
Abstract
Objectives
To evaluate and compare the shear bond strength (SBS) of orthodontic brackets by employing a conventional composite bonding agent and an alternative self-cure acrylic resin for bonding orthodontic attachments to three different provisional crown materials.
Methods
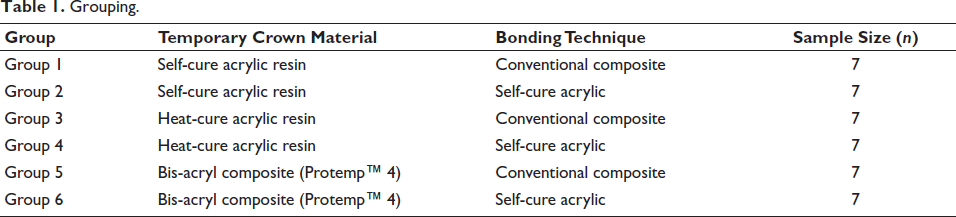
A total of 42 material specimens were prepared: 14 discs, each made of provisional crown materials, namely, bis-acryl composite, self-cure acrylic resin, and heat-cure acrylic resin. These 14 discs of each provisional crown material were randomly allocated into two groups: the first group of 7 was bonded using the conventional bonding technique, and the other group of 7 was bonded with self-cure acrylic resin as the bonding agent. SBS was measured using a Hounsfield universal testing machine, and the Adhesive Remnant Index (ARI) was evaluated. A post hoc power analysis was performed to validate the statistical findings.
Results
One-way analysis of variance revealed significant differences (P < .001). Self-cure acrylic resin demonstrated the highest mean SBS when bonded to self-cure acrylic crowns (13.48 MPa). The lowest SBS was observed in heat-cure acrylic crowns bonded with composite resin (6.14 MPa).
Conclusion
Bonding brackets to self-cure acrylic provisional crowns using self-cure acrylic resin results in the highest SBS. While all groups met clinically acceptable thresholds, the alternative self-cure protocol provided superior bond strength compared to the conventional method across all tested materials.
Introduction
Orthodontic practitioners frequently encounter complex clinical scenarios involving severely hypoplastic, heavily restored, or fractured teeth, as well as morphological variations such as peg-shaped laterals and teeth that have undergone endodontic therapy. In such instances, the placement of a provisional restorative crown is often a clinical necessity before the commencement of active orthodontic treatment. 1
While orthodontic attachments can be either bonded or banded onto these provisional crowns, direct bonding is the preferred, time-efficient method widely adopted in modern practice. 2 Historically, as noted by Zachrisson, acrylic resin has served as a viable bonding agent for attaching appliances to acrylic surfaces. 3 The advancement of materials has led to a wide variety of temporary alternatives, such as bis-acryl composites and resilient heat-cured resins, which pose distinct challenges for conventional bonding methods.
Despite numerous studies investigating various surface preparation techniques and adhesives, there remains a critical lack of research on the efficacy of using modern self-cure acrylic resin as a primary bonding agent across these different substrates. 1 When a conventional composite resin bonding agent is utilized to bond orthodontic attachments to acrylic-based provisional materials, the resulting shear bond strength (SBS) frequently falls below the clinically acceptable threshold of 6-8 MPa, as established by Reynolds. 4 These suboptimal bond strengths lead to high failure rates, which adversely affect clinical efficiency, increase treatment costs, and compromise patient comfort. 2
The current literature presents uncertainty regarding the most effective combination of provisional crown material and bonding agent. While composite resins rely on micromechanical retention, self-cure acrylic resins may offer superior chemical affinity through interfacial polymerization. Therefore, the objective of this in vitro study was to evaluate and compare the SBS of brackets bonded to three distinct types of provisional crown materials—self-cure acrylic resin, heat-cure acrylic resin, and bis-acryl composite—using both a conventional composite bonding system and an alternative self-cure acrylic resin protocol. The null hypothesis tested was that no significant difference exists in the SBS regardless of the provisional material or the bonding agent employed.
Materials and Methods
Study Design and Specimen Preparation
A total of 42 specimens (n = 7 per group) were used; this sample size was determined based on previous similar bond strength investigations, which aimed to minimize biological variation through high environmental control.2, 5 Given the high precision of the Hounsfield universal testing machine and the standardized preparation of the specimens, this sample size provides sufficient statistical sensitivity to detect meaningful differences between bonding protocols without unnecessary material waste. To validate this choice, a post hoc power analysis was conducted using G*Power software (Version 3.1.9.7). For a one-way analysis of variance (ANOVA) with six experimental groups and a total sample size of N = 42, the study achieved a power (1 – β) of 0.80 for a large effect size (f = 0.55) at a significance level of α = 0.05. This indicates that the study was statistically robust enough to detect significant differences between the bonding protocols tested. The selection of n = 7 per group is consistent with standardized in vitro protocols for dental materials testing, where environmental variables are strictly controlled to minimize variance.
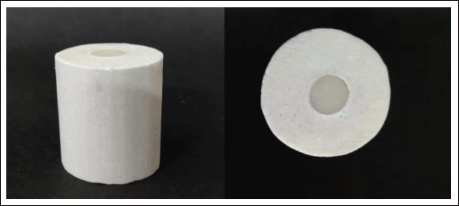
Approval for the study protocol was granted by the Institutional Review Board. Three distinct provisional crown materials were evaluated: self-cure acrylic resin (DPI™), heat-cure acrylic resin (DPI™), and bis-acryl composite (Protemp™ 4). Fourteen discs (8 mm diameter, 4 mm thickness) were fabricated for each material group using a customized putty mold (Figure 1). The specimens were mounted in blocks of plaster of Paris to ensure stability during testing (Figure 2). To standardize the bonding surface, all specimen surfaces were polished with silicon carbide sandpaper (400 and 600 grit), rinsed with water, and air-dried for 30 s.
Mold for Fabrication of Samples.

Provisional Crown Material Samples Mounted in Gypsum Cylinders.
Randomization and Grouping
The 42 specimens (Figure 3) were assigned to six experimental groups using simple randomization. A shuffled sequence of numbered envelopes (blinded selection) was utilized to ensure unbiased allocation to each of the two bonding protocols (Table 1). Furthermore, a blinding protocol was implemented where the investigator performing the SBS testing and ARI scoring remained unaware of the group assignments until all data were recorded.
All Samples with Brackets Bonded.
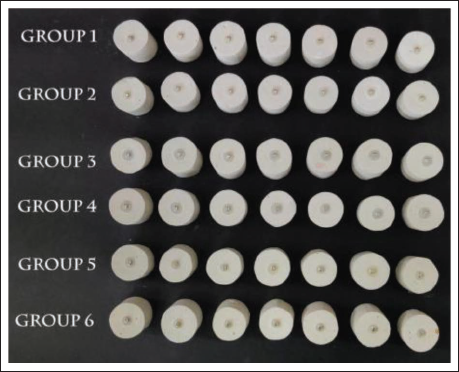
Grouping.
Bonding Protocols
Pre-adjusted edgewise premolar brackets with an MBT prescription (0.022-inch slot, bracket base area = 13.94 mm2) were utilized. Two distinct bonding techniques were employed: Conventional composite protocol (Groups 1, 3, 5): The surfaces were treated with 37% orthophosphoric acid, rinsed, and then allowed to air-dry for 15 s. A thin layer of Transbond™ XT primer was applied and cured with light for 20 s. Next, Transbond™ XT light-cure composite resin was placed on the bracket base, after which the bracket was positioned and cured with light for 20 s (10 s on each side). Alternative self-cure acrylic protocol (Groups 2, 4, 6): Surfaces were similarly cleaned with 37% orthophosphoric acid. Instead of a primer, a thin coat of DPI™ Cold Cure monomer (methyl methacrylate) was applied using a brush to enhance surface wettability and chemical affinity. Self-cure acrylic resin was placed on the bracket base, and the bracket was pressed manually for 30 s to ensure full polymerization. Note: While 37% orthophosphoric acid does not significantly alter the surface topography of acrylic resin, it was utilized in both protocols to remove debris and contaminants generated during specimen preparation, thereby ensuring a clean bonding interface.
Shear Bond Strength Testing
The bonded samples were kept in distilled water at 37°C for 24 h to replicate oral conditions. 6 SBS was evaluated using a Hounsfield Universal Testing Machine (Figure 4), with force applied in an occlusogingival direction at a crosshead speed until debonding occurred. The failure load was recorded, and SBS was calculated in megapascals (MPa) by dividing the failure load by the bracket base area.
Samples Mounted on Hounsfield Machine for Testing of Shear Bond Strength.

Adhesive Remnant Index Scoring
Following debonding, the adhesive remnant on the crown surface was quantified using the Adhesive Remnant Index (ARI), as described by Artun and Bergland. 7 Scores ranged from 0 (no adhesive remaining) to 3 (all adhesive remaining with a distinct bracket mesh imprint).
The Shapiro–Wilk test was used to evaluate the normality of the data distribution, which was further validated by visually inspecting Q–Q plots. All groups showed a nonsignificant departure from normality (P > .05 for all groups), thereby justifying the use of parametric statistical methods (one-way ANOVA and Tukey’s post hoc test) for intergroup comparisons. Data were analyzed using ANOVA and Tukey’s post hoc test for SBS, and Kruskal–Wallis and Dunn’s tests for ARI scores. All statistical analyses were performed using SPSS Version 25.0, with the significance level set at α = 0.05.
Results
Intragroup Evaluation of Shear Bond Strength
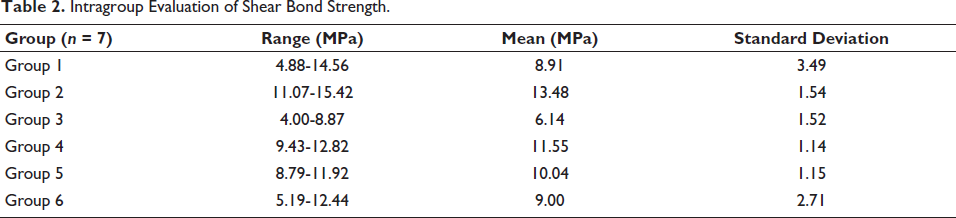
Descriptive statistics for SBS, including mean values, standard deviations, and ranges, are summarized in Table 2 and Figure 5.
Intragroup Evaluation of Shear Bond Strength.
Graph Showing Comparison of Mean Shear Bond Strength.
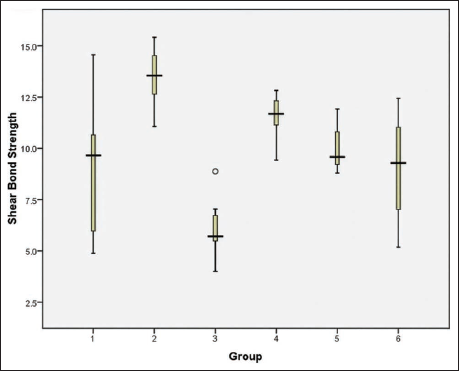
The highest mean SBS was achieved in Group 2 (self-cure acrylic crown + self-cure acrylic bonding agent) at 13.48 MPa, followed by Group 4 (heat-cure acrylic crown + self-cure acrylic bonding agent) at 11.55 MPa. Group 5 (bis-acryl composite + composite bonding agent) and Group 6 (bis-acryl composite + self-cure acrylic bonding agent) recorded mean strengths of 10.04 and 9.00 MPa, respectively. Group 1 (self-cure acrylic crown + composite bonding agent) followed at 8.91 MPa. The lowest mean SBS was recorded in Group 3 (heat-cure acrylic crown + composite bonding agent) at 6.14 MPa.
Intergroup Comparison of Shear Bond Strength
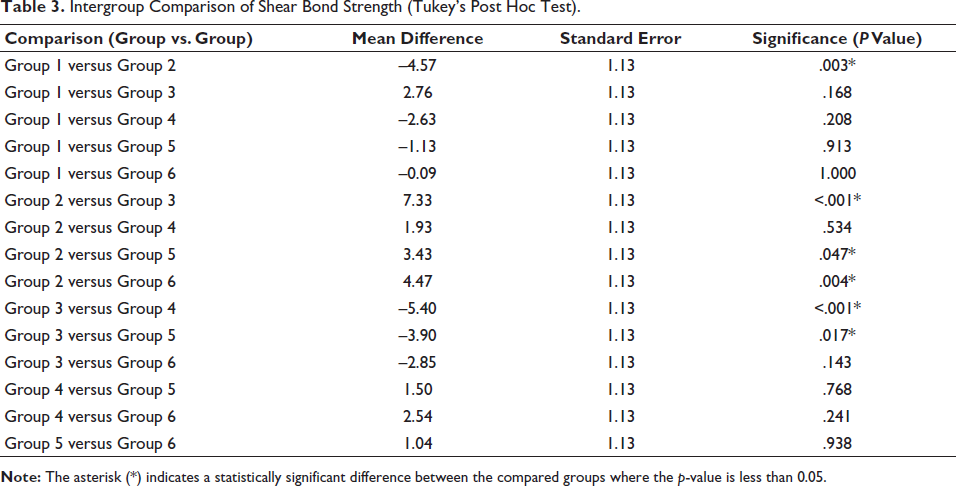
One-way ANOVA revealed significant differences in SBS across the experimental groups (P < .001), leading to the rejection of the null hypothesis. Subsequent intergroup comparisons using Tukey’s post hoc test (Table 3) identified the following significant findings: Group 2 exhibited significantly higher SBS than Group 3 (P < .001), Group 5 (P = .047), and Group 6 (P = .004); Group 4 showed significantly greater SBS than Group 3 (P < .001); Group 5 was significantly stronger than Group 3 (P = .017).
Intergroup Comparison of Shear Bond Strength (Tukey’s Post Hoc Test).
Adhesive Remnant Index Analysis
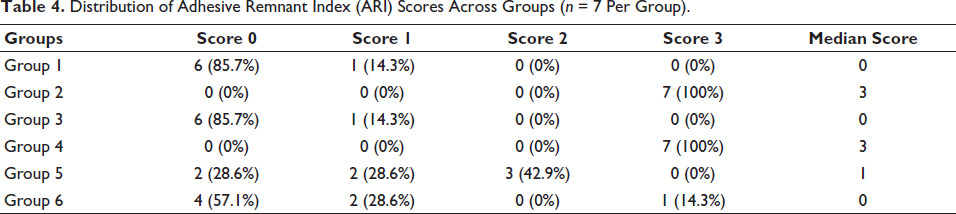
The distribution of ARI scores and median values for each group are detailed in Table 4 and Figure 6.
Distribution of Adhesive Remnant Index (ARI) Scores Across Groups (n = 7 Per Group).
Graph Showing Box Plot for Comparison of Adhesive Remnant Index Scoring.
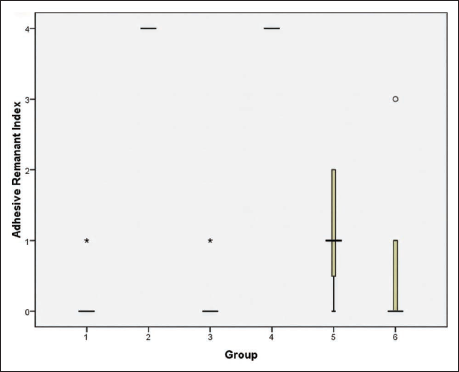
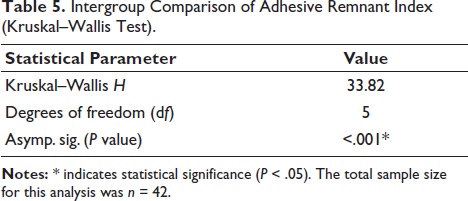
Kruskal–Wallis testing demonstrated significant intergroup differences in ARI scores (P < .001) (Table 5). Groups 2 and 4 (self-cure acrylic bonding) achieved the highest median ARI score of 3, indicating that the bond at the crown–adhesive interface was stronger than the bond at the bracket–adhesive interface. In contrast, Group 1, Group 3, and Group 6 showed median scores ranging from 0 to 1, suggesting more frequent failure at the crown–adhesive interface.
Intergroup Comparison of Adhesive Remnant Index (Kruskal–Wallis Test).
Discussion
The selection of an optimal adhesive system to ensure reliable bond strength is a cornerstone of successful orthodontic therapy, particularly when dealing with provisional restorations. This in vitro study evaluated the SBS of orthodontic brackets on three distinct provisional crown materials using two different bonding protocols. Our findings demonstrate that the choice of bonding agent significantly impacts the resulting bond strength and the mode of interfacial failure, supporting the broader consensus by Pasquale et al. and Pai et al. that adhesive selection is critical to bond performance.1, 8
The Mechanism of Chemical Interaction Versus Micromechanical Retention
The superior SBS observed in Group 2 (13.48 MPa) can be attributed to the chemical affinity and interfacial polymerization between the self-cure acrylic bonding agent and the poly(methyl methacrylate) (PMMA)-based provisional material. Unlike composite resins, which rely primarily on superficial micromechanical retention, the application of methyl methacrylate (MMA) monomer acts as a chemical pretreatment that dissolves and swells the surface of the provisional crown. 9 This creates a gel-like transformation that allows the new acrylic resin bonding agent to interlink with the existing polymer chains, forming a secondary semi-interpenetrating polymer network (IPN). 10 This transitions the interface from a simple surface contact to a deep chemical integration, effectively creating a monolithic-like bond.
Conversely, the lower bond strength observed in heat-cure acrylic groups when using composite resin (6.14 MPa) highlights the limitations of traditional acid etching on acrylic surfaces. While phosphoric acid creates well-defined microporosities for deep resin penetration in enamel, it primarily serves a cleaning function on acrylic.9, 11 Without the chemical “softening” provided by the monomer, the composite resin lacks sufficient chemical compatibility with the highly cross-linked polymer chains of heat-cure acrylic, resulting in a bond that is more susceptible to shear forces.1, 2
Adhesive Performance and Literature Integration
The integration of specific adhesive technologies is critical for clinical success. Our findings align with Pai et al., who emphasized that while conventional systems like Transbond™ XT remain a benchmark, the integration of newer material technologies can significantly influence the performance of the adhesive–bracket interface. 8 This underscores the necessity for material-specific bonding protocols rather than a “one-size-fits-all” approach to orthodontic bonding.
Furthermore, as investigated by Vasudevan and Sundareswaran, the physical characteristics of the adhesive, such as viscosity and surface wetting, play a pivotal role in SBS. 12 In the present study, the low-viscosity self-cure acrylic likely achieved superior surface penetration compared to the more viscous light-cure composite resin. The monomer application likely enhanced surface wettability, allowing the adhesive to flow into the microscopic irregularities created during specimen preparation, thereby augmenting the overall bond integrity.1, 12
Clinical Relevance and Debonding Safety
From a clinical standpoint, achieving an SBS within the 6-8 MPa range is considered essential to withstand both orthodontic and masticatory forces, as suggested by Reynolds and Whitlock et al.4, 13 While most groups in this study met or exceeded this threshold, a balance must be struck between bond stability and surface preservation. SBS values exceeding 13-14 MPa, as seen in our self-cure acrylic groups, sit at the upper limit of the safety threshold. While these values ensure minimal bond failure during treatment, they may elevate the risk of surface damage or fractures during debonding.14, 15
The results of this study demonstrated that Group 2 achieved the highest mean SBS (13.48 ± 1.54 MPa), significantly exceeding the clinically acceptable range of 6-8 MPa established by Reynolds. While this superior bond strength ensures excellent bracket retention during active orthodontic treatment, it warrants clinical caution during the debonding phase. Bond strengths approaching 14 MPa have been associated with an increased risk of cohesive failure within the provisional material or potential enamel/substrate fractures. Therefore, to minimize sudden stress concentrations on the crown surface, clinicians are advised to utilize specialized debonding pliers and a “squeezing” or “peeling” force at the bracket base rather than a pure shear force.
The ARI scores provided further validation of bond quality. In the high-strength groups (Groups 2 and 4), the predominant ARI score of 3 indicated that the bond between the adhesive and the crown was stronger than the bond at the bracket mesh. While this necessitates a more diligent cleanup of the adhesive remnant, it suggests a safer failure mode for the provisional crown material compared to a score of 0, which indicates a complete failure at the crown–adhesive interface.1, 7
Study Limitations and Future Scope
Despite these findings, certain limitations must be acknowledged. While the sample size (n = 7 per group) is smaller than what is typically seen in clinical trials, it is statistically validated for this controlled in vitro design; our post hoc analysis confirmed a power of 0.80, and the low standard deviations observed across primary groups (e.g., Groups 2, 4, and 5) suggest that the cohort provided stable, reproducible mean values. However, this small cohort size may restrict the power to detect subtle differences, particularly in groups where higher standard deviations might occur. Future studies should utilize a priori power calculations and larger cohorts to further strengthen the precision of intergroup comparisons. Additionally, as an in vitro study, these results do not fully account for the complex oral environment involving thermal cycling, pH fluctuations, and salivary contamination, which can degrade materials over time.6, 13
Future research incorporating thermocycling and long-term aging simulations, alongside in vivo clinical trials, is necessary to evaluate the long-term durability of these material-specific bonding protocols under functional loading. Additionally, the research presents the intrinsic limitation of being evaluated for only 24 h instead of long-term, and the bracket must undergo intraoral testing on the crown over an extended period.
Conclusion
Within the limitations of this in vitro study, the following conclusions can be made: When a patient requires full-coverage crowns before orthodontic treatment, placing a self-cure acrylic provisional crown and bonding the orthodontic attachment on it using self-cure acrylic as a bonding agent is the most effective among the groups tested with regard to the bond strength. Placing a heat-cure acrylic provisional crown and bonding orthodontic attachments with a composite bonding agent may not provide clinically adequate bond strength. When bonding on either self-cure or heat-cure acrylic resin provisional crowns, employing self-cure acrylic resin as the bonding agent provides better bond strength than the traditional composite bonding adhesive. Orthodontic attachments can be bonded on provisional crowns made of bis-acryl composite with either a composite bonding agent or self-cure acrylic resin with reasonable bond strength. Within the limitations of this in vitro study, the alternative self-cure acrylic bonding protocol demonstrated significantly higher SBS compared to the conventional composite method across all tested provisional materials. While these values are clinically effective for bracket retention, further in vivo trials are necessary to validate these findings under complex intraoral conditions.
Footnotes
Authors’ Contributions
Conceptualization: JOV, DS. Data curation: JOV. Formal analysis: JOV, DS. Funding acquisition: None. Methodology: JOV. Project administration: JOV, DS, JMH, PA. Visualization: JOV, JMH, PA Writing—original draft: JOV, DS. Writing—review & editing: JOV, DS, JMH, PA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
Obtained from the Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.