
Abstract
Introduction
Cephalometric norms are often population-specific due to ethnic and environmental influences. The Shimla Hills region of Himachal Pradesh, India, represents a distinct population influenced by high-altitude and cold climatic conditions, which are known to affect craniofacial morphology. This study aimed to establish McNamara cephalometric norms for this population and evaluate their deviation from Caucasian standards.
Materials and Methods
Digital lateral cephalograms of 200 adult subjects (18-29 years) native to the Shimla region, with Class I occlusion, were analyzed. Skeletal, dental, and airway parameters were measured and compared with Caucasian norms and regional Indian data.
Results
The Shimla population exhibited a distinct craniofacial pattern. Maxillary and mandibular positions were significantly more retrusive compared to Caucasians. Mandibular length (Co-Gn) was significantly shorter, mirroring South Indian trends more closely than Maratha (Central India) or Caucasian standards. Vertical analysis showed reduced anterior facial height but a steeper mandibular plane angle. Pharyngeal airway dimensions were significantly narrower when compared to Caucasians. Sexual dimorphism was evident, with males generally exhibiting a proportionately larger skeletal framework and females showing slightly more dental proclination.
Conclusion
McNamara’s Caucasian norms are not directly applicable to the Shimla population. The established population-specific norms reflect a unique phenotype of bimaxillary retrusion and reduced airway space, emphasizing the need for individualized diagnostic standards in orthodontic and orthognathic planning for this region.
Introduction
Modern orthodontics emphasizes individualized treatment to achieve functional occlusion and facial harmony, which requires an understanding of normal craniofacial growth and population-specific morphological variation. Age, sex, race, facial type, and malocclusion severity significantly influence craniofacial parameters and must be considered during treatment planning.1, 2
Radiographic cephalometry, introduced by Broadbent 3 and Hofrath 4 in 1931, remains a cornerstone of orthodontic diagnosis, enabling standardized assessment of skeletal and dental relationships through angular and linear measurements. Reliable cephalometric norms are essential for identifying deviations from ideal craniofacial relationships.5, 6 Several analyses, including those by Downs, 7 Steiner, 8 Tweed,9, 10 Ricketts, 6 Sassouni, 11 Jacobson, 12 McNamara, 13 and Harvold, 14 have contributed to defining these standards.
McNamara’s analysis utilizes linear measurements referenced to the nasion perpendicular, facilitating objective assessment of sagittal and vertical skeletal relationships in orthodontic and orthognathic planning. 13 This innovative approach is notable for its sensitivity not only to the position of the teeth within the supporting bone but also to the spatial relationships among the jaws and cranial base structures. However, most cephalometric norms are derived from Caucasian populations, and significant ethnic variations in craniofacial morphology have been documented,15-17 suggesting that a “one-size-fits-all” approach fails to account for the unique morphological characteristics inherent to diverse ethnic groups.
India’s marked ethnic and geographic diversity has led to the establishment of population-specific cephalometric norms, with several studies reporting significant deviations from Caucasian standards.18-24 Application of McNamara’s analysis across different global and Indian populations has consistently demonstrated variations in skeletal, dental, and airway parameters, underscoring the need for localized normative data.19, 25-28
The population of the Shimla hills and surrounding regions, shaped by specific high-altitude and cold climatic conditions, exhibits distinct craniofacial phenotypic characteristics that differentiate it from Caucasian and other Indian ethnic groups.22-24 Although sexual dimorphism in craniofacial structures is well established,29-32 limited studies have evaluated this specific cohort using McNamara’s cephalometric analysis. Therefore, the present study aimed to establish population- and gender-specific craniofacial and airway norms for the Shimla Hills cohort. Furthermore, we aimed to compare these parameters with established Caucasian norms and previously published Indian data to evaluate their diagnostic and clinical relevance. The findings are intended to provide population-specific reference values to enhance diagnostic accuracy and treatment planning in local orthodontic practice.
Materials and Methods
This cross-sectional study was conducted at a government-run teaching hospital in Northern India, following approval from the Institutional Ethical Committee.
The sample size was calculated based on previous cephalometric studies19, 32 conducted on Indian populations. To detect a clinically significant difference of 1 mm in linear measurements and 1° in angular measurements, with a power of 80% and a significance level (alpha) of 0.05, a minimum sample size of approximately 64 subjects per group was required. The present study included a total of 200 subjects aged 18-29 years, obtained from departmental records and patients seeking orthodontic treatment. This sample size exceeded the minimum requirement, ensuring high statistical power and adequate representation of the population’s morphological diversity.
Sample Stratification
To facilitate the evaluation of sexual dimorphism within the cohort, the total sample of 200 subjects was divided into two distinct groups based on biological sex:
Group 1: 88 males Group 2: 112 females
Inclusion criteria required subjects to have an Angle’s Class I molar relationship, a well-balanced facial profile, a full complement of teeth, minimal crowding or spacing, and no prior orthodontic treatment. To ensure ethnic relevance, all included subjects were verified as natives of the Shimla district and adjacent mid-hill regions of Himachal Pradesh.
Radiographic Technique
Standardized digital lateral cephalometric radiographs were obtained using the Carestream CS 8100 SC digital cephalometric unit, with subjects positioned in natural head position, teeth in maximum intercuspation, and lips in a relaxed state. The lateral cephalograms were analyzed using McNamara’s cephalometric analysis to evaluate skeletal, dental, and pharyngeal airway parameters. All radiographs were traced and measured by a single investigator to ensure consistency. To eliminate intra-examiner error, a subset of 40 cephalograms was retraced after a 3-week interval, and Dahlberg’s formula was applied to assess reliability.
Cephalometric Analysis
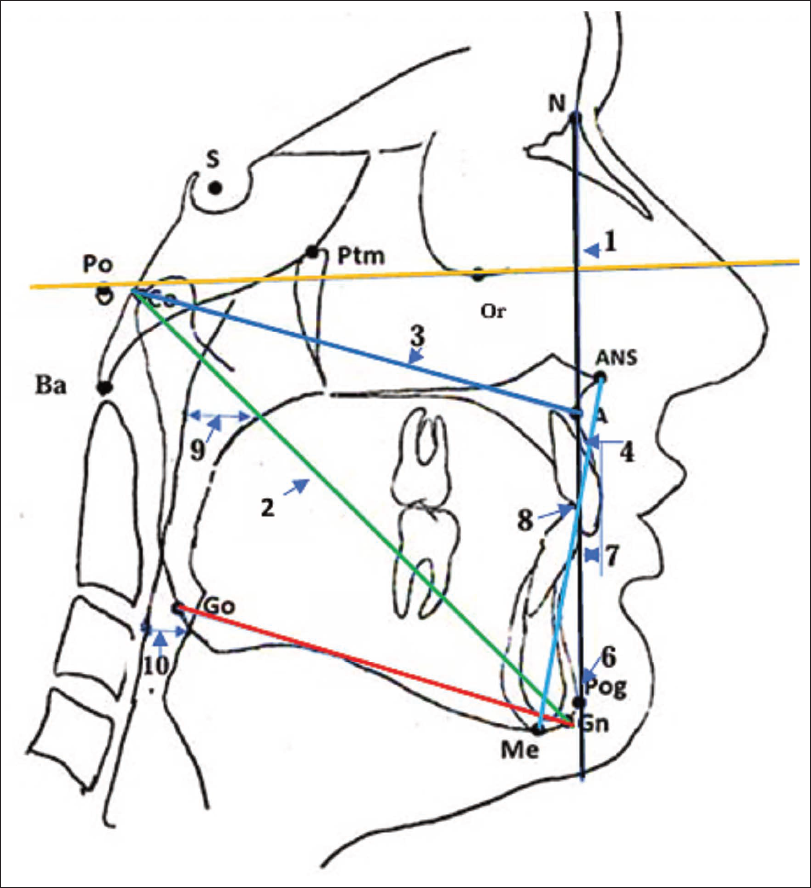
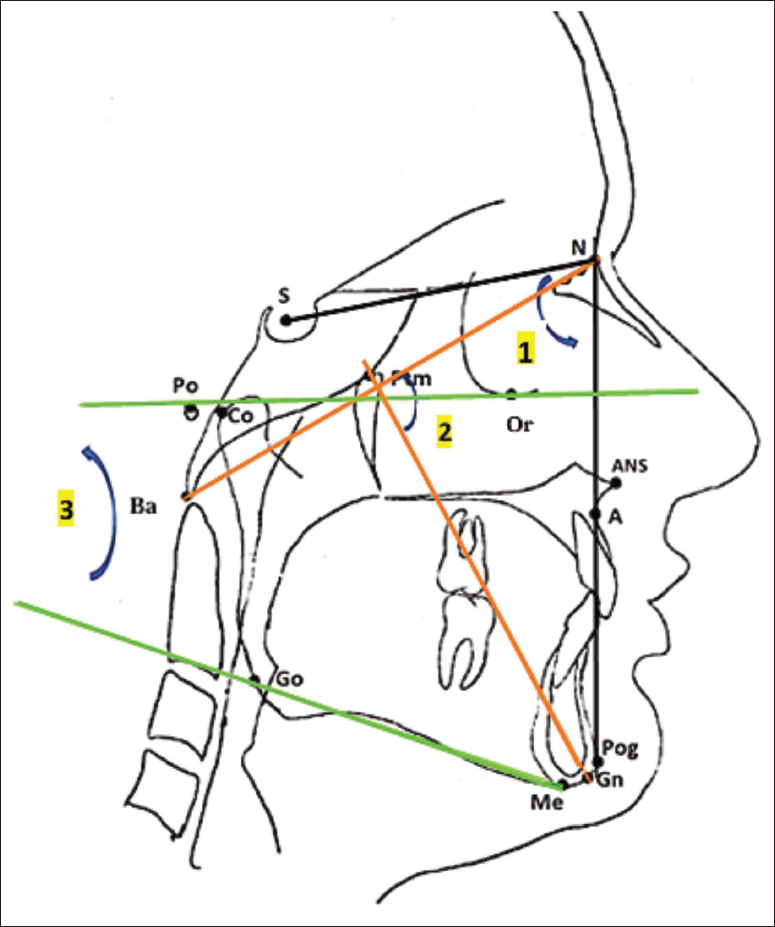
McNamara’s cephalometric landmarks and measurements were identified and traced manually. A total of 13 parameters were evaluated in the present study, comprising 10 linear (Figure 1) and 3 angular measurements (Figure 2). Parameters evaluating the maxilla–mandible relationship, mandibular and midfacial lengths, dentoalveolar positions, vertical facial dimensions, and airways were assessed.
Statistical Analysis
The mean values and standard deviations were calculated and statistically compared with established Caucasian norms using a one-sample t-test. In addition, intergender comparisons were performed to assess sexual dimorphism within the Shimla population. The method error was calculated using Dahlberg’s formula to determine the mean technical error of measurement. Additionally, the Intraclass Correlation Coefficient (ICC) was employed to assess the consistency of the repeated measurements; all ICC values exceeded 0.80, indicating excellent reliability. The significance of the P value was determined at P < .05 (significant), P < .01 (highly significant), and P < .001 (very highly significant).
Results
The results showed that 11 parameters in males and 9 parameters in females demonstrated statistically significant differences when compared with the Ann Arbor Caucasian sample.
In Males
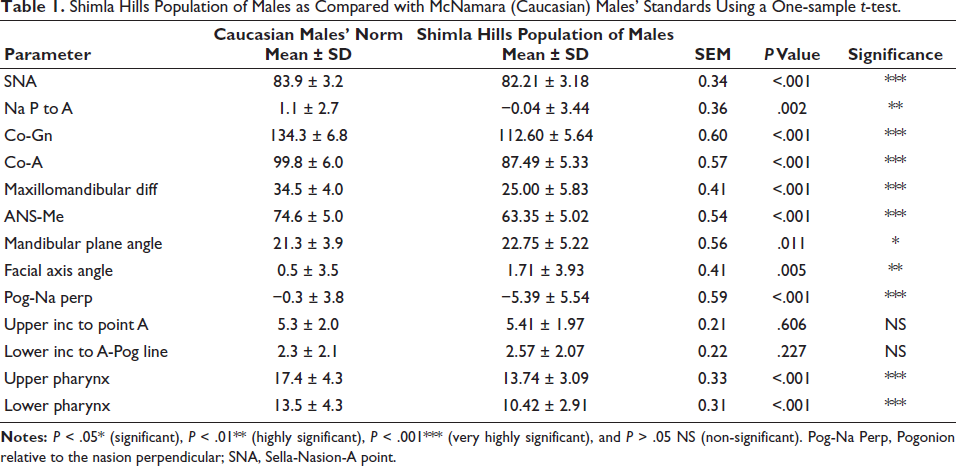
Sella-Nasion-A point (SNA; P < .001), effective midfacial length (Co-A; P < .001), mandibular length (Co-Gn; P < .001), maxillomandibular differential (P < .001), lower anterior facial height (ANS-Me; P < .001), upper pharyngeal width (P < .001), and lower pharyngeal width (P < .001) were significantly smaller in the Shimla population as compared to Caucasian males. In contrast, the mandibular plane angle (P < .05) and facial axis angle (P < .05) were significantly greater. Pogonion relative to the nasion perpendicular (Pog-Na perp) was significantly more negative, indicating mandibular retrusion relative to the cranial base (P < .001). No statistically significant differences were observed for upper or lower incisor position (P > .05; Table 1).
Shimla Hills Population of Males as Compared with McNamara (Caucasian) Males’ Standards Using a One-sample t-test.
In Females
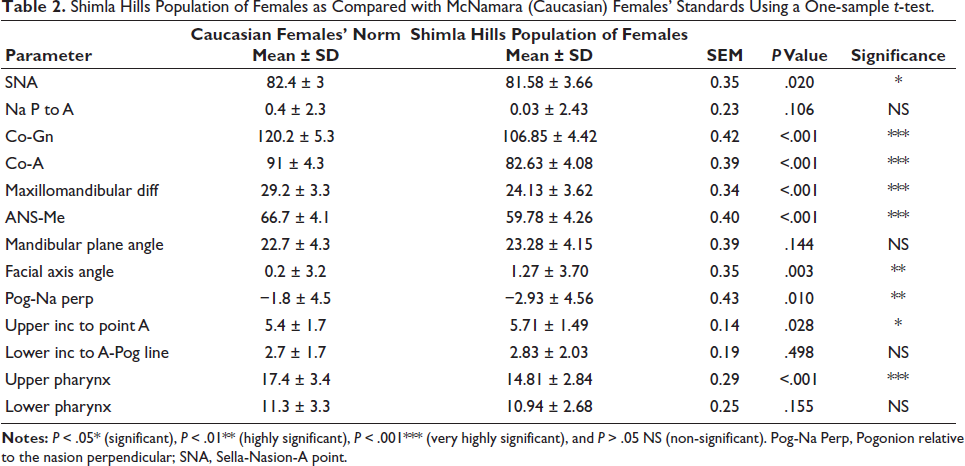
SNA (P = .020), effective midfacial length (Co-A; P < .001), mandibular length (Co-Gn; P < .001), maxillomandibular differential (P < .001), and lower anterior facial height (ANS-Me; P < .001) were significantly smaller in the Shimla population (Table 2). Pog-Na perp was significantly more retruded (P = .010), while the facial axis angle was significantly greater (P = .003). Upper incisor position relative to point A was significantly increased (P = .028). Upper pharyngeal airway width was significantly reduced (P < .001), whereas lower pharyngeal airway dimensions did not differ significantly from the Caucasian norms (P = .155; Table 2).
Shimla Hills Population of Females as Compared with McNamara (Caucasian) Females’ Standards Using a One-sample t-test.
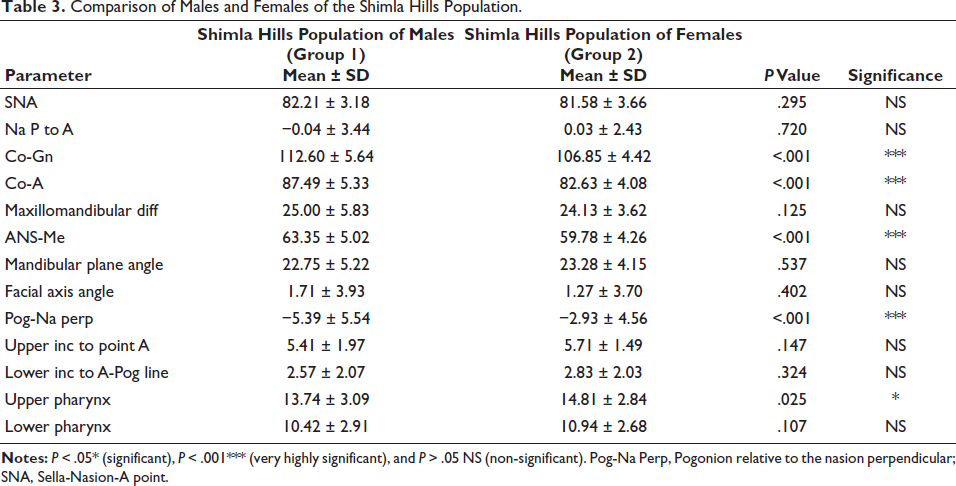
Comparison of McNamara cephalometric parameters between groups 1 and 2 of the Shimla population revealed statistically significant sex-related differences in selected skeletal and airway parameters. Males exhibited significantly greater mandibular length (Co-Gn; P < .001), effective midfacial length (Co-A; P < .001), and lower anterior facial height (ANS-Me; P < .001) compared with females. Pog-Na perp was significantly more negative in males (P < .001). Upper pharyngeal airway width differed significantly between sexes, with higher values observed in females compared with males (P = .025; Table 3).
Comparison of Males and Females of the Shimla Hills Population.
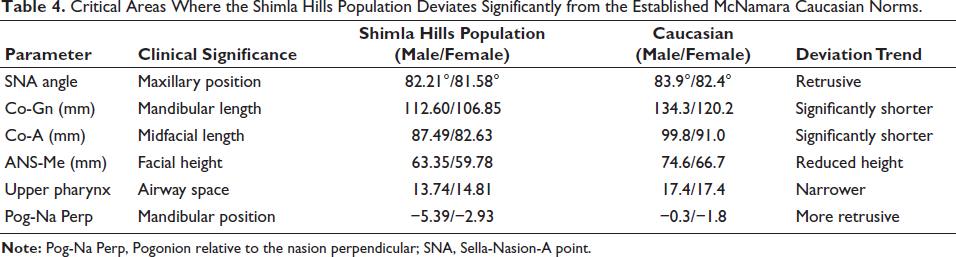
Based on the results of our study, Table 4 highlights the most critical areas where the Shimla Hills population deviates significantly from the established McNamara Caucasian norms.
Critical Areas Where the Shimla Hills Population Deviates Significantly from the Established McNamara Caucasian Norms.
Discussion
Cephalometric analysis is fundamental to orthodontic diagnosis and treatment planning; however, the applicability of normative values is influenced by genetic, ethnic, and environmental factors.15-17 McNamara’s analysis, 13 though clinically efficient and widely used, was derived from Caucasian samples, warranting careful application in diverse populations.
India’s extensive ethnic and regional diversity results in considerable variation in craniofacial morphology.27, 29, 33 The Shimla district and surrounding hills present an intricate mosaic of high mountain ranges (Dodra-Kwar region bordering Uttarakhand state and Tibet), hills bordering Kinnaur and Mandi districts of Himachal Pradesh, with an altitude ranging from 2,000 to 3,500 m above mean sea level. This cohort represents a distinct subgroup potentially influenced by specific high-altitude and environmental factors. The present study evaluated the applicability of McNamara’s analysis in this cohort and established sex-specific cephalometric norms.
Both male and female subjects demonstrated significant maxillary and mandibular retrusion relative to the cranial base when compared with Caucasian norms. 13 Reduced SNA values and negative nasion perpendicular measurements indicated posterior positioning of both jaws. In addition, effective midfacial (Co-A) and mandibular (Co-Gn) lengths were significantly smaller in both sexes, resulting in a reduced maxillomandibular differential. These findings suggest that the characteristic craniofacial pattern of the Shimla population represents a proportionately smaller bimaxillary skeletal framework rather than isolated maxillary or mandibular deficiency. Similar patterns have been reported in other North Indian, 33 Indo-Aryan, 21 and Himalayan Kathmandu populations, 34 whereas, in contrast, Turkish 26 and Black South African populations 35 frequently demonstrate craniofacial dimensions comparable to or exceeding Caucasian norms.
Vertical skeletal analysis revealed significantly reduced lower anterior facial height in both sexes. Despite this reduction, males in our study exhibited a steeper mandibular plane angle, whereas females demonstrated higher facial axis values compared with Caucasian norms. 13 This combination of reduced anterior facial height and a steeper mandibular plane is a unique finding that contrasts with the typical vertical growth patterns seen in Caucasian populations. Comparable findings have been reported in Maratha 19 and Himalayan populations, 34 while increased vertical dimensions are more common in Saudi 36 and Black South African groups. 35
Despite the skeletal retrusion observed in both jaws, dentoalveolar compensation was minimal. Upper and lower incisor positions in the males of this population were comparable to Caucasian norms, 13 whereas females demonstrated only mild maxillary incisor protrusion. This suggests that the craniofacial morphology of the Shimla population is predominantly skeletal in origin rather than dentoalveolar, in contrast to the bimaxillary dentoalveolar protrusion reported in South Indian 27 and African populations. 35
A clinically important finding was the reduction in pharyngeal airway dimensions. Upper pharyngeal airway width was significantly reduced in both sexes, while lower pharyngeal airway width was reduced only in males. These findings are consistent with other Indian32, 37 and Nepalese studies. 38 The reduction in upper airway space observed in this cohort likely reflects evolutionary and physiological adaptations to the local environment. Populations native to high-altitude and cold climates experience evolutionary pressure to develop narrower nasal and upper airway dimensions to increase air turbulence, which aids in warming and humidifying harsh mountain air before it reaches the lower respiratory tract. 39 This adaptive morphology, combined with the inherently smaller and more retrusive jaw lengths identified in this cohort, contributes to the reduced baseline airway dimensions.
While Vaid et al. 23 and Uppada et al. 40 established norms for Mongoloid and Tibeto-Burman groups in the broader region, our data suggest that the Shimla population represents a distinct ethnic admixture. Although these groups share high-altitude skeletal adaptations (such as reduced overall skeletal dimensions), the Shimla cohort displays a less protrusive craniofacial model than these traditional counterparts.
The findings of the present study demonstrated that sexual dimorphism was significant only in selected skeletal parameters, not broadly across all skeletal measurements within the Shimla hills cohort. Males exhibited significantly greater midfacial length (Co-A), mandibular length (Co-Gn), and lower anterior facial height (ANS-Me) than females, indicating larger overall craniofacial dimensions. Mandibular sagittal position also differed significantly, with males showing a more negative Pog-Na perp, reflecting greater mandibular retrusion relative to the cranial base. Dentoalveolar parameters showed minimal sexual dimorphism, with only a tendency toward greater incisor protrusion in females. Airway assessment revealed significant sexual variation, with females demonstrating a wider upper pharyngeal airway compared to males, whereas lower pharyngeal dimensions did not differ significantly.
Our study was limited by its cross-sectional design and reliance on two-dimensional cephalometric analysis. Furthermore, a potential limitation could be that baseline magnification differences between our Carestream unit and the historic Ann Arbor equipment may introduce minor systematic bias in linear measurements.
Clinical Implications
The reduced midfacial and mandibular dimensions in the Shimla population suggest that the application of Caucasian norms during orthognathic surgical planning may result in excessive jaw advancement and an unnaturally protrusive facial profile.
Given the inherently narrower pharyngeal airway dimensions, surgical movements that may further compromise airway space, particularly mandibular setback procedures, should be approached with caution. Pre-surgical airway evaluation should be an integral component of treatment planning to ensure that esthetic correction does not adversely affect upper airway patency and long-term respiratory function.
Conclusion
The Shimla population exhibits distinct cephalometric characteristics when evaluated using McNamara’s analysis, with significant deviations from Caucasian norms.
A proportionately smaller craniofacial skeletal framework with retrusive maxillomandibular relationships and reduced lower anterior facial height was observed.
Pharyngeal airway dimensions were narrower, particularly in the upper airway, with minimal dentoalveolar compensation.
Sexual dimorphism was evident, with males showing larger skeletal dimensions and females demonstrating relatively greater dental proclination.
The significant ethnic and gender-related differences observed in this study justify the establishment of population-specific cephalometric norms. McNamara’s Caucasian norms are not directly applicable to the Shimla population, and the newly derived normative values provide a more reliable reference for accurate diagnosis and individualized treatment planning in this region.
Authors’ Contributions
Anuranjan Sehgal: Concept, sample acquisition, cephalometric tracing, analysis or interpretation of data, and drafting of the original manuscript.
Sankalp Sood: Supervision, conceptualization, study design, and critical revision of the article for intellectual content.
Monika Mahajan: Supervision and editing.
Susheel Negi: Supervision.
K. S. Negi: Conceptualization, supervision, and study design.
Dimple Chainta: Supervision.
Nishant Negi: Supervision.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Ethical Committee of H.P. Government Dental College & Hospital, Shimla. Formal clearance was accorded and conveyed on May 31, 2024 (Ref. No. HFW(GDC)B(12)50/2015-Vol-II-2319), following the recommendations of the committee meeting held on March 2, 2024.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Informed Consent
Informed consent was obtained from all individual participants included in the study. All participants were briefed on the nature of the cephalometric study and the use of their diagnostic records for research purposes, ensuring that their privacy and anonymity were maintained in the final report.