
Abstract
This study investigates the interplay between temporal and emotional dynamics during the first wave of the COVID-19 pandemic at a public hospital in the Grand Est region of France, and their influence on strategic crisis management. We use the concept of concert time to analyze how temporal structures and temporal work were reconfigured under conditions of extreme urgency and uncertainty. Our qualitative case study is based on interviews with twelve hospital decision-makers and a range of internal and external documents. The findings reveal that in the absence of established routines, emotionally charged real-time coordination became central to collective action. Concert time encouraged a sense of alignment, cohesion, and togetherness among staff, enabling more effective decision-making. In contrast to dominant narratives that frame crisis emotions primarily in terms of fear or anxiety, our study highlights the mobilizing role of shared positive emotions—such as pride, moral purpose, and collective enthusiasm. These emotions served not only to support resilience but also acted as a mechanism for temporal coordination. However, the findings also point to the fragility of emotional alignments, which often dissolve when emotional labor is left unrecognized after the crisis. By examining how time is experienced as a lived phenomenon and how emotions function as organizational forces, this study contributes to emerging literature that foregrounds the constitutive role of emotions in decision making and coordination during crises.
Introduction
The COVID-19 pandemic completely changed the way time as a lived phenomenon was experienced by the decision-makers in hospitals. Researchers have highlighted how crises lead to temporal disruptions, which unsettle the pace, phase and/or sequencing of organizational work (Pérez-Nordtvedt and Harrison, 2025). These disruptions often result in dismantling and rearranging of temporal structures through which the humans interact with the world (Venkatesan and Joshi, 2022). Because crises bring about profound temporal disruptions, they also represent opportunities for reconfiguring time prompting new processes of temporal structuring and restructuring. Although these dynamics have been recognized (Pérez-Nordtvedt and Harrison, 2025; Venkatesan and Joshi, 2022), management research has yet to explore in detail how temporal structuring and restructuring unfold during crises. This gap is particularly evident in the study of emotions in crisis; while existing literature has increasingly acknowledged the role of emotions in organizational decision-making amid crises, it primarily focuses on negative emotional states, such as fear or anxiety, while neglecting the mobilizing potential of shared positive emotions (Kayes, 2004; Turner, 2007). Furthermore, studies tend to treat time as a structural constraint—compressed or accelerated—rather than exploring how emotional intensity may itself serve as a temporal coordination mechanism in the absence of routines.
Our empirical setting is a public hospital located in Nancy, in the Grand Est region of France. By employing the case study method, we aimed to gain an in-depth understanding of how this particular organization navigated the challenges posed by the COVID-19 crisis. To achieve this, we conducted interviews with 12 members from the hospital’s Decision-Making Unit (DMUs), all of whom played direct roles in managing the pandemic response. In addition, we collected internal, such as communication and meetings’ minutes) and external documents, including regional and national directives. More concretely, our study examined how hospital decision-makers experienced time as a lived phenomenon during the crisis. In addition, given that crises often disrupt established temporal patterns, we explored the impact of emotions on decision-making during these turbulent periods. This article is organized as follows. We begin by presenting a review of the literature on time as a lived phenomenon, along with an examination of how crises act as temporal disruptions. Next, we discuss existing research on temporal reconfigurations during crisis situations, emphasizing how these processes influence emotions and consequently affect decision making. The methodology section follows, where we outline our research questions, describe and justify the use of the case study approach, provide details about the case context, and explain our data collection and analysis procedures. We then present the results of our study. At the end, we present the discussion and summary of our key findings.
The contributions of this study to general management are multifaceted. First, it advances our understanding of how time is perceived and managed during crises, particularly by hospital decision-makers under the pressure of the COVID-19 pandemic. By focusing on the lived experience of time and the emotional aspects of temporal disruptions, the study reveals that crises require organizations to rapidly dismantle and reconstruct temporal structures. This creates a pressing need for new temporal norms—norms that may or may not rely on temporal regularities and routines, depending on the immediacy of decisions required.
In addition, we believe we extend our understanding of the role of emotions in decision-making under pressure. By shifting attention away from threat-based emotions, such as fear and anxiety, we emphasize the importance of understanding the collective emotional dynamics in crisis situations (Fredrickson et al., 2003) and the role of positive shared emotions in facilitating group coordination and effective decision-making under pressure. Our findings also contribute to theories of emotional sensemaking (Maitlis and Sonenshein, 2010) by illustrating the temporal fragility of collective emotions and their potential long-term consequences on organizational cohesion.
Finally, the concept of “concert time” introduced in the study provides managers with a practical tool for enhancing coordination and communication. By promoting shared attention and intensive interaction among team members, managers can create stronger alignment and more effective collaboration, especially when routines are disrupted or time is compressed. Overall, these insights offer valuable guidance for general managers seeking to lead organizations through periods of uncertainty and rapid change.
Literature review
Time as a lived phenomenon
Time as a lived phenomenon is central to our analysis of crisis-time decision-making. Drawing on Henri Bergson’s (1907) distinction between clock time and lived time (la durée), we see that while clock time offers an objective, measurable framework, lived time is shaped by subjective perception and unfolds as a continuous, qualitative flow. This distinction between objective and subjective time is particularly significant in organizational contexts, where disruptions such as the COVID-19 crisis challenge established temporal frameworks and call for a deeper understanding of how individuals and groups experience time.
In organization studies, time has been defined as “a non-spatial continuum in which events occur in apparently irreversible succession from the past through the present to the future” (Ancona et al., 2001: 513). Most of the researchers agree that time can be objective or independent of human action, and subjective meaning socially constructed by human action through interactions and social processes (Orlikowski and Yates, 2002: 689). This means that the experience of time varies across conditions and actors; it relates directly to the perception of the passage of time (Ancona et al., 2001). Following the same line of thought, Reinecke and Ansari (2015) talk about clock time, which is the absolute, unitary and linear time, and process time, which is subjective, relative, and organic. The perception of time is defined as “the understanding and knowledge of time acquired through the senses” (Ancona et al., 2001: 518). In this sense, Mattley (2002) describes inner time as the physical sensation of time passing – a subjective experience unique to each individual – which connects human experiences and forms a continuous flow.
Although time perception is generally regarded as an individual-level factor in psychology, it can also be extended to groups, organizations, and societies (Ancona et al., 2001). Sharron (1981, 1982) introduced the concept of concert time as “the concerted and agreed-upon time perception of interacting individuals” (Sharron, 1982: 72). This phenomenon happens when an individual’s inner time aligns with that of others, thereby fostering social unity and enabling shared understanding (Mattley, 2002; Sharron, 1982).
Sharron (1982: 72) points out that while each person moves in “a unique and unshared space,” temporal togetherness is created by the focused attention of group members on the same object with the same intensity. Hence, concert time is a social creation and continues as long as group members interact (Mattley, 2002). However, the idea of aligning inner times does not mean that all activities must be synchronized. In situations of prolonged crises, maintaining a shared focus does not require that all routines be carried out at the same time. The “togetherness” of the group is maintained even when specific routines are temporarily desynchronized or decoupled. For instance, a group may respond to a crisis immediately, disregarding slower funding considerations, and later adjust their actions by retrospectively modifying timelines or establishing buffers to safeguard upcoming activities (Geiger and Harborth (2025). This demonstrates that concert time is socially constructed, and that achieving unity can involve managing experiences that are not always simultaneous.
Plesner (2025) provides a practical mechanism for this shared alignment through the “accordion effect,” a metaphor describing how groups maintain cohesion by treating time as elastic. This implies that for concert time to persist during a prolonged crisis, the group must collectively allow their shared time to “stretch” when the complexity of the task requires it, while “compressing” elsewhere to maintain stability and operability. This time elasticity ensures that group unity is preserved not through identical pacing, but through a shared, flexible commitment to expansion and/or contraction of the collective efforts.
Emotions are experienced within inner times, and when people’s moods align, their inner experiences of time also become synchronized. Joint actions often facilitate the merging of moods and the formation of concert times. Leaders, such as team leaders, play a key role in harmonizing these internal timeframes and maintaining the resulting stability within the group (Sharron, 1982). It is important to highlight that this stability must be supported by planners and staff, who actively step in to adjust rhythms and tasks. By reorganizing schedules and willingly helping each other navigate delays, these team members perform the crucial work that keeps the group moving smoothly from the bottom up (Plesner, 2025).
Crises as temporal disruptions
Crises are associated with temporal disruption defined as “exogenous shocks that upset the temporal demands—in objective (clock) time—of an individual (e.g., alterations to the pace, phase, or sequencing of their temporal (sub)structures)” (Pérez-Nordtvedt and Harrison, 2025: 25). Such temporal disturbances interfere with the way organizational actors carry out their tasks affecting the speed at which activities are performed (pace), imposing new demands to perform activities at different times than previously (phase), or altering the order in which demands are executed (sequencing). Temporal disruptions can impact one of these factors, two or all three of them at the same time (Pérez-Nordtvedt and Harrison, 2025). Although these events disrupt actors’ objective or clock-based time, they also exert a clear effect on how time is subjectively experienced. In essence, “while the disruption is exogenous, the impact is endogenous” (Pérez-Nordtvedt and Harrison, 2025: 25).
This dual impact is particularly evident during the pandemic, where the dismantling and reconfiguration of familiar temporal markers led to a profound collective and individual sense of temporal disorientation. With the spread of the COVID-19 pandemic, all known markers of time along with the conception of measurable time underwent through dismantling, rearrangement and reconfiguration (Venkatesan and Joshi, 2022). Pandemic time can be experienced at multiple levels: individually, collectively within a community, or organizationally.
Both Antentas (2020) and Venkatesan and Joshi (2022) observed that the COVID-19 crisis was marked by a paradoxical experience of time—simultaneously feeling like a standstill and a period of rapid acceleration. While the pandemic brought many socio-economic relationships to a halt, it also catalyzed significant changes, such as the rapid advancement of digitalization (Antentas, 2020). For healthcare workers, this sense of acceleration was especially pronounced as their responsibilities in managing contagion and patient care intensified, making time feel as if it was moving faster. Importantly, this acceleration was not steady or predictable; rather, it was characterized by a sense of hyper-velocity and overwhelming unpredictability regarding the unfolding events and their consequences (Venkatesan and Joshi, 2022).
Temporal reconfigurations in crisis situations
Because crises represent profound temporal disruptions, they also represent opportunities for temporal reconfigurations, which are associated with temporal structuring and restructuring. Organizations embed temporal structures, norms and assumptions about time that are produced and reproduced through ongoing activities and social interactions (Bansal et al., 2022). In most cases, these elements are unquestioned and taken for granted, which does not prevent them from being occasionally changed during the production and reproduction process in the normal functioning of the organization (Orlikowski and Yates, 2002).
According to Bansal et al. (2022: 11), temporal structures are “shared temporal norms, routines, and devices, such as schedules, timelines, and calendars, that people enact in their everyday practices and that thereby structure social processes over time.” Temporal structuring can occur through four distinct mechanisms: entrainment, planning and scheduling, agency, and chance or serendipity (Pentland et al., 2025). Underpinning these structures are temporal regularities (Zerubavel, 1985), which can be intentionally shaped and adjusted through temporal work to accomplish specific goals (Reinecke and Ansari, 2015). Temporal structures are significant not only because they shape the pace, rhythm, and speed of organizational life—that is, how individuals experience time—but also because they influence what garners attention, the types of challenges that emerge and the way they are addressed. They are equally important in how various phenomena, such as crises, are interpreted. When organizations encounter crises situations that disrupt established temporal frameworks, the process of temporal structuring and restructuring becomes particularly critical. What is unquestioned and taken for granted can become visible, rethought, and reconfigured during a crisis.
The attempt to structure temporal environments can produce conflicts within the organization and with external stakeholders (Reinecke and Ansari, 2015). Adopting an agentic view of temporal structures, we recognize that these structures are formed through action, and, thus, remain inherently flexible (Reinecke and Ansari, 2015). This perspective also acknowledges that temporal structures can be intentionally crafted and altered to guide and manage organizational change, as well as to make social phenomena subject to specific managerial actions, including during crises (Reinecke and Ansari, 2015). The construction of new temporal structures can help resolve conflicts and foster consensus within organizations, which becomes especially vital when anticipation and adaptability are required in crisis situations. To the best of the researchers’ knowledge the role of temporal structures in crises remains underexplored in existing research, and it is this gap we aim to address. Having established the importance of temporal structures within organizations—particularly in the face of crisis—it is crucial to recognize that time-related disruptions do not occur in isolation. Instead, they are deeply intertwined with the emotional landscape of organizational life. As we turn our attention to the interplay between temporal disruptions, emotions, and decision-making, we further explore how these factors collectively shape organizational responses during periods of uncertainty.
Temporal disruptions, emotions, and decision-making
Emotions and their management are essential elements of organizational strategic management (Ashkanasy et al., 2017; Lerner et al., 2015) and crisis management (Faÿ, 2014; Gherardi, 2017; Jin and Pang, 2010; Lerner et al., 2015). Crises—whether economic, health-related, political, or environmental—profoundly transform the perception of time and influence strategic decision-making through individual and collective emotional reactions. Because of their impact on perception and information-processing mechanisms, emotions “constitute powerful, pervasive, predictable, sometimes harmful, and sometimes beneficial drivers of decision-making” (Lerner et al., 2015: 799). In contexts of extreme uncertainty, decision-makers must contend with severe temporal constraints and intense emotional fluctuations, which can alter their rationality and management capacities. The onset of induces a sense of urgency that disrupts conventional temporal structures and creates an impression of time acceleration. The need for rapid response increases the cognitive load on decision-makers (Hällgren et al., 2018). These situations are strongly marked by negative emotions such as stress, anxiety, fear, and sadness (Kayes, 2004; Stein, 2004). These pressures affect how organizational members perceive and interpret the crisis and the uncertainty it generates (Maitlis and Sonenshein, 2010). This heightened uncertainty can further increase stress levels and lead to misinterpretations (Weick, 1990). Furthermore, interpersonal communication is strongly influenced by these emotional states. Certain emotions, such as sympathy, anger, or even pleasure in others’ difficulties (Timothy Coombs and Holladay, 2005), can facilitate communication and crisis management, whereas excessive anger, fear, or anxiety may hinder them (Jin et al., 2016; Turner, 2007; Turner and Stets, 2006).
Temporal acceleration was particularly evident during major economic crises, such as the 2008 financial crisis. During this period, markets underwent extreme fluctuations, forcing investors to make rapid decisions under intense stress (Taleb, 2014; Weick and Sutcliffe, 2011). Financial decisions made during the subprime crisis demonstrated behavior strongly influenced by emotions, leading to market panics and suboptimal strategic choices. This widespread panic resulted in excessive market reactions and hasty decisions by investors and financial institutions (Mdaghri et al., 2024). Furthermore, the limited availability of information led decision-makers to rely heavily on intuition and simplified heuristics. While these heuristics can enhance responsiveness, they can also introduce cognitive biases leading to strategic errors (Kahneman et al. 2011). Thus, these crises highlight the importance of effective emotional regulation in mitigating irrational behaviors and managing emergency situations (Van Bavel et al., 2020). Similarly, natural disasters such as Hurricane Katrina illustrate how the urgency of the situation can lead to rapid but sometimes ineffective decisions, where major failures in decision-making are often attributed to emotional reactions to the emergency (Moreau, 2005).
The COVID-19 pandemic characterized by an extreme acceleration of decision-making processes and unprecedented emotional intensity (Frimousse and Peretti, 2020). While some companies adopted rapid innovation strategies to adapt to emerging constraints, others maintained more cautious approach driven by risk aversion (Amankwah-Amoah, 2020). Several studies have underscored the importance of transparent communication and strategic flexibility in mitigating the negative impact of emotions on organizations (Zahra, 2021).
Emotions exprienced in crisis situations and under temporal constraints fundamentally shape decision-making (Dejoux et al., 2011), particularly by influencing risk perception and motivation to act (Lerner and Keltner, 2001). In a crisis context, negative emotions such as fear and anxiety often induce a more cautious or even defensive stance, whereas optimism can encourage bolder and more innovative strategies (Fredrickson, 2001; Fredrickson et al., 2003). Conversely, acute stress tends to reduce cognitive flexibility and narrows the range of options considered (Starcke and Brand, 2012).
In light of the challenges posed by temporal ruptures in extreme situations, emotional regulation is central to decision-making effectiveness. Cognitive reappraisal, for instance, facilitates the restructuring of event interpretations to mitigate the impact of negative emotions (Sala and Haag, 2016). Furthermore, research indicates that leaders with high emotional intelligence are better equipped to manage crises while maintaining a stable strategic vision (Goleman, 2019).
Finally, multiple studies have demonstrated that emergency situations and threats can also elicit positive emotions and foster resilient behaviors, particularly when frontline managers demonstrate courage and compassion (Quinn and Worlin, 2008). Police officers and healthcare professionals, for example, often navigate moral ambiguity by engaging their own emotions to demonstrate empathy and commitment (Margolis and Molinsky, 2008). Furthermore, integrity-based behaviors appear to strengthen self-confidence and trust in others (Colquitt et al., 2011). Slaughter et al. (2021) also found that employees’ emotional states fluctuate based on their perception of leadership reliability in crisis management. Lastly, organizations that successfully navigate major crises are those that integrate stress management strategies and build resilience in the face of adversity (Giovannini and Giauque, 2023).
These insights underscore how both positive and negative emotional responses play a pivotal role in organizational adaptation and crisis management. Recognizing the complex interplay between temporal disruptions and emotional dynamics, it is essential to investigate how decision-makers experience and navigate time during crises, and how emotions influence their choices. To address these issues, we now present our research questions and outline the methodology guiding this inquiry.
Methodology
Research questions
The research questions this study seeks to answer are the following: How is time experienced as a lived phenomenon by decision-makers during crises? What role do emotions play in shaping decision-making during periods of temporal disruption?
Case study approach
To answer our research questions, we adopt a qualitative approach based on the case study method developed by Yin (2014, 2018). Our research examines the strategic management of the COVID-19 crisis within a French public healthcare organization: the Center Hospitalier Régional Universitaire (CHRU) of Nancy, located in the Grand Est region. Crisis-related decision-making in this setting relies on a multi-level strategic management approach that involves medical, administrative, and logistical stakeholders. A case study is particularly appropriate for investigating a contemporary phenomenon within its real-world context, especially when the boundaries between the phenomenon and its context are not clearly evident (Yin, 2014). Three key dimensions justify this methodological choice: - Decision-Making Under Constraints: In a CHRU, decisions are not solely determined by an administrative hierarchy but are also shaped by medical, sanitary, and political constraints, as well as by resource limitations. - Shared and Adaptive Governance: Crisis management involves a diverse range of actors—including hospital directors, physicians, intensive care teams, and logistical staff—each playing a role in shaping a collective response to the emergency. - An Evolving Decision-Making Process: Unlike standardized management situations, decision-making in a CHRU during a crisis is iterative. Decisions must be continuously reassessed in response to evolving epidemiological data and hospital capacity.
Case context
The Center Hospitalier Régional Universitaire (CHRU) of Nancy was at the forefront of the COVID-19 pandemic from its earliest stages. The virus first emerged in the Alsace region in February 2020 before rapidly spreading westward. Due to its geographical proximity, the CHRU of Nancy faced a critical situation, operating with a time lag of approximately one week compared to hospitals in Alsace. The COVID-19 crisis extended over 2 years and it was marked by multiple waves, each characterized by distinct propagation dynamics, management strategies, and organizational behaviors.
This study focuses on the first wave, during which critical care management had to be swiftly reorganized to accommodate the influx of patients. This wave spanned approximately 4 months (February–May 2020). For the CHRU of Nancy, the first wave officially began on February 29, 2020, with the establishment of a dedicated critical care unit for COVID-19 patients. Chronologically, this phase was shaped by several key milestones requiring significant strategic decisions and specific organizational structures (Gamel, 2020): 1. Detection of the First COVID-19 Cases and Initial Organizational Response: On February 29, 2020, a specialized unit (P3) was opened to accommodate the first COVID-19 patients. Equipped with four critical care beds for highly contagious diseases, this unit facilitated the isolation of early cases and initiated crisis management efforts. 2. Implementation of Crisis Governance: As case numbers surged in the surrounding areas (southern Meurthe-et-Moselle and the Vosges), a crisis steering committee was established on March 12. Consisting of a hospital director, an intensive care specialist, and an anesthesiologist, this committee was responsible for coordinating critical care operations and anticipating intensive care capacity requirements. 3. Initial Restructuring of Hospital Capacity: On March 13, a restructuring of intensive care services was initiated. Medical intensive care units were converted into units dedicated to COVID-19. This increased capacity to 30 beds and enabled the hospital to manage the growing number of hospitalizations effectively. 4. Crisis Mode Activation and Territorial Cooperation: On March 15, the Plan Blanc was triggered, marking a critical shift in pandemic management. This decision formalized the collaboration between public and private healthcare institutions, enabling the pooling of resources and the coordinated critical care patient management. 5. Centralization and Optimized Management of Intensive Care Beds (March 24–April 3, 2020): On March 24, a centralized management system for intensive care beds was implemented to optimize bed occupancy across hospitals within Groupements Hospitaliers de Territoire (GHT) 7 and 8. The peak in hospitalizations was reached on April 1 at the CHRU of Nancy and on April 3 at the regional level. 6. Expansion of Intensive Care Capacity (March–April 2020): A five-phase expansion plan was developed to progressively increase critical care capacity. By converting continuous care units, cardiology wards, post-rehabilitation units, and post-surgical monitoring rooms, the CHRU expanded its intensive care capacity from 68 to 173 beds. Within a period of 15 days, the number of COVID-dedicated intensive care beds increased fivefold, peaking at 165, with 128 designated exclusively for COVID-19 patients. 7. Decline Phase and Gradual Return to Normal (April 8, 2020): From April 8 onwards, the stabilization of intensive care patient numbers enabled the initiation of a five-phase de-escalation plan, mirroring the initial expansion. This phase marked the beginning of a gradual reduction in intensive care capacity and a reallocation of hospital resources.
Data collection
To ensure the reliability and validity of our case study, we employed two complementary data collection methods: - Semi-structured interviews, which provided direct access to the perceptions of hospital stakeholders involved in decision-making, highlighting the challenges and trade-offs they faced. - Document analysis, which enabled an examination of protocols, guidelines, and internal communications that structured crisis management.
Informants and interviews.
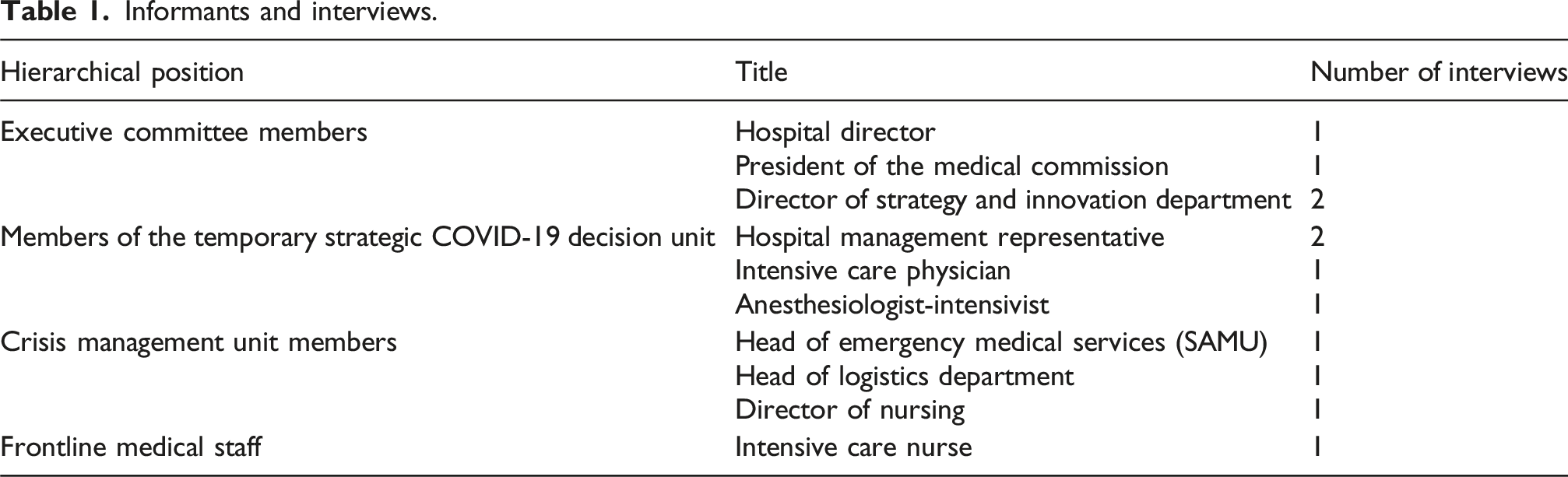
The interviews were conducted in French between April 2021 and March 2022, after the critical phase of the health crisis. They were carried out as part of a broader research initiative launched in early 2021 (Project REMAHO: Renouvellement du Management Hospitalier et Adaptabilité des Organisations), developed in response to the difficulties encountered by key socio-medical stakeholders in the Grand Est region of France in managing the health crisis.
The Grand Est region was one of the hardest-hit areas in France during the COVID-19 pandemic. This research project followed an intervention research approach, aiming to support decision-makers in improving crisis management mechanisms. The study sought to analyze the decision-making processes implemented, identify key drivers and constraints, and provide scientifically grounded recommendations to optimize institutional responses to large-scale health crises. Consequently, interviews were conducted retrospectively, allowing participants to reflect on their experiences with hindsight and analyze the decision-making dynamics enacted during crisis management.
The interviews lasted between 1.5 and 2 hours and followed a semi-structured approach, combining a pre-established framework, guided by an interview protocol, with the flexibility to encourage respondents to express themselves openly. A rigorous preparatory phase was undertaken to ensure the quality of the interviews and mitigate biases. This preparation included a thorough analysis of interviewees’ profiles, considering their professional background, role in decision-making, and involvement in the COVID-19 crisis management. Such an approach allowed us to tailor discussions to the specific context of each participant and refine the relevance of the questions asked.
During the interviews, participants were asked to describe their involvement in crisis management and decision-making processes in detail, specifying their role, actions taken, decisions made, and their perceptions of the crisis. Emphasis was placed on identifying key factors that influenced crisis management. In addition, more elaborate and specific questions were asked to obtain concrete and detailed examples of the measures adopted. The interviews thus encompassed both factual events and decisions as well as respondents’ subjective perceptions, exploring the underlying motivations and justifications behind the choices made. This approach helped mitigate retrospective rationalization biases by encouraging participants to provide precise, context-based narratives, thereby reducing the risk of ex post reconstruction of decisions and actions taken during the crisis.
Document analysis enabled us to examine both the external and internal decision-making context at the CHRU of Nancy during crisis management. The following documents were analyzed: - National and regional government directives (Ministère de la Santé, Agence Régionale de Santé, Plan Blanc CHRU, ORSAN framework). - Expert testimonies published in mainstream and specialized media. - Minutes of crisis meetings: chronological records of decisions and measures adopted. - Internal communications, such as emails, WhatsApp exchanges among hospital executives.
Data analysis method
Data analysis was conducted using thematic analysis (Braun and Clarke, 2006) following a three-step approach: - Initial coding of interviews and documents. - Grouping of codes into broader themes (e.g., “decision-making dynamics,” “organizational adaptation,” “collective sensemaking”). - Interpretation of results in relation to existing theoretical frameworks.
Data analysis was carried out concurrently with interview data collection to ensure a deeper understanding of the sequence of events and to progressively refine the chronology of actions and the roles of various actors in crisis management and decision-making. This iterative approach allowed us to develop a comprehensive view of the decision-making process by identifying key phases, major activities, actions undertaken, and the roles played by different stakeholders.
All interviews were transcribed and analyzed jointly by both interviewers, ensuring cross-validation and a rigorous interpretation of participants’ narratives. Each respondent was also treated as an individual case study, allowing for an in-depth description of their actions and responses to the crisis while identifying the factors that shaped their behavior over time. This dual-level approach enabled us to: - Gain a nuanced understanding of organizational and temporal dynamics at the institutional level. - Conduct a detailed analysis of individual perceptions and decision-making.
To synthesize and structure the findings, data were organized into key thematic categories, systematically comparing participants’ accounts. This approach facilitated the identification of convergences and divergences across narratives, allowing us to uncover significant patterns while accounting for the diversity of experiences and perspectives. From this analysis, five major themes emerged: - Time as a lived phenomenon during crisis - New temporal structures - Organizational concert time - Emotions and decision-making process - Emotions and decision-making success
Findings
Time as a lived phenomenon during crisis
Venkatesan and Joshi (2022) talk about the fact that the COVID-19 crisis was experienced by people both as a halt and as acceleration, the latter being the case in health care institutions since they had to manage and control the spread of the virus. Our analysis shows that the experience of time by the decision-makers during the COVID’s first wave had many different nuances and phases. The interviewed representatives of the DMUs described the time of the COVID-19 pandemic as “exceptional,” “without a reference,” “completely different and surrealist,” “improbable circus,” and even “paradise.” The reasons for this are as follows. To begin with, the initial wave of COVID-19 presented a completely unprecedented scenario. The staff were uncertain about the appropriate course of action. There were no established routines to follow, as the existing plan blanc was not adequate for a prolonged crisis lasting several months. According to one of our interviewees: “The plan blanc is designed to manage a derailed train. So, you’re at full speed for three days, four days, five days, and then it goes down … but it is not for a sanitary crisis that lasts for months and months.”
Second, while the general population was required to pause their activities because of the lockdown, the hospital staff continued their duties without interruption. As one of our interviewees explained: “...at the hospital, we worked. It was one of the last places where people continued to work.” This made the medical staff, including the decision-makers at the hospital, feel different and even privileged because as one interviewee highlighted: “We had the right to go out as we wanted. Of course, it was only to go to work …but we still had a social life that continued a little bit. There are people who didn’t leave their homes for weeks.” The time of the first wave was also described as euphoric, because the situation was unfamiliar and this sparked a renewed sense of motivation and engagement. As one interviewee put it: “So, the first wave until the end of the first lockdown in May-June 2020 was really euphoric, it was truly euphoric!” Another respondent added: “There was euphoria, especially during the first wave, when people thought it would last a few weeks and then everything would be fine.” The euphoria can also explain why the situation was described by some of our informants as “paradise” since everyone wanted to be involved. In the words of one of the interviewees: “The most disappointed were those to whom they said “No! We have enough people already.’ Everyone wanted to do this, the emergency physicians, the nurses, the reanimators…”. In addition, many experienced a sense of euphoria, largely stemming from the uncertainty about the crisis’ duration. Their initial assumptions did not extend to the possibility of the pandemic lasting for several months or even years; instead, most believed it would conclude after the first wave.
The acceleration of time was directly linked to the rapid surge in COVID-19 patient admissions over a brief period. Interviewees described this acceleration through the heightened intensity of interactions both among themselves and with the public. This was especially evident for Emergency Medical Assistance Service (EMAS), which, in the initial days, had to manage an overwhelming volume of calls. As one informant noted, their activity increased by five or six times.
What enabled the various departments at the hospital to better anticipate this acceleration of time was the fact that Mulhouse—the city where COVID-19 first appeared in France—was roughly a week ahead in the course of the pandemic. The Nancy hospital maintained a strong connection with Mulhouse, as even prior to the crisis, Mulhouse struggled with understaffing and had sought Nancy’s assistance in handling some EMAS calls (though this collaboration did not materialize). Furthermore, the individual overseeing EMAS in Mulhouse had formerly worked at the Nancy hospital. This relationship ensured that the Nancy teams were well informed about developments in Mulhouse and could adapt their response accordingly. As one interviewee recounted, “So, when they [Mulhouse] started to have problems, we said to ourselves ‘Ouh là là, ou là là,’ and a few days later we had the first cluster in Nancy and in a few days, we exploded the regulation.”
New temporal structures
In addition to the fact that decision makers at the hospital had a complex experience of time during the COVID-19 pandemic, the situation also led to the formation of new DMUs, specifically the two trios 1 . They operated with new temporal norms, and they used new devices. It is important to highlight that no routines were established, as they were required to adapt constantly and make rapid decisions, leaving no opportunity for a regular temporal rhythm to emerge during the first wave.
Temporal norms
The new temporal norms, which were established and governed the newly created DMUs, made time plastic by blurring the line between personal and work time. Members of each trio could contact one another at any time, including during nighttime and weekends. As one of the interviewees put it: “So, depending on the time of the crisis, when we had fewer and fewer beds and we had to decide on the opening of new sectors, we were in very close communication, which was not always the case before. Hence, we called each other once a day, twice a day, three times a day… including on Saturday and Sunday.”
This newly established temporal norm marked a clear departure from previous practices, which relied primarily on e-mail as the standard form of communication. In contrast, maintaining constant connectivity throughout the crisis became essential for ensuring that all trio members remained continuously informed. As one interviewee emphasized: “… between the three of us, we always had the same level of information.”
Because the decision-making team consisted of just three members who maintained constant communication, they were able to coordinate closely and make decisions swiftly, effectively responding to the rapid acceleration of time brought on by the surge in the number of COVID-19 patients. In the words of one of our informants: “when three people make the decisions, we were the trio, connected all the time, it was more efficient, it was indisputably more efficient, it was less democratic, but it was more efficient”.
Devices
To facilitate regular communication among trio members, they used Teams—a platform that was unfamiliar to some of them prior to the crisis. For example, one of the interviewees said: “we adjusted [the decisions] from one meeting to the other by Teams from our mobile phones.”
Additionally, for planning, they used a map of France that was two meters long to organize the transportation of COVID-19 patients by train and plane. As one interviewee described: “...on a surface of 2 m where we had the map of France, we managed our planes...in the past, we would have taken a paper and a pencil.” These tools helped in a decision-making process, qualified by one of our informants as “almost immediate.”
The introduction of new temporal structures and communication tools shaped how the two DMUs interacted, fostering a shared sense of time and coordination among their members.
Organizational concert time
The experience of concert time within a team is characterized by the alignment of members’ internal, subjective perceptions of time. This concerted focus emerges when individuals concentrate on the same issue (in this case, the COVID-19 crisis), share an intense level of attention (reflected in the frequency and depth of their interactions), and develop a strong sense of togetherness. We will present how the members of the trios and other decision-making agents at Nancy hospital experienced these aspects.
Object of attention
The object of attention was the sudden and very rapid increase of COVID-19 patients arriving at the Nancy hospital. This influx drove the hospital to escalate quickly through its emergency response levels, ultimately reaching level 6 out of a possible 7. In response, the staff opened their final available sector and convert it for patient care. At this critical juncture, the number of incoming patients finally began to decline. As one informant reflected: “…we had gone up to, I remember well, there had been seven levels planned, the seventh was ours to transform a unit of short stay to an intensive care unit. We equipped it and then it was not activated because it started decreasing just at that time.”
Besides the complexity created by the increased number of COVID-19 patients, the sanitary crisis led to simplification of the medical staff’s work since during the first wave, they practically had to handle only COVID-19 patients. As it was highlighted by one of our interviewees: “During the first and the second wave, the hospital stopped, it handled only COVID-19. But really only that. And, so, everything was focused on saying we’re moving forward on this subject.” All other illnesses seemed to disappear—a phenomenon that remains unexplained. As one interviewee remarked: “… everyone had the same objective as there was only one category of patients. There were no more road accidents since people were confined and on the medical level, there were no more infarctions, no more strokes … the usual things. We wondered what had happened with them. Two years later, there is not necessarily an explanation for that.”
In addition, the pandemic simplified the relationship by making people forget their differences and conflicts. In the words of one of our informants, the relational problems that people had before the COVID-19 crisis “...completely disappeared during the crisis.” Another informant assured: “Overall, relations have been fairly simple and simplified by the crisis.” The reduction in interpersonal conflicts among the medical staff can also be attributed to a shared sense of collective euphoria, which spread throughout the staff and helped to dissipate tensions. The crisis has left an emotional mark on people as a unique experience. As one interviewee put it: “It was extraordinary! When I say I feel it, I feel it with a lot of emotion… This crisis was lived with all my soul and went through my inner being. The emotion of the human being, and above all this closeness, this closeness of all at the service of the sick. It was extraordinary. A human adventure that I think we will never know again. And I am happy to have lived it. It was unique and an adventure that I will never know again in my life”.
Intensity of attention
The intensity of attention manifested itself in the number of interactions, which was imposed by the need to make decisions very quickly to respond to the sudden and fast increase of COVID-19 patients. New temporal norms were established, which permitted effective decision making in real time. As it was highlighted by one of our informants: “… it’s not the same thing when you see someone once every 36 months and when you see them almost 24 hours a day by videoconference.” Alongside the trio’s close coordination, regular gatherings were organized with the Crisis Cell—comprising roughly 150 participants—where the team communicated the trio’s decisions, and staff were encouraged to pose questions and express their views freely.
Feeling of togetherness
The sense of unity stemmed from the fact that everyone was focused on a single, shared objective, devoting the same level of attention to the pressing issue of COVID-19 patients. As noted earlier, the extraordinary nature of the crisis and the urgent need for a swift, effective response prompted members of the trio to set aside their prior disagreements and come together, working in concert toward a common goal. By describing the way they worked during the crisis, one of our interviewees said: “...we were complementary, we forgot our differences, and we tried to see what was best for the hospital.”
Furthermore, numerous interviewees underscored that they faced significant challenges with the Regional Agency of Health (RAH), which failed to coordinate effectively with them or to make adequate decisions throughout the COVID-19 crisis. This lack of alignment was cited as a unifying factor that brought the Nancy hospital’s medical staff closer together. In the words of one of our respondents: “It’s unfortunate but the fact that the RAH was a little complicated with us, it also federated everyone”.
The interviewees emphasized that this sense of unity extended to include the hospital Administration, with both the trio and the Administration expressing this shared sentiment. As one member of the trio reflected: “Before, we were never this close to management. And to see the effect of our decisions on the hospital so quickly, that was rather new, rather unusual.” One member of the hospital's Administration highlighted that physicians came to appreciate the role of management within the institution, emphasizing that the “proximity of governance” is the one aspect that should be preserved after the COVID-19 crisis. The experience of organizational concert time shared by both DMUs and their closest colleagues resulted in a unified vision, coordinated decision-making, and aligned actions throughout the management of the COVID-19 crisis.
Emotions and decision-making process
The findings highlight the structuring role of shared emotions in reinforcing adaptive rationality and shaping the power dynamics in the hospital.
Rationality
The management of the COVID-19 crisis at the Nancy University Hospital was grounded in adaptive rationality, activated in a context of extreme urgency. Emotions did not hinder analytical thinking; rather, they intensified and oriented it toward immediate action. The crisis was led by a compact leadership trio, structuring a decision-making process based on daily meetings and up-to-date information systems, enabling effective operational coordination. One senior team member explained: “We had a meeting every morning at 9 a.m. It was very intense. Every morning, we made decisions.” Another professional noted: “We had to adapt constantly to the situation, so we were adjusting almost every day.” This fast and continuous rationality was reinforced by the acute perception of the crisis’s severity: “What really changed was the immediacy of decision-making and implementation.” Emotions related to urgency, responsibility, and the fear of hospital overload supported the cognitive mobilization of actors.
Power
Leadership was perceived as legitimate and mobilizing, largely due to emotional proximity with frontline teams. Mutual trust helped prevent open conflict. One leader reflected: “We needed to convince, not impose. And in a crisis, we had to convince quickly.” Still, the balance was fragile: “There were moments when decisions came from the top without consultation, and it wasn’t always well received.” Despite strong centralization, efforts to build consensus remained constant. The patient dispatching system, inter-institutional coordination, and daily interactions fostered a collective dynamic and coordination. As one respondent described: “We made decisions together. There was a lot of consultation, even though someone had to make the final call.” Another interviewee emphasized the fluid coordination: “We had daily updates with leadership, physicians, and logistics leads.” Participation was enabled by strong operational proximity. The crisis reduced hierarchical distances and accelerated cross-functional cooperation. As one respondent stated: “What worked is that we were very close to the field.” Another added: “Hierarchical barriers fell; we directly contacted heads of units, nurses, and doctors.” This dynamic was emotionally supported by a shared sense of engagement and solidarity: “The crisis broke down silos.” and “We had never communicated this much.”
By adapting to urgent needs and encouraging open communication, leadership remained legitimate, enabled swift decisions, and boosted staff morale—proving that flexible leadership and emotional unity were vital during the COVID-19 crisis. Shared emotions of urgency and solidarity sharpened focus and drove rapid, coordinated action.
Emotions and decision-making success
The findings show that emotions significantly shaped the process and the performance of decision-making during the crisis, by accelerating the pace of action, enhancing clarity and collective satisfaction, fostering organizational learning, and enabling an exceptional mobilization of individual competencies. Emotions played a decisive role by fostering a strong sense of collective alignment and purpose, enabling fast, agile and coherent decisions, supporting lasting organizational learning, and catalyzing structural innovations as well as the feeling of shared purpose.
Speed
Decisions made during the first wave of COVID-19 were characterized by exceptional speed, driven by intense emotional mobilization. The awareness of vital risk prompted actors to bypass typical bureaucratic delays. One leadership team member reflected: “Sometimes, only 30 minutes passed between the decision and its implementation. It was madness.” Another professional echoed this accelerated pace: “We made decisions in the morning and implemented them by the afternoon.” These swift decisions were seen as necessary and meaningful, despite the burden they placed on staff.
Clarity and satisfaction
In this complex context, emotions paradoxically fostered clarity. Shared objectives—saving lives and maintaining hospital operations—reduced organizational ambiguity. As one professional noted: “It wasn’t confusing. We knew what we were doing and why.” Team satisfaction, though moderated by fatigue, was rooted in a sense of pride and usefulness: “There was strong pride despite the fatigue. We felt we were at the heart of something important.” Another participant affirmed: “Honestly, I wouldn’t do it much differently.”
Organizational and individual learning
The emotional intensity of the crisis acted as a catalyst for organizational and individual learning. It encouraged a reassessment of prior practices and inspired new ones. One interviewee explained: “We learned to work differently. To trust each other faster.” Another added: “We’ve retained some of those practices—direct communication circuits, stronger links between departments.” The crisis enabled exceptional mobilization and development of competencies, often beyond formal roles. One respondent recalled: “Those who were usually quiet came out of their shells.” Another observed: “We saw colleagues doing things we’d never imagined.” Some emphasized seamless synergy: “There was harmony, a tacit complementarity.” Yet this adaptability also had costs: “There was a huge shift… leading to exhaustion, tensions, resignations.” Here, emotions served a dual role—both as catalysts for self-transcendence and as sources of emotional strain.
Shared purpose
The success of crisis management at the Nancy University Hospital was deeply linked to the emotional alignment of actors around a shared mission—saving lives. Interviewees repeatedly emphasized a strong sense of collective purpose, built on shared emotional commitment and moral urgency. One respondent stated, “We are all fighting for the same cause… we are all in the same boat,” highlighting the emotional glue that underpinned unified action. This alignment created a feeling of clarity and reinforced the legitimacy of decisions, reducing ambiguity in the face of complexity and uncertainty.
Agility and simplicity
Participants viewed the rapidity and clarity of decision-making as key success factors, both made possible by the emotional intensity of the moment. The immediacy of decisions, bypassing normal bureaucratic filters, was supported by trust and emotional readiness: “Our decisions were simple and reasonable… we will never make a decision that doesn’t make sense.” Emotional urgency compressed time, catalyzing action and reducing friction.
Innovation
Emotions also contributed to innovative practices, including resource sharing, creation of mobile expertise teams, and real-time coordination software. Participants emphasized the emotional readiness to collaborate: “There was harmony… a tacit synergy.” The combination of emotional engagement and structural reform enabled exceptional results, such as increasing bed capacity by 2.5 times and establishing regional dispatch systems. These achievements were not only technical but also important emotional milestones.
Discussion
This study helped us shed some light on the way time was experienced by the members of the DMUs and their closest collaborators at the hospital of Nancy. While the broader medical staff sometimes felt time had slowed or stopped (Antentas, 2020), those directly involved in the DMUs and their closest collaborators consistently experienced a sense of acceleration.
The decision makers were responsible for determining the required number of beds, designating which departments would manage them, establishing their opening timelines, and assigning staff to provide care for COVID-19 patients. According to our sources, these choices had to be made extremely rapidly—within a maximum timeframe of 48 hours. The acceleration of time though was much more nuanced as reported in previous research (Antentas, 2020; Venkatesan and Joshi, 2022).
In response to the accelerated pace of events, the DMUs established new temporal structures grounded in new norms. Their standard became remaining connected around the clock via mobile devices and the Teams digital platform, ensuring that all members accessed real-time information and could make swift, well-informed decisions. Typically, temporal structures rely on established routines (Bansal et al., 2022). However, the rapid pace of events during the crisis made it impossible for the DMUs to develop such routines. In contrast, the Crisis Cell—which included approximately 150 members—was able to maintain a routine by holding weekly meetings via Teams. These sessions served as opportunities for decision makers to update the broader medical staff about actions taken and implemented in the hospital. It is important to note, though, that these meetings were not intended for the actual process of making decisions.
In addition, we must highlight the importance of the new digital tools (such as the Teams platform) in the enactment of the new temporal norm, which required the members of the DMUs to be connected 24/7. These devices, which were appropriated by the DMUs’ members, made the process of timely information sharing, coordination and decision-making possible. In addition, the director of the hospital’s Strategy and Innovation Department mapped all decisions made by the DMUs on a timeline. This enabled the DMUs’ members to not only stay informed about the rapid decisions being made, but also to understand the rationale behind each decision.
The hospital decision-makers’ experience of time was intimately tied to episodes of temporal disruption, which altered the pace, phase, and sequencing of tasks for everyone in the hospital (Pérez-Nordtvedt and Harrison, 2025). The emergence of a new temporal norm—marked by ongoing interaction among DMU members—fostered a sense of temporal togetherness, as all attention converged on the COVID-19 crisis with a shared intensity of focus (Sharron, 1982). This is the way concert time manifested itself within the two DMUs during the COVID-19 crisis. Building on the Sharron’s definition (1982), we define concert time in organizations as the concerted and consented time perception of the members of a team or an organization. In other words, concert time is a temporal alignment of the members of a team or an organization based on being focused on one objective with the same (or similar) intensity of focus. This temporal alignment is possible because the team members agreed on a shared temporal norm, which enables continuous interaction among the members of a group. As a social product, concert time exists as long as the members interact together (Sharron, 1982).
Since it is based on continued interactions, concert time is undeniably related to the experience of emotions, which were also shared among the interacting members of a group. During the initial wave of COVID-19, members of the DMUs and the entire medical staff felt a sense of euphoria, as they faced a novel disease and were able to continue working while the rest of the people remained at home under the French government’s lockdown.
The adoption of shared temporal norms, structures, and tools can evoke emotional responses that influence how team members perceive and experience time. In our research, we specifically identified a sense of organizational euphoria—an emotional state that is rare during crises, where positive feelings such as hope, relief, and joy have been typically studied by previous research (Maitlis and Sonenshein, 2010). There are many internal (same object of attention) and external factors (social recognition) to explain the emergence of this shared emotion among the medical and the nursing staff of the Nancy hospital, but one reason is the constant interactions, which allow the spread of emotional states, or in other words which produce emotional contagion (Barsade, 2002). In crisis situations, collectively shared emotions may override individually felt emotions. The perception of alignment and togetherness among the members of a group may cause other members to reshape their own feelings about the reality of the crisis. In addition, the perception that others share the same emotions may motivate people to act. Collective emotional states can arise not only from shared interpretations, experiences, and organizational culture (Mackie et al., 2000; Van Maanen and Kunda, 1989), but also from heightened interaction and coordinated actions. In this sense, our study shows that in certain situations characterized by intensified interactions and actions, temporal structures in crisis situations cannot be only regarded as “shared temporal norms, routines, and devices” (Bansal et al., 2022: 11) but also as shared emotional states.
In addition, previous research shows that positive emotions can help broaden the vision and actions of decision makers (Fredrickson and Branigan, 2005) and even enhance the ability of individuals to cope with the stress generated by the crisis (Fredrickson et al., 2003). At the Nancy hospital, the collective euphoria experienced during the initial COVID-19 wave ensured that there were sufficient personnel to manage the influx of patients—a situation that did not last in subsequent waves. This abundance of medical and nursing staff stemmed from a surge in volunteers eager to contribute to patient care during the crisis. The positive emotional climate also fueled rapid decision-making and implementation, reinforcing the perception that crisis management efforts were effective. Yet, it is important to recognize that such heightened positive emotions can foster overconfidence and lead to misjudging the severity of the crisis, particularly when these emotions reach high levels of intensity (Mayer et al., 1992). Accordingly, future research should examine the potential drawbacks of concert time and the spread of positive emotions in crisis contexts.
Conclusion
Our study looks at the way time is experienced as a lived phenomenon by the decision-makers in a hospital during the COVID-19 crisis and how the emotions associated with living a temporal disruption impact the decision-making process. We believe we contribute to the increasing body of literature on time in organizations in several ways. First, to the best of our knowledge, the role of temporal structures in crisis situations has not received a lot of attention in the existing literature.
Our research contributes to organizational time studies by highlighting that crises often disrupt established temporal structures (Venkatesan and Joshi, 2022), requiring the creation of new norms that may or may not rely on established temporal patterns (Zerubavel, 1985) or routines (Bansal et al., 2022). Whether these new norms are based on regularities or routines largely depends on how quickly decisions must be made.
Second, based on Sharron (1982), we provide a definition of concert time in organization, which is a temporal alignment of the members of a team, or an organization based on being focused on one objective with the same (or similar) intensity of focus. We argue that concert time is an important concept in management of organizations, especially when they face crisis situations due to two main reasons. First, when everyone is united around a common goal, it becomes easier for group members to streamline the flow of information and coordinate their actions regarding the issue at hand. This is especially crucial during crises, as the rapid pace and disruption of normal timing, sequencing, and task phases (Pérez-Nordtvedt and Harrison, 2025) increase the complexity of decision-making. Second, the intensity of interaction creates the feeling of togetherness that motivates the group members and increases the mutual reliability and trust.
This study also advances current research on the role of emotions in decision-making under crisis by showing how temporal disruptions can intensify emotional experiences and, in turn, become central to organizing processes. While temporal structures are usually anchored in routines and shared expectations (Bansal et al., 2018), our findings reveal that in the absence of such routines—particularly during the urgency of the COVID-19 crisis—emotional intensity emerged as a key coordinating mechanism. The concept of concert time, characterized by continuous interaction and emotional alignment, illustrates that time in crises is not merely compressed or accelerated, but emotionally charged. This resonates with recent findings by Venkatesan and Joshi (2022) and Pérez-Nordtvedt and Harrison (2025), who highlight the inseparability of temporal and affective coordination in high-pressure contexts.
Moreover, this research challenges dominant narratives that frame crisis-related emotions primarily in terms of fear, anxiety, or stress (Kayes, 2004; Turner, 2007). Instead, we document how shared positive emotions—such as pride, moral purpose, and collective enthusiasm—can fuel rapid collective mobilization. This aligns with Fredrickson et al. (2003), who demonstrate that positive emotions broaden cognitive repertoires and support adaptive coping. However, our findings also underscore the fragility of such emotional alignments. As the crisis subsided, the lack of organizational recognition for the emotional efforts invested by actors gave rise to a sense of disillusionment and betrayal. This phenomenon reflects the concerns highlighted by Maitlis and Sonenshein (2010), who argue that while emotional sensemaking is crucial during crises, it can rapidly break down if the emotional work involved is overlooked.
Similarly, Huy (2011) warns that overlooking group-focused emotions can generate resentment and undermine strategic cohesion in the long run. Through this lens, our study contributes to a growing body of literature emphasizing that emotions are not peripheral but central to how crises are experienced, managed, and made sense of—both during and after the event.
In addition, past research demonstrates that the emotions felt and shared within a group can predict the level of cohesion or conflict among its members (Huy, 2012). Our research shows that concert time, characterized by a shared focus on one objective (the COVID-19 patients), and the intensity of interactions among DMU members, as well as the experienced feeling of togetherness and euphoria, helped some actors overcome their differences and past conflicts. This facilitated collaboration during the COVID-19 pandemic. Future research can explore whether the experience of concert time always leads to overcoming conflicts or in some cases, it may lead to the escalation or exacerbation of conflicts.
This study has several limitations. It is based on a single case study of a French public hospital, which restricts the generalizability of the findings. Future studies can expand the scope by looking at other organizations—both public and private—and explore the ways crises impact organizational temporal structures. It will also be of interest to investigate how temporal disruptions and the emotions they generate influence the decision-making process across different institutional contexts. Second, this study is based on interviews with decision-makers at a public hospital, whose working conditions are specific and context-dependent. Future research could examine private-sector organizations, which operate under different constraints and possess unique characteristics, providing valuable comparative perspectives on how these factors influence organizational responses to crises.
Third, our study relies on retrospective accounts provided by our interviewees (Eisenhardt and Graebner, 2007). Since participants’ narratives are shaped not only by their memories of the events but also by the present-day context, this may alter their interpretations and evaluations over time. While this retrospective bias was partially mitigated by relying on the accounts of highly knowledgeable respondents—as was the case in our study (Eisenhardt and Graebner, 2007)—we nonetheless acknowledge the possibility that such bias may have influenced the data.
Finally, this research provides practical guidance for managers. When crises disrupt established temporal patterns, it becomes essential for managers to quickly create new time-related norms that fit the emerging needs. Additionally, the idea of concert time proves vital in crisis management. By fostering unified attention on a common goal and promoting frequent, focused interactions, managers can improve team coordination and streamline communication, both of which are critical in challenging times.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.