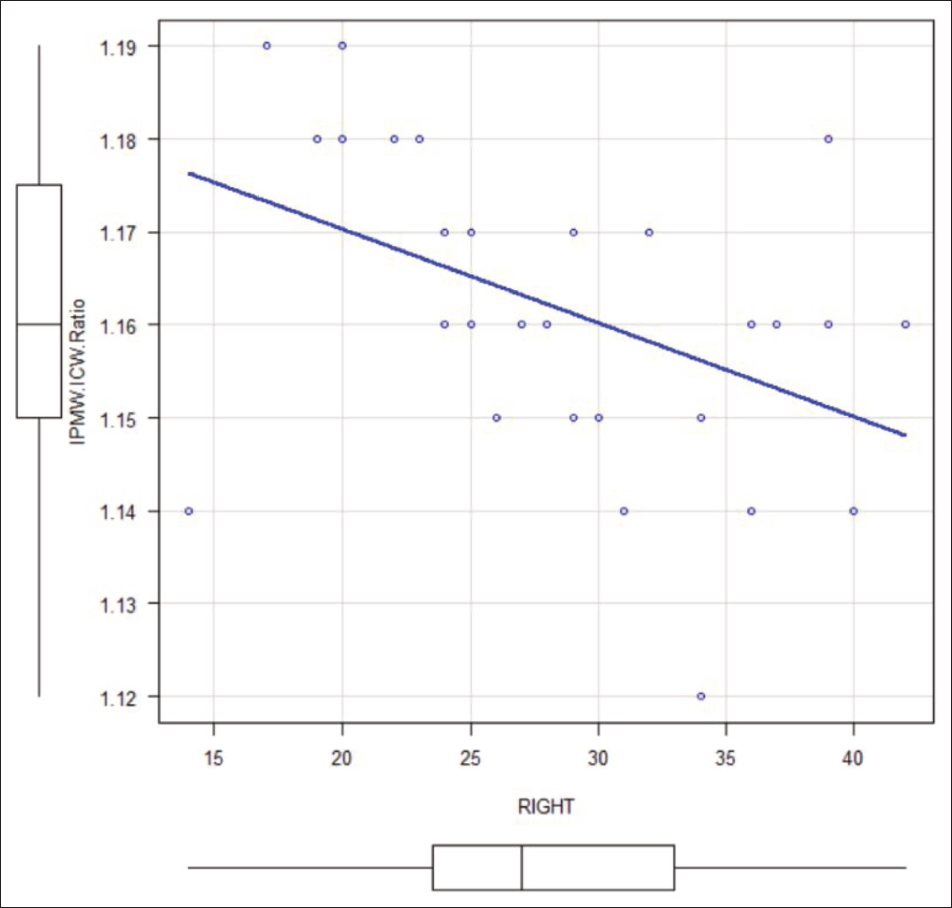
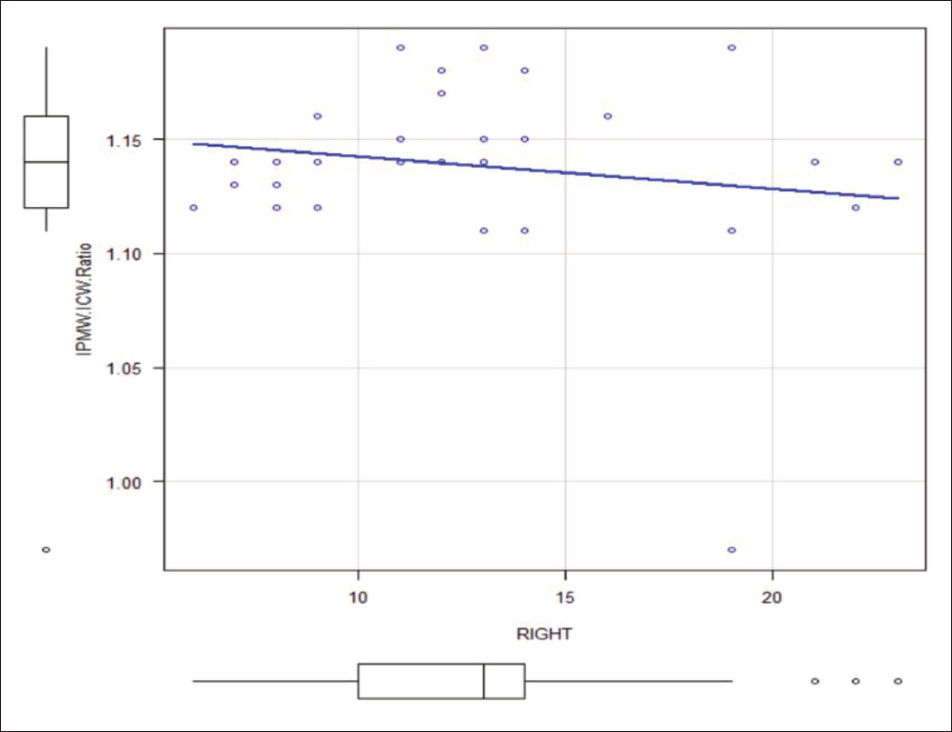
Pearson’s correlation coefficients between maxillary arch width and hearing thresholds are provided in Table 5. Within the experimental group, a negative correlation was observed for the left ear (r = −0.487; P = .003) and the right ear (r = −0.436; P = .009) (Figures 1 and 2). In the control group, correlations were weaker for both the left ear (r = −0.250; P = .147) and the right ear (r = −0.163; P = .351) (Figures 3 and 4).
Assessment of the Relationship Between Maxillary Arch Width and Hearing Thresholds Using Pearson’s Correlation Test.
Assessment of Correlation Between Left Ear Hearing Threshold and Maxillary Arch Width in Experimental Group.
Assessment of Correlation Between Right Ear Hearing Threshold and Maxillary Arch Width in Experimental Group.
Assessment of Correlation Between Left Ear Hearing Threshold and Maxillary Arch Width in Control Group.
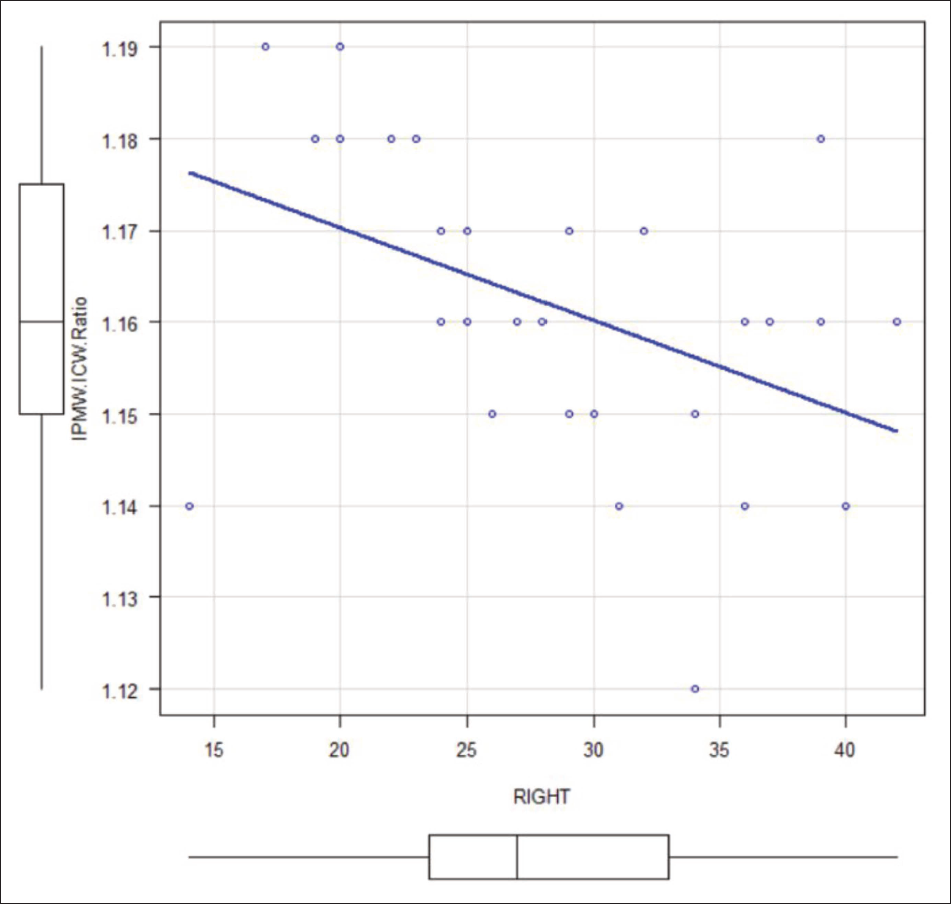
Assessment of Correlation Between Right Ear Hearing Threshold and Maxillary Arch Width in Control Group.
Discussion
Maxillary constriction is a common skeletal anomaly characterized by a narrow, high-arched palate and posterior crossbite, and it is often linked to chronic middle-ear problems.4, 7 Our data show that children with transverse maxillary constriction have significantly poorer hearing thresholds in comparison to children with normal arch widths. The mean left-ear threshold in the constricted group was 27.68 ± 6.77 dB, compared to 11.85 ± 4.95 dB in controls; the right ear showed a similar pattern, at 27.94 ± 6.89 dB versus 12.97 ± 4.34 dB, respectively. This bilateral difference, averaging approximately 15 dB, was highly statistically significant (P < .0001). However, this indicates a mild but clinically relevant conductive hearing loss in the affected children.
Our results are consistent with previous studies. Kiki et al. found that children aged 7-15 years with narrowed maxilla and deep palatal vaults exhibited slight conductive hearing loss up to 24 dB. 17 Peyvandi et al. reported that children with conductive hearing loss were 3.5 times more likely to have maxillary constriction than controls. 18 Kılıç et al., who examined children with refractory otitis media with effusion, found that all had measurable maxillary constriction and mean air-conduction thresholds around 30 dB. 19 Similarly, Hershey et al. reported air–bone gaps of 20-25 dB in children with narrow arches and chronic effusion, although their study included both cleft and non-cleft patients. 20 Laptook described a case of conductive hearing loss reaching up to 50 dB in a patient with maxillary constriction. 21 A systematic review by Fagundes et al. of RME studies further supports this pattern, noting that many authors have suggested a link between maxillary transverse deficiency and conductive hearing loss. 22
Calvo-Henriquez et al., in their meta-analysis of pediatric maxillary expansion studies, reported a mean baseline conductive hearing threshold of approximately 13 dB, reflecting mild conductive hearing impairment in children prior to expansion therapy. 23 Leite et al. more recently analyzed 12 RME studies and reported a pooled 18 dB hearing loss. 24
The biological mechanism underlying this association is closely linked to the anatomy and function of the ET. In infants and young children, the ET is shorter, approximately 18 mm, and more horizontally oriented, forming an angle of just 0°-10° relative to the horizontal plane. This anatomical configuration impairs normal middle-ear drainage and ventilation, making children more prone to ET dysfunction and associated middle-ear conditions. As the child grows, the ET gradually elongates and reorients into a more vertical position, reaching a length of approximately 30-38 mm and an angle of 30°-45° in adults, improving its function.4-7 Ishijima et al. demonstrated that by early adolescence, both the angle and length of the ET approach adult values. 23 However, the impact of maxillary narrowing has different effects on young versus older children. In early childhood, even a moderately high-arched palate can significantly flatten the ET and impair its function, and if persistent maxillary constriction continues as the child grows older, it will disrupt the typical maturation by altering the position and action of key muscles responsible for opening the ET—namely, the tensor veli palatini and levator veli palatini.25, 26
Overall, our findings support a strong and consistent association between maxillary constriction and mild conductive hearing loss in children. In contrast to interventional RME studies, which primarily report hearing gains after expansion, the present cross‑sectional data quantify the magnitude of baseline hearing differences attributable to maxillary constriction alone in an orthodontic clinic population. This supports incorporating basic hearing screening and interdisciplinary referral into the evaluation of children presenting with significant transverse maxillary deficiency.
As a cross-sectional design, it does not establish etiology between maxillary constriction and hearing loss, which can be performed with the help of tympanometry or otoscopy, which are limitations. All participants were recruited from an orthodontic setting, which may introduce selection bias and limit the generalizability of the findings.
Hence, future research should prioritize longitudinal and interventional studies to clarify causality and to assess auditory changes following maxillary expansion. Advanced imaging modalities such as cone-beam computed tomography or magnetic resonance imaging may also be leveraged to further understand the anatomical relationship between palatal dimensions and the ET orientation and function.
Conclusions
A constricted, high-arched palate can impair ET function and middle-ear ventilation during development.
Children with maxillary constriction exhibited slight-to-mild bilateral conductive hearing loss compared to those with normal arch width.
Early orthodontic evaluation and interdisciplinary collaboration may help identify and manage craniofacial factors contributing to pediatric auditory dysfunction.
Footnotes
Acknowledgments
The authors express sincere gratitude to all participants and their families for their cooperation throughout this study. The authors thank the orthodontic faculty and staff for their support during data collection and the biostatistician for guidance in statistical analysis. Special appreciation is extended to the audiometry technicians for their expertise in hearing assessments.
Authors Contribution
Dr. Anisha Valli Anumallasetty: Concept and design, data collection, statistical analysis, and manuscript preparation.
Dr. RSVM Raghu Ram: Concept and design, supervision, interpretation of results, and critical revision of the manuscript.
Dr. Inuganti Ranganayakulu: Data collection and critical revision of the manuscript.
Dr. Neelapala Rohini: Audiometric assessments and data interpretation.
Dr. Ghanta Sunil: Concept refinement, supervision, and critical review of the manuscript.
Dr. Kanaparthy Sri Kavya: Data collection and management, statistical support, and manuscript preparation.
Data Availability
The datasets generated and analyzed during this study are not publicly available due to ethical and privacy considerations protecting participant confidentiality. However, de-identified data may be made available by the corresponding author upon reasonable request with appropriate institutional approvals and data use agreements.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Ethics Committee at GSL Dental College & Hospital, Rajahmundry (Approval No.: GSLDC/IEC/2024/123, dated April 15th, 2024). The study protocol was prospectively registered with the Clinical Trials Registry—India (CTRI No. REF/2025/05/106690).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the parents or legal guardians of all child participants prior to enrollment.