
Abstract
There is an increasing interest in mentally ill offenders’ (MIOs) treatment experiences in forensic settings. This study focuses on the treatment perspectives of MIOs in treatment as well as in prison settings in Flanders. Seventeen MIOs were interviewed about the treatment they received. Data were analyzed using thematic analysis to derive key themes while acknowledging the individuality of the participants’ experiences. Treatment perspectives of MIOs in both settings revolved around similar themes, including “good” staff and privacy. However, their views differed on two themes: MIOs in treatment settings reported on feelings of lacking control and experiencing too much pressure, whereas MIOs in prison settings reported the opposite. The positive experiences in prison settings may complicate the transition from prison to a forensic treatment setting. The study further underscores the major challenge to create more opportunities for MIOs to meet their needs of self-determination in secure forensic treatment settings.
Introduction
There is an increasing interest in gaining clients’ personal perspectives on care in forensic mental health services (Coffey, 2006; Faulkner & Morris, 2003; Morrison, Burnard, & Philips, 1996; Ryan et al., 2002; Sainsbury, Krishnan, & Evans, 2004; Wood, Thorpe, Read, Eastwood, & Lindley, 2008), contrary to the past, when little attention was paid to psychiatric service users’ own views on their treatment (Rogers, Pilgrim, & Lacey, 1993). Persons with mental health problems were seen to lack the objectivity in determining the appropriateness and quality of treatment they received (Lebow, 1982) and were deemed unable to give valid opinions (Weinstein, 1979). However, mental illness does not preclude people from offering clear, valid, and objective perspectives in the services they receive (Hoge et al., 1998; Lidz et al., 1995). Service users’ views can inform professional responses to their complex needs (Coffey, 2006) and may help to determine health needs, which could lead to improvements in quality of life and increased satisfaction with services (Sullivan, 2003).
Mentally ill offenders (MIOs) residing in forensic institutions often have complex support needs and multiple problems to address in treatment. A Belgian study showed that approximately 75% of the imprisoned MIOs had a double or triple psychiatric diagnosis (Cosyns, D’Hondt, Janssen, Maes, & Verellen, 2007). Another study found that 45% of imprisoned MIOs showed co-morbidity of a major mental illness and a substance abuse disorder (Young, 2003). The treatment of MIOs in forensic settings is further challenging due to the dual objective of protecting society on one hand, while treating the MIOs on the other hand. Recent publications on the rehabilitation of MIOs emphasized the importance of pursuing treatment, rather than only concentrating on risk reduction (Andrews & Bonta, 2010; Barnao, Robertson, & Ward, 2010; Robertson, Barnao, & Ward, 2011; Ward & Brown, 2004; Ward, Yates, & Willis, 2012). In this respect, the Good Lives Model of Offender Rehabilitation (Ward & Brown, 2004; Ward et al., 2012) is a promising strength-based approach because of its focus on the offender’s personal hopes, quality of life, and well-being, while addressing the offender’s criminogenic needs (Ward et al., 2012). From this standpoint, efforts to disclose how MIOs perceive treatment may be regarded as paramount in responding to the MIOs’ complex support needs.
Previous international research on the service users’ perspectives in forensic mental health services mostly focused on specific subgroups of MIOs such as older MIOs (De Smet et al., 2014; Schroeder, 2013), forensic patients with personality disorders (Ryan et al., 2002; Sainsbury et al., 2004), or MIOs with an intellectual disability (Wood et al., 2008), as forensic mental health users are not homogeneous group. A review study of Coffey (2006) pointed out that service users in forensic mental health valued the therapeutic relationship and that providing supportive yet challenging therapeutic assistance was helpful. Furthermore, institutional controls were seen as punitive and negative experiences of professional responses were reported in relation to self-harming behavior, control and restraining procedures, and failing to establish clear therapeutic boundaries. Moreover, restrictions on liberty were a concern, and, finally, communication of information needed to be improved.
To gain insight into the factors that might facilitate or hinder treatment of MIOs, the current study aims to assess the perspectives of medium- and high-risk MIOs on their treatment (admission, treatment, and discharge process) in forensic institutions in Flanders, the northern part of Belgium. This is an interesting case, as the development of forensic psychiatric treatment services, housing high- and medium-risk MIOs, is still in its infancy (e.g., Boers, Vandevelde, Soyez, De Smet, & To, 2011; Casselman, 2000; Cosyns, Van Peteghem, Raes, & Sabbe, 2006; Naudts et al., 2005; To et al., 2014). Therefore, the situation in Flanders lends itself well for a profound analysis of MIOs’ perspectives to help shape treatments, which can be relevant for other countries as well.
Focusing on the personal treatment experiences of MIOs, a qualitative approach was adopted to address the following research questions:
Method
Settings and Participants
The study was conducted in Belgium where MIOs who are not considered responsible for their offences are subject to an internment measure. This internment procedure, which is undefined in duration, is considered a safety measure to protect society while providing psychiatric treatment to MIOs.
This study targeted medium- and high-risk interned MIOs residing in forensic institutions in Flanders. Participants were selected from two types of forensic residential settings where medium- and high-risk MIOs of Flanders currently reside: treatment settings as well as correctional settings (where high-risk MIOs currently reside).
Treatment settings consisted of eight treatment wards located in all medium-secure forensic institutions existent in Flanders. All institutions had similar inclusion and exclusion criteria. Examples of exclusion criteria are psychopathy, high-risk, sexual offences, and intellectual disability. Examples of inclusion criteria include being adult or having a predominantly psychotic or personality disorder. Two out of three institutions organized their wards based on the key psychopathological disorder (psychotic and personality disorder) and then by the progress in treatment, whereas the third institution mainly structured the wards on the progress of the treatment, having patients with mixed psychopathological disorders in one ward. Only one institution included female MIOs. Although all institutions were organized in a similar way, having a ward program (ward activities and duties) and an individual therapeutic program (individualized therapy and duties), the atmosphere and ward rules differed from institution to institution, even from ward to ward. For example, wards differed in their policies regarding the access to their room, whether patients can have a key of their room, the degree of privacy in the ward, and so on. Furthermore, all wards differed in size (from 6 to 27 beds) as well as in the patient composition (e.g., mixed gender vs. only male, mixed disorder vs. predominantly one disorder, the phase of treatment).
Correctional settings consisted of two correctional institutions in Flanders where MIOs resided if no proper treatment alternatives were available. Currently, all high-risk MIOs reside in prisons, since at the time of this study, high-secure forensic treatment institutions were still absent in Flanders. Care for MIOs in correctional settings was provided by one or more multidisciplinary teams who work independently from the prison system and who comply with the medical confidentiality. In contrast to a treatment setting, there are no ward programs, as these MIOs are locked up in individual or shared prison cells, sometimes even with inmates who are not interned. The therapeutic programs are provided for MIOs on a voluntary basis, because the goal is to motivate MIOs to participate and not to force them to comply. Therapeutic activities are often less extensive compared with treatment settings because of staff shortages.
Participants were only included in the study when it was reasoned by the institution’s psychiatrist that they were capable (a) to give their informed consent, (b) to communicate in Flemish, and (c) to participate in an interview. All of the participants have been assessed by an expert-psychiatrist as part of the internment procedure under the Belgian Law and were considered “not criminally responsible” due to a mental illness or intellectual disability.
To obtain the perspectives of a diverse sample of medium- and high-risk MIOs—including MIOs with different psychopathological disorders and at different stages of their treatment—a modified, stratified sample method was used to ensure maximum variation and heterogeneity. For the treatment settings, a sample matrix was developed combining the different psychopathological disorders (predominantly personality or psychotic disorder) with the different phases of their treatment (continuum in treatment plan) to randomly select one participant from each category in the matrix. Medium-secure forensic institutions have two or three treatment phases represented in different wards. The first treatment phase takes place in a closed reception ward, where the focus lies in observation and starting up treatment. There is usually no or limited access to the outside world (e.g., outside activities are always under the supervision of staff). The last treatment phase occurs in an open ward, where the emphasis is on treatment and re-socialization. Some institutions have an extra treatment phase between the first and last treatment phase. Such wards concentrate on treatment, and access to the outside world is usually determined individually. In the prison settings, only a distinction in disorders (predominantly personality or psychotic disorder) was made, as there is no distinction in treatment phases. Table 1 shows the sample matrix where the distribution of the sample is demonstrated by setting, treatment phase and psychopathological disorder.
Sample Matrix.
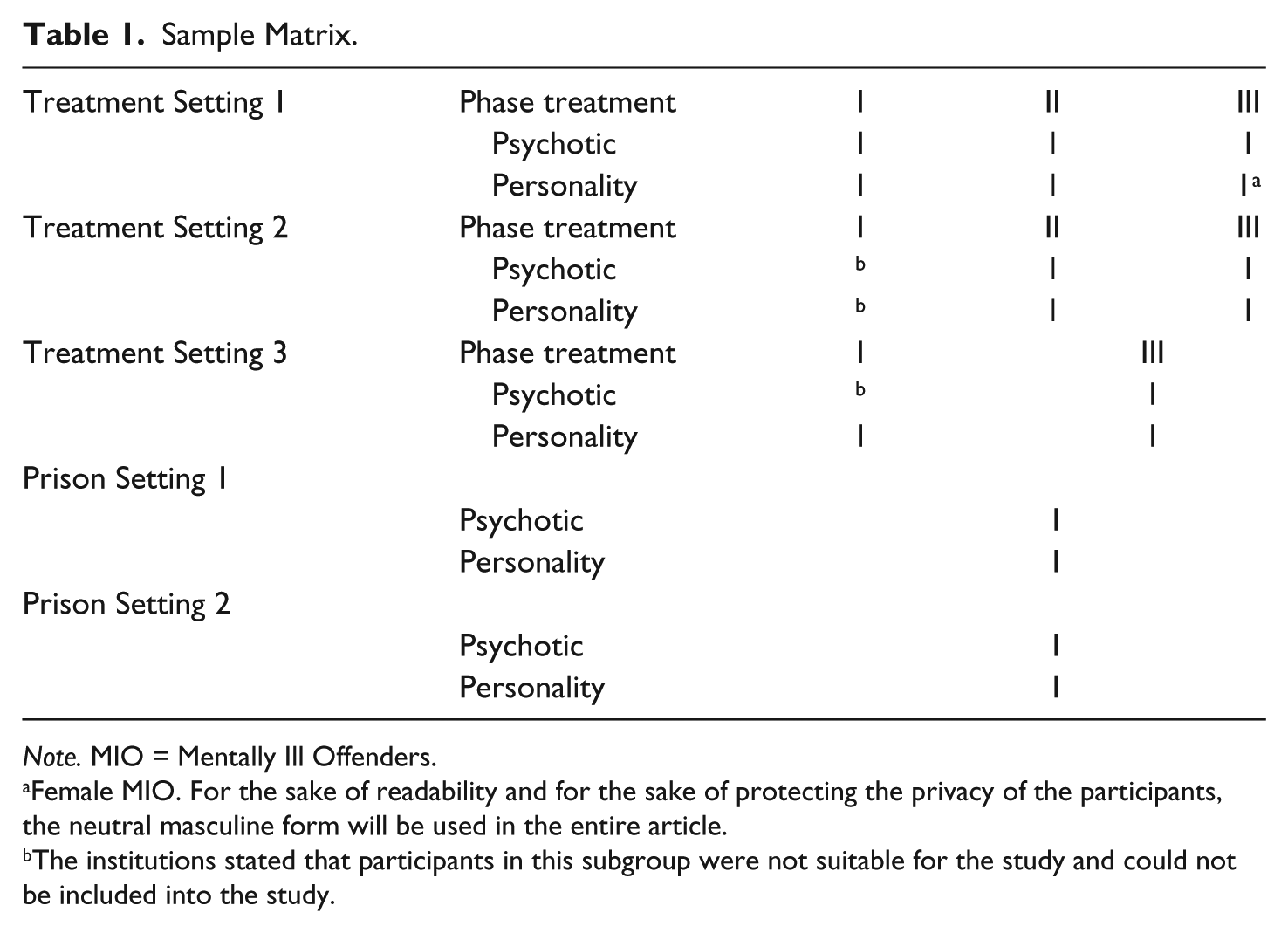
Note. MIO = Mentally Ill Offenders.
Female MIO. For the sake of readability and for the sake of protecting the privacy of the participants, the neutral masculine form will be used in the entire article.
The institutions stated that participants in this subgroup were not suitable for the study and could not be included into the study.
Seventeen MIOs took part in the research, of which 16 men and 1 women (only 1 medium-secure forensic institution included women). All participants were interned because of their mental illness.
Procedure
A period of participant observation was first integrated to get acquainted with the forensic setting and the participants. Then, semi-structured interviews took place.
Participant observation
A period of participant observation was adopted to examine the forensic setting, its treatment, and to install a relation of trust with the participants to maximize the potential to participants’ personal perspectives on the treatment. Participants were reassured that their responses were confidential and that these would not be passed on to the clinical team. The principal researcher, a female clinical psychologist, was independent of all clinical teams and had no clinical contact or responsibility for the participants. The observation period varied from 7 days in correctional setting to 17 days in treatment setting. In both settings the participant observation started with a period of observing each ward facility and its organization. Thereafter, therapeutic treatment sessions were allowed to be observed when all participants had given their consent.
Semi-structured interviews
Semi-structured interviews aimed at mapping participant’s perspectives on the treatment they receive and were based on an interview schedule to obtain information to the purpose of the study. However, it was sufficiently flexible to allow participants to talk about their experiences. The interview format covered the following themes: experience(s) of previous admissions, experience(s) of admission process, experience(s) of change of wards, overall experience of treatment received (daily activity, individual therapy, group therapy, . . .), experience(s) of the relationship with multidisciplinary team, and experience(s) of the relationship with other patients. The average length of interview was 1 hr. The interviews were digitally audio recorded and transcribed verbatim.
Data Analysis
The interviews were transcribed verbatim. Then, thematic analysis was used to derive key themes, while acknowledging the individuality of participants’ experience (Braun & Clarke, 2006). An inductive and semantic approach was applied within thematic analysis to identify themes that are strongly linked to the data (Patton, 1990). By using an inductive or data-driven thematic analysis, the themes identified may bear little relation to the specific questions that were asked in the interview (Braun & Clarke, 2006). Furthermore, it was not the aim to fit the themes into an existing coding frame or specific theory using data-driven thematic analysis (Braun & Clarke, 2006). Following the semantic approach in thematic analysis, themes were identified at a semantic level and not at an interpretative level (Braun & Clarke, 2006). Thus, the first analyses were descriptive in nature, paraphrasing the most remarkable participants’ perceptions on treatment not involving any forms of interpretative work. Then, going over each list of remarkable perceptions on treatment of each participant, connections between the perceptions of different participants were explored, and themes or categories were identified. These themes were regularly discussed among the first two and the last author, which made it possible to “test” in consecutive stages of the analysis process whether or not the emerging themes were consistent with the data and how these themes could be further refined. The second author was involved in the process of checking the confirmability of the themes that were detected.
Ethical Approval
Ethical approval was granted by the University Hospital Ghent (Belgium) for the forensic care settings (2010/514) and by the Ethics Committee of the Faculty of Psychology and Educational Sciences at Ghent University (2011/66) for the correctional settings. Ethical approval was always obtained in collaboration with the participating institutions prior to collecting the data.
Results
This study revealed seven themes from MIOs’ treatment experiences in treatment settings and four recurrent themes from MIOs’ treatment experiences in prison settings. The seven themes emerging from the participants’ experiences in treatment settings are (a) the feeling of lacking control, (b) the pressure to perform, (c) their label of interned MIO, (d) the feeling of responsibility and trust, (e) privacy, (f) staff, and (g) living with other MIOs. The recurrent themes emerging from the participants’ experiences in prison settings are (a) feeling of control, (b) no pressure to perform, (c) privacy, and (d) staff. To determine whether themes emerged predominantly from participants’ experiences in treatment or prison settings, frequency counts were made for each theme across the participants. These figures are shown in Table 2. The specific themes are illustrated by quotes of MIOs.
Frequencies of Themes in Service Users’ Account.
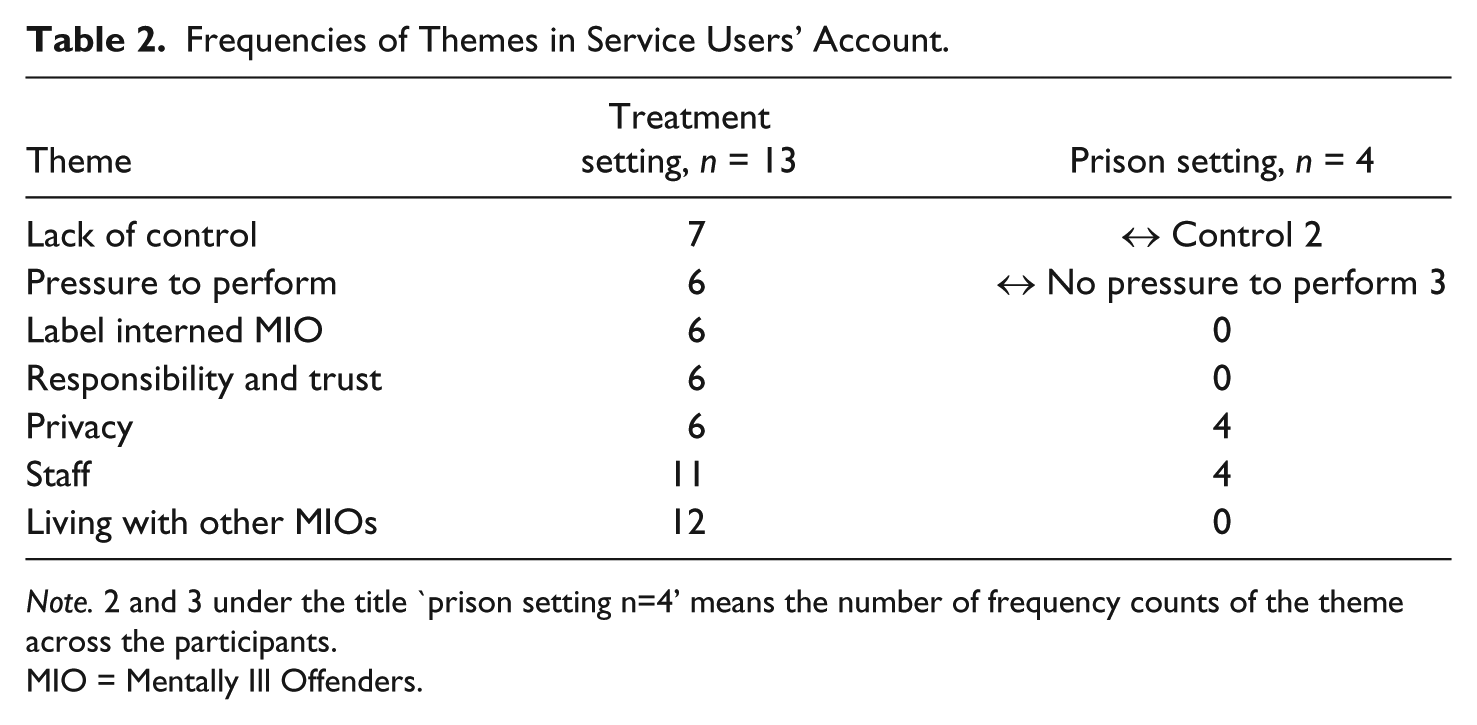
Note. 2 and 3 under the title `prison setting n=4’ means the number of frequency counts of the theme across the participants.
MIO = Mentally Ill Offenders.
Lack of Control
The experience of lacking control figured strongly in the perspective of the MIOs in treatment settings in great contrast to the perspective of MIOs in prison settings. Lack of control was especially stated in the first treatment phase in forensic treatment settings where MIOs are controlled by many external ward rules and restrictions upon their ability to control day-to-day things. Participant observation revealed that ward rules and restrictions were present in all wards in different forms. There were general ward rules and restrictions that apply for every ward member (e.g., wake up hour) and individual rules only applicable for individual ward members (e.g., limited control over their finances). Some rules and restrictions were written down in a document or in the form of a poster visible in the shared areas; others were verbally communicated and known by all ward members. Especially, in the first treatment phase, many general ward rules and restrictions were applied for every ward member and often written down in documents. These rules were often applied to provide structure for the MIOs (e.g., day structure) or for security or organizational reasons and were perceived as obstructive to the participant’s feeling of control. In the interviews, participants reported experiencing the ward rules and restrictions as stressful, childlike, too strict, too rigid, and not adjusted to the individual needs of each person. Especially in the first phase of treatment, regulations like a strict day structure, limited access to facilities like the fridge, no access to their room during day time, no key to their room, staying in a locked room at night for security reasons, and therefore not able to smoke at night in their locked room were experienced as negative. They complained about having no control over small things in a ward setting. This is illustrated in the following quotes of MIOs talking about the rigid rules in the first phase of treatment in comparison with later phases of treatment:
There are too many rules, e.g., if you want to cook something, you cannot cook whenever you want. You can only cook between 4 and 5 p.m., later than that it is not possible. Also, smoking in your room is not allowed anymore, so when your room is closed at night [because of security reasons] you can’t smoke any cigarettes. (MIO in his 30s, Treatment Phase 3, talking about the first treatment phase)
Only one MIO residing in a forensic treatment setting noted that the ward rules were needed. Another MIO reasoned that some ward rules should be personalized and adjusted to the individual needs of each person.
Lack of control in treatment settings was further experienced in terms of not having control over their money, not having control over their sex life, not having the freedom to access or lock their own room, and having to ask staff members everything:
The only thing that bothers me is the fact that I have to ask everything and almost have to beg to get something. I am so sick and tired of that. (MIO in his 40s, Treatment Phase 3)
MIOs in prison settings did not report feelings of lacking control given their incarceration. All four imprisoned MIOs, having experienced treatment in forensic mental health institutions in the past, preferred being in prison rather than going to a forensic mental health institution. One of the main reasons for their preference for prison settings is their perception of opportunities for choice (e.g., go to therapy or stay in cell), in other words their feeling of having some control in prison (e.g., deciding how to spend their time in own cell) and thus experiencing some freedom, even in a penitentiary context. Two of the four MIOs in prison expressed this awareness of more freedom in prison and refused to apply for an intake in forensic mental health institutions, which is the most common way for MIOs to get out of prison working toward integration into society. These MIOs were young (one MIO was in his 20s and one MIO was in his 30s) and both had opportunities to get admitted in a medium-secure forensic treatment center.
I hate the fact that the therapies in forensic treatment centers are compulsory. For instance, in that particular forensic treatment institution the rooms were locked during the day, so you were sitting with the whole group encaged in the living room. So you are in a way locked up, but the difference with prison is that in prison you will have your own cell to be in alone . . . prison works better for me compared to a forensic treatment institution, because I have more space to do my own thing. I am incarcerated, but nevertheless I do feel freer because I can do my own thing, like meditating. (MIO in his 30s, prison)
Pressure to Perform
The pressure to perform every day in treatment was reported by MIOs in forensic treatment settings in all phases of treatment. Every day MIOs sense the pressure to perform well in treatment out of fear of being sent back to prison if rules were violated.
I am so afraid to make a misstep here. I always fear for that . . . they can always send you back to prison: when you don’t cooperate or if you do not do what you need to do. (MIO in his 20s, Treatment Phase 2)
The constant fear of being sent back to prison demotivates people and creates elevated levels of stress for MIOs in forensic treatment settings.
As expected, there was no pressure experienced by MIOs in prison settings to do well in treatment, as treatment is not mandatory in prison and as there is nothing that serves as a threat when you are unmotivated for treatment in prison. Three out of four MIOs residing in prison reported feeling more calm in a less uptight prison setting.
Label of Interned MIO
Internment is an indefinite measurement, in contrast to a sentence. Not knowing when the measurement ends often makes MIOs hopeless. Mostly MIOs in treatment settings described this label of internment as very burdensome and stressful in all phases of the treatment. The uncertainty about when the internment measurement will end is damning while in treatment.
An offender gets a sentence and knows when he is a free man again. An interned mentally ill offender has to wait and does not know when it ends and that is making me crazy, you do not have an idea when it ends. (MIO in his 20s, Treatment Phase 2)
Furthermore, their experience of being more susceptible to be send back to prison because of their label is burdensome and perceived as unfair.
Trust and Responsibility
The importance of having the feeling back of trust and responsibility in treatment settings is endorsed by six MIOs. MIOs feel the urge to be trusted again.
In a later phase of treatment, MIOs appreciate being trusted and they see it as an opportunity to take responsibility.
A positive thing about this ward is that they have faith in you, you get responsibility. It sounds banal and simple, but it is a big difference. If they trust you, you get the key of the fridge; you can take out and put in whatever you want. That’s trust. (MIO in his 40s, Treatment Phase 3)
The sense of responsibility is very strong in the last phase of treatment. MIOs are pushed to take responsibility as they will need this in society to which they return.
In this ward you do need to take back your responsibility, because in the first and second ward staff partly took that over. Here it’s up to you to show them how well you cope with this responsibility. (MIO in his 40s, Treatment Phase 3)
Privacy
The need for privacy is stressed by MIOs in treatment (in all treatment phases) as well as in prison settings, often represented by the need of having an own room. Examining the ward organization through participant observation had elucidated that, in both settings, bedrooms were allocated on a first come, first served basis. Thus, new coming MIOs will typically have to share a room with other MIOs, while others will then have the opportunity to move to a “better” room (e.g., a room alone). Given the shortage of space in prison, MIOs will often find ways to enforce a private cell. Two MIOs in prison disclosed in the interview that they have found a way to get an own room by for instance working in prison (workers in prison are privileged to have an own room) or by threatening to hurt any cell mate if they need to share a cell. The importance of having an own room or space to rest and unwind is endorsed by many MIOs.
In the first ward I was so angry, because I was always surrounded by people and I did not have any privacy . . . I was so happy that I had my own room, because it wasn’t fun constantly being around people you cannot stand. Before when I shared a room with three other persons, it was as if I was in prison. You cannot flee from those persons and as long as you cannot be on your own, you find no rest. Here, I have my own room and that made me calmer. (MIO in his 20s, Treatment Phase 2)
Lack of privacy is also reported when consulting staff members of the treatment team. One MIO argued that the lack of privacy while meeting with the psychiatrist resulted in no more requests to see the psychiatrist. He argued that it is a bit strange to have a psychiatrist consultation in an open space where staff members are present.
First of all you have to make an appointment to see the psychiatrist in person; so there has to be a reason to meet him . . . but to have an appointment while the staff is present, that’s a bit weird . . . that’s the reason I don’t see the necessity to talk to the psychiatrist “in private.” (MIO in his 20s, Treatment Phase 2)
Staff
The importance of “good” staff was mentioned by most MIOs in treatment and prison settings. MIOs in treatment settings expressed positive as well as negative experiences with staff, whereas MIOs in prison settings only expressed positive experiences. The majority of MIOs in prison (four MIOs) as well as in treatment settings (six MIOs) reported having a good relationship with the staff.
Four MIOs in forensic mental health settings described their relationship with staff members as good, but somewhat artificial and professional.
Staff is very friendly here. Well, friendly. They do their best to be friendly, but I think it is all a bit professional. They are friendly because they have too . . . it is their job. (MIO in his 40s, Treatment Phase 3)
Two MIOs suggested staff to be more pro-active toward patients in treatment. One MIO thought staff members of the first phase of the treatment were a bit patronizing. He could not stand the sarcasm and cynicism of these staff members.
Living in Group With Other MIOs
Living in group with other MIOs was an issue that had been reported by almost all MIOs in forensic treatment settings. Negative experiences of living with MIOs were mostly expressed in relation to mixed treatment wards or mixed therapies where patients with different pathologies come together. This experience is expressed by MIOs in all stages of treatment and is especially perceived as noisy, stressful, and chaotic when the group size is large.
I experienced the first ward as a very stressful ward, because you had to deal with so many different people who had different problems. It was very difficult . . . everybody is doing their own thing. It was very chaotic. (MIO in his 20s, Treatment Phase 2)
MIOs reported that living in a group is not easy, but is something you get used to. However, after a certain time of living in a group, they look forward to live on their own.
MIOs also reported positive experiences living with other MIOs. Most of them had a good buddy in the same ward or enjoyed having company all the time, never feeling alone in the ward. Furthermore, they stated that the group helped putting things in perspective and motivate them to go to therapies.
Discussion
By exploring the personal experiences of MIOs on their treatment in both treatment and prison settings, this study aims at mapping factors that might facilitate or hinder treatment of MIOs in forensic treatment centers. The most important results will be discussed in relation to international findings, and future suggestions will be formulated.
The results of this study revealed interesting differences in treatment experiences between MIOs in treatment settings as opposed to MIOs in prison settings.
First, when describing their present and past treatment experiences, similar themes emerged from MIOs in both settings; however, their views on particular themes differed. Some themes that were raised in relation to treatment settings also appeared in prison settings, other themes might not have been applicable or less applicable in prison settings because of the specific context, for example, the theme “living with other MIOs.” This theme is less relevant in prison settings as there are usually no day rooms, and MIOs mostly stay in their prison cell. Overall, MIOs in treatment as well as in prison settings certified the importance of good staff and enough privacy in this study. However, experiences of MIOs in prison settings mainly noted positive experience with staff members compared with MIOs in treatment settings. In line with the findings of De Smet et al. (2014), MIOs in this study appreciated the support from the staff from prison care teams and the activities that they organized despite the staff shortages in prison. Generally, MIOs in prison settings felt that staff appeared to genuinely invest in their well-being, whereas MIOs in treatment settings presented some hesitation in the authenticity of the staff’s understanding. This ambivalence in the patient–staff relationship was also described in the study of Johansson and Eklund (2003): “It feels like the staff uses empty phrases as if they get money to for saying certain things, but that they don’t fully understand” (p. 343). Yet, in previous research, the quality of the helping relationship has been perceived as an important vehicle to improve care (e.g., Björkman, Hansson, Svensson, & Berglung, 1995; Johansson & Eklund, 2003; Koivisto, Janhonen, & Vaisanen, 2004; Schroeder, 2013; Shattell, McAllister, Hogan, & Thomas, 2006; Shattell, Starr, & Thomas, 2007). Regarding privacy, MIOs from both settings expressed their need for privacy, mostly in terms of an own room or a private space to be able to rest and unwind. The importance of patient privacy was also described in the study of Morrison and colleagues (1996) conducted in a small forensic unit and in the earliest studies of consumer satisfaction conducted in the 1970s (Raphael & Peers, 1972). Thus, although living with other MIOs can offer some positive experiences in treatment settings, for example, motivating each other, the possibility to withdraw in a quiet room to escape from the noise and presence of the other MIOs is desired by all MIOs. On the issues of not having enough control and experiencing too much pressure to perform in forensic institutions, the opinions of MIOs in treatment settings differed from MIOs in prison settings. Participants indicated having more control and freedom in prison settings and having no pressure to perform compared with forensic treatment settings. They experienced less rules and obligations in prisons compared with forensic treatment settings. Participants in forensic treatment settings described frustrations of losing control over many activities that we take for granted, which is in line with the findings of Wood and colleagues (2008). Experiencing “feeling controlled” and “being forced to be cooperative” corresponds with aspects which are characteristic for all therapeutic environments. These aspects include confronting clients by giving feedback to stimulate personal change, transferring responsibility as much as possible to the clients themselves, and providing structure and safety by offering clear rules and regulations, among other (Boers et al., 2011; Fortune, Ward, & Polaschek, 2014). A therapeutic environment and “good staff members” who are attentive for the therapeutic alliance (Ross, Polaschek, & Ward, 2008) enable clients to gradually take more control and responsibility within a climate of trust and safety (Fortune et al., 2014). So, even though risk management in a forensic setting unavoidably means a certain degree of control, these findings highlight the importance of remaining mindful of the effects that this has upon the individual (Wood et al., 2008). Furthermore, it seems that MIOs in prison settings do not experience any pressure to perform in prison settings compared with treatment settings, as a prison setting is usually the last resort for MIOs.
Second, this study found negative experiences to be far more pronounced in treatment settings than in prison settings. Positive as well as negative experiences were described by MIOs in treatment settings, whereas MIOs in prison settings mainly expressed positive experiences in prison compared with their past forensic treatment experiences. This is in line with the recent findings of De Smet et al. (2014). They found that older MIOs reported more positive and less negative experiences regarding penitentiary settings when compared with institutional care settings. In this study, all examined MIOs in prison stated to be better-off in prison than in a forensic treatment setting, expressing some aversion of medium-secure forensic treatment institutions. Although they were incarcerated, they felt more free (in their choice) and less “under pressure” in prison. They rather stayed in prison than applied for an admission in forensic mental health institutions. A direct transfer to non-forensic mental health care is seen as the only solution to get out of prison by the MIOs in prison settings, as they want to avoid forensic mental health. Non-forensic mental health care is further seen to be a shorter pathway to regain full freedom by the examined MIOs in prison. However, when a detained MIO is ready to be treated in less secure condition, transfer to an institution with an intermediate level of security is often considered to be safer than direct discharge to the community (Bailey & MacCulloch, 1992). The difficulties in the classic transfer from prison to medium-secure forensic treatment settings have been witnessed by a medium-secure forensic treatment institution and penitentiary institution in Flanders. They observed that some MIOs refused an admission in a medium-secure treatment institution after they received more information about the treatment or because of past experiences in forensic treatment settings. The importance of improving the transfer process had also been emphasized by Skelly (1994a, 1994b) as the route from high- to medium-secure facilities might be ineffective—manifested by a high-readmission rate back to high-secure institutions. They examined the experience of MIOs on the transfer from a high- to a medium-secure institution and found that MIOs often experienced this as a “backward step” with all the restrictions and stress that reduce the quality of life (Skelly, 1994a). The most institutionalized patients (i.e., MIOs detained for more than 10 years according to Skelly, 1994a) in their study saw little gain in their transfer and actively desired to remain at the high-secure institution. The MIOs who were less overtly institutionalized (i.e., MIOs detained for less than 10 years according to Skelly, 1994a), however, had difficulty coming with the new demands of transfer rather than in a wish to avoid the demands altogether (Skelly, 1994a). This is in line with our findings. However, three out of our four MIOs in prison settings in this study were detained for less than 10 years, indicating that extensive institutionalization (using the cutoff of 10 years for institutionalization according to Skelly, 1994a) is coincidental rather than causative for this perspective.
Although it is difficult to compare our findings with other studies that assess service users views, because of slightly different target groups and different research methods, our findings correspond with the findings of the study of Wood and colleagues (2008) with regard to the themes “lack of control,” “relationship with staff,” and “living with other service users.” The study also corresponds with the study of Ryan and colleagues (2002) concerning the themes “staff quality.” Furthermore, our results relate to the finding of De Smet and colleagues (2014) with respect to the theme “quality staff” and to the findings of Morrison and colleagues (1996) concerning “privacy.”
The findings of this study could be related to some concepts of the Good Lives Model of Offender Rehabilitation (GLM; Barnao et al., 2010; Ward & Brown, 2004; Ward et al., 2012), which aims at equipping the individuals with skills and resources to obtain primary human goods in socially acceptable and personally meaningful ways (Barnao et al., 2010; Robertson et al., 2011; Ward & Brown, 2004; Ward & Steward, 2003). The GLM is a positive strength-based approach that focuses on the patient rather than the risk reduction (Barnao et al., 2010). That is, individual patients are seen as self-determining agents rather than disembodied carriers of risk (Ward & Maruna, 2007) as interpreted in more risk-centered approaches, such as the Risk Need Responsivity model (Andrews & Bonta, 2010). An exclusive risk-centered approach to forensic treatment often limits treatment to those factors assessed as contributing to risk and fail to encompass a consideration of universally accepted needs that are essential to well-being (Barnao et al. 2010). Based on the results of this study, we can identify an important primary good or human need emerging from MIOs experiences in forensic treatment: agency (i.e., autonomy and self-directedness; Deci & Ryan, 2000; Ward & Brown, 2004). Agency relates to the themes of “lack of control” and the importance of “responsibility and trust” experienced by the MIOs in this study and reflects the need for more autonomy in forensic treatment in terms of less external regulations in treatment and more responsibility. Residing in a secure forensic mental health institution may be seen as an environmental constraint in adapting secondary goods to meet the need of self-determination. (Barnao et al., 2010). Although challenging, opportunities can be created to promote the attaint of this highly valued good by, for example, allowing MIOs to contribute to decision making about treatment plans (Barnao et al., 2010). Another potential of the GLM is its focus on the importance of a strong therapeutic relationship with the offender (Ward & Brown, 2004) which relates to the theme of “good” staff reported in this study. This positive strength-based approach could lead to reduced recidivism (Bouman, de Ruiter, & Rooney, 2009) and can provide evidence for a policy that focuses on offenders’ individual strengths (Vanhaelemeesch, Vander Beken, & Vandevelde, 2014).
The present study has a number of limitations. The strength of the study, providing a deeper understanding of MIOs’ treatment experience without relying on a set format of a questionnaire, also reflects its limitations (Wood et al., 2008). The disadvantage of carrying out a qualitative study is the limited sample of 17 research participants in this study. Similarly, the participants were recruited from a clear-cut geographical area (Flanders), however, reflecting the potential candidates for the forensic psychiatric treatment center in the same area (including medium- and high-risk MIOs in that area). Furthermore, we only included one female MIO in this study. This is an effect of the dearth of treatment possibilities for female MIOs in Flanders, as only one medium-secure forensic treatment center accepts female MIO for treatment. Finally, the subsamples of MIOs from treatment settings and MIOs from prison settings were not equally spread, having a smaller sample of only four MIOs in prison settings. In light of these limitations, the generalizability of the findings is limited. Therefore, these findings are best regarded as an exploration of topics and areas where improvements need to be considered, as revealed by the MIOs themselves.
Conclusion
This study has demonstrated that the personal treatment experiences of MIOs in treatment as well as prison settings revolved around similar themes. MIOs from both settings emphasized the importance of privacy and “good” staff in treatment. However, the views differed on two other themes. The feeling of lacking control and the feeling of too much pressure in treatment were described by MIOs in treatment settings, whereas MIOs in prison settings experienced the opposite. Feeling less pressured and perceiving opportunities for choice by MIOs in prison settings may complicate the transition from prison to a less secure treatment setting even more. This article adds to the current knowledge of how MIOs perceive treatment and how this may influence the application of the Good Lives Model in this population, as there are only a limited number of publications—up until now—on the GLM in forensic mental health (Robertson et al., 2011). According to Barnao et al. (2010), who have adapted the GLM to the Good Lives Model of forensic mental health (GLM-FM), mental illness may prevent offenders in their striving for a fulfilling life. Interestingly, treatment for this mental illness may both positively and negatively influence the pursuit of a “good” life, as it
may provide alternative ways of achieving primary human goods, serving as a transient way of achieving goods such as relatedness, community, excellence in work and play, and inner peace that can later be replaced by more normative means as individuals develop the requisite skills. On the other hand, “treatment” may at times unintentionally present obstacles to the attainment of primary goods through restrictions on a person’s autonomy and, depending on the range and quality of care provided, curtailing or blocking access to other primary goods such as knowledge, creativity, excellence in work and play, relationships. (Robertson et al. 2011, p. 480)
Keeping this in mind, our study clearly points to the major challenge to create more opportunities for MIOs to meet their needs of self-determination in secure (forensic treatment) settings. It also may offer an explanation as to why many MIOs show conflicting and hostile relationships toward staff members in forensic mental health services as well-intentioned, and necessary treatment efforts may be perceived as frustrating rather than supportive. The findings may have important implications for the rehabilitation of offenders, whether it is from a Risk Need Responsivity–oriented or GLM-based point of view, as treatment outcomes for a great part depend on the way we are able to cope with responsivity issues within the therapeutic alliance between staff members and clients.
Footnotes
Acknowledgements
The authors are grateful to all participating institutions for being part of this study and to all participants for their valued contribution. Furthermore, the authors would like to thank the steering committee of the research project for their advice during the research process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financed by the Research Fund of University College Ghent and was conducted by the University College Ghent, Faculty of Education, Health and Social Work in partnership with Ghent University, Center OBRA, and Platform FPC Ghent.