
Abstract
Research has indicated that medical doctors and paramedics are at higher risk of being stalked than the general population. In particular, mental health care professionals alone represent one third of the victims of harassment. Because of the lack of studies in this specific sector, especially in Italy, in this study, we examined the stalking of psychiatrists by their patients, considering gender differences and the incidence of stalking in private practice and public mental health clinics in Rome. We found that the rate of stalking in private mental health settings is higher than that in public settings and that the perpetrators of stalking are mainly women who mostly target mental health professionals working in private practice. Implications of the findings are noted and discussed.
Introduction
The typical stalker or “modal” stalker has been described as a male in his fourth decade of life pursuing a prior sexual intimate (Meloy, Mohandie, & Green, 2011). He is usually single or separated; he is not able to control his emotions and anger which, if associated with obsessional behaviour, might lead to violent actions (Morrison, 2001). Clinical and epidemiological studies and daily evidence from antiviolence and antistalking units confirm that the primary perpetrators of this crime are men and that the overwhelming majority of victims are women. More precisely, female stalkers are outnumbered by male stalkers by four to one (Pathé & Mullen, 1997).
Nonetheless, stalking is a gender-neutral behaviour and both genders can be victims and perpetrators of stalking. The so-called “same-gender stalking” differs from other types of stalking in the characteristics of the prior relationship between the victim and the stalker, the motivations for the pursuit being mainly workplace disputes, and/or conjugal betrayals (Strand & McEwan, 2011a). In their classification of stalking, this type of stalking was classified as “resentful” by Pathé, Mullen, and Purcell (2000).
Except for the literature on erotomania, little attention has been given to women who persistently intrude on and stalk others. Nonetheless, stalking by women is not uncommon. The consequences of this harassment may have serious psychopathological consequences. Psychiatrists and those working in related subspecialties, such as forensic psychiatry, appear to be, among the various medical specialties, at greater risk of being harassed (Abrams & Robinson, 2011). Studies on these topics and pertinent literature are noted and discussed below.
Literature Review
Community-based studies of stalking victimization indicate that women are identified as the perpetrators in 12% to 13% of cases (Tjaden & Thoennes, 1998). Zona, Sharma, and Lane (2005) reported that 32% of participants (24 out of 74) investigated by a specialist antistalking unit were female, 6 of whom were classified as erotomanic. Harmon, O’Connor, Forcier, and Collins (2004) similarly found that 33% of stalkers (16 out of 48) referred to a forensic psychiatry clinic were female, although this rate dropped to 22% in a subsequent and larger study. Other studies have reported lower rates, between 17% (Meloy et al., 2011) and 22% (Palarea, Zona, Lane, & Langhinrichsen-Rohling, 1999).
Despite the frequency with which women engage in stalking, and although women are less likely than men to use violence, except for the category of “ex-intimate stalker” (Meloy et al., 2011), no study to date has considered the context in which this behaviour emerges among women or whether female stalkers differ from their male counterparts in relation to stalking characteristics or propensity for violence. This last aspect has been examined only in recent psychopathological studies that indicate that in both genders, violence is proportional to the level of intimacy of the relationship (Morrison, 2008). Violent female stalkers are reported to be more likely to suffer from personality and affective disorders than male stalkers, who more often display obsessive and psychotic behaviours (Strand & McEwan, 2011b).
Victimization studies indicate that women are seldom prosecuted for stalking offenses, with criminal justice intervention most likely to proceed only in those cases involving a male suspect accused of stalking a woman (Hall, 1998). The available evidence suggests that stalking by women has yet to be afforded the degree of seriousness attached to harassment perpetrated by men. This is despite any empirical evidence that women are less intrusive and persistent in their stalking or pose any less of a threat (physical or otherwise) to their victims.
The literature demonstrates that female stalkers do not differ from their male counterpart in terms of their demographic profiles or psychiatric status, but male stalkers are more likely to have histories of criminality and substance abuse (Purcell, Pathé, & Mullen, 2001). The intrusiveness and duration of stalking activities are equivalent for males and females, as are the rates of associated threats and violence. What does distinguish female from male stalkers is their choice of victim, which is effectively the underlying motivation for their stalking and the context in which their behaviour emerges. Almost all women tended to pursue an individual already known to them. Dressing, Scheuble, and Gass (2006) found that a substantial proportion (40%) fixed their attention on those with whom they had professional contact, particularly psychiatrists, psychologists, family physicians, and occasionally on teachers and legal professionals. Although the choice of victim among female stalkers was heavily skewed toward professional contacts, male stalkers pursued a broader range of victims, with similar proportions harassing prior intimate partners, acquaintances, strangers, and professionals. Stalking by men was more strongly gendered, with 91% pursuing victims of the opposite sex, in contrast to women, who were equally likely to target either men or women. Although it is often assumed that same-gender stalking cases involve homosexuality in either the perpetrator or the victim, or both, the data suggest that this is the exception rather than the rule (Purcell et al., 2001).
Among the various disorders examined in female stalkers in one study, erotomania was present in from 6% to 20% of cases (Meloy & Boyd, 2003). The nature of the “hoped-for intimacy” desired by these stalkers, usually romantic or sexual in type, includes aspirations such as establishing a friendship or even a mothering alliance with the victim. Therefore, it is not surprising that mental health clinicians are so frequently targeted by female erotomaniacs, their professional concern and empathy reconstructed as romantic interest.
One study that used Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision; DSM-IV-TR; American Psychiatric Association, 2000) diagnostic criteria found that female stalkers often had a diagnosis of personality disorder (PD), especially Cluster B type (also defined as “melodramatic”) according to DSM-IV-TR criteria (West & Friedmen, 2008). Another study found that borderline PD had been recently diagnosed in 15% of female stalkers in samples of prisoners and in 40% of female stalkers who had no history of criminal offenses (Sansone & Sansone, 2010).
The methods of harassment used are largely equivalent between male and female stalkers, and even their tenacity is strikingly similar. Thus, although the contexts for stalking vary between men and women, the intrusiveness of the conduct and its potential for psychological harm to the victim does not (De Smet, Buysse, & Brondeel, 2011). There is no reason to presume that the impact of being stalked by a female would be less devastating than that by a man (Kuehner, Gass, & Dressing, 2012), although the number of studies conducted on this specific issue is still rather limited.
Although driven in some instances by resentment or retaliation for perceived hurt, the majority of female stalkers are motivated, as already specified, by a desire to establish an intimate relationship with the victim, who often is a current or former professional helper. Doctors and health care professionals are at greater risk of being stalked than the general population, particularly by their patients (Pathé, Mullen, & Purcell, 2002; Purcell, Pathé, & Mullen, 2005). Pathé and Mullen (1997) found that health care professionals, particularly medical doctors, were overrepresented in a sample of victims who self-referred to a stalking clinic.
In one study, clinicians attending a state psychiatric conference in the United States were surveyed. Nearly a third had been subjected to stalking and a further 41% reported other forms of distressing intrusions, including damage to property (Lion & Herschler, 1998). Psychologists also appear to be at higher risk, according to results from two large random surveys. Gentile, Asamen, and Harmell (2002) found that 10% of a sample of American psychologists had experienced serious stalking events during their careers; in an Australian sample, Purcell et al. (2001) found that nearly 20% had experienced stalking, nearly half of which had occurred in the previous year. Several studies have surveyed mental health staff working within defined settings. Sandberg, McNiel, and Binder (2002) surveyed the clinical staff employed in an American inpatient unit. More than half of the respondents reported having experienced some type of stalking, as well as threatening or harassing behaviour during their career. Also included were threats, telephone calls, and unwanted approaches. Yet, shadowing and violence were rather rare.
Perpetrators usually targeted staff members who had previously treated them. Staff commonly confronted the patients about their behaviour, but did not find this strategy particularly helpful. Patients who stalked staff were more likely than a comparison group to have a diagnosis of PD and/or paranoid disorder. In addition, they were more likely to have never been married, to misuse drugs and alcohol, and to have a history of assaultive, fear-inducing, and self-harming behaviour, and multiple hospitalizations (Sandberg, McNiel, & Binder, 1998).
In a recent Italian survey conducted by psychiatric units in cooperation with the University of Modena and the region of Reggio Emilia (Galeazzi, Elkins, & Curci, 2005), mental health professionals working in public and private practice within a defined geographical area were screened for harassment by patients. One third of staff were found to have been harassed in defined ways, and 11% were found to have been stalked without a strict operational definition. Clinicians were occasionally threatened, but physical attacks were rare. Most of the victims were nurses, but psychiatrists and psychologists also experienced extended periods of stalking. As with a recent study by McIvor and Petch (2006), the stalkers, most of whom had a diagnosis of psychosis or PD, tended to target staff who were directly involved in their care.
The above studies point to the stalking of clinicians as a salient and potentially damaging behaviour. In our experience, mental health practitioners who have been stalked by patients often are the recipients of judgmental rather than sympathetic responses from their colleagues, with accusations of incompetence in managing transference issues common in such cases (Anderson & West, 2011).
Stalker Characteristics
Stalkers do not tend to have normal psychological profiles, and by definition, those who target mental health professionals are more likely to suffer significant psychological difficulties. They tend to have difficulties in forming and maintaining interpersonal relationships and those who target clinicians may harbour unrealistic or misplaced expectations of intimacy arising from the normal therapeutic relationship. This is particularly so for incompetent-suitors stalkers and intimacy-seeking stalkers. For example, in the survey conducted by Galeazzi et al. (2005), the majority of mental health professionals reported the patient’s desire for more intimacy as the perceived motivation for their behaviour, together with feelings of anger for being abandoned once the therapeutic relationship was over.
Patients may be overtly psychotic, often borderline, and their delusional system and, not infrequently, substance misuse drives their stalking behaviour. Interestingly, also in this case, pure erotomania is rather rare (see, for example, Kienlen, Birmingham, Solberg, O’Regan, & Meloy, 1997). Not surprisingly, patients who stalk but are not psychotic, particularly those suffering from PD, display different motivations for their behaviour compared with erotomaniacs. Some scholars have suggested that “the common thread in such patients is a narcissistic drive that defends against humiliation in response to the more confrontational aspects of treatment, especially in-patient care or in cases of coercive care” (Meloy, 1999, cited in McIvor & Petch, 2006, p. 404). Projection of blame can be a potent motivation for stalking, particularly within the resentful stalker typology. Patients may develop a grudge for some perceived wrongdoing or dereliction of duty on the part of the health care worker, with complaints being made to hospital authorities and professional regulators.
Victim Factors
Scientific medical information is more widespread than in the past (e.g., Anderson & West, 2011; Galeazzi et al., 2005; Sansone & Sansone, 2010). Therefore, doctors and other mental health professionals are more likely to be blamed by dissatisfied or poorly informed patients who, rightly or wrongly, may complain about what they see as unusual handling of their therapy. The incidence of stalking of these professionals must be sought in the characteristics of their job, as they deal with emotional and psychological problems. Psychiatrists, psychologists, psychotherapists, family counselors, and social workers deal with delicate issues concerning life, distress, emotional problems of the patients and their families, who often also may suffer from psychopathological difficulties. Psychiatric patients frequently tend to “translate” their emotional disorder into obsessional behaviour that can extend beyond the call for care and comfort and lead to persistent and exhausting behaviour against caregivers. Given the close relationship that develops between the doctor and the patient, it is not always easy for the therapist to manage relation dynamics and the incongruous requests of the psychiatric patient, in particular the pharmacological treatment and the dynamics of the social and family relations of the patient. Similar situations are experienced in psychotherapeutic and psychoanalytic settings. Disappointed expectations and misbeliefs, but also bad management of therapeutic methods, can create anger and disappointment in the patients who may resort to acrimony and revenge.
Doctors and other health care professionals may develop a degree of tolerance to antisocial or threatening behaviour because of its prevalence in their everyday practice. As a result, they may minimize persistent harassment in the hope that it will resolve spontaneously or be managed within the therapeutic relationship. This perception may be reinforced by feelings of guilt or inadequacy concerning clinical practice, or concern at what colleagues might think. Moreover, because of the patient’s mental illness, in mental health care settings, there is often a reluctance to involve the police or criminal justice system in managing the problem.
It is important to emphasize that stalking can have a significant impact on the psychological, occupational, and social functioning of the person being stalked (Pathé & Mullen, 1997), even though the victim is a doctor and/or a mental health worker (supposedly knowledgeable about such reactions and their possible avoidance). For health care professionals, this can lead to increased stress, fear, helplessness, and disenchantment (Sandberg et al., 2002). Moreover, more overt psychiatric illness may develop, which can have an impact on the functioning of the health care service itself (Abrams & Robinson, 2011).
This Study
Although in Italy the stalking of women has been widely studied and monitored in the last few years, thanks to the work of counseling centres, monitoring centres, and associations for the protection of female victims of violence; the stalking of men, and especially of mental health care professionals, is still underestimated and underreported. In Italy, except for the study conducted on mental health care professionals by Galeazzi et al. (2005), no other studies have been conducted on this issue to analyze gender differences among the victims of stalking by patients who suffer from psychological disorders.
Two aspects are extremely important in assessing stalking by women: (a) among female stalkers, the choice of victims is closely related to the motivation for the stalking and (b) for almost one half of the stalkers, the stalking emerges from a desire to forge an intimate relationship with the victim.
The aim of this study was to examine gender differences among stalkers and between public and private psychiatric settings. For this reason, we examined stalking by women, with particular reference to mental health care settings and professionals, assessing differences between male and female stalkers and evaluating the stalking of psychiatrists working in public and private clinics, including psychiatric and psychotherapeutic practice. Because of the lack of literature data in this specific field, our study is obviously exploratory.
Method
We surveyed two groups of psychiatrists: those working in public clinics and those in private practice. An epidemiological assessment was conducted of all psychiatrists working in the Mental Healthcare Departments (DSM) of the Health Centres in the province of Rome. The 45 mental health centres in the province of Rome that are connected with DSMs belonging to 8 Local Health Centres were contacted. A total of 42 mental health centres agreed to participate. The 3 centres that did not participate gave no reason for not doing so.
The case material of the patients was drawn only from outpatient units, excluding those psychiatric units for severe cases only where patients are hospitalized until pharmacological stabilization is reached. These outpatient units of the DSM see patients on a long-term basis and use therapeutic and rehabilitation programs. Thus, the relationship between patients and caregivers is closer than the units with inpatients.
We collected data with the cooperation of those responsible for the services. Following our written request for voluntary support, data were collected with the consent of all persons surveyed, maintaining the anonymity of psychiatrists and patients. Data were collected from the beginning of April to November 30, 2011.
Other case material was drawn from psychiatrists working in private health centres, individual practices and associate practices, private clinics and/or clinics operating within the national health service, mental health care associations, and consulting offices for the treatment of mental disorders. This subgroup is comparable with the previous in terms of number of participants. As with the other survey, the identity of participants, victims, and perpetrators of the stalking and harassment was not disclosed.
Although the phenomenon of stalking is generically described as the malicious repetitive, almost persecutory harassment of another person (Meloy, 1997), there is no real agreement in international literature on a univocal definition of “stalking behaviour.” For this reason, we included in our study all the cases of multiple (not less than 10 episodes) harassing behaviours suffered by the victim for at least 6 months, excluding, therefore, cases of one-off harassment that could have been misinterpreted as stalking. The events had caused in the victims anxiety and distress, well-founded fear for their own or a loved one’s safety and a change in living habits. These are the criteria used in the Italian criminal code (Codice Penale, art. 612 bis) that defines and punishes threats and harassment related to the crime of stalking.
Participants
The participants ranged in age from 30 to 60 years. They were interviewed by the authors in their outpatients departments or offices (public and/or private). All the psychiatrists working in the province of Rome were asked to take part in the study and the majority agreed to be included in the sample. They were questioned about their age and gender, years of work in public or private settings, workplace, and the number of experienced harassing and stalking events. In addition, they were asked about the methods used by the stalker (telephone calls, text messages, emails, loitering, unwanted presents, surveillance in public, surveillance at work, unwanted visits at home, unwanted visits at work, indirect control by following, surveillance of car and/or front door, advertisements using the victim’s telephone number, baseless legal actions, any cyberstalking behaviours). The psychiatrists were asked about the types of experienced threats, possible experienced physical attacks, and damage to objects/property by the stalker. In addition, participants were asked about changes in lifestyle, possible change of workplace to escape stalking, psychological disorders caused by stalking, physical disorders caused by harassment, possible involvement of a third party in the stalking (“stalking by proxy”), and any legal actions taken against the stalker.
To ascertain the characteristics of the stalker, we asked the victims about the age of the patients at the beginning of stalking, the age at the end of stalking, the gender of the perpetrator, the duration of stalking (in months), the Axis I and/or Axis II diagnosis according to DSM-IV-TR criteria, any transfer of the patient to another professional, the medical measures taken for the patient (changes in pharmacological treatment, hospitalizations in mental health clinics following stalking behaviours), and the possible complaints to patients. Some information was also obtained by consulting the medical records of the patients. All the data were registered and assessed by the authors and subsequently reviewed by independent statisticians.
Results
Psychiatrists Working in Public Clinics
In total, 246 psychiatrists were surveyed (112 male, 134 female). Twenty-five cases of stalking were found in the sample (10.16% of the total). In 13 cases (5.28%), the victim of stalking was female (M age = 44 years) and in 12 cases (4.87%), the victim was male (M age = 47 years). The average number of years of work within the public mental health unit was 15.6 years for the female victims and 18 years for the male victims.
In nearly all cases, the methods of harassment were repeated telephone calls to the reception office of the outpatient unit and loitering near the workplace (18 cases out of 25, with equal rates between genders). Loitering near the victim’s house (3 cases, one male and two female perpetrators) and cyberstalking (2 cases, male perpetrators) were rare. In 5 cases, three men (12% of the victims) and two women (8% of the victims) experienced physical assaults.
The perpetrators of the stalking behaviours were almost evenly divided genderwise (13 males and 12 females). All stalkers pursued medical staff of the opposite sex. The mean age of male stalkers was 42 years, whereas the mean age of female stalkers was 38 years. The average duration of stalking was equivalent between groups (12 months).
Regarding the psychiatric status of the patients, six women had a diagnosis of PD (Cluster B traits, predominantly borderline in type) and six other women had a diagnosis of schizophrenic psychosis. Among the male stalkers, we found eight cases of paranoid schizophrenia, three cases of PD, and two cases of bipolar disorder during a period of excitement, part of the manic phase. In five cases (four men, one woman), the perpetrators were reported to the judicial authorities for stalking behaviour against their caregivers.
Psychiatrists in Private Practice
A total of 232 psychiatrists were surveyed (112 male and 120 female.) Forty-five cases of stalking were found in the sample (19.3% of the total). In 19 cases, the victim of stalking was female (8.15%) in 26 cases, the victim was male (11.18%), the mean age being 38.5 and 45 years, respectively.
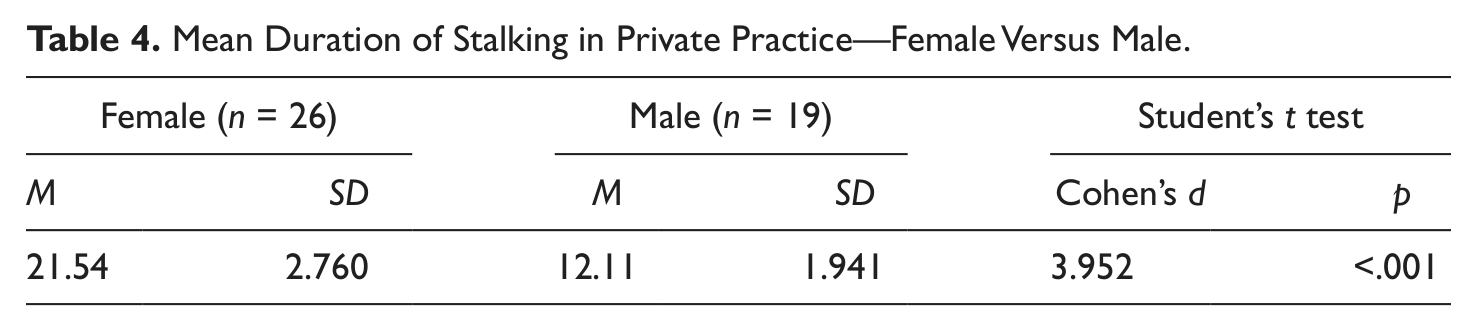
The average number of years of work of female and male victims was 11 and 15 years, respectively. Harassment and stalking methods were fairly constant and again similar to experiences reported in the media and in the literature but they were more varied compared with the previous sample. In nearly all cases, the methods of harassment were repeated telephone calls, text messages, and loitering near the workplace (38 cases out of 45, with equal rates between male and female). Loitering near the victim’s house (10 cases: 6 female, 4 male) and cyberstalking (11 cases: 5 male, 6 female) were less frequent. In 8 cases, 3 men (1.2%) and 5 women (2.14%) experienced physical assaults. The perpetrators of the stalking behaviours were 19 males and 26 females. All the stalkers pursued medical staff of the opposite gender. The mean age of the male stalkers was 42 years, whereas the mean age of female stalkers was 33 years. The average duration of stalking varied according to gender, averaging 21.54 months for women and 12.1 months for men.
Regarding the psychiatric status of the patients, 17 women had a diagnosis of PD (Mixed Cluster B traits, mainly borderline personality), 7 women had a diagnosis of schizophrenic psychosis and two of bipolar disorder (obsessive phase). Among the male patients, we found 7 cases of paranoid schizophrenia, 11 cases of PD, and 1 case of bipolar disorder during a period of excitement, part of the manic phase. In 13 cases (8 men, 5 women), the perpetrators were reported to the judicial authorities for stalking behaviours against their caregivers.
Comparison of Groups
We analyzed the data concerning the two groups and assessed the differences between them, with particular reference to the cases of patients who pursued their caregivers and the cases of the psychiatrists who were victims of stalking. We analyzed possible differences in the relationship between patients and psychiatrists working in private and public practice, and we assessed any possible repercussions relative to the number and type of stalking events. Important values and differences emerged from these analyses. We examined the differences in percentages between the two samples and their significance from a statistical point of view.
There were no significant differences between the groups with respect to gender. However, there was a large difference as to the number of stalking events: 45 cases were found in the sample of psychiatrists working in private practice as opposed to 25 cases found in the sample of psychiatrists working in public clinics. The cases of stalking recorded in private mental health settings (19.3%) outnumbered those reported in public settings (10.2%). As to the distribution/rates of stalking among the two genders, the number of male (19-13) and female (26-12) stalkers was higher in the subgroup of mental health professionals working in private practice.
We assessed the ratio between male stalker/private patient (i.e., a patient referring to a private clinic) and male stalker/public patient (i.e., a patient referring to a public clinic), and the ratio between female stalker/private patient and female stalker/public patient. From a statistical point of view (=0.0109), we found that the percentage of female stalkers was higher in private mental health settings (11.2%) than in public settings (4.9%), whereas no considerable difference was found in the two settings as to the percentage of male stalkers. Female stalkers in the group of private patients were more likely to suffer from a PD than those in the group of public centre patients. This difference in the two groups is statistically important (n = 0.01). The frequency of stalking committed by men and women within the same sample was assessed. Male stalkers slightly outnumbered female stalkers in the subgroup of public patients and female stalkers clearly outnumbered male stalkers in the subgroup of private patients (see Table 1 and Figure 1).
Comparison Between Patients Who Stalk Private Psychiatrist and Public Health Service Psychiatrist (Percentages).
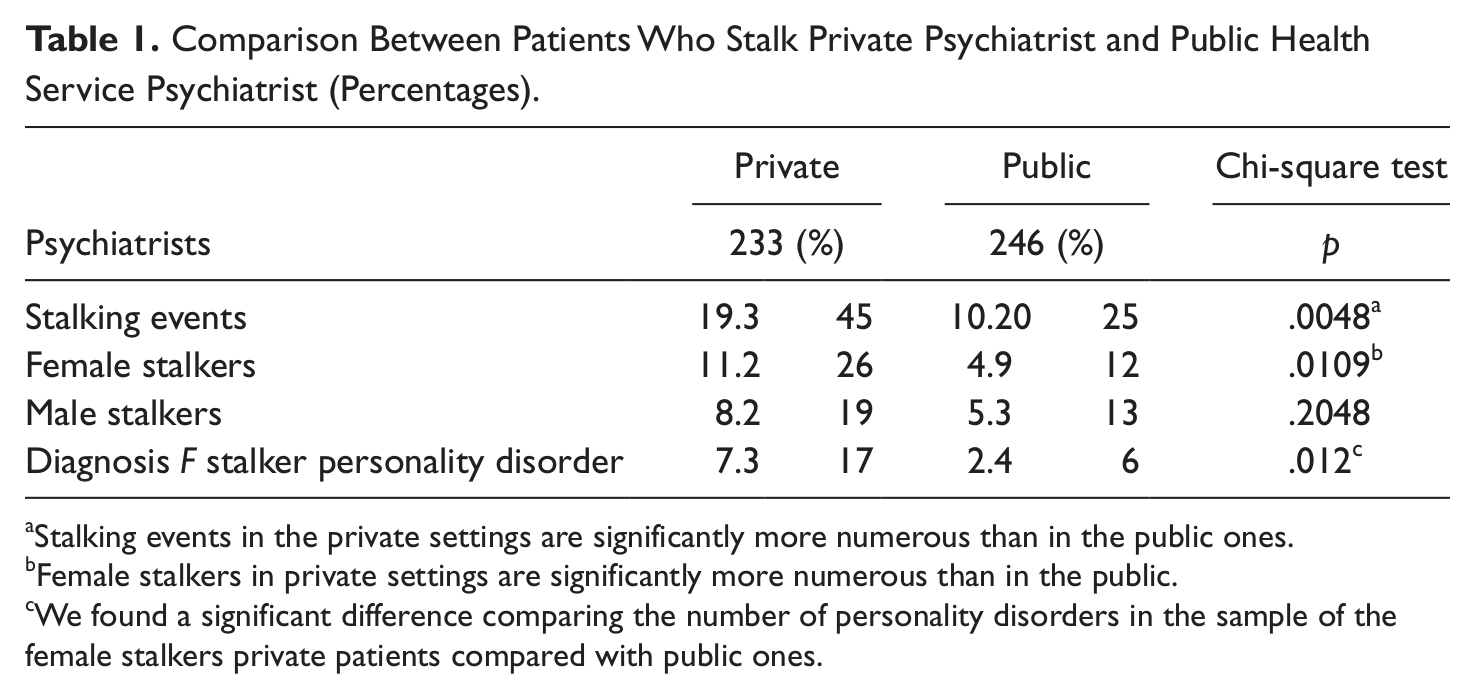
Stalking events in the private settings are significantly more numerous than in the public ones.
Female stalkers in private settings are significantly more numerous than in the public.
We found a significant difference comparing the number of personality disorders in the sample of the female stalkers private patients compared with public ones.
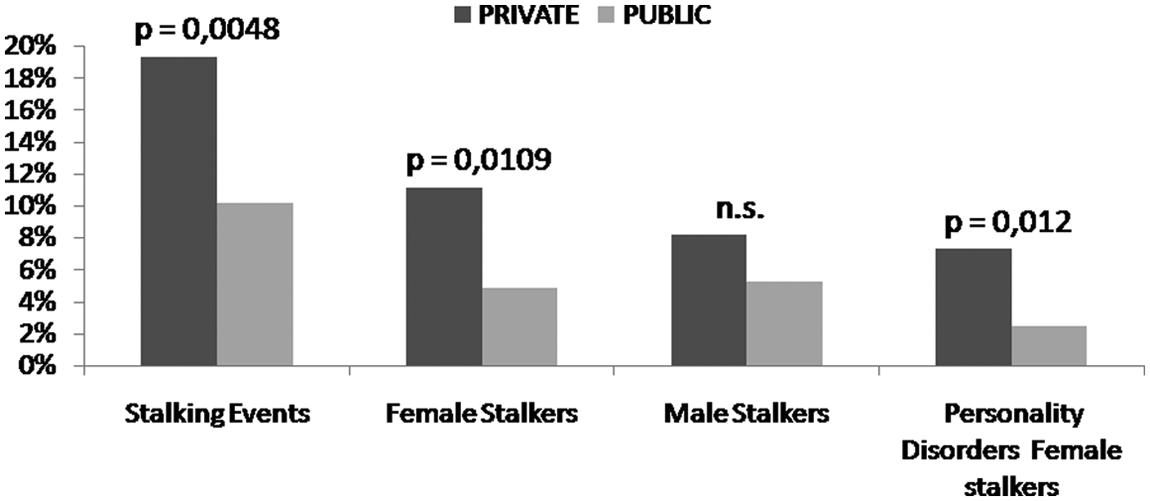
Stalking of psychiatrists: Comparison between private and public health services patients.
The mean age of stalkers in the two groups was compared. The significance of the differences found in the samples and the homogeneity of the variance of age in both groups was verified using Cohen’s d effect size. The mean ages were comparable only when the distribution was not too wide; that is, when standard deviations did not differ too much from the mean (otherwise, this assessment would not be significant). Homogeneity was tested in all the following assessments.
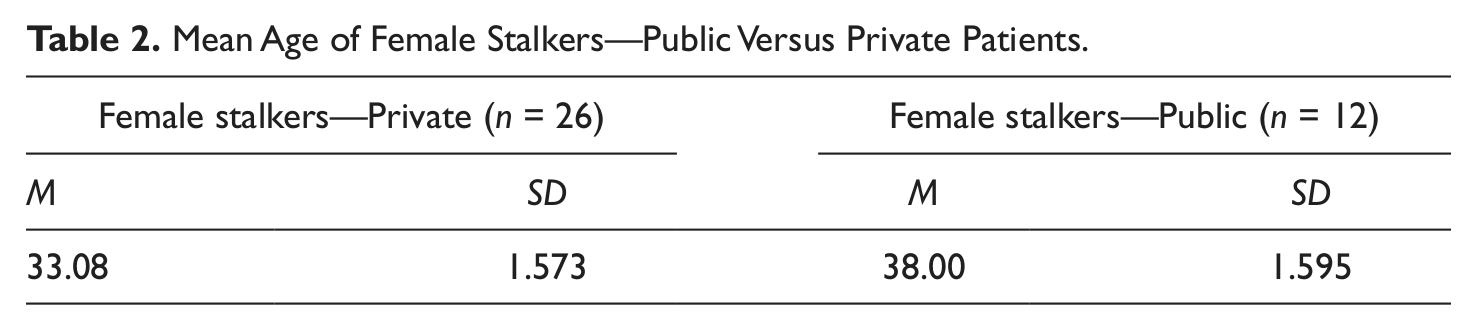
Although there were no substantial differences between the two samples of male stalkers, female stalkers in the group of private patients were much younger than those in the group of public patients (average 33.08 vs. 38.00; see Table 2).
Mean Age of Female Stalkers—Public Versus Private Patients.
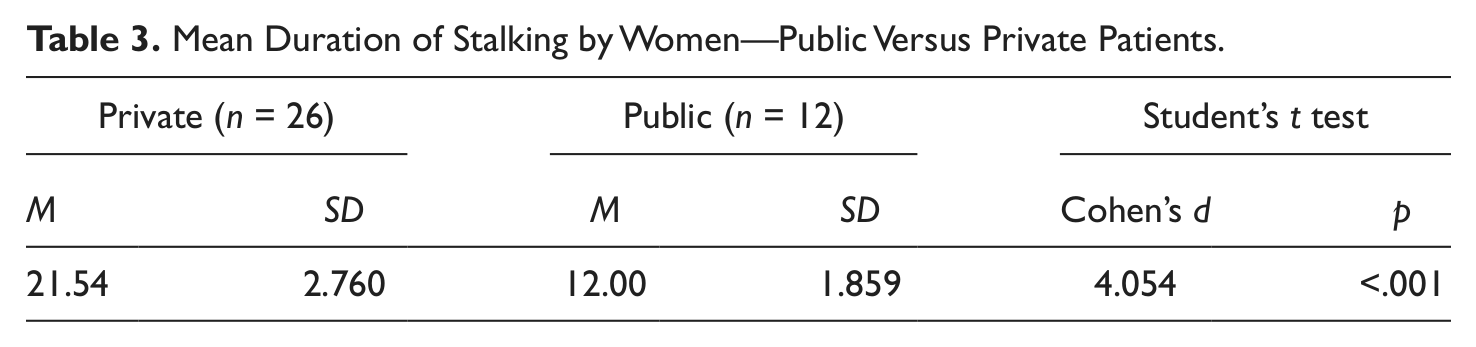
As to the mean duration of stalking, we found that female stalkers in the group of private patients pursued their victims for a longer period than those in the group of public patients (M 21.54 vs. 12 months). The difference was statistically significant (see Table 3).
Mean Duration of Stalking by Women—Public Versus Private Patients.
In the group of private patients, female stalkers pursued their victims for a longer period compared with their male counterparts as shown in Table 4.
Mean Duration of Stalking in Private Practice—Female Versus Male.
The percentage distribution of diagnoses made on patient stalkers in both groups, according to DSM-IV-TR criteria, was also assessed. The majority of the stalkers in the group of private patients suffered from PDs, especially the women, as reported above (PD women 65%, men 57%). In the group of the public service patients, the frequency rate of psychotic and PDs was equal in women and higher in men (psychosis = 61.5%, PD = 23%). The findings are summarized in Figures 2 and 3.
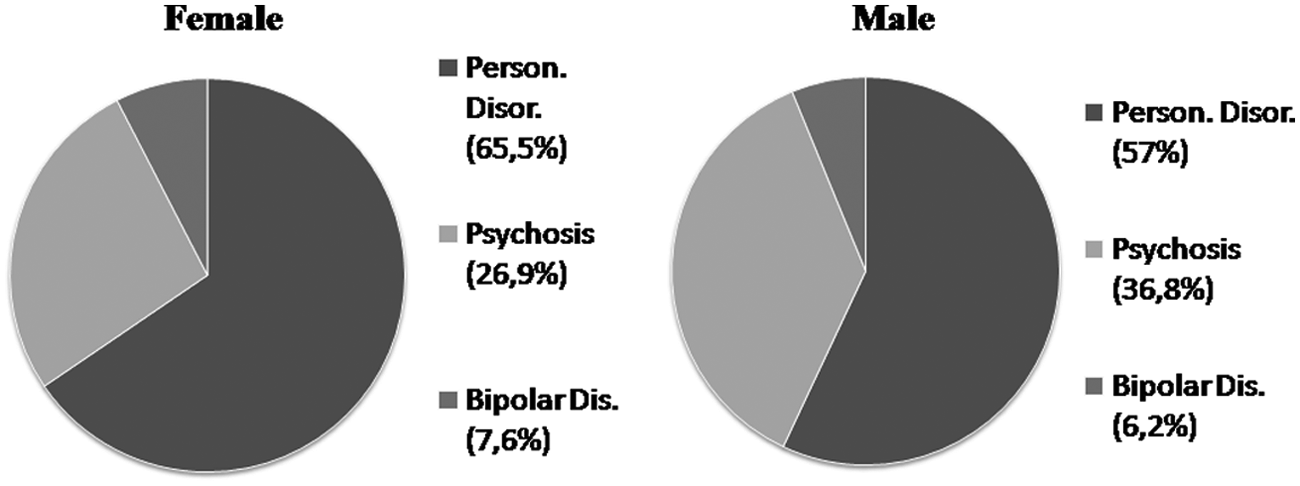
Stalker diagnosis Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision; DSM-IV-TR)—Private patients.
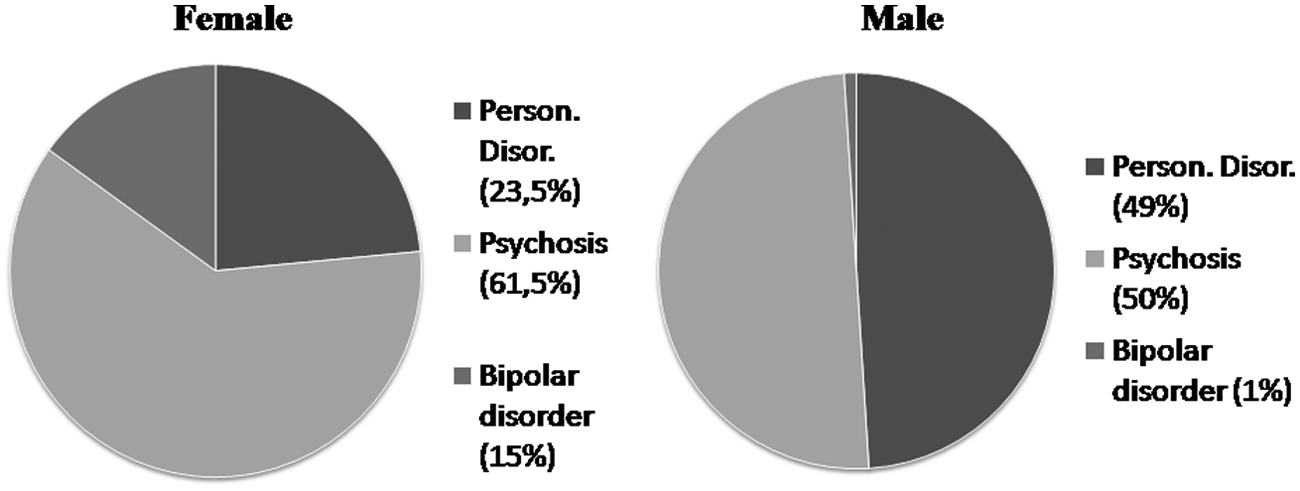
Stalker diagnosis Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision; DSM–IV-TR)—Public patients.
Female stalkers were more likely to target men who are older than they are, in public and private practice, whereas men referred to private practice were more likely to pursue younger women. (This difference can be assessed with a simple arithmetic comparison, but it is not statistically important.) As to the other assessed variables, we found no important differences between the two subgroups and the two genders within the same subgroup.
It should be noted that in Italy, medical doctors who work in public health facilities can also work in their own private practice or in hospitals; therefore, the same psychiatrist might be the victim of stalking in both the public and private practice. This would represent a disturbance factor in statistical assessments. However, in the present study, we found no cases of this kind. Nor did we find cases of stalking of psychiatrists by same-gender patients.
Discussion
In the general population, the majority of victims of stalking are women. Both the literature and the media clearly demonstrate that they are more likely to be at risk of violent and aggressive behaviour, which can even result in homicide. As a result of these findings, many centres for female victims of harassment have been set up in Italy, and greater attention is being given to this phenomenon. It is also true that the stalking of men is an underestimated and sometimes even underrecognised phenomenon. A deeper knowledge and better awareness of this phenomenon are therefore extremely necessary considering that, as shown in literature (Kuehner et al., 2012), men have the same psychopathological symptomatology as do women and that the impact of stalking on men is usually underestimated.
Although health care professionals are at higher risk of being stalked than the general population, clinicians, especially in Italy, receive little training on the concept of stalking and its management, as demonstrated in the study of Modena Group on Stalking (2005). Despite increasing emphasis on risk assessment in relation to suicide, violence and homicide, explicit awareness of stalking remains limited.
The stalking behaviour of psychiatric patients is motivated by specific symptoms (including obsessional thoughts, impulse dyscontrol, intolerance to frustration), by patients’ inaccurate beliefs, and by misplaced expectations about treatment, which may lead to resentment for what they perceive as improper behaviour toward them or inappropriate treatment.
The stalking of mental health care professionals has been widely reported in the international literature, but the importance of gender differences and the impact of therapeutic settings (public or private) on the incidence of the phenomenon seem to have been underestimated. The aim of the present study was to fill this gap by evaluating the stalking of psychiatrists working in public and private clinics, as those in psychiatric and psychotherapeutic practice, and assessing differences between male and female stalkers.
One limitation of the data presented is that the study is an exploratory assessment based on epidemiological reports. Nevertheless, it clearly shows that, at least in Italy, psychiatrists working in public practice are at lower risk of being stalked than their colleagues working in private practice. The study found that the incidence of stalking events in public mental health units and other health care units is equal, the lifetime percentage of stalking of the public centre doctors being 10%, whereas it is almost twice as much in private practice.
This difference is most likely due to various aspects that differentiate psychiatric outpatient activity in public mental health units from private practice in Italy. First, there is better-screened communication within the public Mental Health Units. For example, patients rarely know the telephone number of their doctor because their calls are screened by the secretarial staff, operators, nurses, or administration personnel. Second, in the public services, it is easier to refer patients to colleagues working in the same unit in case of problems or conflictual relationships. Moreover, a colleague’s problem with a patient is often considered to be a problem of the entire unit. Finally, there is a less personalized relationship between patients and doctors: Patients who are referred to the DSM (public mental health department) consider themselves as patients of the centre rather than of a single psychiatrist in private practice. They are mostly chronic psychiatric patients who easily move from one doctor to another because medical doctors might change workplace or have a different schedule and are more used to changing doctor than are private patients. Therefore, doctors working in public practice seem to be more “protected” than their colleagues working in private practice who have a more individual relationship with patients and are more likely to be approached directly by them, for instance by phone. (Psychiatrists or psychotherapists who have their own private practice usually give patients their address and personal phone number.)
In the cases examined in this study, we found that the rate of stalking activities was equivalent between genders, and that in the sample of private patients, the perpetrators were mostly women. This is in contrast with what has been reported in other populations of stalkers where the number of male stalkers may be 4 times higher than that of female stalkers. This finding could be justified by the fact that, especially in private practice, women are more likely to turn to psychiatrists and psychoanalysts than men. Moreover women tend to pursue professionals and someone previously known to them with whom they had personal contacts (see, for example, Englebrecht & Reyns, 2011; Purcell et al., 2001; West & Friedman, 2008).
Men and women used the same harassment methods in both groups. The number of physical assaults was lower than expected, but was almost equivalent between subsamples. However, stalkers mostly targeted individuals of the opposite sex.
The analysis of stalking in private practice showed that health care professionals working in private practice are at twice the risk of being stalked than their colleagues working in public practice. Male psychiatrists and psychotherapists were the preferred victims of stalkers in this group, contrary to what has been reported in the literature and to what was observed in the other sample in which male stalkers were outnumbered by female stalkers. In the above-mentioned group, female stalkers were more numerous and they also outnumbered male patients in their own subsample. Female stalkers tended to pursue private caregivers for a longer period of time than female patients in public practice. The female stalkers turning to psychiatrists working in private practice were much younger than those in the other group. There were no differences between the two groups as to the age of male stalkers and of the victims (male and female).
Similar to what is reported in the literature (e.g., Dressing & Gass, 2010; Spitzberg & Veksler, 2007), in this study, there is a prevalence of PD, Cluster B type according to DSM-IV-TR (American Psychiatric Association, 2000) criteria (especially borderline PD) diagnosed in women, more precisely in female stalkers who pursued their therapists. The rate of psychotic disorders (erotomania included) and PDs diagnosed in the male population is more balanced, with a prevalence of psychosis in the subsample of patients of the psychiatrists in public practice. It can be theorized that this is due to the difference between the patients reporting to public health care facilities and those reporting to private facilities, who may belong to a higher social and economic class.
From these assessments, a preliminary picture can be drawn of the woman who harasses and stalks her therapist. She is a young woman with emotional and personality problems who tends to dramatize, seduce, and manipulate and who cannot control her impulses. She has past experiences of abandonment and violence and tends to forge a relationship with her therapist, misinterpreting his professional concern and empathy, which may be misconstrued as romantic or even sexual interest (Lewis, Fremouw, Del Ben, & Farr, 2001). When this delusion is frustrated by the therapist’s behaviour, uncontrolled emotional reactions arise as a consequence of the distorted traits of personality. If the patient has no ego strength to handle this delusion, she begins to alternate seduction (“I will make you change your mind”) with anger (“I cannot be rejected again”) or even revenge (“You deceived me, you will pay for this”). The more incongruous her analysis of reality, the more aggressive and frequent her behaviours are.
The literature and the present study demonstrate that “stalking by women,” especially stalking of psychiatrists, is an underestimated and underresearched phenomenon. This is a particularly worrying problem in private practice where, although women, and especially men, are at higher risk of being stalked than those working in the public arena, awareness of stalking remains limited. It is therefore necessary to increase such awareness through seminars, conferences, and information campaigns, which should involve mental health staff working in the public and private sectors. In addition, administrative and clinical policies on harassment and stalking by patients should be developed and enforced in the workplace to ensure prompt intervention and better protection of health care professionals.
There are no clear guidelines on how to deal with persistent harassers, probably because it is a complex phenomenon and because patients have few or no reasons to change their behaviour. To minimize the risk of being stalked, when screening patients, psychotherapists should collect detailed information on specific topics with each patient (family of origin, psychological and psychopathological profile, school and work experiences, present life). Therapists should also assess the phenomenon from different points of view, that is, collecting and processing data on the patient focusing on the four areas of analysis which are closely related to the dynamic of stalking (biological, emotional, cognitive, and behavioural). They should make an in-depth psychodiagnosis aimed at outlining the psychobehavioural profile of the patient with appropriate means (talks, interviews, questionnaires, tests).
Considering the specific characteristics of stalking and the behaviour of patients who try to establish an intimate relationship with their psychotherapist, especially of the opposite sex, mental health professionals should stress, in a respectful but firm way, what the borders of the therapeutic relationship are. They should be concerned about their privacy, inform their colleagues about stalking events of which they have been a victim, consider transferring patients who stalk or harass to other colleagues, and, when necessary, consider taking legal action. Understandably, therapists are reluctant to take legal action against patients, as their criminal conduct may be closely related to their pathology; however, in extreme cases, it may be necessary. Risk management strategies should be promoted. Interventions such as targeted family counseling may be necessary, as most stalkers have a history of domestic violence (Kurt, 1995).
The authors agree with other researchers on this topic (e.g., Abrams & Robinson, 1998) that the phenomenon of stalking can be controlled only by adopting a comprehensive and integrated approach to the stalking patients. Such an approach should include psychotherapy, psychiatric pharmacotherapy, practical measures for handling the patients as mentioned above, but above all a more complete information exchange and efforts to increase awareness of the problem among psychiatrists and other mental health professionals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.