
Abstract
This study predicted music performance anxiety in skilled flute players. Participants played two orchestral excerpts under audition conditions. Prior to the performance, participants completed the State (STAI-S) and Trait (STAI-T) Anxiety questionnaires from the State–Trait Anxiety Inventory (STAI), the Kenny Music Performance Anxiety Inventory (K-MPAI) and the Fear of Negative Evaluation (FNE). They also had electromyography (EMG) and electrocardiography (ECG) measures taken before and during their performances and provided information on their musical achievements and how much time they had spent practicing the test pieces. Specially developed rating scales assessed prior level of musical achievement. Hierarchical regression analysis assessed relationships between each group of variables entered and music performance anxiety assessed with K-MPAI. The final model included the anxiety measures (STAI-T, STAI-S, FNE), a rating of the highest level of achievement as a soloist, number of minutes they practiced the test piece, and the physiological measures (EMG and heart rate [HR]). This model accounted for 70.4% of the variance in music performance anxiety (MPA) but only STAI-S and FNE contributed significant unique variance to the prediction of it. A number of methodological issues were identified in studies on music performance anxiety, and suggestions made for the conduct of future research into music performance anxiety.
A number of common factors have been implicated in both the experience of music performance anxiety and expert ratings of musical performance in studies that have simultaneously addressed both music performance anxiety and performance quality (Craske & Craig, 1984; Kirchner, 2002; LeBlanc, Jin, Obert, & Siivola, 1997; Lederman, 1999). These include level of accomplishment as a musician (Kokotsaki, 2006), technical mastery of one’s instrument, the difficulty of the work to be performed (Horvath, Herleman, & McKie, 2006); the amount and quality of practice undertaken (Jabusch, Alpers, Kopiez, Vauth, & Altenmuller, 2009; Repp, 2005), psychological factors, such as trait anxiety, situational anxiety, and fear of negative evaluation (Kenny, 2009; Reiss, 1991) and physiological measures such as muscle tension (Steptoe, 1983) and heart rate (HR) (Abel & Larkin, 1990).
Research on performance anxiety in general and music performance anxiety in particular has focused on its psychological features (worry, dread, and apprehension about an impending performance), physiological manifestations (“flight-and-fight” responses of somatic arousal, which include muscle tension, tremor, dry mouth, and increased heart rate or palpitations) and observed behaviours (shaking, trembling). Wilson (2002) developed a three-dimensional model of music performance anxiety in which three factors interact to determine the level of anxiety that will be experienced during performance. These are (a) the trait anxiety of the performer; (b) the degree of task mastery achieved of the works to be performed; and (c) the degree of situational stress that accrues to the performance (presence, size and characteristics of the audience; the “stakes” of the performance—audition, solo recital, examination, etc). In the music performance literature, Wilson (2002) is one of the few theorists who specifically addressed the issue of task mastery as an important component in both the etiology and outcomes of music performance anxiety. His model makes similar predictions to those of Martens, Burton, Vealey, Bump, and Smith (1990) and Hardy and Parfitt (1991) with respect to the various interactions of these three factors. Martens et al. (1990) noted the separate contributions of cognitive anxiety, related to concerns about the consequences of failure, and somatic anxiety, defined as a negative perception of the meaning of physiological arousal prior to performance in competitive sport anxiety. Hardy, Beattie, and Woodman (2007) added a third factor to their model, that is, effort required to perform the task. They hypothesized that a performance catastrophe may be due to the relationship between cognitive anxiety and effort rather than or as well as cognitive anxiety and physiological arousal (experienced as somatic anxiety). In two studies that manipulated task difficulty as a way of increasing effort, and social pressure and ego threat instructions to manipulate levels of cognitive anxiety (worry), their findings supported a processing efficiency theory explanation of anxiety-induced performance catastrophes.
McNally (2002), in a critique of a number of theories of sports performance anxiety noted the failure of researchers to consider how practice interacts with the effects of cognitive or somatic arousal. The importance of good practice habits has been acknowledged through the ages (Flesch, 1939; Galamian, 1962; Spohr, 1833). Elite musicians spend an average of 4 hours per day in deliberate, concentrated practice (Ericsson, Krampe, & Tesch-Romer, 1993). Ostwald (1994) estimated that a 22-year-old violinist making her concert debut will have practised for about 15,000 hours to prepare for a debut concert performance. The goal of practice is to achieve mastery of the complex tasks required of musicians; it is almost a truism to say that performance quality is strongly related to adequate practice. However, the amount of time practiced is not a sufficient condition to achieve mastery; the type and quality of practice is also obviously important (Ericsson et al., 1993). For a professional woodwind instrumentalist it is usual to divide practice time into three sections—work on tone (including sonority exercises), work on technique (including scales and studies), and work on pieces (including orchestral excerpts and repertoire) (Crawford, 2003). Repetitive slow practice with the aid of a metronome underpins the performance preparation of most aspiring professional musicians (Fortune, 2007).
In building models of music performance anxiety that include physiological measures such as electromyography, care must be taken to identify the specific physiological demands that different instruments place on the body of the performer and to select those relevant muscles for investigation. The muscles most likely to become tense in a performing situation for flute players are those under the highest demand in terms of fine motor skills, which for flute players include the facial muscles involved in forming the embouchure necessary to play the instrument and the upper limb muscles that are principally involved in instrument support and operating the keys. Flute players must hold their left arm pronated at shoulder height in front of the body with wrist in slight flexion. They must also hold the right arm up at 90° to the resting position with a further 90° flexion at the elbow, whilst moving the fingers of both hands during performance. This means that the upper limbs and trunk are in constant repetitive use during flute performance (Fortune, 2007). Muscle tension may occur due to either the physical demands of playing the instrument, from excessive playing time without rest breaks, or due to the complexity of the music being performed even in the absence of music performance anxiety.
Kenny (2009) recently offered the following definition of music performance anxiety, based on all of the available research literature; it will serve as the working definition of music performance anxiety (MPA) in this paper, as operationalized in the Kenny Music Performance Anxiety Inventory:
Music performance anxiety is the experience of marked and persistent anxious apprehension related to musical performance that has arisen through specific anxiety-conditioning experiences and which is manifested through combinations of affective, cognitive, somatic and behavioural symptoms. It may occur in a range of performance settings, but is usually more severe in settings involving high ego investment and evaluative threat. It may be focal (i.e. focused only on music performance), or occur comorbidly with other anxiety disorders, in particular social phobia. It affects musicians across the lifespan and is at least partially independent of years of training, practice, and level of musical accomplishment. It may or may not impair the quality of the musical performance (2009, p. 433).
This study explored the interrelationships between some of the factors outlined in this definition; that is, between generalized anxiety (worry factor), situational anxiety, physiological arousal, task difficulty, task mastery, and practice and assessed their relative contributions to the experience of music performance anxiety during skilled musical performance.
Method
The study was approved by the Human Research Ethics Committee of the University of Sydney. All participants signed an informed consent for all aspects of the research prior to commencement.
Participants
Participants were tertiary students of flute currently enrolled in the Bachelor of Music (with a major in flute performance) (in any of the 4 years of that undergraduate degree), Master of Music (Performance), or who had graduated from these courses in the previous year from the Sydney Conservatorium of Music. A recruitment circular was distributed by post to 30 eligible flute students. In addition, signs were located at the conservatorium, flute society meetings, and orchestral rehearsals. A total of 24 flute players expressed interest in participating and were provided with the participant information statement, of whom 20 (three males, 17 females) flute players subsequently completed the study. Seventeen (n = 17) were enrolled in the Bachelor of Music and three in the Master of Music (Performance) degrees. Participants were aged between 19 and 32 years of age. They had been studying flute for a minimum of 10 years and a maximum of 22 years. Fifteen of the participants (75%) wanted to become professional musicians, three were undecided, and two did not wish to become professional musicians.
Procedure
We attempted to mimic the audition setting, in which applicants for orchestral positions play unaccompanied set works comprising extracts from orchestral flute parts. Ten days before the scheduled simulated audition, participants were sent two of the psychological (FNE and STAI [trait form only]) questionnaires, the required orchestral extracts, an instruction letter, a map of how to get to the venue, and clothing instructions. These practices are employed in most orchestral auditions, thus giving participants exactly the same time frame in which to prepare the music. The STAI-S was completed on the day of testing immediately before the performance.
All performances were audio-recorded. Whilst playing the musical protocol (described in the following lines) participants had an electromyographic trace taken and their HR recorded. In keeping with electromyography (EMG) studies involving the left upper trapezius muscle, participants were requested in their instruction package to wear tank tops, singlets or vests and to avoid polo-necked garments and collared shirts to allow the traces in the neck to be unimpeded by clothing. The performances were recorded in audio format. All testing occurred in four 2-hr periods in the Australian Centre for Applied Research in Music Performance (ACARMP), Sydney Conservatorium of Music, The University of Sydney. An expert flute player with extensive adjudicator experience subsequently blind rated all the performances in terms of musical and technical proficiency from the industry standard recording.
Prior to performance, participants were familiarized with the markings on the floor to indicate where to stand and were encouraged to warm up their instruments and become accustomed to the room acoustics. The microphone was lined up to the embouchure during warm-up practice. All participants played their own instruments, which were solid silver, open-hole flutes made by Powell, Brannen, Muramatsu, Nagahara, and Altus. None of the participants performed on gold, platinum, or wooden instruments. Several instruments had B foot joints.
After warm-up, surface electromyography electrodes were attached to the central belly of the left upper trapezius muscle and participants were given the opportunity to accommodate to this with a further period of warm-up playing. Sound levels were then calibrated and the first piece of music (the unevaluated piece determined by randomization) was placed on the music stand. Prior to commencement, participants completed the State Anxiety Inventory (STAI-S). Powerlab recording was commenced and the neutral arm posture maximal voluntary contraction (MVC) was recorded with the levels adjusted appropriately. Once measured successfully the MVC was repeated for flute-playing posture. Participants were then instructed to begin playing after the researcher tapped on their shoulder using three counts. The performance protocol included technical work (scales) and the set pieces. All participants played the first piece until requested to stop by the researcher. The instructions to the second piece were standardized thus: “All the recordings of the performances today of the (Strauss/Debussy) are being sent to a panel of expert judges for their evaluation.” This instruction was given to manipulate (i.e., increase) the level of performance anxiety experienced.
Measures
Achievement measures
Solo and ensemble rankings
Two musical performance achievement rating scales were developed for use in this study. The first and second authors, both performing musicians, constructed the scale according to the various routes by which music students train and the milestones achieved during their training. The first author then consulted four senior pedagogues about the weight they would give to some of the musical milestones listed. The 10 items were presented to the four pedagogues in random order and they were asked to rank them in order from 1 to 10 based on their perception of the level of achievement attained. These rankings were unanimous for both the solo performance and ensemble performance ranking scales.
Participants were asked to give details about their highest level performing experience in solo and ensemble settings. Participants were awarded points on the 10-point scale, as follows:
Solo performance ranking scale:
1 or 2. Achievements below Grade 8 with an examining board such as Trinity College of Music, London, or Australian Music Examination Board.
3. Achieved Grade 8 level or equivalent level with an examining board such as Trinity College of Music, London, or Australian Music Examination Board.
4. Associate diploma from recognized examining board.
5. Licentiate diploma from recognized examining board.
6. Junior recital (requirement of Bachelor of Music degree).
7. Senior recital (requirement of Bachelor of Music degree).
8. Masters’ recital (requirement of Master of Music Performance degree).
9. Recital or concerto performed outside the conservatorium; played as a soloist with a community or youth orchestra.
10. Played as soloist with a professional symphony orchestra (e.g., ABC Young Performer’s Awards).
Ensemble performance ranking scale:
1 or 2. Small ensemble experience at high school level.
3. Completed requisite small ensemble components of their undergraduate degree.
4. Players selected for the Conservatorium Symphony Orchestra; playing as a member of the resident “Stables” flute choir.
5. Playing in weekend youth orchestras such as the SBS Youth Orchestra or Sydney Youth Orchestra.
6. Selected to tour internationally with SBS Youth Orchestra or Sydney Youth Orchestra.
7. Member of Australian youth orchestra.
8. Member of a semiprofessional orchestra (or equivalent).
9. Played casually with a professional orchestra.
10. Held a contract with a professional symphony or pit orchestra. (None of the students or recent graduates in the study had yet held a full-time position with either a symphony or pit orchestra.)
Psychological measures
State–Trait Anxiety Inventory – Trait (STAI)
The State–Trait Anxiety Inventory (STAI; Spielberg, 1983; Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983) is a 40-item scale used to measure state and trait anxiety. High scores indicated higher levels of trait anxiety. Good to excellent internal consistency has been reported for both scales (Cronbach’s alphas between 0.86 and 0.95) across adult, college, high school, and military recruit samples (Spielberger et al., 1983). Adequate 30-day test-retest reliability with high school students (r = 0.71 [state]; r = 0.75 [trait]) and 20-day test-retest reliability with college students has been reported (r = 0.76 [state]; r = 0.86 [trait]) (Spielberger et al., 1983). Convergent validity of the STAI-T and other trait measures of anxiety are evident among both community samples and samples with an anxiety disorder. Internal consistency of the state (α = 0.90) and trait scales (α = 0.82) in the present sample was strong.
Kenny Music Performance Anxiety (K-MPAI)
This inventory (Kenny, 2011) was developed to assess the emotion-based theory of anxiety proposed by Barlow (2000) as it applies to anxiety in the context of music performance. Items were either specially constructed or selected from other scales to address each of Barlow’s theoretical components, including evocation of anxious propositions (e.g., uncontrollability, unpredictability, negative affect, situational cues); attentional shift (e.g., task or self-evaluative focus, fear of negative evaluation); and physiological arousal. In addition, two memory items were added because of the importance of performing from memory in major solo performances. Questions are answered on a 7-point Likert scale ranging from 0 (strongly disagree) to 6 (strongly agree). Higher scores indicate greater anxiety and psychological distress. The internal reliability of the scale has been assessed on three samples—opera chorus artists (Kenny et al., 2004); tertiary-level music and dance students (Kenny, Ackermann, & Driscoll, 2009); and professional orchestral musicians (Kenny, 2011)—all demonstrating excellent internal reliability > 0.90.
Fear of Negative Evaluation Scale (FNE)
The Fear of Negative Evaluation Scale (FNE; Watson & Friend, 1969) assesses expectations of being evaluated negatively. The FNE consists of 30 items that are answered either “true” or “false.” Higher scores indicate higher fear of negative evaluation. High internal consistency (α = 0.94–0.96), strong 1-month test-retest reliability (r = 0.78–0.94), and criterion validity have been demonstrated for this measure (Watson & Friend, 1969). Across several college samples (Watson & Friend, 1969), the FNE significantly correlated with a measure of general anxiety (r = 0.60), social-evaluative anxiety (r = 0.47), and social approval (r = 0.77). Although a shortened 12-item version of the original FNE was used in this study, internal consistency of the FNE in the present sample was α = 0.88.
Music protocol
Technical work (scales)
Participants were requested to play a G major scale all slurred followed by an E flat melodic minor scale double tongued. G major is a relatively straightforward scale to play on the flute due to its simple key signature, ease of execution, and general familiarity amongst flute students from an early age. Some players presented the scale across the entire range (three octaves commencing from Middle C). Others played in an (easier) two-octave format. Both versions “sit well under the fingers” and are easily rendered legato. The scale is frequently found in the flute literature, prominent examples including the Mozart’s Quantz and Vivaldi’s G major flute concertos.
E flat melodic minor scale is one of the most difficult scales on the flute. The key signature is 5 flats and the melodic minor scale differs in execution between the ascending and descending portion. The scale is difficult to play across the entire range. There are several problems with the execution of the descending portion, one of which is the need to alternate rapidly from c-flat to b-flat. Use of the thumb Briccialdi key is awkward and places undue stress on the first metacarpal joint with repeated use. Better alternatives include the lever or first key of the right hand, use of which requires greater coordination overall. In addition the double tonguing action is demanding, especially since the scale starts in the low register of the instrument. All participants attempted the scale at some speed. Many took several attempts to get it right due to incorrect notes and imprecision of articulation and some attempted to play single notes. Most attempted the scale across two octaves; some tried for the entire range (C1 to C flat 4) and one player played this scale in an impressive three-octave version with good execution of the altissimo notes: D4, E flat 4, and D flat 4.
On the 10-point rating scale, points were awarded for execution elements of each of the scales. The maximum score for the G major scale was 4 and for the E flat melodic minor, 6 points. For G major scale, points were awarded for accuracy, fluency, phrasing, and tone quality; for the E flat melodic minor scale, correctness, fluency, tempo, articulation, tone quality, and quality of double tonguing were assessed and awarded points accordingly.
Set works
L’Après-Midi d’un Faun (Debussy)
Claude Debussy’s Prelude to L’Après-Midi d’un Faun (Figure 2) work begins with a solo flute arabesque that recurs several times throughout the short work and represents the fantasies of the faun on a hot summer’s afternoon. The scoring protocol for the Debussy excerpt was as follows (note: each mark required the standard to be met for all grades below the grade given):
3. (or lower) Could not play notes correctly, adhere to rhythm or tempo, or capture the style.
4. Played the correct notes and was rhythmically correct at the marked tempo.
5. Maintained an even tone quality in the excerpt with good pitch control.
6. Observed marked articulation and dynamic changes and displayed good breath control.
7. Imbued each recurrence of the phrase with interesting variations in tone color and vibrato.
8. Obtained a distinctive and evocative tone color that drew the listener in.
9. Created a flexible range of tone colours, supple rhythmic flow, well-graded direction within the phrases, and demonstrated superior breath control.
10. Fully polished performance containing all the elements listed in points 4–9.
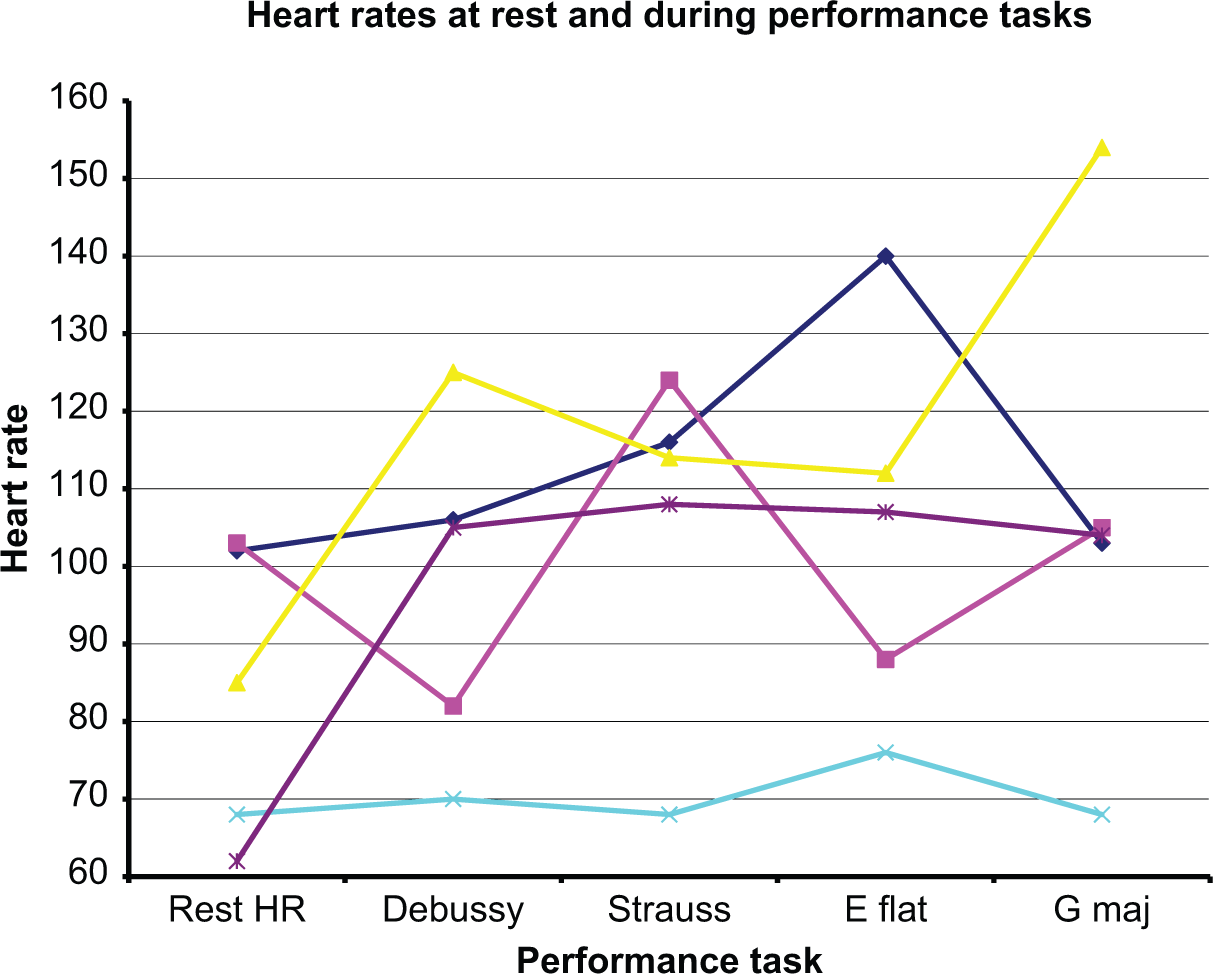
Changes in heart rate over resting heart rate for five female flute players.
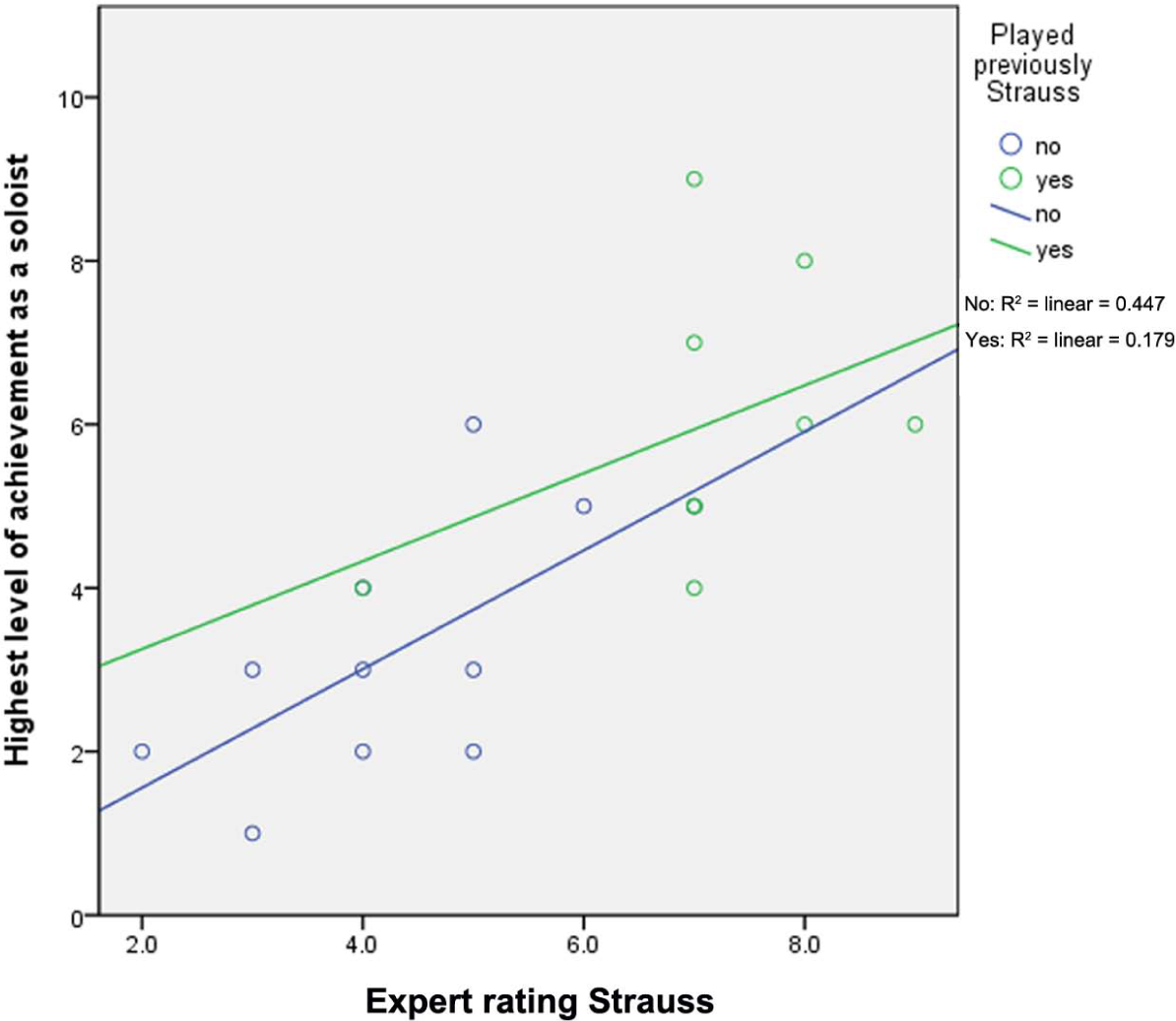
The relationship between expert rating of Strauss and highest level of achievement as a soloist for those who had played the piece previously and those who had not.
Till Eulenspiegels Lustige Streiche (R. Strauss)
The second excerpt included two passages from Richard Strauss’ Till Eulenspiegels Lustige Streiche (Op. 28) (Figure 2) which are noted for their technical difficulty. They were reproduced in enlarged format for the participants on the day of performance to avoid any changes to the performance stance or muscle tension readings as a result of craning forward to read the small font of this complex music. The excerpts require a high degree of technical accomplishment. The intervallic leaps are wide and rapidly executed. The fingering needs to be well thought through with careful planning of when to use the B flat thumb and other B flat fingerings throughout the excerpt. The scoring protocol for Strauss was as follows (note: each mark required the standard to be met for all grades below the grade given):
1–3. Unable to maintain basic shape of phrases with a clear beat. Lapses in notation, rhythm, and/or tempo.
4. Maintained the basic shape of the phrases with a clear beat (with some notation errors and other inaccuracies).
5. Played the correct notes.
6. Adhered to marked dynamics.
7. Displayed good rhythm throughout and acknowledged full length of the rests.
8. Played the excerpt at a close speed to the marked tempo (this varies throughout the excerpts and suggestions were provided in the margins of the music).
9. Correctly played the passage that changes to four time; created a vibrant tone with clear articulation.
10. Captured the elegant and giocoso nature of the work.
Participants were invited to rate their level of nervousness on a 10-point scale where 0 = “not at all nervous” and 10 = “extremely nervous” immediately prior to each performance. They also self-rated their performances on each of the musical tasks on a scale of 0–10 where 0 = worst possible performance and 10 = best possible performance.
Physiological measurement
Electromyography (EMG)
Surface electromyography (EMG) is a safe and noninvasive method for measuring the nerve activation that occurs in a muscle as a result of voluntary or reflex activation (Turker, 1993). Stress levels and occupational loads are two factors that have been reported to influence surface EMG output readings, with particularly responsive sites for these measures in the upper trapezius and frontalis muscles (Attebrandt, Mathiassen & Winkel, 1996; Westgaard, 2000). These muscles are sensitive to the presence of pain, which may affect the level of activation and subsequent EMG readings of a given muscle during musical performance (Berque & Gray, 2002). The left upper trapezius muscle was chosen for the electromyographic recordings. The midpoint between acromion and C7 spinous process was found on the upper trapezius. The skin above the muscle to be measured using EMG was lightly abraded using sandpaper, and cleansed with alcohol swabs prior to application of silver chloride electrodes. In addition the area of the skin over the C7 spinous process was treated similarly for application of the earth electrode. Meditrace electrodes were placed 2 cm apart on the left upper trapezius muscle. Electrode leads were secured to avoid any noise artefact that could interfere with measurements. Participants were then requested to play freely to establish a trace, check the levels on the recording equipment, and allow them to accustom themselves to playing whilst connected to the leads and in the deadened acoustic environment. 10-second window measurements were taken from the EMG recording of the upper left trapezius muscle. A ratio of the maximal contraction from the EMG (in Hz) to a reference voluntary contraction was recorded.
To establish each participant’s MVC in the neutral arm position participants were requested to stand tall and push their shoulders up against the resisting downward force of the researcher’s hands placed on either side of their neck. In some cases this step was repeated, either because of insufficient effort or because the scale of frequency readings on the PowerLab (PL3508/P; ADInstruments) trace had been exceeded and needed to be reduced. The flute players were then instructed to hold their instruments in the position where they were about to put their flute to their lips at two bars before an entry in the music and the process was repeated in order to establish the maximal voluntary contraction in the flute-playing position. For the data analysis process, all EMG recordings were normalized using root means square and expressed as a percentage of the neutral MVC to allow comparison of relative amounts of muscle tension used between individual performers.
Heart rate (ECG)
A silver chloride electrode was used to measure heart rate. Female participants swabbed the area directly in front of the heart’s apex and applied the required tracer. A faithful tracing was achieved through placement in these participants in the midclavicular line on the left fifth intercostal space. Maxima from the heart rate trace were averaged over blocks of time immediately before performance to achieve a resting heart rate and during performance of each of the musical and technical items.
Recording
A Brüel & Kjær (B&K) Type 4190 ½ inch free-filled microphone was used for audio recordings. This was connected to the B&K 2670 microphone preamplifier and powered by the B&K 2829 microphone power supply unit, which was connected into the Tascam DA20 digital audio tape (DAT) recorder. The sampling frequency was set at 48 Hz for calibration. The microphone was positioned 1 m from the embouchure of the flute player, directly in front of the participant. Strips of adhesive tape were marked on the floor behind which participants lined up their left foot to ensure that the 1-m distance was maintained. All performances were undertaken in the ACARMP laboratory, an acoustically treated environment that captures most reflections but is still suited to flute performance and also suitable for scientific audio capture.
Coordination of the EMG and heart rate traces to the performances
To achieve coordination on the DAT tape recording with that of the two Powerlab traces, the DAT tape was set to minutes:seconds format presentation. The researcher started the player by pressing down lightly on the left shoulder of the flute player after the count of three, which could be heard on the DAT recording. This appeared as a downward deviation in the traces of the EMG for each participant and allowed all the further traces to be located with places in the music.
Data analysis
All data were analyzed using the Statistical Package for the Social Sciences v18 (PASW software).
Results
Sample characteristics
Table 1 summarizes the player characteristics, expert and self-ratings on musical performances and the physiological measures.
One-way analysis of variance showed that participants who indicated that they wanted to become professional flute players reached a significantly higher level of both solo (F = 5.276, p = .034) and ensemble achievement (F = 7.316, p = .015) compared with those participants who did not want to become professional flute players. In addition, the expert rater awarded higher ratings to the former group on the Debussy (F = 4.793, p = .042) but not the Strauss excerpt. There were no differences between these two groups with respect to any of the anxiety measures.
Means, standard deviations, minima and maxima for player responses to anxiety measures, experience and practice, expert and self-ratings of musical performance, and physiological measures.
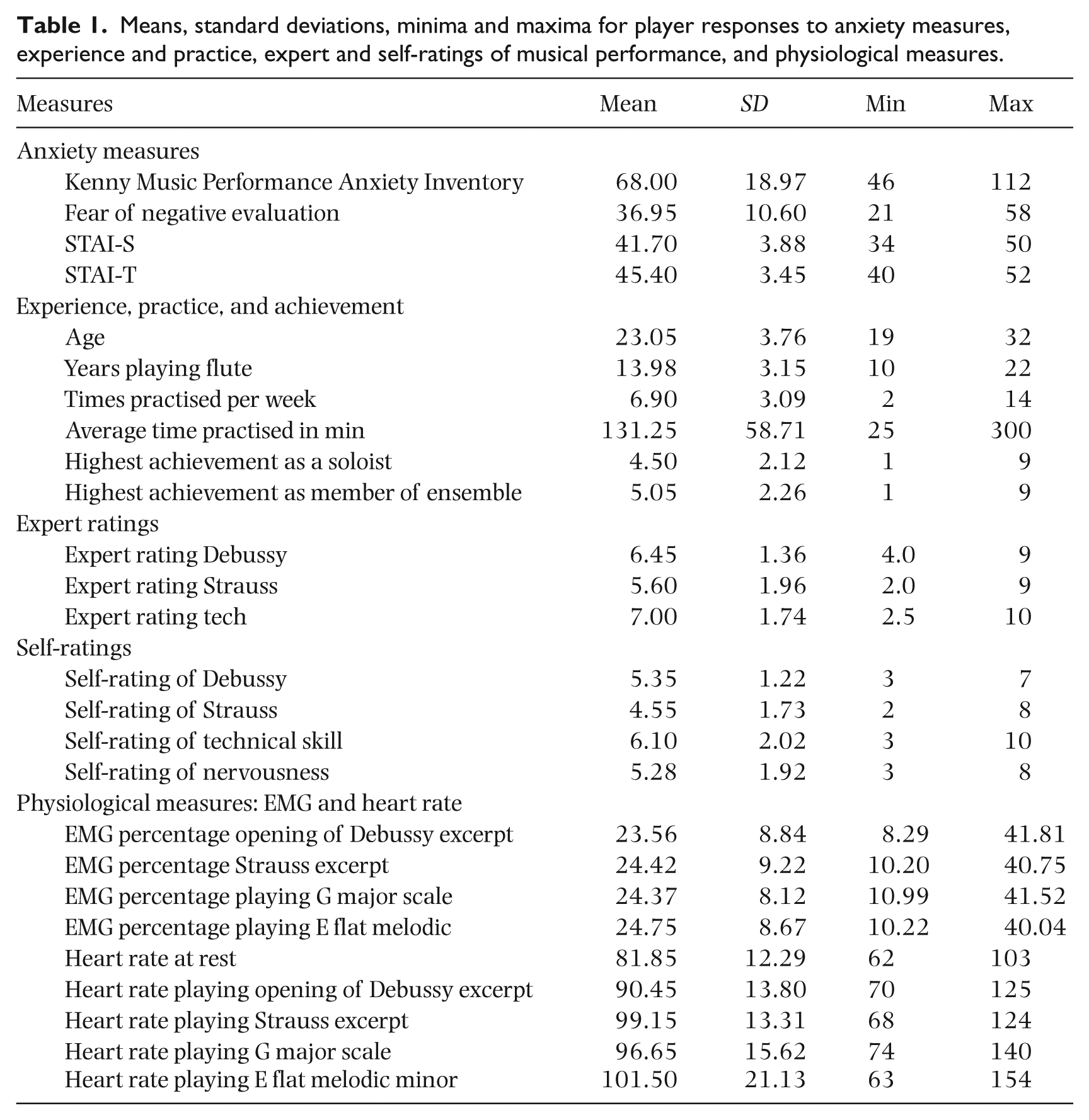
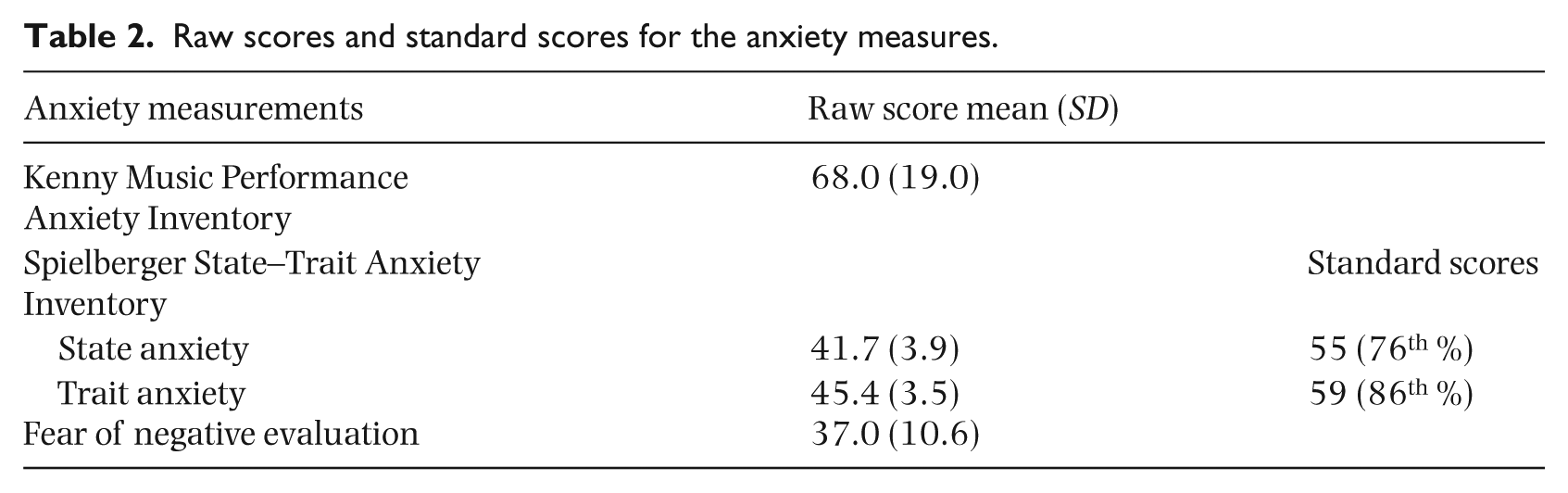
Table 2 gives the raw and standard scores for the anxiety measures. It is noteworthy that this sample of flute students’ average score fell at the 76th percentile for state anxiety (STAI-S) and at the 86th percentile for trait anxiety (STAI-T) compared with a normative population of the same age and gender.
Raw scores and standard scores for the anxiety measures.
Since no reliable normative data are available for musicians, raw scores were used for all the measures in subsequent analyses. An assessment of the distributions of scores for each of the scales was undertaken to determine their suitability for parametric statistical analysis. All measures were normally distributed with Kolmogorov-Smirnov P-values greater than 0.2, skewness and kurtosis values between −1 and 1 and there were no extreme values.
Correlation analyses
Pearson correlation coefficients between student’s self-ratings and expert ratings of the Debussy and Strauss excerpts and technical mastery were undertaken. There were significant correlations between expert and student ratings for the Strauss excerpt (r = 0.519; p = .02) and for the technical work (0.613; p = .004), but not for the Debussy excerpt (r = 0.139; p = .56).
Correlation analyses between the anxiety measures showed that the only significant relationships were between K-MPAI and FNE in the expected direction (r = 0.56, p < .05) and STAI-S and FNE in the opposite to expected direction (r = −0.44, p < .05). However, regression of these two variables showed that the relationship was variable and weak (R sq linear = 0.19). With respect to correlations between all the other factors and K-MPAI, only the relationship between the number of times students reported practising each week and K-MPAI was significant, but the correlation was negative; those who practiced least reported the highest MPA (r = −0.46; p = 0.04).
There were also significant correlations between expert ratings of the Strauss and Debussy excerpts, technical mastery, and rankings of achievement as a soloist and as an ensemble player, with the strongest correlations occurring between expert ratings and ratings for highest achievement as a soloist, Debussy: p = 0.71; p = .001; Strauss: r = .76; p = .001; technical mastery: r = 0.57; p = .008). The only nonsignificant association occurred between highest rating of achievement as an ensemble player and expert rating of technical ability.
There were no relationships between resting HR and STAI-S, FNE, or K-MPAI; and no relationships between HR during Strauss and STAI-S, FNE, or K-MPAI. Heart rate change patterns over the five measurements (resting, Debussy, Strauss, and E flat melodic minor and G major scales) were highly variable. Figure 1 shows some of the indicative patterns; for example, resting HR low and stays low across all performances; resting HR low then elevates to a similar level across all performances; resting heart rate high and remains high; heart rates rise and fall above and below resting HR; resting HR high then elevates over this baseline at variable rates across the four performances.
Unlike heart rate, there were highly significant intercorrelations between all of the EMG measurements, indicating consistency in muscle tension across performance tasks. All correlations exceeded r = 0.72; p = .001, with the highest correlation between EMG Strauss and EMG E flat melodic minor scale (r = .95; p = .001).
Pearson’s correlation coefficients were also used to explore relationships between playing history, practice, induced anxiety (advised that performance would be evaluated by an expert panel) and anxiety scores. The degree of music performance anxiety (as assessed by the K-MPAI) was significantly negatively correlated with highest achievement as an ensemble player (r = −0.68, p < .001). A similar trend was found for highest achievement as a soloist but this relationship did not reach statistical significance (p = 0.07). Highest achievement in ensemble was also significantly negatively correlated with fear of negative evaluation (r = −0.53, p < .05). Years of playing the flute, number of practice sessions per week and amount of weekly practice were not significantly associated with any of the anxiety measures. Self-ratings of nervousness (assessed on one question: “please rate how nervous you feel right now on a scale of 0–10, where 0 = not at all nervous and 10 = as nervous as I could possibly be”) just prior to their performances were significantly associated with scores on trait anxiety (r = 0.45, p < .05).
Comparison of high and low music performance anxiety groups
Participants were divided into two groups based on their score on the K-MPAI. Those scoring below the mean (68) for the group were classified as low MPA; those scoring above the mean for the group were classified as high MPA. Independent t tests were conducted to assess the relationships between high and low MPA on heart rate and EMG. There were no significant differences in heart rate between high and low MPA groups for any of the musical tasks. However, there were significant differences between the MPA groups on EMG for all of the musical tasks, but in the opposite of predicted direction. Those with high MPA had lower EMG readings (Table 3).
Means, standard deviations and t tests for EMG percentage by low (n = 11) and high (n = 9) MPA group membership for each musical task.
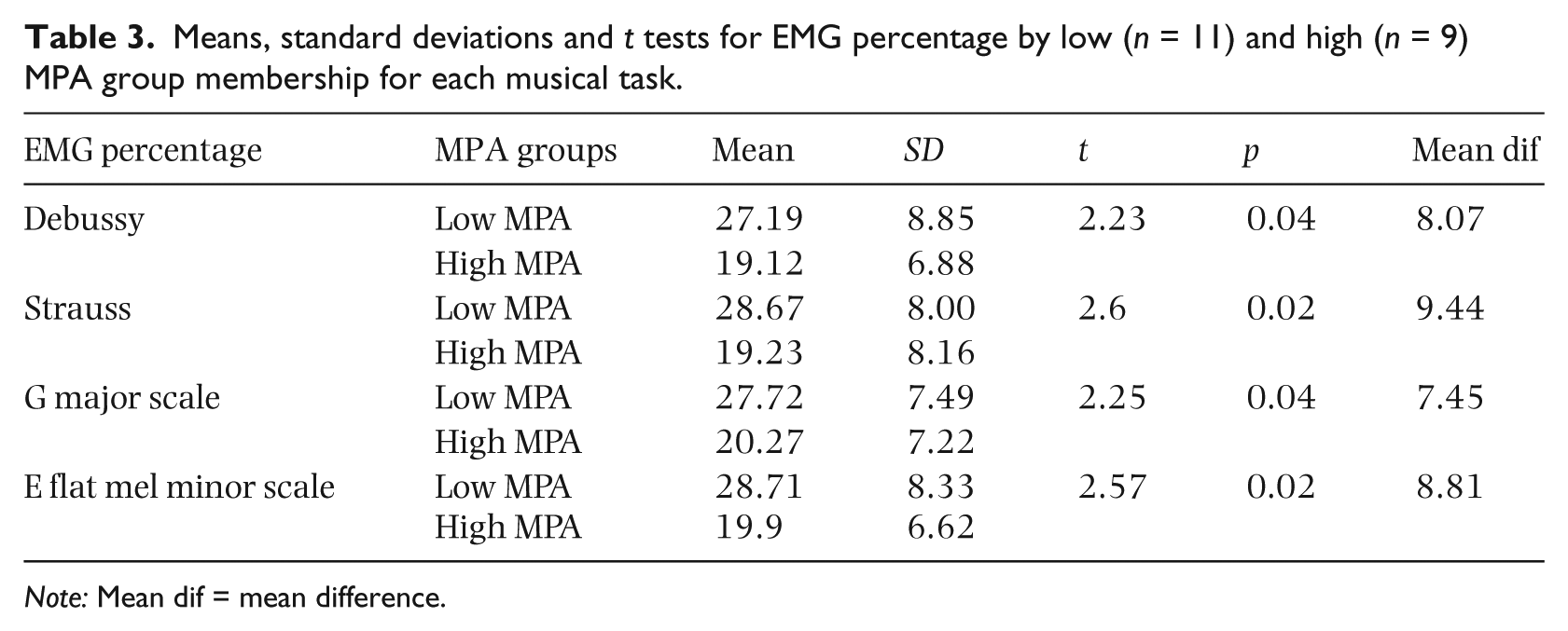
Note: Mean dif = mean difference.
High and low MPA groups were assessed for differences on the other anxiety measures and the expert and self-ratings. FNE was significantly higher for the high MPA group compared to those in the low MPA group (43 [10.9] vs. 32 [7.5]; F 1,18 = 7.02, p = 0.02). There were no differences between high and low MPA groups on number of years playing the flute or the amount of practice undertaken for the test pieces.
Effect of previous experience with test pieces
Previous experience of playing the test pieces had a significant effect on all but one (HR for Strauss) of the measures indicated in Table 4.
Means, SD and t tests showing effect of previous experience playing Debussy and Strauss on expert rating, EMG and HR.
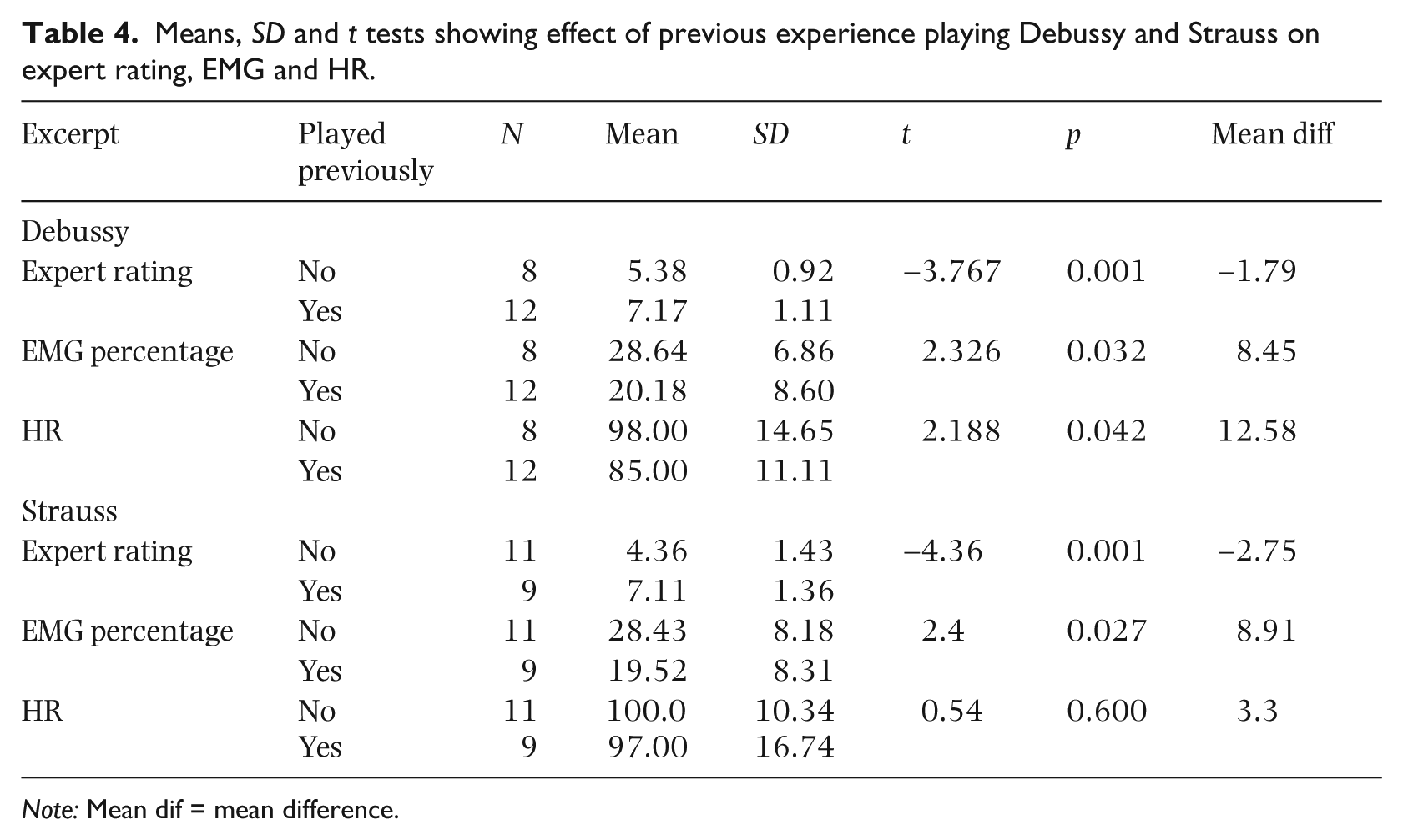
Note: Mean dif = mean difference.
Expert ratings were significantly higher and EMG significantly lower for both the Debussy and Strauss excerpts for those who had played the pieces previously. Those who had not played the Strauss previously had almost 50% more muscle tension (EMG readings of 28.43 compared with 19.52) than those who were previously familiar with the work. HR was significantly lower in those who had played the Debussy previously but there was no significant difference in HR for those who had played the Strauss excerpt previously.
Instruction about expert ratings
Just prior to performance, each participant was told that his/her performance of their second piece (either Debussy or Strauss) would be “evaluated by a panel of expert judges.” However, this experimental manipulation did not produce any significant differences in expert ratings, EMG, or heart rate for participants who were told that their performance would be evaluated by a panel of experts compared to those who were not told about the evaluation.
Regression analyses
Hierarchical regression analyses were used to test the hypothesis that the specified variables would account for variation in music performance anxiety assessed by the K-MPAI. Prior to developing the model, and in view of the high intercorrelations between some of the measures, multicollinearity of the variables was assessed using the collinearity statistics, tolerance and variance inflation factor. The tolerance is the percentage of the variance in a given predictor that cannot be explained by the other predictors. When the tolerances are close to zero, there is high multicollinearity and the standard error of the regression coefficients will be inflated. A variance inflation factor (VIF) greater than two is usually considered problematic. Variables with low tolerance and VIF > 2 were sequentially removed from the model until all VIF were < 2.0. For example, the two variables, “highest achievement as a soloist” and “highest achievement in ensemble playing” were identified as problematic because they were significantly correlated (r2 = .62). Tolerance values showed that 40–80% of the variance in one predictor could be explained by the other predictor. Hence “highest achievement as an ensemble player” was removed from the predictor set and the analysis was rerun. Other pairs of variables with high VIFs included expert rating of Strauss and highest achievement as a soloist; expert rating of Strauss and years playing the flute; heart rate and EMG. In each case, the variables with highest standard deviations were included in the model.
Other confounding factors in the set of variables were also identified before finalizing the model. Those who had played the Strauss excerpt previously scored higher expert ratings. To assess the effect of previous experience on expert rating, further analysis was undertaken. Those who received higher expert ratings also had achieved higher ratings for achievement as a soloist and had previously played the Strauss excerpt. The plot of residuals by the predicted values showed that the variance of the error was a little greater for those who had previous knowledge of the set work. There was, otherwise, good scatter. To check for influential points, the centred leveraged value was plotted against Cook’s distance. The resulting scatterplot showed that those who had played the Strauss excerpt previously had a higher leverage and thus higher influence. Their higher leverage gave them extra weight in the computation of the regression line, and the high influence indicates that it may have affected the slope of the regression line. Figure 2 shows that the relationship between expert ratings on the Strauss excerpt and the highest level of achievement was significant only for those who had not previously played the Strauss excerpt. For those who had, scores clustered around the higher end of the expert rating scale but occurred across a wide range of ratings on previous achievement as a soloist. For this reason, (and also because of its mulitcollinearity with highest achievement as a soloist) the expert rating of Strauss was not included in the final regression model.
Because the variables in the predictive model were on different scales, they were converted to z-scores with a mean of 0 and a standard deviation of 1 before being entered into the regression analysis. In the first model, the anxiety measures (STAI-T, STAI-S, and FNE) were added. In the second, the anxiety measures and highest achievement as a soloist; in the third, anxiety measures, highest achievement, and practice; and in the fourth and final model, the anxiety measures, highest achievement, practice, and EMG and HR representing the physiological measures were added. Table 5 summarizes the results.
Hierarchical regression models predicting music performance anxiety (K-MPAI).
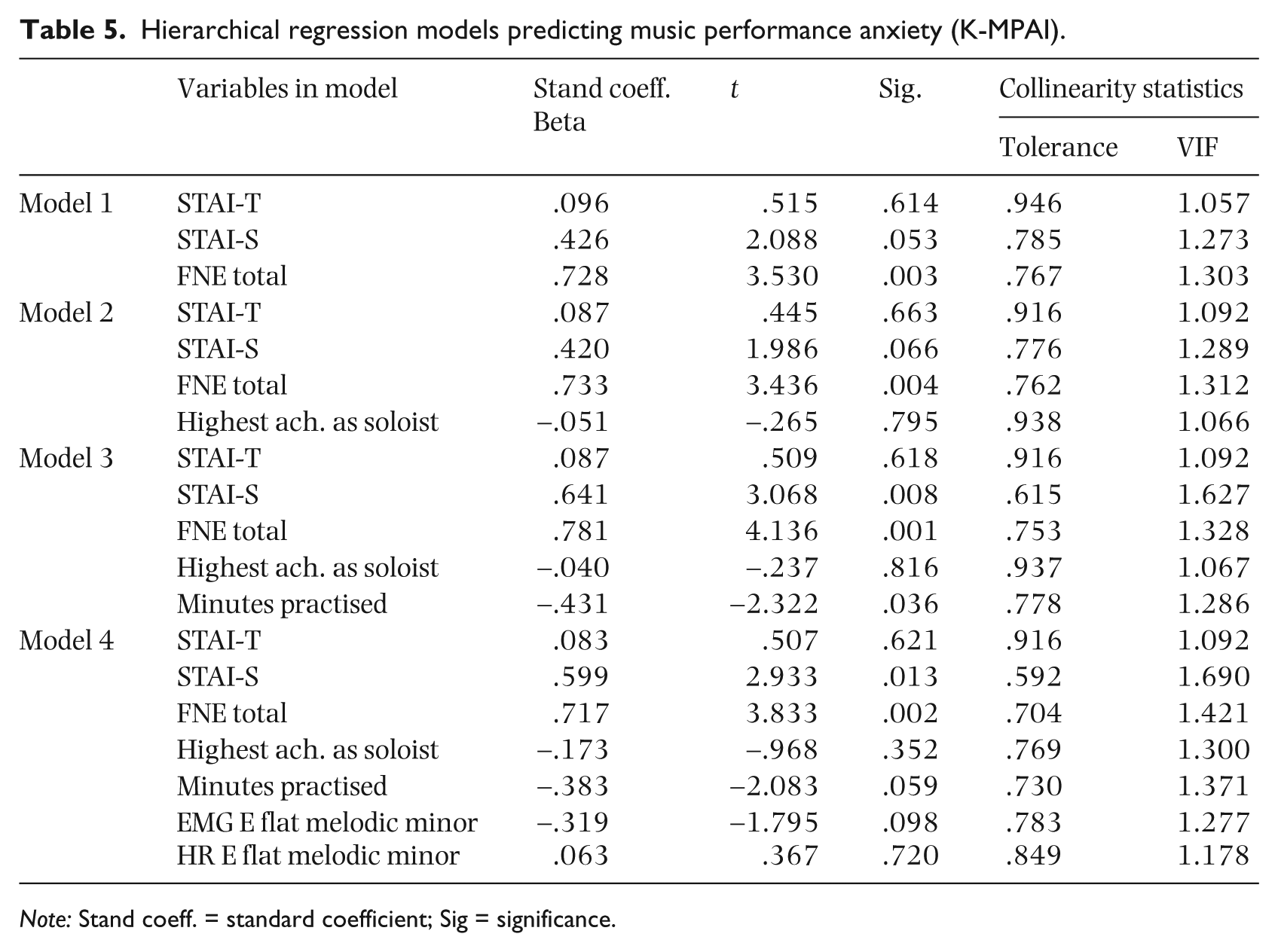
Note: Stand coeff. = standard coefficient; Sig = significance.
Table 8 shows that the final model accounted for 70.4% of the variance in music performance anxiety. The other anxiety measures accounted for 48% total variance in the MPA scores, with the other variables collectively adding a further 23% to the model.
F statistics, significance and R square for the four models of music performance anxiety.
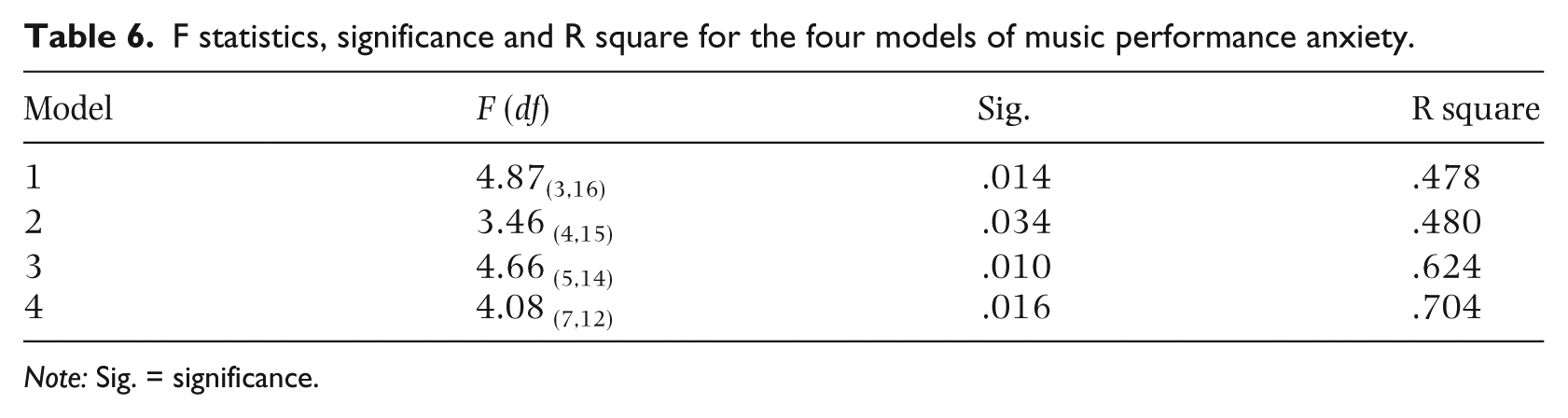
Note: Sig. = significance.
Discussion
A robust predictive model of music performance anxiety was identified in this study of tertiary-level flute players, providing support for previous theories that have identified the contribution of multiple, yet partially independent factors in the experience of music performance anxiety during skilled musical performance. These included measures of trait anxiety, situational anxiety and fear of negative evaluation; the level of accomplishment that one has achieved on one’s instrument; the amount of practice undertaken for the performance; and physiological factors such as EMG and heart rate.
Anxiety and other psychological and physiological measures
In the univariate tests, those who reported most anxiety during their performance also reported the highest levels of trait anxiety. The association between high levels of trait and state anxiety has been observed in many other studies (Hardy & Parfitt, 1991; Huston, 2001; Kenny, Davis & Oates 2004; Noteboom, 2000). Also consistent with other studies that show at least a partial independence between the different measures of anxiety (e.g. physiological and psychological measures [Wilson, 2002]), there was no concordance between self-reported anxiety on the STAI or the K-MPAI and the HR and EMG measures. This group of flute players had mean trait anxiety values that placed them at the 86th percentile of age- and gender-matched community samples, indicating that ceiling effects or restriction of range effects may have been operating for this variable. Although there was no effect of the experimental manipulation to increase anxiety and arousal by telling some students that their performance was going to be evaluated by an expert panel of judges, the study situation itself resulted in significantly elevated heart rates over baseline resting levels for many, but not all participants, by as much as 20 beats per min when compared with the HR during performance of the E flat melodic minor scale, which produced the highest mean heart rate. The recorded resting heart rate for 10 of the 17 women and one of the three men fell into the poor cardiovascular fitness category (> 83). Given that this sample was young and healthy and 19 of the 20 reported exercising regularly (at least weekly), we assume that these readings may have been too proximal to the performance and therefore may have been contaminated by anticipatory anxiety. Some degree of physiological arousal is necessary for a good performance and will only impair performance if it is appraised negatively (Kenny, 2009; Steptoe, 2001), or exceeds an optimal level such that it interferes with the quality of the performance (Kokotsaki & Davidson, 2003). Many of the students experienced a performance breakdown while attempting to play E flat melodic minor scale. This is one of the most difficult scales for the flute; the students had not been advised to practice it and, as indicated by their heart rates, had a significant increase in physiological arousal, which may have contributed to performance impairment on this task.
A somewhat unexpected finding was that there was an inverse relationship between self-report of music performance anxiety on the K-MPAI and the number of practice sessions per week. Those practicing least reported the highest levels of MPA. There are no previous reports of such a finding in the literature, so this result warrants further exploration. It is possible that practising triggers feelings of MPA and is therefore experienced as aversive and thus avoided. An alternative explanation is that those high in MPA may have poor strategic skills in musical preparation and are more likely to be unprepared for performances by virtue of inadequate practice and its consequences such as failure of technical mastery and exacerbation of MPA.
Prior musical experience and music performance anxiety
Participants had played the flute between 11 and 22 years but the amount of time they had been playing their instrument was not associated with how much music performance anxiety, fear of negative evaluation, or state or trait anxiety they experienced. Length of time one has been playing one’s instrument may be a poor proxy for the quality of practice that the performer undertakes, the amount of musical ability the performer has, and the level of musical achievement that is reached during that time. In this study, a more sensitive measure was the highest level of achievement attained in solo and/or ensemble performance. Experience performing in ensembles, such as playing in a weekly youth orchestra or undertaking casual work in a professional orchestra was associated with significantly lower music performance anxiety compared to those who had not had similar ensemble experience. Frequent exposure to ensembles was associated with reduced performance anxiety in this study. While this association is correlational, it is likely that increased ensemble experience leads to better understanding of and comfort with the ensemble music literature; and frequent playing in front of peers and conductors (provided that the atmosphere in which these performances occur is supportive) acculturates young musicians to performance situations. Hence they become more able to cope with performance assessment. This finding has implications for the way in which music tuition is delivered in Australia. Unlike in conservatoria in Europe, instrumental teaching in Australia is predominantly conducted via one-on-one teaching in a studio. Most young instrumentalists play predominantly only for their teachers in weekly lessons and at the occasional informal soirée for family and friends or Australian Music Examination Board (AMEB) music exam. This contrasts with students in France and Germany who play in front of a full class including their professor twice weekly and are encouraged to receive criticisms from fellow students on a regular basis. It is not surprising that students who have had exposure to their peers in an ensemble setting feel less anxious when presented with the high-pressure situation of a mock audition. Those students in our study with the most ensemble experience and achievement also had significantly less fear of negative evaluation.
Physiological measures (HR and EMG) and music performance anxiety
Several studies of music performance anxiety have used heart rate as a dependent measure (Brotons, 1994; LeBlanc et al., 1997; Ryan, 1998, 2004) with varying results. Heart rate can be affected by many factors and may be difficult to interpret in experimental studies. In the univariate tests in this study, HR was not significantly different for groups reporting high or low music performance anxiety. This disjunction between the various indicators of music performance anxiety has been observed by other researchers (Craske & Craig, 1984; Studer, Danuser, Hildebrandt, Arial, & Gomez, 2011; Weinberger, Schwartz, & Davidson, 1979). Within-subject heart rate showed variability across the test protocol with several patterns of HR change being observed (see Figure 1). It was of interest to note that the Debussy excerpt, L’après midi d’un Faun, produced the lowest mean heart rate among all the musical tasks in the protocol (90 bpm compared with the Strauss excerpt 99 bpm and E flat melodic minor 102 bpm). There are a number of possible explanations for this finding. Since the order in which the pieces were performed was randomized, the higher HR during Strauss excerpt was not attributable to order effects. This result may be interpreted as heightened sympathetic arousal or increased music performance anxiety in response to the more technically demanding Strauss excerpt. An alternative, but less plausible explanation is that the Debussy excerpt was more musically restful in mood, and that this produced a lower heart rate in performers. A more likely explanation is that the Debussy excerpt required advanced breath control to be satisfactorily rendered. Several participants prepared for their performance of the opening line of Debussy by engaging in deep breathing exercises. The use of a Valsalva maneuver (i.e., in which a person tries to exhale forcibly with a closed glottis [windpipe] so that no air exits through the mouth or nose) amongst this group of players may have accounted for the lowering of Debussy heart rates over heart rates for all other musical tasks in this study. The highest mean heart rate for the E flat melodic minor scale could perhaps be explained by the fact that this requirement came as a surprise to the participants (who had been sent the music for the Debussy and Strauss excerpts prior to the testing day, so they were aware of this component of the protocol). Further, it is a very difficult scale for the flute (most students had some form of performance breakdown while trying to render this scale).
Heart rates of those playing the Strauss excerpt for the first time were not significantly higher than those already acquainted with the excerpt, reflecting the fact that this excerpt induces a stress response in even the most experienced orchestral flute players. However, the heart rate for those with prior familiarity with the Strauss excerpt was more variable. Observation of performances indicated that this group attempted to play the piece as closely as possible to the very fast tempi required, which may have induced more anxiety than in those who were not familiar with the tempi expectations and/or disregarded the instructions regarding tempo provided in the music. If heart rate continues to be used in studies of music performance, all of the possible influences on HR differences need to be carefully considered. Recent research in emotional regulation has explored the use of heart rate variability (HRV) as an alternative measure (Thurber, 2007). HRV is caused by the interaction of the excitatory influence of the sympathetic nervous system and the inhibitory influence of the parasympathetic nervous system on the heart. HRV could be caused by either increased sympathetic activity or decreased parasympathetic inhibition, which has been associated with anxiety (Holden & Barlow, 1986; Shinba et al., 2008) and increased emotional arousal in stressful situations (Murray & Raedeke, 2008). The use of HRV rather than HR may be a more sensitive measure (Valentine, Fitzgerald, Gorton, Hudson, & Symonds, 1995) in studies of music performance anxiety.
Counterintuitively, flute players with higher levels of MPA showed a significant decrease in levels of upper trapezius activity. The high-MPA group (i.e., the more anxious participants) actually had lower EMG measurements than those who reported feeling less anxious. Further exploration of this finding may require consideration of the anatomy of this region. Flute playing involves fine manipulation and agility of the fingers. Kinetic chain theory suggests that these fine tasks need good proximal support; indeed, the “high demands on force and precision of the repetitive work performed by the fingers and wrists is known to increase the static load on these proximal muscles” (Milerad & Ericson, 1994, p. 81). The upper trapezius is part of a complex arrangement of individual muscles in the shoulder region that includes the deltoids, supraclavicular and infraclavicular, as well as rotator cuff group muscles. Due to the muscular multiplicity of the region, a certain work task may be accomplished through a number of different combinations of individual muscle actions. Mathiassen, Winkel, and Hagg (1996) demonstrated that EMG amplitude increases in a linear or exponential pattern during continuous isometric shoulder exertion at constant force in healthy subjects as well as in subjects with musculoskeletal disorders. Milerad and Ericson (1994) stated that “tasks demanding manual precision may imply an increase in EMG amplitude….however, upper trapezius responded only slightly to precision demands, although some individuals were exceptionally sensitive” (1994, p. 81). In this study, there was a significantly lower than expected set of EMG readings for the most anxious participants in this proximal musculature, that is, in the left upper trapezius muscle. This drop in the activation of the left upper trapezius muscle in the most anxious players suggests some redistribution of muscle activity amongst the flute players. Wessa and Flor (2002) have noted hyperreactivity of certain muscle groups to stress whilst others seemed unimpaired. In flute players, in which a dual role of support and manipulation of the key work is required simultaneously, it is not unreasonable to postulate that perhaps the tension (as measured by EMG) may be redistributed distally to these muscle groups in preference to the more proximal shoulder musculature. Given the findings regarding anxiety by van Galen, Müller, Meulenbroek, and Gemmert (2002), it is possible, that in flute players, it is normal to use the left upper trapezius to support the flute, and perhaps the presence of MPA leads to a reduction in normal motor processes.
Alternatively, it is possible that muscle tension travels even more proximally to involve the lips and cheeks of wind players affected by MPA. Research by Dana (1998) suggests some involvement of the embouchure musculature which may compensate for inadequacies or weaknesses in other parts of the system causing strain and diminished endurance. Both patterns of “transference of tension” are in keeping with anecdotal and pedagogical reports from flute players performing under stressful conditions. It is possible that there is a redistribution of forces to other less ideal areas such as the fingers or the face muscles. There are many cases in the flute pedagogical literature of these being responsive to stress in terms of becoming excessively rigid. It is possible that MPA leads to overthinking about fingers and embouchure (Dana, 1998), which in turn may lead to reduced activation of normal supporting musculature as this effort becomes transferred distally (or to what the high MPA performers may perceive as critically relevant areas for their flute performance). In a study of people with general anxiety disorder, changes in EMG were observed between peripheral and proximal musculature, thought to reflect a redistribution induced by the stressful input. There was an increase in tension-related muscle activity in the gastrocnemius muscle most likely due to sympathetic nervous system (SNS) arousal (Hoehn-Saric, Hazlett, Pourmotabbed, & McLeod, 1997). It is possible that the flute players in this study with higher MPA showed a similar SNS effect of decreased central muscle activity as increased activity focused on peripheral muscle groups. It is also possible that MPA may exert a distraction effect on surface EMG readings, in this case from the forearm that may result in a redistribution of muscle activity—possibly to further distally in the left arm and/or the embouchure muscles. In a study by van Galen et al. (2002), six of the eight measures of low-anxious participants reached a higher EMG activation than for those of the high anxious participants. These researchers speculated that there could be differential effects of anxiety on phasic and tonic musculature. Alternatively, they proposed an interpretation of a differential response to task stressors by proximal and distal musculatures. Interestingly, the study also explored the potential confounding/interacting effects of pain on EMG and anxiety. We did not take EMG measures of the fingers or the embouchure in this study and future research could usefully investigate these areas.
Limitations
In this study, we used only one expert rater. Replication studies will need to use additional raters to establish interrater reliability of the rating scales that we developed for the study. For the highest level of achievement in solo and ensemble performance scales, we obtained unanimous rankings from expert pedagogues, but the scales constructed to assess quality of performance in the excerpts will require further assessment with respect to their test-retest and interrater reliability. We believe that the development of very precise rating criteria for each of the musical excerpts and the use of a very experienced flute player and adjudicator as the rater of performance quality enhanced the reliability of these ratings in this study.
It is difficult to find works for these types of studies with which none of the participating musicians has had previous experience. It might be necessary to eliminate the confounding element of previous knowledge of musical excerpts by having pieces specially composed for use in such studies if local composers are available and willing to assist.
Finally, the sample size was small and confined to one instrument, the flute. We need further studies with larger numbers and varied instruments to fully understand the multiple factors that contribute to the experience of music performance anxiety in skilled musical performance.
Conclusion
This study has developed a comprehensive model to test a number of possible predictors of self-reported music performance anxiety in skilled tertiary-level flute players. These included self-report measures of trait and state anxiety, fear of negative evaluation, physiological measures (EMG and ECG), performance experience, and technical and task mastery. The main hypothesis, that each of these components would contribute additional unique variance to scores in music performance anxiety was not confirmed. Like other musician groups that have been assessed for trait anxiety, this young group of tertiary-level flute players had very elevated mean trait anxiety scores compared with a comparable population sample. Probably because of the restriction of range of scores at the higher end of the scale, trait anxiety did not contribute to the prediction of MPA, as hypothesized. State anxiety and fear of negative evaluation were the only independent significant predictors in the final model. Contrary to expectation, highest level of achievement, either as a soloist or ensemble player did not contribute uniquely to the prediction of MPA when all of the other factors were added. Amount of practice was independently significant in Model 3 but not in Model 4 where technical competence factors were added and the unique variance was distributed between technical competence and amount of practice undertaken. Each of these factors approached significance and need to be evaluated in larger samples to further assess their contribution to prediction of MPA. This model shows the multifactorial nature of the factors contributing to MPA. Future studies will need to consider all of these factors in a single model in order to maximize prediction. The other surprising and unexpected finding concerned the direction of effect in the relationship between MPA and EMG. Higher anxiety resulted in lower tension in the EMG traces. We are not aware of this effect having been reported previously in musicians; this phenomenon is deserving of further attention, particularly given the high prevalence of musculoskeletal and repetitive strain-related pain in musicians. These aspects of the study can usefully be explored further in flute players and other instrumentalists, expanding on the variables included and using larger samples.