
Abstract
A significant number of prisoners experience mental health problems, and adequate social support is one way that facilitates better mental health. Yet, by being incarcerated, social support, particularly family support, is likely to be strained or even negative. In this study, we examine whether familial support—either positive or negative—in-prison and after release affects mental health outcomes post-release. Using the Serious and Violent Offender Reentry Initiative (SVORI) dataset, we regress post-release mental health on in-prison familial support, post-incarceration familial support, and changes in familial support. We find that while in-prison family support does not affect mental health, post-release familial support does. Also, experiencing an increase in negative familial support is associated with lower post-incarceration mental health. We conclude with a discussion of policies which may facilitate better familial support environments.
Introduction
A growing literature discusses the consequences of incarceration for both physical and mental health, leaving no doubt that incarcerated individuals have significantly more health problems than the general population (Dumont, Brockmann, Dickman, Alexander, & Rich, 2012). Given the link between mental health issues and the increased likelihood of re-incarceration, of particular concern is the mental health of former prisoners (Baillargeon, Binswanger, Penn, Williams, & Murray, 2009; Baillargeon et al., 2010). A significant number of prisoners experience mental health problems (Fazel & Lubbe, 2005; Freudenberg, 2001; Freudenberg, Daniels, Crum, Perkins, & Richie, 2005; Mallik-Kane & Visher, 2008), with some studies reporting that between 15% and 26% of former prisoners having been diagnosed with a mental health problem (Ditton, 1999; Wilper et al., 2009). Currently, prisons are the largest institution housing the mentally ill (Dumont et al., 2012; Freudenberg, 2001; Torrey, 1995).
The current era of mass incarceration and re-entry compounds the problem of mental health issues among former prisoners (Schnittker, 2014). More than 700,000 individuals leave prison each year (West & Sabol, 2008); nearly 50% of whom will be re-incarcerated within 3 years (Langan & Levin, 2002). Individuals entering prison tend to have more health problems than the general population and often leave with those health problems exacerbated (Wakefield & Uggen, 2010). With large numbers of individuals returning to the society, families, neighborhoods, and the criminal justice system are not likely prepared for or capable of handling the mental health needs of these individuals. While in the past, parole officers’ roles were aimed at assisting in successful re-entry, nowadays their primary role is to monitor returning prisoners (Clear, 2007), not to facilitate former prisoners receiving mental health care. As such, returning prisoners lean more readily on family, friends, and neighborhood resources to stay crime free and reintegrate into society (Clear, 2007). Unfortunately, incarcerated individuals are likely to strain these integral sources of support, leaving family and friends in a poor position to assist in positive re-entry outcomes, such as good mental health (Clear, 2007; Comfort, 2009; Harris, Evans, & Beckett, 2010). Therefore, understanding whether the mental health of former prisoners affects their successful re-entry is an important undertaking for public health officials and the criminal justice system.
Our study seeks to explore how family support—both while incarcerated and post-release—is related to mental health. To examine whether social support affects mental health outcomes, we use a unique dataset which studies serious and violent offenders during their time in prison and after release. We do this by examining the Serious and Violent Offender Reentry Initiative (SVORI) dataset which studies ex-prisoners’ relationships with their families, as well as the changes that support from pre-release to several months following re-entry. By studying these offenders at two different periods, we are able to assess their mental health progression post-release and whether the familial social support factors were associated with any changes, controlling for pre-release levels of mental health.
Social Support, Mental Health, and Returning Prisoners
Social support refers to the actual or perceived emotional, informational, or practical aid that is received from others, particularly significant others, family members, and friends (Thoits, 1995). Over the past few decades, substantial evidence has found that social support has both causal and collateral effects on a plethora of physical and mental health outcomes, though the psychosocial mechanisms at work are interconnected and complex (Cohen & Wills, 1985; Silver & Teasdale, 2005; Thoits, 1995; Travis, 2005; Uchino, 2004; Uchino, Cacioppo, & Kiecolt-Glaser, 1996; Umberson & Montez, 2010). Specifically, social support may enhance the quality of mental health directly by fostering a sense of purpose in life or indirectly by attaching symbolic meaning to responsibility and promoting a sense of personal control (Thoits, 1995; Umberson & Montez, 2010). Strong social ties have been found to protect individuals from a myriad of mental health problems ranging from mild depression to suicide (Thoits, 1995). In addition, social support has been found not only to increase the rates of recovery from mental illness but also decrease the likelihood of onset as well (Uchino et al., 1996).
Studies examining the relationship between social support and personal health consider two primary models: the main effects model and the stress-buffering model (Cohen & Wills, 1985). The main effects model posits that those with strong social support have better overall health than those with weak social support, net of exposure to life stressors. The buffering, or indirect, model posits that those who have strong social support are in better positions to combat chronic stressors or negative life events. In addition, strong social ties better attenuate the stress response and strengthen a person’s perceived ability to reduce or eliminate psychological damage in the future (Cohen & Wills, 1985; Thoits, 1995). Consistent with both models of social support, the majority of empirical research concurs that perceived emotional support by loved ones buffers the physical and mental detrimental outcomes related to enduring strains and adverse events (Cohen & Wills, 1985; Thoits, 1995; Uchino et al., 1996). In addition, the presence of a confidant has been found to be an influential, yet easily accessible, measure of emotional support and significantly reduces psychological damaging effects (Cohen & Wills, 1985; Thoits, 1995; Uchino et al., 1996).
For former prisoners, social support is vital to both their success in the community and their mental health, yet their ability to obtain social support is compromised. Imprisonment has long been acknowledged as an acute stressor (Schnittker, 2014; Schnittker, Massoglia, & Uggen, 2012), making social support an important buffering mechanism for the negative health impacts prison may have on mental health (Visher & Travis, 2011). It is common for ex-prisoners to be homeless or marginally housed (Dumont et al., 2012; Fleisher & Decker, 2001); however, a strong social network can provide an ex-prisoner a place to stay until they can get back on their feet. Indeed, the vast majority of prisoners report staying with family or friends post-release (Visher, 2010; Visher & Travis, 2011). Therefore, this kind of support decreases the chances of homelessness and potential recidivism (Fleisher & Decker, 2001).
However, a support system is hard to come by in prison. Both current and former prisoners have little social and familial capital (Clear, 2007). While incarcerated, prisoners are unable to form and keep relationships that often lead to high stress and a state of depression (Wakefield & Uggen, 2010). With very fragile social networks prior to incarceration, prisoners seldom have the support needed for readjustment and reintegration into their communities (Clear, 2007). In addition, this reintegration is made even more difficult by the ex-prisoner’s attempt to end the relationships they previously had with crime and rekindle the relationships that were stressed by their removal from their communities (Clear, 2007).
One reason for the stressed relationships is the difficulty that family and friends face in contacting prisoners; indeed “incarceration imposes its own financial strains on families wishing to maintain contact with the incarcerated” (Dumont et al., 2012, p. 332). Inmates are often from poor urban areas; however, prisons are usually located in rural areas (King, Mauer, & Huling, 2004; Lynch & Sabol, 2004). Throughout the duration of a prison sentence, families and friends have trouble traveling the distance to visit their loved ones, and relationships eventually wane (Lopoo & Western, 2005; Massoglia & Warner, 2011). Given that most prisoners come from low socioeconomic status neighborhoods, maintaining healthy familial relationships and support with an imprisoned loved one is likely very difficult and expensive (Clear, 2007; Wakefield & Uggen, 2010). For instance, prisons may make arrangements with local phone service providers to charge substantially more money for collect calls made from the facility (Dumont et al., 2012). In New York, a charter service to a local prison costs approximately US$40 round trip and takes more than 8 hr to arrive, costing families valuable time and resources (Christian, 2005). One study shows that poor women spend approximately one third of their income staying in contact with an incarcerated partner (Grinstead, Faigeles, Bancroft, & Zack, 2001). Furthermore, the families of prisoners often hold the burden of debt for their incarcerated loved one (Harris et al., 2010). Collectively, these familial issues make social support during and after prison strained (Comfort, 2009; Wakefield & Uggen, 2010).
Though visiting loved ones in prison may be burdensome on families, research has found that maintaining visits improves the inmate’s institutional behavior, reduces the likelihood of recidivism and parole violations upon release, and enhances social support networks (Bales & Mears, 2008; Duwe & Clark, 2011). In a recent study examining presence and frequency of visitation, Duwe and Clark (2011) found that any visitation reduced the risk of recidivism by 13% and reduced the risk of technical violations by 25% after release. In addition, the findings suggest that when the visits were more frequent, closer to release date, and involved a variety of friends and family members, recidivism risk was further lowered (Duwe & Clark, 2011; Jacoby & Kozie-Peak, 1997). Similarly, in a longitudinal study of mentally ill offenders released into the community, the level and maintenance of visitation in prison and social support pre- and post-release was positively associated with an enhanced quality of life and negatively associated with the number of problems the ex-offender dealt with on a daily basis (Jacoby & Kozie-Peak, 1997). Other research have suggested that visitation may reduce prisoners’ overall stress and psychological anxiety felt in overcrowded prisons by producing a sense of personal space and a connection to the outside world through their visitors (Wooldredge, 1997). Associating with others or believing that others have a stake in their well-being helps the prisoners cope while incarcerated and provides mental strength post-release (Jacoby & Kozie-Peak, 1997; Wooldredge, 1997).
Mental health of prisoners and ex-prisoners is influenced by social factors as well. Typically, people who are incarcerated tend to be disadvantaged; consequently, prisoners often have a variety of health care needs (Mallik-Kane & Visher, 2008; Wakefield & Uggen, 2010). Furthermore, despite that it is a constitutional right, health care in prison tends to be inadequate (Travis, 2005; Wakefield & Uggen, 2010). When asked, more than half of prisoners described medical treatment as one of their primary re-entry needs (Visher & Travis, 2011). With a support system in place upon release, ex-prisoners have a better chance at reducing their risk of recidivism and acquiring some of these health care items they mentioned a need for.
Though recidivism is a concern for all ex-prisoners, inmates with mental health issues are more likely to have a violent criminal history than their healthy counterparts (James & Glaze, 2006; Silver & Teasdale, 2005). In addition, 47% of mentally impaired repeat offenders recidivated violently, and approximately 25% of them had served three prior incarcerations (James & Glaze, 2006). Silver and Teasdale (2005) concluded that the relationship between mental disorder and violence diminished considerably when stressors and impaired or negative social support were controlled for, showing the imperative nature for social support.
Indeed, research demonstrates the effective nature of social support in facilitating positive re-entry outcomes. Positive familial support has been found to lower recidivism rates for recently released inmates, net of other recidivating factors (Brown, Amand, & Zamble, 2009; Spjeldnes, Jung, Maguire, & Yamatani, 2012). Likewise, informal social support has been found to increase the likelihood of successful re-entry for those with co-occurring mental health disorders and substance abuse (Brown et al., 2009). Because the vast majority of inmates are eventually released into society and structured community-based services for mental health are limited and subject to change (Wallace & Papachristos, 2014), post-release social support from families is crucial in the desistance process of mentally ill offenders (James & Glaze, 2006; Spjeldnes et al., 2012).
Current Study
While the stressors of prison stem from social isolation and violence, reintegration poses different, yet equally challenging, hardships for former prisoners. Post-release, ex-prisoners continue to be at risk for physical and mental health illnesses. One such hardship is reintegrating with family and friends and garnering social support at a time when former prisoners have been separate from family for extended periods of time. Our study seeks to explore how family support—both while incarcerated and post-release—is related to post-release mental health. We do this by examining the SVORI dataset which surveyed serious offenders regarding their familial and social backgrounds while in prison and for several months post-release. We capitalize on SVORI’s multi-wave structure which enables us to establish levels of familial emotional support for the respondents during incarceration and 9 months after release. As such, we can examine how familial emotional support—both positive and negative—changes upon release and how this affects mental health post-release.
From a policy perspective, this study is important given that social support is mutable. Social support is something that can be increased during incarceration through simple policy changes, such as longer visitation times, more privacy during visitation, relocating prisoners closer to family whenever possible, and lowering the cost of family visits. In the United States today, policies related to family visitation are designed by state prison administrators rather than by national guidelines. As such, policies aimed at building family support for prisoners can be implemented at the state or national level.
Method
Data
This study employs two waves from the adult male sample of the SVORI dataset. SVORI is a federally funded initiative aimed at enabling states to develop programs intended to ease former prisoners’ transition from prison to community and better re-entry outcomes (Visher & Travis, 2011). The data collection effort for SVORI involved interviewing subjects and collecting detailed information on the facilities subjects were incarcerated at from 12 different programs within prisons in 14 different sites across the nation (Lattimore & Visher, 2009; Visher & Travis, 2011). Before data collection began, the initiative narrowed down possible impact sites based on the ability to implement the program, the size of the target population, the availability of a comparison group, and the willingness of subjects to participate. Then recruitment began with letters, telephone contacts, and site visits (Lattimore & Visher, 2009).
In-person interviews with subjects were conducted 1 month before release from prison, and 3, 9, and 15 months after release. For this study, we were interested in Waves 1 and 3, which correspond to in-person interviews conducted 1 month before release and 9 months post-release. Each interview lasted approximately 1.5 hours. The first interview was used to document the experiences the ex-prisoner underwent during incarceration, their plans upon release, and their physical and mental health. The follow-up interviews were used to document post-incarceration relationships, connections and experiences, such as employment, family, health, and crime, and delinquency (Lattimore & Visher, 2009). Compensation was given to those that attended the follow-up interviews. There was a significant loss of respondents to attrition between pre-release and 9 months post-release. The initial sample had 1,697 adult males, while the Wave 3 sample included 1,035 adult males, only 70% of the original Wave 1 sample (Lattimore & Visher, 2009). Individuals who were re-incarcerated before 9 months were not included in our models simply because they are likely to be different in both their mental health and familial support than those individuals who are not incarcerated. As a result, after cleaning and excluding the individuals who were re-incarcerated at Wave 3, our final sample size was 550.
Dependent Variable
The dependent variable for the analysis was the SF-12 Summary Mental Health Scale (MHS; Ware, Kosinski, & Keller, 1996). The SF-12 MHS is a shorter version of the SF-36 MHS and captures elements of psychological well-being and distress, social and role functioning, and overall vitality (Ware et al., 1996). The MHS scores are weighted averages of item responses, so that 50 represents the mean with a standard deviation of 10 (see Ware et al., 1996, for more details on scoring and scale construction). The MHS was given to the ex-prisoners at Wave 1 and Wave 3. The MHS is coded so that higher scores mean better mental health while lower scores equate to poorer mental health. The MHS was standardized in our models.
Independent Variables
We included several independent variables in the analysis. In general, “social support is usually defined as the existence or availability of people on whom we can rely, people who let us know that they care about, value, and love us” (Sarason, Levine, Basham, & Sarason, 1983). We capture these elements of social support—both positive and negative—in two scales. First, we included a measure of positive familial social support for Wave 1 and Wave 3. The positive familial support variable is a factor variable made from six questions—the same across waves—including “I feel close to my family,” “I want my family involved in my life,” “I have someone in my family to talk to about problems,” “I have someone in my family to turn to for suggestions,” “I have someone in my family who understands my problems,” and “I have someone in my family to love me.” These six items were factored using principal components analysis. For Wave 1, one factor emerged with an Eigenvalue of 3.67 and factor loadings ranging from 0.67 to 0.86. The factor for Wave 3 is similar with an Eigenvalue of 3.98 and factor loadings ranging from 0.65 to 0.9. Both factors were then standardized. Here, higher scores on the positive family support variables mean higher levels of positive familial social support.
We also included a measure of negative familial social support for Wave 1 and Wave 3. Negative familial social support is meant to capture if former prisoners do not feel that they are loved or valued (Sarason et al., 1983). The negative family support variable consists of the following three questions: “I fight a lot with family members,” “I often feel like I disappoint my family,” and “I am criticized a lot by my family.” For Wave 1, one negative family support factor emerged with an Eigenvalue of 1.6 and factor loadings ranging from 0.66 to 0.8. Similarly, for Wave 3, one negative family support factor emerged with an Eigenvalue of 1.88 and factor loadings ranging from 0.76 to 0.84. Both factors were then standardized. Higher levels on the negative family support variables equate to higher levels of negative emotional support or a more noxious familial environment.
We also created two variables that estimate change in either positive or negative family support across the waves. These two measures, Positive Family Support Change and Negative Family Support Change, were constructed by subtracting a respondent’s Wave 1 score of either positive or negative family support from their Wave 3 score of either positive or negative family support. Here, a positive score means a gain in that type of family support while a negative score means a loss in that type of family support.
We included several controls in our analyses. First, we included a dummy variable indicating whether the ex-prisoner currently (Wave 3) reported having any chronic illnesses. They were given a 1 on the chronic illness variable if they indicated having any of the following: asthma, diabetes, heart problems, arthritis, back problems, tuberculosis, HIV/AIDS, and hepatitis B or C. We also include four other health-related variables that are likely to account for mental health issues. Needs Health Care is a dummy variable signaling that the ex-prisoner currently needs and does not have health care post-release. Needs Mental Health Care is also a dummy variable signaling that the ex-prisoner currently needs and does not have mental health care post-release. Needs Drug/Alcohol Treatment is a dummy variable signaling that the ex-prisoner currently needs and does not have drug or alcohol addiction treatment post-release. Has Insurance is a dummy variable designating that the respondent has health insurance.
We also included variables that would account for the respondents’ contact with their family while they were in prison. Mail in Prison is a categorical variable regarding the frequency at which the respondent reported receiving mail from family members while in prison with 0 representing only a few times or never, 1 representing monthly mail, and 2 representing receiving weekly or daily mail. Similarly, Phone Contact in Prison is a categorical variable regarding the frequency at which the respondent reported having phone contact with family members in prison with 0 representing only a few times or never, 1 representing monthly phone calls, and 2 representing weekly or daily phone calls. Finally, Visitation in Prison is a categorical variable regarding the frequency of family visitation in prison with 0 representing only a few times or never, 1 representing monthly, and 2 representing weekly or daily.
Next, we included the ex-prisoner’s age in years which is grand mean centered. We also included a dummy variable signaling if the ex-prisoner had only been incarcerated once (First-Time Offender); we view this control as important given that the negative health consequences of prison may be cumulative and that mental health issues may be more significant for those who are experiencing their first incarceration. Also included are dummy variables signaling whether the ex-prisoner is Black or of Other race. Currently in Relationship or Married is a dummy variable demonstrating that post-release, the former prisoner is in a serious relationship or married. We also include a battery of dummy variables showing who the respondent currently lives with; living alone is the reference category. There variables include Lives With Partner (this includes spouses and significant others), Lives With Family Member (such as an aunt/uncle, cousin, or grandparents), Lives With Parents (this includes step-parents), Lives With Their Children, and Lives With Other. We included a variable regarding whether the respondent felt their current living is better than before. Housing Situation Better Than Before is a categorical variable where 0 signals their housing situation is worse, where 1 signals it was about the same and 2 signals it was better than their previous living situation. Finally, we include a dummy variable that signals the respondent participated in the SVORI programs while in prison. Table 1 includes the summary statistics for all variables. On average, respondents have lower mental health scores in prison than post-release, suggesting that individuals’ mental health is better when out of prison.
Summary Statistics for All Variables (N = 550).
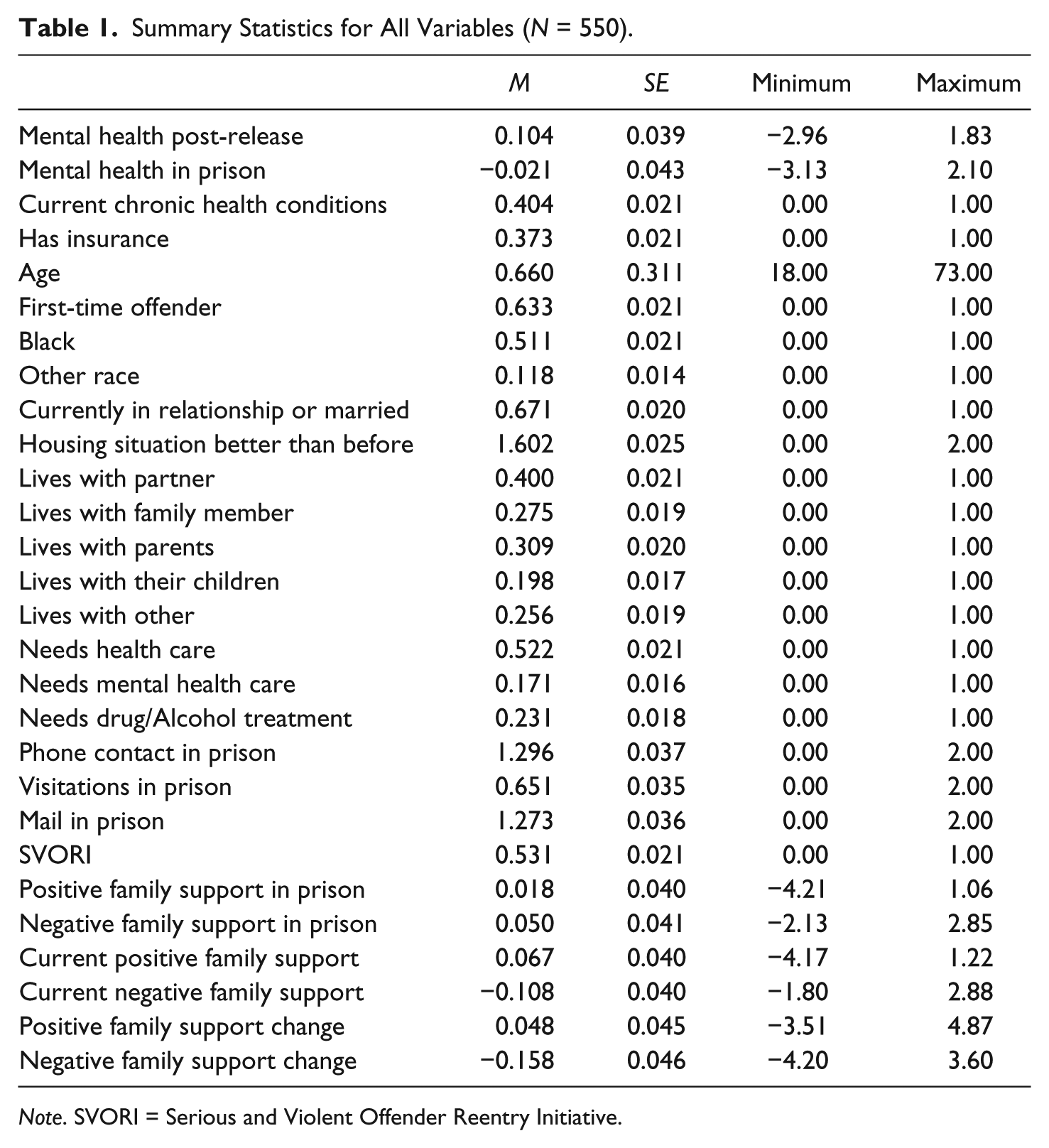
Note. SVORI = Serious and Violent Offender Reentry Initiative.
Analysis Plan
This study employed an ordinary least squares (OLS) regression with a lagged dependent variable. Specifically, we predicted current (or Wave 3) mental health with lagged Wave 1 (pre-release) mental health while controlling for other correlates of mental health, demographic and personal characteristics, and our independent variables regarding positive and negative familial support. We present three models: (a) the impacts of in-prison positive and negative familial support on mental health, (b) the impacts of in-prison and current positive and negative familial support on mental health, and (c) the impacts of the change in positive and negative familial support between in-prison and post-release on mental health. Variance Inflation Factors (VIFs) were examined for each model run and we found no issue with multicollinearity. The highest VIF for the models presented here is 1.3, well below the cutoff of 10 for troublesome multicollinearity.
Results
Table 2 showcases the results from all models. Before discussing the independent variables, we note the significant controls. As expected, lagged, or in-prison, mental health has a significant positive relationship with current mental health. Next, individuals who currently need mental health care report worse mental health than individuals who do not. Individuals reporting needing drug and/or alcohol treatment also report poorer mental health than individuals who do not. Note that there are no race differences in mental health, nor do chronic health conditions affect mental health. These findings are consistent across models. Given previous research regarding the benefits of visitation in prison (Bales & Mears, 2008; Duwe & Clark, 2011; Jacoby & Kozie-Peak, 1997), we were surprised to find there was no effect of any type of in-prison contact with post-release mental health. Relatedly, we were also surprised by the lack of effect current housing situation has on current mental health given the importance of social and family ties in successful re-entry outcomes (Dumont et al., 2012; Fleisher & Decker, 2001; Visher, 2010; Visher & Travis, 2011). However, the lack of findings for visitation and housing status may simply be a consequence of our modeling strategy, given that lagged dependent variables often account for a significant amount of variation in models.
OLS Models Predicting Current Mental Health With Lagged Mental Health, Controls, and the Familial Support Variables.
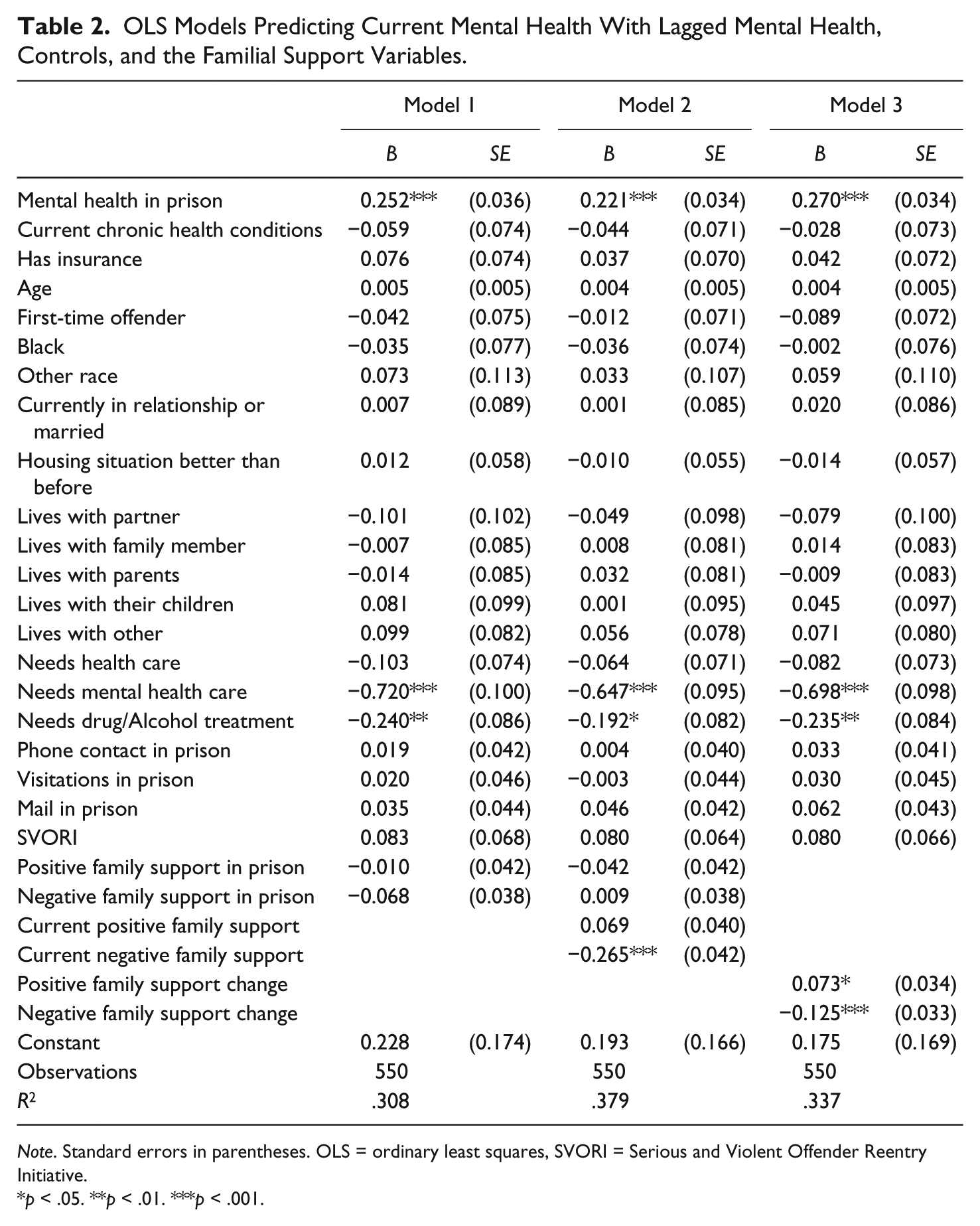
Note. Standard errors in parentheses. OLS = ordinary least squares, SVORI = Serious and Violent Offender Reentry Initiative.
p < .05. **p < .01. ***p < .001.
Moving on, Model 1 shows the impact of in-prison family support on current mental health. Here we see no effect. Family support in prison, whether that support was positive or negative, has no effect on current levels of mental health. This is unexpected given that we anticipated social support, generally, to have some relationship with post-release mental health. Prior research suggests the importance of in-prison social support (Jacoby & Kozie-Peak, 1997). This suggests that the social contexts of prison are perhaps more salient for mental health while in prison than one’s family context, which is not immediately accessible.
Model 2 displays the impact of both in-prison and post-release family support on current mental health. Post-release levels of negative family support impact current levels mental health controlling for other variables. There is a strong and significant (p < .001) negative relationship between current levels of negative family support and current mental health. Because the family support scales are standardized, we can interpret change in standard deviation units. For every one standard deviation increase in negative family support, current mental health decreases by about −0.27; in other words, the higher negative family support is, the poorer the individual’s current levels of mental health. Note too that the size of the coefficient for current negative family support is larger than the coefficient for lagged mental health in prison. Thus, current levels of negative family support are a stronger predictor of mental health than prior mental health. Accordingly, it appears that negative family support has a stronger relationship to mental health than positive family support. Unfortunately, little prior research tells us why this may be the case given that the focus of previous studies have been on positive family interactions, visitation, and support. A simple explanation may be that while positive social support is needed, the mental health of former prisoners may be more affected by negative family dynamics.
Finally, in Model 3, we show the results for changes in the level of both positive and negative familial supports. Again, there is an effect for negative family support, but now we also see an effect for changes in positive family support. These models show the importance of both in-prison support and post-release family support: There is a small, but positive, relationship between changes in positive family support and mental health, while there is a negative relationship between changes in negative family support and mental health. The former relationship is demonstrated in Figure 1, which shows the predicted value of Wave 3 mental health by the range of change in negative family support. Remember that a higher score on the MHS is associated with better mental health. For individuals who experienced a large decline in negative family support between being in prison and 9 months after release, their mental health levels are higher. For instance, a decline of −3.5 equates to a mental health score of more than 0.5. Put another way, a sizable decline in negative family support equates to an above-average mental health score.
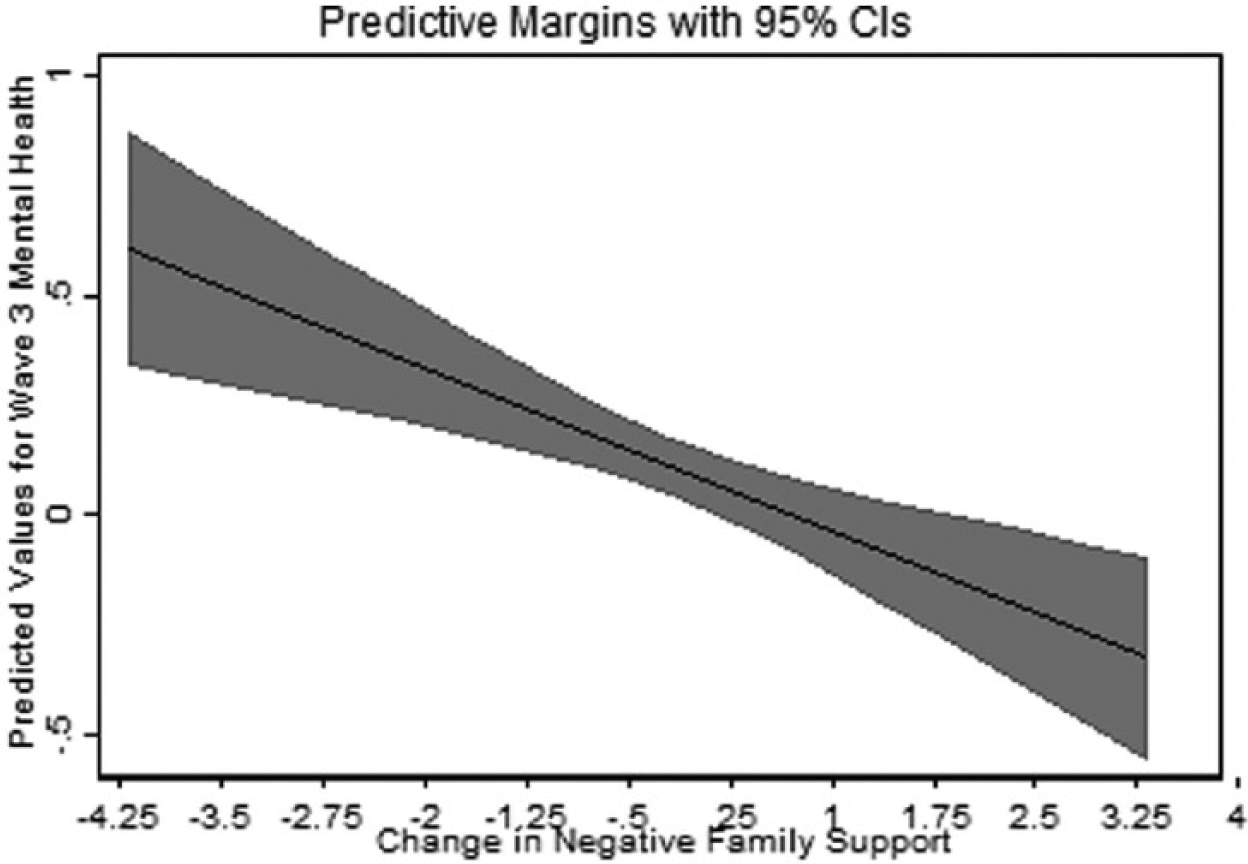
Predicted values of Wave 3 mental health by change in negative family support.
Discussion
With the prevalence of psychiatric disorders among inmates being higher than that of the general population (Schnittker et al., 2012) and the likelihood of imprisonment being more common among today’s population (Schnittker et al., 2012; Uggen, Manza, & Thompson, 2006), understanding the correlates of good mental health for former prisoners is important not only for public health reasons, but also as a way to help former prisoners stay out of prison. Our study explores the role that familial social support, both in prison and post-release, plays in shaping the mental health of released prisoners. We examine not just positive familial support and its influence on mental health but also negative familial support, where the former prisoners report feeling that they have disappointed their family or feel criticized by family members. Next we discuss our primary results, which are threefold.
First, we demonstrate that familial social support while respondents were in prison—whether negative or positive—has no direct bearing on mental health post-release. This is surprising given that past research has shown that inmates who take part in prison visitation programs report having stronger social ties to their family as well as feeling closer to them (Carlson & Cervera, 1992; Howser, Grossman, & Macdonald, 1984; Howser & MacDonald, 1982) and positive social support is consistently linked to better mental health (Cohen & Wills, 1985; Thoits, 1995; Uchino et al., 1996). Our expectation here was that in-prison familial support would be a correlate of post-release mental health given that support is readily tied to social functioning and re-entry is highly stressful to returning prisoners (Clear, 2007; Massoglia, 2008; Wang et al., 2009). Surprisingly, however, in-prison support was not significant compared with current levels of family support. We turn to those models next.
Unlike in-prison support, post-release familial support does affect post-release mental health, though negative familial support is far more consequential than positive familial support. Given the dearth of research demonstrating the importance of social support and ties for mental health (Cohen & Wills, 1985; Sarason et al., 1983; Thoits, 1995; Uchino et al., 1996), the non-significant effect of positive familial social support was unexpected. Research putting forth policy recommendations regarding family ties and support typically suggests enhancing such programs when the prisoner returns to the community (Visher & Travis, 2011). Yet, our results suggest that for better mental health outcomes post-release, families need not simply enhance existing positive ties but also lower negative forms of support in family dynamics.
Finally, while in-prison familial support may not directly affect post-release mental health, the change in that support from in-prison to post-release does affect mental health. This is the case for both positive and negative family support. As shown in Figure 1, our results demonstrate that when negative familial support decreases (i.e., it becomes better), former prisoners have higher, or better, mental health. On the contrary, when negative familial support increases (i.e., negative support becomes more prominent), former prisoners’ mental health decreases. The prominent conclusion here would be that for positive re-entry outcomes, in particular, good mental health, any changes in familial support, should generally be positive or, at least, the changes should result in fewer negative familial dynamics. It is possible that former prisoners are more sensitive to negative familial support and dynamics than positive ones; this could be due to the expectation of a positive reunification with family and friends upon release (Clear, 2007). The disjuncture between expectations and reality may be particularly troublesome for the mental health of former prisoners, particularly when family dynamics continue to worsen post-release. Future research should examine how the differences between expectations of familial support and actual receipt affect former prisoners’ mental health.
One way to facilitate better mental health outcomes for prisoners is the opportunity for conjugal visits. Though conjugal visits are usually thought of as private time allowed for married couples, the term has been used to denote time with other family members, sometimes referred to as family reunion programs (Gordon, 1999). The primary objective of these extended family visits is to encourage the maintenance of family bonds to facilitate the inmate’s adjustment upon release (Carlson & Cervera, 1991; Gordon, 1999). In addition, states that allow conjugal or family visits have noted inmates’ improved disciplinary records and more successful re-entry outcomes (e.g., lower likelihood of recidivism and higher likelihood of employment upon release; Carlson & Cervera, 1991). While we found that in-prison family support does not affect mental health, fostering positive family support among inmates and their families may be a way to combat the deleterious effects of negative familial support.
Another policy change relevant to mental health that prisons could implement is virtual visitation. While prisons are often located further away from major city centers and towns for safety or overcrowding (Christian, 2005), with the advent of modern technology, the costs for transportation could be defrayed by allowing use of virtual methods of communication. Some states have commissioned this, most notably Pennsylvania, in addition to their allowance of face-to-face visits (Crabbe & Immarigeon, 2002). Unfortunately, there is a concern that this policy might cause prisons to limit in-person visitation as a result.
There are a few limitations worth noting in our study. First, because many of the programs the SVORI aimed to evaluate had never been implemented before, there were some issues in getting the programs to fully function; as such, this may affect some of the questions we used from SVORI, though it is unlikely. In addition, the study called for interagency coordination and cooperation, but this was not seen in all sites (Lattimore et al., 2004). Next, there was considerable attrition across waves. The highest response rate was in Wave 1 or in prison. However, analyses by Lattimore and Visher (2009) suggested that the attrition was random and not related to participation in the SVORI study. As such, we believe that our final sample is not statistically different from those who left the study after Wave 1.
Conclusion
Our study has demonstrated that social support is important for mental health outcomes for prisoners recently released from prison; however, the negative elements of social support are more influential to this relationship. Future research and programming needs to simultaneously examine ways to foster familial support for prisoners both in and out of prison, as well as help families negotiate the strain and stress of a prisoner returning from prison. Former prisoners are unlikely to find employment and housing immediately, causing family members to feel burdened by them. Thus, programmatic ways to help families as well as former prisoners cope with the strains of re-entry are likely to improve familial relationships and therefore promote better mental health outcomes among former prisoners.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.