
Abstract
Interventions for family violence in Aboriginal communities should take a culture-based approach and focus on healing for the whole family. The purpose of this research was to identify risk issues from the perspective of service providers for couples counseling with Aboriginal clients following intimate partner violence. A total of 25 service providers participated in over the phone interviews concerning risk with Aboriginal men in couple counseling. Five concepts emerged including (a) collaterals, (b) commitment to change, (c) violence, (d) mind-set, and (e) mental health. It was concluded that culturally competent interventions should involve the entire community and have a restorative approach. The concepts were compared and contrasted with the available literature.
Aboriginal peoples in Canada include First Nations, Métis, and Inuit peoples. The effects of multiple, collective, and cumulative traumas continue to be felt across the generations following European contact. Exposure to disease and loss of life, confinement and banning of cultural practices, as well as mass removals of children from families and communities continue to seriously threaten the well-being of individuals, families, and communities. The present overrepresentation of Aboriginal peoples in the justice system, where they comprise 23% of the federal inmate population but only 4% of the Canadian population, is a manifestation of this colonial history (Sapers, 2013). Aboriginal men make up approximately one quarter of all corrections admissions (Perreault, 2014), are more likely than non-Aboriginal men to be serving time for a violent offense (Perreault, 2009), and about one third are at high to moderate risk for intimate partner violence (IPV; Rugge, 2006).
Following release, reconnections with family and community members can be positive as well as challenging. In a study within one Canadian province, the rate of lifetime reconviction following a prison sentence for domestic violence was nearly half (48%; Department of Justice, 2009). Although both institutional- and community-based programs for men range in effectiveness, they generally produce positive effects on recidivism (Babcock, Green, & Robie, 2004; Eckhardt et al., 2013). Community programs for women and children who are affected by IPV can reduce isolation and improve social support (McWhirter, 2011). However, proponents of gender-segregated IPV treatment have argued against therapists seeing couples together given the potential for blame on the woman for violence as well as concern for her safety (Bograd & Mederos, 1999).
Recently, there has been attention to circumstances under which it may be appropriate to work with couples following IPV (Stith, McCollum, Amanor-Boadu, & Smith, 2012) along with considerable conceptual development (Stith, McCollum, & Rosen, 2011). This model includes the need for changing patterns of power and control, including thinking and behavior, as well as promoting responsible and effective ways of understanding and solving interpersonal problems in relationships (George & Stith, 2014). It is a combination of feminist and systemic schools of thought. Violence is understood as the perpetrator’s responsibility and its existence a reflection of power imbalance within the relationship (Lawrence, 2014). Solution-focused notions of strength and solution-building, emphasizing current resources and future hopes instead of present problems and past causes (Kaslow, Bhaju, & Celano, 2011), are also attended to in this model.
In addition, interventions for family violence in Aboriginal communities must take a culture-based approach and focus on healing for the whole family (Alaggia, & Vine, 2006). Research on effective counseling with Aboriginal peoples indicates that positive experience depends on how well the counselor understands and operates from within an Aboriginal cultural perspective, including attending to spiritual aspects of healing (Heilbron & Guttman, 2000). Furthermore, appropriate counseling for Aboriginal families where violence has been experienced should recognize the violence as a product of colonization. The contextual model must be sensitive to the historical and contemporary contexts of oppression, cultural genocide, and massive group trauma across generations. The conditions of poverty, substance abuse, and intergenerational violence must be countered therapeutically with an emphasis on the strengths of communities, families, and individuals. Flexible and multi-level interventions (Oetzel & Duran, 2004) that include important parts of Aboriginal worldviews such as spirituality, ceremony, and interconnections are required (Weetra et al., 2006).
There are no conceptual or practice models that are culturally specific for intervention following IPV with Aboriginal couples (Willmon-Haque & BigFoot, 2008). The intent of the present study was to explore issues associated with risk, from the perspectives of individuals who have provided service in Aboriginal communities, that must be attended to in the development of culturally appropriate practice for couple-based IPV treatment. Specifically, the present study has a dual purpose to (a) determine which factors counselors identify for addressing IPV risk in the treatment of Aboriginal couples overlap with factors found in current IPV risk assessment instruments, and (b) identify additional relevant cultural factors by counselors working with Aboriginal couples in treatment for IPV.
Literature Review
The topic of the risk has been studied a great deal in relation to violent offending in general and IPV in particular. However, there has been less research on risk for violence among Aboriginal men. Specifically, and most relevant for the purposes of the present study, there has been little research on risk in couples counseling following IPV and none on risk in couples counseling for IPV with Aboriginal clients.
There appears to be support for the use of major risk factors to predict re-offense among both non-Aboriginal and Aboriginal offenders (Shepherd, Adams, McEntyre, & Walker, 2014; Smallbone & Rallings, 2013). In relation to violent recidivism, these factors include criminal history, pro-criminal attitudes, pro-criminal associates, antisocial personality characteristics, substance abuse, and leisure activities among Aboriginal men (Gutierrez, Wilson, Rugge, & Bonta, 2013). However, there have been mixed results regarding problems with education and employment as well as family problems, which are predictive of recidivism among non-Aboriginal men but less useful for predicting risk for Aboriginal men (Rugge, 2006).
Factors that may not predict re-offense for violence, but are important considerations for Aboriginal men involved in corrections, have been identified. There is considerable evidence that Aboriginal men are disproportionately affected by education and employment difficulties (Howells, Day, Byrne, & Byrne, 1999), as well as sense of identity, acculturation pressures and stress, separation from family and culture (Martel, Brassard, & Jaccoud, 2011), as well as both interpersonal and systemic discrimination (Jones, Masters, Griffiths, & Moulday, 2002). These non-criminogenic needs such as family disruptions, personal and family trauma and loss, as well as mental health challenges must be countered with a focus on strength, ties to land and culture, and spirituality (Howells et al., 1999).
Although several instruments have been developed for use with men who have been convicted of IPV, none have been validated for use with Aboriginal men nor have they been validated for use in couples counseling. However, professionals in the field of risk assessment have used them for men who have experienced IPV and the instruments themselves were familiar to participants in the present study. In addition, they provided a structure to discuss major, established factors related to risk that may be considered in IPV counseling.
Risk Factors for IPV
In general, decisions about risk involve consideration of the nature, frequency, and severity of the violence in addition to the likelihood that it will occur (Hart, 2001). Frequently used risk assessment tools for mandated clients are the Spousal Assault Risk Assessment Guide (SARA) and the Ontario Domestic Assault Risk Assessment (ODARA). These tools assess risk of future partner assault in addition to the frequency and severity of these assaults. The SARA has good internal consistency and differentiates between individuals with and without a history of IPV (Kropp & Hart, 2000). In addition, ODARA has predictive accuracy for IPV among men who do not have prior assault against a partner or a corrections history (Hilton & Harris, 2009). In a recent review of instruments ranked on the basis of predictive validity for IPV recidivism, and most relevant for the purposes of the present study, the SARA and ODARA were the top two (Messing & Thaller, 2013).
The SARA (Kropp, Hart, Webster, & Eaves, 1999) consists of 20 items that represent five main risk factors: (a) criminal history, (b) psychosocial adjustment, (c) spousal assault history, (d) current and most recent offense, and (e) other considerations. The 20 items were identified primarily from the literature on characteristics of assaultive husbands, the predictors of violent crime, and clinical experience.
The ODARA was empirically derived from an initial pool of potential risk factors gleaned from police files on 589 domestic violence perpetrators (Kropp, 2000). The 13 risk factors include (a) previous domestic incident, (b) previous non-domestic incident, (c) prior correctional sentence of at least 30 days, (d) failure on previous conditional release, (e) threat to harm or kill anyone at the index assault, (f) confinement of the partner during/at the index assault, (g) victim concerned/fearful of future assaults, (h) two or more children, (i) victim has a biological child from a previous partner, (j) perpetrator’s violence against others, (k) perpetrator’s substance abuse, (l) assault on victim when pregnant, and (m) any barrier to victim support.
Criminal history
An important factor to consider in a male’s risk for IPV is criminal history. This could include both violent and non-violent criminal charges, with special attention to current and most recent offense(s). Generally, men who are aggressors in IPV are more likely than non-violent partners to be violent or aggressive in other ways and with other people (McHugh & Frieze, 2006). They are more likely to have a criminal history (Roberts, 1987; S. O. White & Straus, 1981) and to have used violence outside of the home (Hotaling & Sugarman, 1986; McHugh & Frieze, 2006). Straus (2004) looked at 17 studies that examined the frequency of perpetrators of partner assault who had a history of previous crime. Men whose assaults on a partner were frequent and severe and involved injury requiring medical treatment, tended to have a history of crime, whereas men whose assaultive behavior was not frequent or severe enough were less likely to be involved in other crime.
Psychological adjustment
A second important risk factor to consider is psychosocial adjustment. This includes general antisocial behaviors and attitudes. Although there is no specific personality profile, higher rates of particular conditions have been found among men who are aggressors in IPV (McHugh & Frieze, 2006). Personality disorders with antisocial, borderline, and narcissistic features occur at higher rates among members of this group (Rock, Sellborn, Ben-Porath, & Salekin, 2013). Early descriptions by survivors indicated that they had traditional sex-role attitudes (Taylor, Nair, & Braham, 2013). Research in the area of assertiveness appears to discriminate between batterers and non-batterers (Banks, Kini, & Babcock, 2013). Negative attitudes about women also play a role in the prediction of risk for IPV (Basile, Hall, & Walters, 2013).
Spousal assault history
A third important risk factor to consider is spousal assault history. This could consist of a recent escalation in violence (Winstok, 2013) and characteristics of the most recent assault (Capaldi, Knoble, Shortt, & Kim, 2012). History of IPV elevates risk for future IPV (Belfrage et al., 2012). Separation and divorce typically do not end the relationship violence (Vatnar & Bjørkly, 2012). One of the primary risk factors for violence against a spouse or significant other was having committed such violence against that same person previously. Rarely did an incident of violence occur in without emotional or verbal abuse and emotional or verbal abuse were risk markers for violence (Riggs, Caulfield, & Street, 2000).
Additional risk factors
Additional considerations for risk include stability of the relationship, employment status, mental health, childhood abuse, or witnessing partner violence (Kropp, Hart, Webster, & Eaves, 1999) as well as motivation for change (Zalmanowitz, Babins-Wagner, Rodger, Corbett, & Leschied, 2013). One of the most consistent findings is that men who were violent were more likely to have a history of violence in their family of origin (Fritz, Slep, & O’Leary, 2012). Furthermore, alcohol abuse and, to a lesser extent, drug use have been associated with IPV (Flett & Hewitt, 2012). Importantly in the search for risk markers, it does appear that couples who are experiencing severe relationship distress are at greater risk of violence than are non-distressed couples, though it is not clear whether the distress leads to violence or the violence leads to distress (Smith & Weatherburn, 2013). Similarly, men of lower socioeconomic status (SES) are at an increased risk of perpetrating domestic violence and also tend to perpetrate more severe violence than their higher SES counterparts (Chilton, Rabinowich, & Woolf, 2013).
There is a considerable literature base for the assessment of risk for IPV among men who have been in contact with the justice system. Risk factors have been established. However, it is not known whether these risk factors are relevant for assessment of couples engaged in counseling, nor what culturally relevant factors should also be attended to. The purpose of the present study was to explore issues associated with risk from the perspectives of individuals who have provided service in Aboriginal communities. The research was exploratory in nature, with a goal of identifying factors that should be recognized in the development of culturally appropriate models for family-based intervention with couples following IPV.
Method
Although initially used for evaluation purposes, concept mapping was later employed in the development of new programs (Cousineau, Houle, Bromberg, Fernandez, & Kling, 2008), logic model development (Petrucci & Quinlan, 2007), and identification of relevant constructs in evaluation (Brownson et al., 2008). Concept mapping is a quantitative analysis of qualitative data. Participants identify the issues and group them together. The role of the researcher is to select the most appropriate number of concepts for the final map, based on the ways that participants organized responses into groups.
Participants
Invitations to participate were extended by the Agency Director to service providers in family violence. Research assistants contacted interested individuals by telephone. The interviews included demographic questions as well as the open-ended question: “How would you address risk with Aboriginal men in couple counseling who use abusive behavior with their intimate partner?”
Participants suggested others who they thought would be interested and those individuals were contacted through their place of employment. A total of n = 25 professionals participated. The age range was 29 to 64, with M = 49. Twenty-five percent of the sample were male. The number of years of experience ranged from 3 to 40, with M = 22. All had worked with Aboriginal couples in a professional capacity.
Participants were asked if they would be interested in taking part in the second phase of the study, where they would be asked to group responses together. A list of interested individuals was compiled with mailing addresses.
Procedure
Each participant provided responses to the question. All responses were written down verbatim. Three members of the research team independently reviewed all responses made. Each member independently identified responses that were unclear or redundant. When the reviews were combined, any response with at least two members identifying it as redundant (e.g., “behavioral instability,” “unstable behavior,” and “erratic conduct” were identified as redundant) was removed. In this example, “behavioral instability” was retained and the other two responses removed. In other cases, responses that were unclear were edited for clarity (e.g., “for the person working with the couple to make sure that they are both safe” was reduced to “making sure they’re both safe”). In the end of the process, there were a total of 98 unique responses. On average, each participant provided approximately 4 unique responses.
Telephone numbers and addresses of all participants who had expressed interest at the time of interview in the sorting task were randomized, and contacted again by both telephone. Sixteen participants were mailed out instructions on how to complete the sorting task and 8 returned their sorts.
Each package of information included a set of cards for each question. Each response was printed on a separate sheet. In addition, participants received sorting instructions summarized by Trochim (1989) as,
each response can only be placed in one pile (i.e., an item cannot be placed in two piles simultaneously); all responses cannot be placed in a single pile, and; all responses cannot be put into their own piles (although some items may be sorted by themselves). (p. 5)
Each was asked to group the cards in a way that made sense to her or him (Trochim, 1989). Each sort data were obtained by telephone.
Data Analysis
Two statistical procedures were used to analyze the sort data. Multidimensional scaling placed the responses as points on a map. Cluster analysis of multidimensional scaling was used to group the responses into concepts.
Sorting data were used to construct a similarity matrix (Kane & Trochim, 2007). The number of rows and columns in the matrix was equal to the number of responses generated for that question. The cells indicated if and how many times the responses were grouped together multidimensional scaling was used to determine proximity of the generated responses to one another, based on the frequency within which they were in the combined similarity matrix. The Concept System (1997) placed each response as a point on a point map. The point map was a visual representation of the combined similarity matrix. Responses that were closer together were more frequently grouped together by participants.
Cluster analysis of the multidimensional scaling values was used to group responses on the point map into clusters that reflected similar concepts (Blashfield & Aldenderfer, 1988). In the beginning of analysis, each response represented its own cluster. In each consecutive stage of the analysis, the algorithm combined two clusters until they were all part of one cluster.
Selection of the optimal number of concepts was based on researcher judgment. Fewer concepts identified the most central ideas. More concepts provided a detailed picture, but in the process, the overall message of the map was lost. Trochim (1989) suggested that when choosing the optimal number of concepts to select as few as possible.
The selection of the final number of concepts was based on qualitative and quantitative data. The qualitative data included the responses themselves, and the choice was influenced by perceived similarity between responses within concepts and difference between responses in different concepts. Quantitative data, in the form of the bridging index, were used to identify the most cohesive concepts (i.e., those with the lowest average bridging indices) and to inform the application of labels for the final concept map based on the responses within each cluster with the lowest individual bridging index because they were seen to be the most central to the content of the concept.
Results
A total of 98 unique responses were made in response to the question and sorted by eight participants. To determine the final map, solutions from 10 to 4 were examined. The 10-concept solution did not show clearly differentiated clusters. Changes introduced during the reduction to 9 were insignificant. Subsequent reductions from 9, 8, 7, 6, and then 5 increased the differentiation between concepts. The 4-concept solution appeared to be overgeneralized. The solution that provided the best interpretability was the 5-concept solution (see Figure 1). Responses and bridging indices are presented in Table 1.
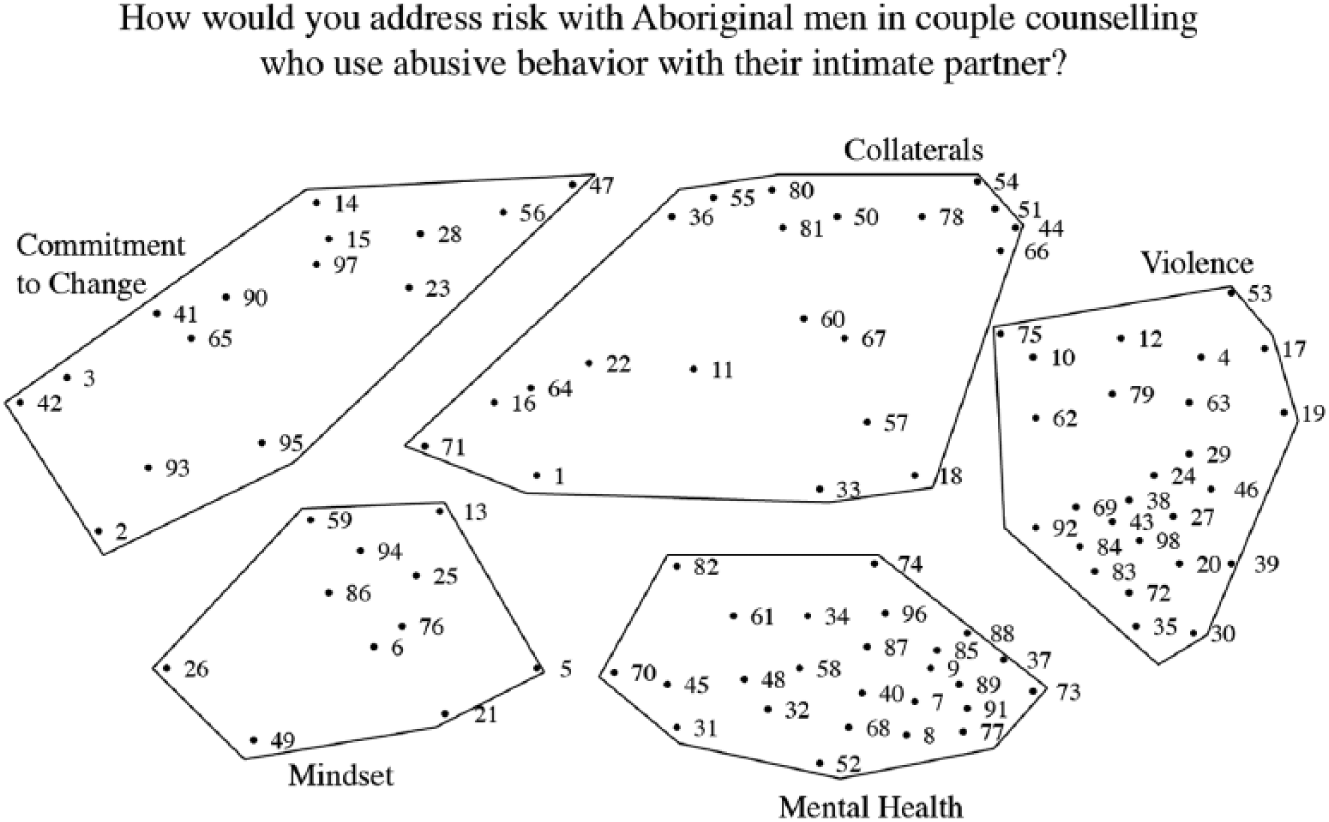
Concept map.
Concept Items and Bridging Values for Concept Map.

Note. SARA = Spousal Assault Risk Assessment.
The bridging index was used to identify the most central responses within each concept and assisted with the labeling of concepts in the final map. The bridging index was a value between 0 and 1. Responses with a low bridging index, between 0.0 and 0.25, indicated that participants had most frequently sorted them with other responses within the concept. Participants equally frequently sorted responses with a high bridging index, between 0.75 and 1.00, with responses in other concepts as well as those within their own concepts. Trochim (1989) noted that highly bridging responses might not fit conceptually with those immediately surrounding them on the map, and were therefore less likely to reflect the overall content of a concept. Based on the individual bridging index values, an overall bridging index was calculated for each concept. The lower the average bridging index values, the greater the coherence of responses within that concept. A stress value was calculated. This value represented the degree to which the map was accurate representation of the sort data. The stress value for this map was 0.27, which was within an acceptable range of 0.05 to 0.35 (Kane & Trochim, 2007).
Concept 1: Collaterals
This concept referred to important secondary information required for the full use of primary information in the assessment of risk. It had a moderate average bridging index suggesting that responses within it were also grouped with responses found in other clusters. The five lowest individual bridging indices ranged from 0.39 to 0.51, and the responses included “cultural factors,” “fighting over kids,” “mental health,” “partner checks,” and “home life of each partner.”
Concept 2: Commitment to Change
This concept referred to the man’s commitment to change as an important consideration in risk. It had a high average bridging index suggesting that responses within it were also grouped frequently with responses found in other clusters. The five lowest individual bridging indices ranged from 0.59 to 0.66, and the responses included “support for males,” “mandated clients,” “good support system,” “contract in place,” and “elder involvement.”
Concept 3: Violence
This concept represented history of violence in the assessment of risk. It had a moderate average bridging index suggesting that responses within it were also grouped with responses found in other clusters. The five lowest individual bridging indices ranged from 0.07 to 0.15, and the responses included “emotional abuse,” “increase in violence,” “gang involvement,” “weapons,” and “pet abuse.”
Concept 4: Mind-Set
This concept reflected the state of mind of the man in relation to risk. It had a moderate average bridging index suggesting that responses within it were also grouped with responses found in other clusters. The five lowest bridging indices ranged from 0.52 to 0.64, and the responses included “denial,” “attitudes,” “remorse,” “conflict and communication patterns,” and “understanding of effects on their children.”
Concept 5: Mental Health
This concept represented mental health as an important factor in the assessment of risk. It had a low average bridging index suggesting that responses within it were rarely grouped with responses found in other clusters. The five lowest bridging indices ranged from 0.00 to 0.02, and the responses included “stalking,” “strangulation,” “child abuse survivor,” “financial problems,” and “suicidal ideation.”
Discussion
In this section, results from the concept map are compared with the literature to identify factors from existing IPV risk instruments that overlap with factors professionals identify for addressing risk in couples engaged in IPV treatment. In addition, results from the concept map that describe cultural factors for addressing risk engaged in IPV treatment are presented.
Risk Factors for IPV
Within each of the concepts, there were several references to factors that were consistent with risk factors for IPV risk assessment that have been presented in the literature and within the SARA and ODARA instruments. There were also some differences, suggesting areas worthy of further research as well as consideration by therapists examining risk in the context of couple’s counseling.
Concept 1: Collaterals
There is a great deal of evidence in the literature on IPV risk to support the practice of information collected from collaterals for use in the assessment (Buchanan, 2012; Rivett & Rees, 2013; Ronan, Dreer, Maurelli, Ronan, & Gerhart, 2014). One concern that has been identified is the potential risk to those who are collaterals, such as children or allies, who may or may not be the same individuals providing risk-related information (Dobash & Dobash, 2012). In addition, information to be used for an accurate risk assessment is to be the most positive indicator of risk (e.g., Andrews & Bonta, 2011). Collaterals who are fearful of change to their relationship or the individual may withhold risk-related information. In addition, the self-report of the individual upon whom the risk is assessed may be of limited value in calculating actual risk given the benefits of presetting favorable information (Poythress et al., 2010). However, we are not aware of a published instrument or procedure that requires collateral information from several others, including both partners, service providers, law enforcement, and corrections records.
Concept 2: Commitment to change
Responses within this concept were consistent with the literature on risk factors for IPV. Commitment to change has been assessed from the perspective of motivational stages of change (Chen, Jacobs, & Rovi, 2013) and reinforced, to a lesser extent, through the use of contracts in family therapy (Karakurt, Dial, Korkow, Mansfield, & Banford, 2013).
Concept 3: Violence
The responses in this concept were consistent with the existing risk assessment literature, identifying similar indicators in relation to general and IPV as well as law enforcement and corrections involvement. There is a significant body of literature on assessing risk of violence. Several instruments have been developed and compared for their utility with men who have been convicted of violent offenses (e.g., Singh, Desmarais, & Van Dorn, 2013). In relation to IPV, reviews have been completed (Nicholls, Pritchard, Reeves, & Hilterman, 2013), and comparisons have been made to determine which instruments obtain the most accurate results for recidivism prediction (e.g., Messing & Thaller, 2013; Singh, Grann, & Fazel, 2011). Common factors in the SARA (Kropp, Hart, Webster, & Eaves, 1999) and ODARA (Kropp, 2008) overlap a great deal with those identified by participants in the present study, including violence history and previous IPV convictions (Straus, 2004), violations of release or escalation of violence (Winstok, 2013), use of weapons (McLaughry et al., 2013), as well as personal experiences of abuse (Fritz et al., 2012).
Concept 4: Mind-set
There is literature on factors identified in this concept in relation to risk. Participants noted that these factors would be necessary prerequisites for couples counseling. The presence of these factors as prerequisites implies that prior to counseling the couple has completed work, typically separately, to achieve this level of awareness. These prerequisites included, egalitarian attitudes about women and men (Banks et al., 2013; Basile et al., 2013), acceptance of official accounts of previous violent behavior with a clear understanding of his personal responsibility for it (Scott & Straus, 2007), and ability to empathize with his partner and children (Maliken & Katz, 2013). In addition, he would have made gains in ability to regulate his emotions (Roberton, Daffern, & Bucks, 2012) and insight about his own processes, such as beliefs and emotions triggered by particular events in his relationship that contribute to his thoughts and behavior.
Concept 5: Mental health
There is evidence in the literature for the use of mental health factors in risk assessment similar to those identified by participants (Yang, Wong, & Coid, 2010). These overlapping factors include personality disorder with significant mood instability and impulsiveness (Ross & Babcock, 2009) as well as controlling behaviors motivated by jealousy, such as stalking (Hall, Walters, & Basile, 2012) that reflect a high risk time for violence during separation (Zeoli, Rivera, Sullivan, & Kubiak, 2013). In addition, financial problems (Chilton et al., 2013) and substance abuse problems (Flett & Hewitt, 2012) were noted.
Cultural Factors
Concept 1: Collaterals
We have interpreted the inclusion of “cultural factors” as indicative of the need for assessors to be aware of culture in risk assessment, as well as specific factors to be considered in determination of risk as referenced in the literature (Howells et al., 1999; Jones et al., 2002; Martel et al., 2011). One difference between responses regarding culture in the present study and the existing literature is the extent of community member involvement as collaterals in the assessment, and in particular, the importance placed by participants in having traditional knowledge holders, such as Elders, contributing to the assessment that was noted by participants in the present study.
Concept 2: Commitment to change
Within this concept, the response “Elder involvement” was particularly relevant to determining commitment to change for Aboriginal men. We interpreted this to mean that commitment referred to openness specifically, meaning that the man was honest about his past, present, and future intentions. Participants also identified that not only should commitment be determined on the basis of non-violence but also on the bases of having a healthy relationship and a healthy lifestyle. The intent is not to minimize risk for violence in determination of commitment to change, but rather, to add the need for assessment of commitment to having a healthy relationship and having a healthy lifestyle. Non-violence is necessary but not sufficient evidence of commitment, from the perspectives of participants in the present study, to be in couples counseling. Community members knowledgeable about the couple, especially Elders, who can gauge this commitment, are essential.
Concept 3: Violence
In this concept, there was a reference to “geographic location.” Although conditions in urban, settlement, and reserve communities vary considerably, when combined, there are significant disparities between standards of living for Aboriginal and non-Aboriginal peoples (J. P. White, Maxim, & Beavon, 2011). The Supreme Court of Canada (Rudin, 2012), recognized conditions that must be considered for individuals involved in the correctional system, including trauma, cultural and spiritual identity challenges, compromised formal education and poverty. The need for access to culturally appropriate methods of healing has also been recognized (Hyatt, 2013).
Concept 5: Mental health
There were two responses in this concept, including “foster care history” and “residential school experience” that were particularly salient for working with Aboriginal men. Personal experiences in family of origin, including abuse and placement in care, as well as family experiences such as residential school attendance, personally or of a parent, also contributed to potential for parenting to be compromised. These issues have received much less attention in the risk literature. It is important to understand the effects of these experiences, as applicable, for couples in counseling because they may have contributed a great deal to the problems that either or both have experienced in their lifetimes and manifest in their relationship. The personal effects of abuse challenge individuals in their relationships in many ways, but often interconnect with a lack of basic trust. Individuals who grow up in care have had several, and potentially multiple, examples of parenting relationships at different points in their childhood that have been more or less healthy but presented as “normal.”
In addition, it is absolutely essential to understand what residential schools represent for Aboriginal communities. The schools, funded by the federal government and operated by the churches from the 1870s to 1996, were cultural genocide efforts using whatever means necessary “to kill the Indian in the child” (Truth and Reconciliation Commission of Canada, 2013). The loss of life and abuse of many who attended affected their families and communities as well as generations that followed. In addition to the trauma and effects thereof on sense of identity and community, knowledge about parenting skipped a generation and was profoundly affected thereafter. Although it is important from a risk and therapeutic perspective in IPV to recognize personal responsibility for behavior, it is fundamentally important to ensure that, for Aboriginal peoples individually and collectively, the federal government and the churches must bear responsibility and accountability for the abuse they committed.
Limitations
There are several limitations to the study that should be noted. First, the approach taken to sample selection does not allow for generalizability of results. However, all who agreed to participate completed the interview. Second, there was some attrition by participants in the sorting task from the original interview suggesting that those who sorted may have been different than those who did not. Third, the cluster averages, with one exception, were in the moderate range of consistency suggesting that the responses contained within them were also grouped with responses in other clusters. However, the overall validity of the concept map was in the acceptable range.
Conclusion
There were many similarities and some differences between the experiences of participants in the present study and the existing literature on risk assessment in IPV. The similarities suggest that, on the whole, factors that counselors identify for addressing IPV risk in counseling with Aboriginal couples overlap considerably with factors found in current IPV risk instruments. Relevant factors for assessing IPV risk appear to be useful for assessing risk within the context of counseling with Aboriginal couples following IPV.
However, there were several cultural factors that participants identified which were not reflected in the existing risk literature including the need for a range of collaterals including community members and Elders, evidence of commitment to a healthy relationship and lifestyle in addition to being violence-free, insight and behavior change in response to previous, gender-specific treatment, recognition of impact of efforts made to commit cultural genocide against Aboriginal peoples in relation to intergenerational trauma, post-traumatic stress and complicated grief, as well as abuse by religious figures and justice personnel against individuals and affecting the collective across generations.
To determine risk relevant for couples counseling with Aboriginal men and their partners for IPV, participants noted that information from a broad range of others who are knowledgeable about the man’s risk and the woman’s safety needs and resources, including both partners, other service providers, law enforcement and corrections as well as family members, such as children and siblings, and community members, including Elders, as appropriate, were required. These individuals also needed the relevant cultural knowledge, as necessary, to evidence engagement in and efforts in traditional healing and a healthy lifestyle.
Another difference between the existing risk literature and the experiences of participants in the present study concerned the need for goals for counseling in addition to living violence-free. Participants indicated that there also needed to be a focus on having a healthy relationship and a healthy personal lifestyle as additional requirements for the couple’s counseling.
In addition, participants noted that evidence in the forms of behavioral change and insight of progress through gender-specific treatment was needed. Couple’s counseling was clearly not viewed as a first-line response to IPV. Couple’s counseling, according to participants in the present study, could be considered following successful gender-specific treatment with evidence of change and ability to meet the requirements for entry.
Finally, another difference between the experiences of participants in the present study and the existing literature concerned the necessity to recognize colonial efforts and the effects on individuals, families, and communities, with enough sophistication to notice and respond to differences in meaning and impact of the abuses committed against clients both directly and indirectly.
Clinical Implications
Although risk factors identified in current research, according to participants, are relevant and viable indicators for assessing risk for IPV in relation to counseling with Aboriginal couples, additional factors were identified, implying the need to attend to both culturally informed means and goals of assessment as well as factors to be considered and a restorative approach to program development and delivery.
There is a clear need to involve the community, beyond the professional community which is necessary but not sufficient, including local leaders, individuals knowledgeable about the family, and importantly, elders. The cultural knowledge collectively held by members of the community is necessary for an accurate assessment of IPV risk and woman’s safety. Without it, inaccurate assessment, either minimizing or inflating risk depending on the community’s awareness of, approaches to and resources for IPV, is likely. The sense of accountability that men have to others in the community, beyond their partners, is a very powerful culturally based risk factor. The accountability and level of responsibility that come with seriously following a traditional spiritual path with an Elder can also play a very important role in risk.
There is also a need to have a decidedly restorative approach toward risk. There has been far too much emphasis placed on “problems” within the Aboriginal community, and far too little emphasis on solutions. Research on responsivity is important to draw from when assessing risk so that there is a clear sensitivity to what is workable for the couple in the context within which they live. In addition, research on protective factors that reduce risk is also important to recognize and consider. However, we are suggesting a deliberate move to install a “good life” as a goal. Although there are many ways to define the concept of a “good life,” our point here is that professionals need look at, as well as beyond, risk when assessing, to embrace positives, strengths, resiliencies, as well as capacities and expectations for reaching this goal.
The established criminogenic factors associated with IPV risk, including those from research with Aboriginal and non-Aboriginal men are relevant and necessary to address risk with Aboriginal couples in IPV treatment. Criminal history, particularly previous convictions for violence and IPV are important factors, as well as antisocial personality traits. Changeable factors, such as substance abuse and employment are to be considered. More culturally specific considerations include self-worth and identity, as well as how these are affected across generations of trauma and loss, and manifest in mental health. The strength factors that should be promoted, because they mitigate risk and promote wellness, are tied to land and culture, tradition, and spirituality.
Finally, it is also important to have a restorative approach toward program development and delivery. Programs should be culturally located and informed from within the communities where they exist. Although systemic, feminist, and narrative theories appear to contain useful elements to draw from for developing culturally relevant programs for IPV among Aboriginal couples, there is a colonial history that cannot be overlooked. The causes of current challenges faced in many Aboriginal communities are a direct result of colonial policies, attitudes, and conduct. In particular, the intrusions of colonial values that support men’s violence toward women exist in sharp contrast to traditional values emphasizing equal as well as distinct and essential contributions of women to leadership and community life. Those who have this cultural knowledge and credibility, who can walk and talk about partnership and non-violence between men and women, are best positioned to influence behavior.
Footnotes
Acknowledgements
We would like to thank the professionals who participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the financial support of this research through a grant from the Social Sciences and Humanities Research Council of Canada.