
Abstract
Hope theory identifies goal, pathway, and agency as essential elements of hope that promote and maximize the effectiveness of treatment. Much significant evidence has indicated that hope is a strong predictor of substance involvement recovery. This study aimed to test the effectiveness of choice-based reality therapy in strengthening hope in recovery for women convicted of drug offences in Taiwan. The participants in the substance involvement treatment program were 44 incarcerated women convicted of drug offences, who were randomly selected and randomly assigned to equal-sized experimental and control groups. The results of the study, obtained by ANCOVA analysis, showed significant differences between the two groups in the posttest scores for sense of hope as measured in the subscales of goal setting and pursuing, adequate energy, and controlling pathway. The effect size values of the three variables suggested a moderate practical significance. The evidence provided in the present study indicates that, upon completion of the choice-based reality therapy for substance involvement, when compared with those who had not yet attended the program, Taiwanese women convicted of drug offences reported a significantly higher level of hope. Hope was measured by their ability in setting goals and overcoming obstacles and persistence in pursuing the goals they had set up, energy for recovery, and their capacity to set up pathways based on their goals. The findings highlight the value of choice-based reality therapy in enhancing hope of recovery for women convicted of drug offences.
Introduction
In a stereotyped view, many people tend to believe that substance involvement is a male issue; however, according to statistical data from the Ministry of Justice (2010), in recent years substance involvement has been the leading cause of incarceration for both males and females in Taiwan. In the past 3 years, in fact, a higher percentage of female new inmates than male new inmates in Taiwan have been classified as drug offenders (44% of 3,543 in 2011, 44% of 3,448 in 2012, and 44% of 3,147 in 2013 for females, as compared with 30% of 32,916 in 2011, 30% of 31,881 in 2012, and 20% of 31,020 in 2013 for males; Ministry of Justice, 2014b). Moreover, there has been a high recidivism rate for female drug offenders, ranging from 86.2% to 96.4% in the last 5 years (Ministry of Justice, 2014a). This statistical evidence has highlighted an urgent need for development of substance recovery treatment programs for females.
Many substance-involved females have suffered traumatic experiences of sexual, physical, and emotional violence suffered from childhood to adult life (Hiebert-Murphy & Woylkiw, 2000; Hien, Cohen, & Campbell, 2005; Koenig, 2004; Najavits, Sonn, Walsh, & Weiss, 2004; Nyamathi, Longshore, Keenan, Lesser, & Leake, 2001; Peterson, Berkowitz, Cart, & Brindis, 2002; Wu, El-Bassel, Witte, Gilbert, & Chang, 2003). An article by Gutierres and Puymbroeck (2006) explores the issue of childhood and adult violence in the lives of women who misuse substances. The authors found that those victims who exhibit negative psychological outcomes of depression and low self-esteem due to childhood sexual and physical abuse may turn to substance usage as a way to cope with these painful psychological consequences. Unfortunately, the substance usage puts them at risk for continued victimization from domestic violence and sexual assault, which further reinforces negative feelings of low self-worth, depression and helplessness that in turn leads to more substance misuse and dependence. Other scholars also found that for substance abusers, depression and self-blame were significantly correlated with hopelessness (Illiceto et al., 2010; Janoff-Bulman & Thomas, 1989). Hopeless women have been found to be more vulnerable than others to having a lifetime risk of substance use dependence (Conrod, Pihl, Stewart, & Dongier, 2000) and greater risk of relapse (Grella, Scott, Foss, Joshi, & Hser, 2003). Even when there is an attempt to seek professional help, Sowards, O’Boyle, and Weissman (2006) found that females with the least hope for their future were most likely to have bad treatment outcomes. Other study results also showed that a sense of hopelessness, unfortunately, was a strong predictor of substance-involved clients’ dropping out from the treatment program (Berman, Kallmen, Barredal, & Lindquist, 2008).
Fortunately, scholars have found that hope is a strong predictor of entering treatment for substance involvement (Jackson, Wernicke, & Hassga, 2003), retention (Hampton et al., 2011), and recovery (Guo & Law, 2013; Law & Guo, 2012; Mathis, Ferrari, Groh, & Jason, 2009). Therefore, instilling hope should be considered essential in the development of substance treatment programs for women (Sowards et al., 2006).
Literature Review
Hope and Substance Involvement Recovery
More than two decades ago, Metzger (1988) declared that, for the success of therapy, it is essential that the clients have hope. Soon after, in the 1990s, at the time of the flourishing of positive psychology, C. Richard Snyder (1994, 2000), a founder of hope theory, expressed concern about the general misperception that hope was mainly formed by genetic inheritance and proposed that a hopeful mind-set could be shaped by learning, with emphasis on intended goal, pathway, and agency as three elements of hope. Hope, then, was defined as the motivation to set up a goal-directed pathway supported by the energy to achieve the goal (Snyder, 1994, 1995, 2000, 2002). Pathway, which is also described as pathway thinking, refers to the individuals’ cognitive appraisal to set up plans as well as self-belief in their own capacity for doing so. Furthermore, it also refers to the ability to find alternative pathways to reach the goal when roadblocks are encountered. Agency, which is also known as agency thinking, refers to the need for individuals to have motivation to pursue the goals as well as belief in their capacity to attain them. Agency is a critical element for goal pursuit; without it, the goals and pathways become meaningless. This is especially true when barriers are encountered during the goal pursuit process. The individuals’ strong energy is essential for persevering through the difficulties (Law & Guo, 2011, 2012; Snyder, 2000, 2002; Snyder, Lapointe, Crowson, & Early, 1998). To integrate his thought, Snyder (2000) used the equation “hope = agency + pathway” to express the reciprocal relationships among the components (p. 10). He proposed that hope will not exist without the combination of agency and pathway and that by reciprocal interaction, these two components affect each other during the goal pursuit process (Snyder, 2000).
Recently, scholars have applied hope theory in substance involvement treatment programs. One relevant study was by Koehn, O’Neill, and Sherry (2012). In their article, they introduced several hope-focused recovery intervention models, in which hope occupied a critical position in substance abuse counseling. Mathis et al. (2009) examined the impact that agency and pathway levels had on substance use abstinence among 90 new residents, both male and female, in a communal living recovery home through a follow-up of 8 months. The results showed that the levels of agency and pathway significantly predicted reported drug abstinence. In another study exploring the implications of the outcomes of a hope-focused treatment program for incarcerated women convicted of drug offences in Taiwan, the participants were 40 female drug offenders who were randomly assigned to experimental and control groups. The 20 experimental group participants received 16 sessions of hope-based substance abuse treatment, whereas the 20 control group participants were put on a waiting list for another term of treatment. The results indicated that the hope-based treatment program succeeded in fostering significant levels of hope in terms of goal setting and pursuing, adequate energy, and controlling pathway for the women who participated in treatment compared with those who did not have the chance to attend (Law & Guo, 2012). To confirm these results, in a similar study, Guo and Law (2013) investigated the effectiveness of hope-based counseling in promoting a sense of hope for incarcerated women convicted of drug offences in Taiwan. The participants, 20 women convicted of drug offences, were randomly assigned to experimental and control groups. The 10 experimental group participants received 12 sessions of hope-based substance abuse treatment while the 10 control group members did not receive any type of treatment. The results confirmed the findings of the previous research, highlighting the value of hope-based treatment for women in recovery from substance involvement.
Taylor, Feldman, Saunders, and Ilardi (2000) pointed out that the concept of hope is fundamentally cognitive in nature. Scholars have proposed theoretically that, through cognitive appraisal of the possibility of carrying out their plans to reach goals, individuals’ agency, that is, energy to reach the goal, will be strengthened. Moreover, an increase in pathway thought might be expected to boost the capacity for positive cognitive appraisal (Law & Guo, 2011; Snyder, 1989, 1994, 1995, 2000, 2002; Snyder, Harris, et al., 1991; Snyder, Irving, & Anderson, 1991; Snyder, Ritschel, Rand, & Berg, 2006). Two empirical studies in Taiwan revealed that women convicted of drug offences who practiced pathway thought in hope-based treatment had significantly increased adequate cognition in the posttest, in other words, they showed greater ability to use positive thinking in viewing recovery (Guo & Law, 2013; Law & Guo, 2012). Many scholars have explored the role of hope in cognitive-behavioral therapies and found a positive effect for this combination (Snyder et al., 2000; Taylor et al., 2000). Among several cognitive theories applied in the counseling field, it seems that the central theme of hope theory is compatible with that of choice-based reality therapy, which maintains that life is a matter of choice and that appropriate choices will intrinsically enhance motivation and hope (Glasser, 1998).
The Choice-Based Reality Therapy View on Substance Involvement
Glasser (1965, 1998) created a choice-based reality theory and proposed that a human being has five basic needs he or she is driven to fulfill, that is, survival, love, power, fun, and freedom. The need for survival refers to the search for food, shelter, and clothing; the need for love refers to seeking belonging and caring; the need for power refers to looking for recognition and worth; the need for fun refers to looking for enjoyment and pleasure; the need for freedom refers to allowing for autonomy and choice. Furthermore, Glasser indicated that each person starts creating a vision of his or her quality world at birth and continues throughout life. Into this quality world, people instill their own ideals about people, experience, and the belief systems that govern their behavior.
Choice-based reality theory proposes that human behavior is composed of action, thinking, feeling, and physiology, and the aggregate is referred to as total behavior. In choice theory, a car is often used to describe total behavior, with the two front wheels identified as action and thinking and the two back wheels as feeling and physiology. Just as in most cars the driving direction is controlled by the front wheels, a human being is more likely to make choices through action and thinking than through feeling and physiology (Corey, 2013; Wubbolding & Brickell, 2009a). Sadly, an individual may develop negative symptoms in total behavior when his or her basic needs remain unfulfilled due to traumatic or harmful experiences. For instance, individuals engaging in negative behavior that is harmful to themselves or others, for example, involvement in substance usage, may subsequently think themselves powerless and become emotionally disturbed. Moreover, physical symptoms may also manifest as a result of continued substance usage. Finally, the substance usage becomes such an integrated component of the person’s quality world that it is seen as essential to fulfillment of his or her needs. The individual may fulfill these needs by using drugs with friends to fulfill his or her need for love, belonging, and fun (Wubbolding, 2011a, 2011b) and letting the powerful stimulation of the drug fulfill the need for freedom (Mottern, 2002).
Finding Hope Through Choice-Based Reality Therapy
To help substance-involved individuals find hope, choice-based reality therapy was designed with a focus on teaching them to understand what their needs are and how to fulfill those needs through appropriate choices (Mottern, 2002), to be responsible for their own choices (Glasser, 1965, 1998; Moore, 2001; Wubbolding, 2011a), and to set priorities among their needs through the WDEP evaluation system (Wubbolding, 2000, 2011a). In this system, W stands for wants, D stands for doing, E stands for evaluation, and P stands for plan. More specifically, the therapist asks individuals to clarify and prioritize their wants to help them in setting goals. Next, the therapist asks individuals where their current choices are taking them and to evaluate whether their current choices are taking them where they want to go to assist them in gaining energy for goal pursuit through an increased sense of self-control. Finally, the therapist asks individuals to make an effective plan to fulfill their wants to assist them in gaining confidence in their pathway planning (Glasser, 1990; Law & Guo, 2014, 2015; Wubbolding, 1990).
Setting Goals Through Prioritizing Wants
Snyder (2000) cited a line from a poem of Coleridge titled “Work Without Hope”: “Hope without an object cannot live” (p. 9). More specifically, hope has to be goal-directed; goals serve as mental targets that human beings have set up to guide their behavior (Guo & Law, 2013; Law & Guo, 2011, 2012; Snyder, 1989, 1994, 1995, 2000, 2002; Snyder, Harris, et al., 1991; Snyder, Irving, et al., 1991; Snyder et al., 2006). In one study, substance-involved clients who were receiving services identified allowing them to make their own choices and set their own goals as an important priority (De Maeyer, Vanderplasschen, & Broekaert, 2009).
To assist clients in establishing their goals, a choice-based reality therapist usually starts a counseling session with the question “What do you want?” Through this type of question, a therapist can assist clients to discover their wants and preferences, which usually reflect their basic needs and the picture of a quality world for each of them. Choice-based reality therapy stresses that, after clarifying and prioritizing their basic needs, clients will be able to make better choices and set up a workable goal (Corey, 2013; Glasser, 1990; Wubbolding, 1990, 2000, 2011a, 2011b; Wubbolding & Brickell, 2009a, 2009b).
Scholars have found that allowing substance-involved clients to participate and make decisions in setting up treatment goals can successfully enhance the clients’ ability to self-regulate healthy behavior, make a commitment to the treatment goal, find the motivation to work toward recovery, and even to reduce substance usage (Boisvert, Martin, Grosek, & Clarie, 2008; Groshkova, 2010; Simoneau & Bergeron, 2003; Wild, Cunningham, & Ryan, 2006). Even when participants were under mandatory treatment, promoting strong internalized motivation has been found to be the key to better attendance and retention in treatment (Ryan, Plant, & O’Malley, 1995). Similarly, studies have found that when participants are allowed to become involved in setting goals, the resulting increase in motivation leads to a greater willingness to seek help (Wild et al., 2006). Although there are few studies in regard to drug treatment specifically for women convicted of drug offences, one empirical study by Law and Guo (2014) deserves attention. They conducted a choice-based reality treatment program in a correctional setting in Taiwan; the participants were 48 women convicted of drug offences, who were randomly assigned to equal-sized experimental and control groups. The results of the study revealed that in contrast to the control group members, members of group who received the choice-based reality therapy showed a significantly clearer understanding of their needs and future goals for recovery.
Gaining Adequate Energy Through Evaluation of Action
Scholars have noted that individuals with a better sense of self-control had higher motivation to enter treatment after detoxification (Kelly, Deane, McCarthy, & Crowe, 2011; Wills & Stoolmiller, 2002). Packer, Best, Day, and Wood (2009) revealed that among participants in a court-mandated treatment program, those with greater self-control showed significantly less intensity in continuation of substance use. Thus, even though setting goals is given first priority in the counseling process, to reach their goals, it is essential that individuals have sufficient motivation and sense of self-control for goal attainment (Guo & Law, 2013; Law & Guo, 2011, 2012; Snyder, 1989, 1994, 1995, 2000, 2002; Snyder, Harris, et al., 1991; Snyder, Irving, et al., 1991; Snyder et al., 2006).
To enhance individuals’ sense of self-control and increase their energy in pursuing goals, the choice-based reality therapist challenges clients with questions, asking, “What are you doing?” and “Will what you are currently doing take you to where you want to go?” Through such questions, the therapist aims to help clients become aware of what they are doing, evaluate how what they are doing affects other aspects of their total behavior, and then consider how altogether this might influence their goal pursuit behavior (Corey, 2013; Glasser, 1990; Wubbolding, 1990, 2000, 2011a, 2011b; Wubbolding & Brickell, 2009a, 2009b). Through this process, clients are able to move their sense of self-control from the external to the internal and to increase the likelihood that they will carry out their responsibility. After all, personal growth will not occur unless clients are willing to make a commitment to make changes in their actions (Corey, 2013; Law & Guo, 2011; Wubbolding & Brickell, 2009b).
A variety of empirical studies have shown the effectiveness of choice-based reality treatment in helping clients gain energy and an increased sense of self-control for working toward substance recovery goals. Xu (1984) and Hsiao (1997) found that after choice-based reality treatment, juvenile delinquents with substance abuse charges in Taiwan were significantly improved in their willingness to assume responsibility for their recovery. Law and Guo (2014) reported that Taiwanese women convicted of drug offences reported an increased sense of self-control in their ability to overcome obstacles and set up plans to pursue their goals after participation in a choice-based reality substance treatment program. Furthermore, the women who received treatment also reported greater persistence in overcoming obstacles and following their plans to reach those goals for recovery after the treatment.
Controlling Pathway Through Action Planning
Tillich (1965) reminded, “Hope is easy for the foolish, but genuine hope is something rare and great” (p. 17); scholars have emphasized that helping clients build up workable pathways is essential for enhancing the sense of hope (Guo & Law, 2013; Law & Guo, 2011, 2012; Snyder, 1989, 1994, 1995, 2000, 2002; Snyder, Harris, et al., 1991; Snyder, Irving, et al., 1991; Snyder et al., 2006). To help individuals set up workable pathways and enhance a sense of self-confidence, the choice-based reality therapist encourages clients not only to set up a goal and develop a plan to fulfill their wants and needs but also to explore how much confidence they have in their ability to carry out this action plan. They are taught that characteristics of an effective plan should follow the principles of SAMIC,3 which refers to a plan’s being simple, attainable, measurable, permitting immediate involvement, and controlled by the clients through their commitment and consistent behavior (Wubbolding, 2000, 2007, 2008, 2011a, 2011b).
Hammerley, Cavelle, and Forayth (1992) confirmed that choice-based strategies could enable adolescent drug offenders to build up self-confidence in their ability to solve problems. According to Law and Guo (2015), after choice-based reality treatment, Taiwanese women convicted of drug offences showed significant improvement in belief in their ability to undertake the necessary actions and change in behavior to move toward a desired outcome in decision-making, coping, and social skills, and planning ability. In other words, when women convicted of drug offences were more confident that they had the ability to choose and create helpful behavior, their motivation for goal pursuit was likely to increase as a result.
Overview of the Present Study
Continuation of the high percentage of incarcerated women convicted of drug offences in Taiwan has presented an urgent need for developing treatment programs for this population (Ministry of Justice, 2010, 2014a, 2014b). Empirical evidence from research in Taiwan has shown that finding hope is a critical factor for substance involvement recovery (Guo & Law, 2013; Law & Guo, 2012). Furthermore, although not using the same terminology, some empirical evidence has revealed that hope-related variables, such as understanding their needs and future goals, persistence in overcoming obstacles, sense of self-control in goal pursuing, and self-confidence in their ability to undertake the necessary actions, and so on, have been shown to be strengthened through choice-based reality therapy (Hsiao, 1997; Law & Guo, 2014, 2015; Xu, 1984). The HELP model developed by Pound and Duchac (2009) is one example of a treatment program which includes hope, evaluation, teaching/learning, and a WDEP action plan in one model. Throughout our literature review, one can sense that many of the studies along this line remain on the level of theoretical description; to our knowledge, there are very few empirical studies that examine the effectiveness of choice-based reality therapy in strengthening hope in terms of goal setting and pursuing, adequate agency, and controlling pathway in substance involvement treatment in either the United States or Taiwan. Thus, this study was structured as a two-group pretest and posttest group design to investigate this matter. Building upon the available evidence, this study has developed a 12-session choice-based reality drug treatment program for women convicted of drug offences. It was hypothesized that this program would help strengthen the prospect of recovery for women convicted of drug offences in Taiwan through enhancement of their hope in terms of goal setting and pursuing, adequate energy, and controlling pathway.
Method
Participants
Although Corey (2012) suggested that “eight members with one leader seems to be a good size” for group counseling, the authors also had to consider the need for a larger sample size for statistical effectiveness (p. 75). As two counselors would be co-leading the group in this study, the authors decided that a maximum of 22 members for each group would promote effective interaction between counselors and participants and allow statistical accuracy. To ensure that the population of the research site was well represented, 44 women convicted of drug offences were randomly selected to participate in this study. A consent form which indicated that participation was voluntary and that individuals had the right to opt not to participate in the research study or to withdraw from the study any time they wished was distributed prior to the data collection. Once the participants signed and turned in the consent forms to show their agreement to participate, they were randomly assigned into experimental and control groups, with 22 women in each group.
The ages of the participants in the experimental group ranged from 18 to 41 years (M = 30 years), and their first instance of drug use occurred at an average age of 15 years. Regarding their marital status, 43% were single, 24% were married, and 33% were divorced. Fifty percent of them had children. In regard to their educational background, 78% of them were middle school graduates, and 22% were senior or vocational high school graduates. Concerning their last employment prior to arrest, 23% reported self-employment, 33% were in service occupations, 24% were engaged in prostitution, and 20% reported being housekeepers or that they had no jobs. Drug-related offences were their major or only offences. Eighty percent had records as previous offenders, while 20% were first offenders. Eighty-two percent reported that their drug of choice was an Amphetamine; the average age of their first drug usage was 23. The average years of drug usage was 7.1.
For the participants in the control group, the ages ranged from 17 to 41 years (M = 31 years), and their first instance of drug use occurred at an average age of 16 years. Regarding their marital status, 44% were single, 23% were married, and 33% were divorced. Fifty-two percent of them had children. In regard to their educational background, 80% of them were middle school graduates, and 20% were senior or vocational high school graduates. Concerning their last employment prior to arrest, 22% reported self-employment, 34% were in service occupations, 24% were engaged in prostitution, and 20% reported being housekeepers or that they had no jobs. Drug-related offences were their major or only offences. Seventy-nine percent had been previous offenders, while 21% were first offenders. Eighty-three percent reported that their drug of choice was an Amphetamine; the average age of their first drug usage was 24. The average years of drug usage was 6.9. To examine whether there were differences between the two groups in the distribution of each demographic variable, a chi-square test of independence was used in this study for data analysis at a significance level of .05. As none of the chi-square values of the demographic variables reached the level of significance (p > .05), this result confirmed the homogeneity between the two groups.
Measurement
This study used the Hope Index for Substance Abuse Offender Recovery (HISAOR), which was developed by the authors in preparation for the present study (Law & Guo, 2012), to measure participants’ ability in goal setting and their motivation and pathway planning for recovery. The development of the HISAOR was based upon the theoretical structure presented in previous research studies (Snyder, 1994, 2000). Ratings for all 20 questions are made on a variation of a Likert-type scale, with responses ranging from 1 (strongly disagree), 2 (disagree), 3 (slightly disagree), 4 (slightly agree), 5 (agree), to 6 (strongly agree). To test the validity of this scale, 153 women convicted of drug offences served as the pilot run sample; a factor analysis was conducted to test the construct validity of this inventory. The ages of the pilot sample ranged from 19 to 50 (M = 38). Among them, 47% were single, 19% were married, and 34% were divorced. As for educational background, 85% of the participants were middle school graduates and 15% were senior high school or vocational high school graduates. The average age for their first incidence of drug use was 15. Bartlett’s test of sphericity was utilized to test the factorability of the pilot data set. The results were shown to be significant (p < .001), and the Kaiser–Meyer–Olkin (KMO) Measure of Sampling Adequacy (MSA) was .936, indicating that factor analysis was appropriate for these data. The principal component analysis (PCA) used for factor extraction revealed that when three factors with eigenvalues >1 were extracted, these factors could account for 71.420% of the variance; the factor loading of each item was between .485 and .831. The results of factor loading after varimax rotation are shown in Table 1.
The Results of Factor Loading of HISAOR After Varimax Rotation.

Note. The instrument items were originally written and used in this study in Mandarin Chinese. They have been informally translated into English for use in this article. HISAOR = Hope Index for Substance Abuse Offender Recovery. GSP = Goal Setting and Pursuing. AE = Adequate Energy. CP = Controlling Pathway.
The extracted factors were labeled Goal Setting and Pursuing, Adequate Energy, and Controlling Pathway. The subscale of Goal Setting and Pursuing assesses the participants’ ability in setting goals and overcoming obstacles and their persistence in pursuing the goals they have set up. The subscale of Adequate Energy assesses the participants’ sense of control in their ability to carry out the plan to attain the goal. The subscale of Controlling Pathway assesses the participants’ confidence in their ability to set up pathways based on their goals. The Cronbach’s alpha coefficient of the whole inventory was .976; the coefficients for each subscale were Goal Setting and Pursuing, .958; Adequate Energy, .881; and Controlling Pathway, .955. Based on the guidelines of Ornum, Dunlap, and Shore (2008), this instrument has very good reliability in conducting measurement.
Then, responses of another group of 150 women convicted of drug offences were used to further validate the scale, and the structural equation model was utilized to reconfirm the three-factor model and the reliability of the instrument. The ages of the subjects ranged from 20 to 52 (M = 39). Among them, 46% were single, 18% were married, and 36% were divorced. As for educational background, 83% were middle school graduates, and 17% were senior high school or vocational high school graduates. The average age for their first incidence of drug use was 16. The goodness-of-fit indices and Cronbach’s alpha coefficients based on this analysis can be found in Table 2.
Confirmation Testing Results of HISAOR.
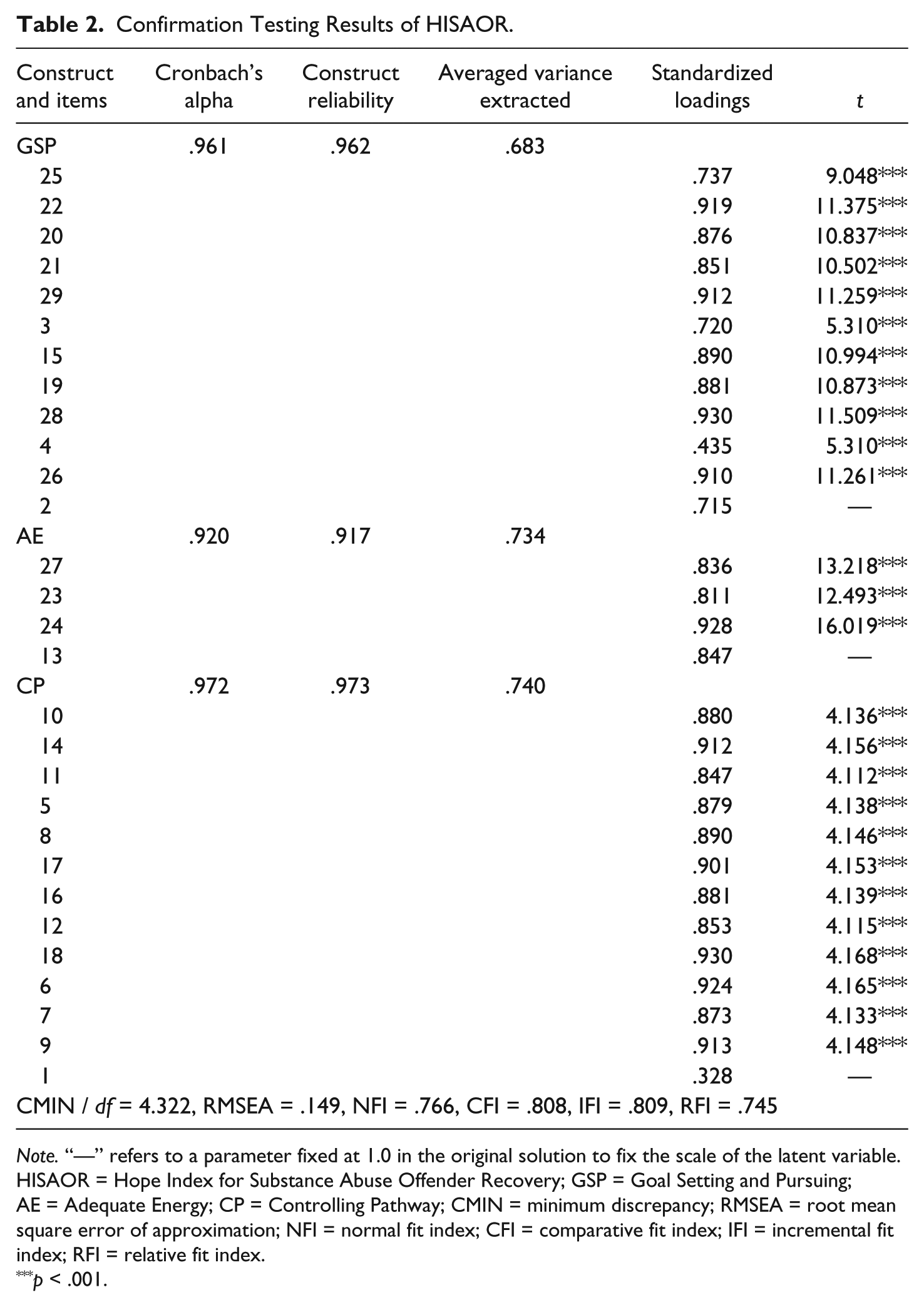
Note. “—” refers to a parameter fixed at 1.0 in the original solution to fix the scale of the latent variable. HISAOR = Hope Index for Substance Abuse Offender Recovery; GSP = Goal Setting and Pursuing; AE = Adequate Energy; CP = Controlling Pathway; CMIN = minimum discrepancy; RMSEA = root mean square error of approximation; NFI = normal fit index; CFI = comparative fit index; IFI = incremental fit index; RFI = relative fit index.
p < .001.
According to guidelines suggested by scholars (Byrne, 2001; Kline, 2005), the values of minimum discrepancy (CMIN) / df, root mean square error of approximation (RMSEA), normal fit index (NFI), comparative fit index (CFI), incremental fit index (IFI), and relative fit index (RFI) indicated only a moderate to reasonable model fit; however, the convergent validity was supported by the evidence that all t values for each indicator were significant and 18 of the 20 standardized loadings were greater than .50 (Hair, Black, Babin, Anderson, & Tatham, 2010). The average variance extracts were .683, .740, and .734. The Cronbach’s alpha coefficient for the whole scale was .986; the coefficients for the subscales were GSP (.961), AE (.920), and CP (.972), indicating that each factor had excellent reliability (Ornum et al., 2008). The results of the confirmatory factor analysis revealed that the model was a good fit and confirmed that the selected items could be properly explained by the three latent factors.
Procedure and Research Design
Prior to conducting the research, the authors sought approval and permission from the first author’s Institutional Review Board and the research site, a female correctional institution in central Taiwan. Upon approval from both institutions, the choice-based reality therapy substance-involved treatment program was conducted to test the research hypotheses. To recruit participants for the research, 44 women convicted of drug offences were randomly selected from among inmates who had been mandated to complete a treatment program during incarceration. A consent form describing the study was distributed to the participants; the form indicated that their participation in this study would be voluntary. To show their agreement to participate, they were asked to sign and turn in the consent forms. Each of those who agreed to participate was required to take a pretest in a group setting. The pretest was a pencil–paper test consisting of demographic-background items and the HISAOR.
To strengthen the internal validity of the study by ensuring that changes in the participants’ scores resulted from the treatment itself and were not due to history, maturation, testing effect, and so on, this study adopted a two-group pretest and posttest control group design to test the research hypotheses (Spata, 2003). To maximize the homogeneity between the two groups, after completion of the pretest, each participant was randomly assigned to one of the groups. The experimental group members received the choice-based reality treatment, which was one 2-hour session per week for a total of 12 sessions. The control group members were put on a waiting list for the same treatment program in another term, with no treatment for the duration of the research. Upon the experimental group’s completion of the 12th session of the treatment, both groups took the HISAOR at the same time as a posttest. The scales took approximately 15 min to complete in a self-administered style. Prior to data collection, the participants were informed that the collected data would be kept confidential and that their names would not be included in any form in the research report. The drug treatment was conducted in the participants’ native language, Mandarin Chinese. The participants received no compensation for their time.
Treatment program
The first author of the study designed the 12 sessions of the choice-based reality substance involvement treatment program based on the work of Law and Guo (2012, 2014, 2015) and Glasser and Wubbolding (1995). The treatment modality for the group was a structured format, as described in the following paragraphs.
Stage 1: Setting goals based on needs and wants
Setting up a goal to serve as a mental target to guide behavior forward and committing to follow through are important elements to enhance hope. Based on this perspective, two sessions were designed to help the participants in setting goals for recovery through exploration of their wants and needs.
Sessions 1 and 2
What do I want in my life and from this treatment? The group leader introduced the construct of the five basic needs, the concept of a quality world, and the transtheoretical model of motivation (DiClemente & Prochaska, 1998). Then, participants shared their past experiences at each stage of recovery and identified their goals for recovery in terms of basic needs and a quality world. Participants stated their commitment to working toward those goals.
Stage 2: Gaining adequate energy through action evaluation
Individuals’ motivation and sense of self-control over their capacity to pursue a goal are essential to goal attainment. Thus, the four sessions in this stage were designed to help empower participants in these areas.
Session 3
What are you doing? The participants used a picture of a car, which is often used as a metaphor to portray total behavior, to describe their current thought and action and the impact of their current thought and action on their feeling and physiology.
Sessions 4 and 5
Where are you going in life and in recovery? The participants used the total behavior they described in the previous session to evaluate how effective their current performance was in leading them toward their life and recovery goals and to identify any changes necessary to increase the likelihood of goal attainment.
Session 6
Can my dream come true? The participants were asked to list their abilities on a picture of a lighthouse, with the explanation that the more abilities the participants were able to list, the greater their sense of being in control would be and the more energy they would have in their effort toward recovery. Then, participants shared their work and made a commitment for recovery goal achievement.
Stage 3: Controlling pathway through action planning
To enhance hope, it is essential to help clients build up a workable pathway and plan and to find the confidence to take action. The last six sessions were designed to fulfill these purposes.
Session 7
How did I get there? The group leader helped members build up confidence through sharing their past experiences of success and exploring how their planning, commitment, and choices had affected the results.
Sessions 8 and 9
How can I get to my life and recovery goal from here? The participants were encouraged to make an action plan for life and for recovery. Then they made statements of commitment to reflect their willingness to take responsibility for their plans and action.
Sessions 10 and 11
How can I overcome barriers? The participants were taught self-assertiveness, stress management, and coping skills that could empower them to reject the temptation to misuse substances.
Session 12: Feedback
The group leader introduced the concept that hope equals pathway plus agency. Participants shared observations about their sense of hope in regard to the entire process of recovery and their commitment to pursue a life without substance abuse.
Statistical Analysis
ANCOVA was used to compare changes in the scores of the two groups in each subscale of the HISAOR to evaluate the effectiveness of the choice-based reality drug treatment program in promoting the sense of Hope (i.e., Goal Setting and Pursuing, Adequate Energy, Controlling Pathway) in women convicted of drug offences. ANCOVA was chosen due to the nature of the pretest and posttest experimental design of this research. Pretest effect could potentially affect the internal validity of the study (Spata, 2003), and it has been suggested that ANCOVA can be “used to increase the precision of a model fit when an uncontrollable but observable nuisance variable has an impact on the response variable” (Silknitter, Wisnowski, & Montgomery, 1999, p. 303). Thus, ANCOVA would be an appropriate tool to handle this limitation. Prior to analysis with ANCOVA, homogeneity within the regression coefficient was tested using the pretest scores on each of the HISAOR subscales. For those data meeting the requirement for homogeneity within the regression coefficient, the ANCOVA would be conducted in further analysis. The pretest scores of each subscale of the HISAOR from both groups would serve as the covariates. The posttest scores on each subscale for the two groups would be used to detect the differences between the groups. The significant alpha level was set at .05.
Results
Forty-four participants, none of whom dropped out of the treatment program during the research period, participated in this research. The same number of participants took the pretest and posttest. The means and standard deviations of the pretest and posttest scores for each subscale of the HISAOR are shown in Table 3.
Sample Size, Mean, and Standard Deviation of Pretest and Posttest Scores of the HISAOR.
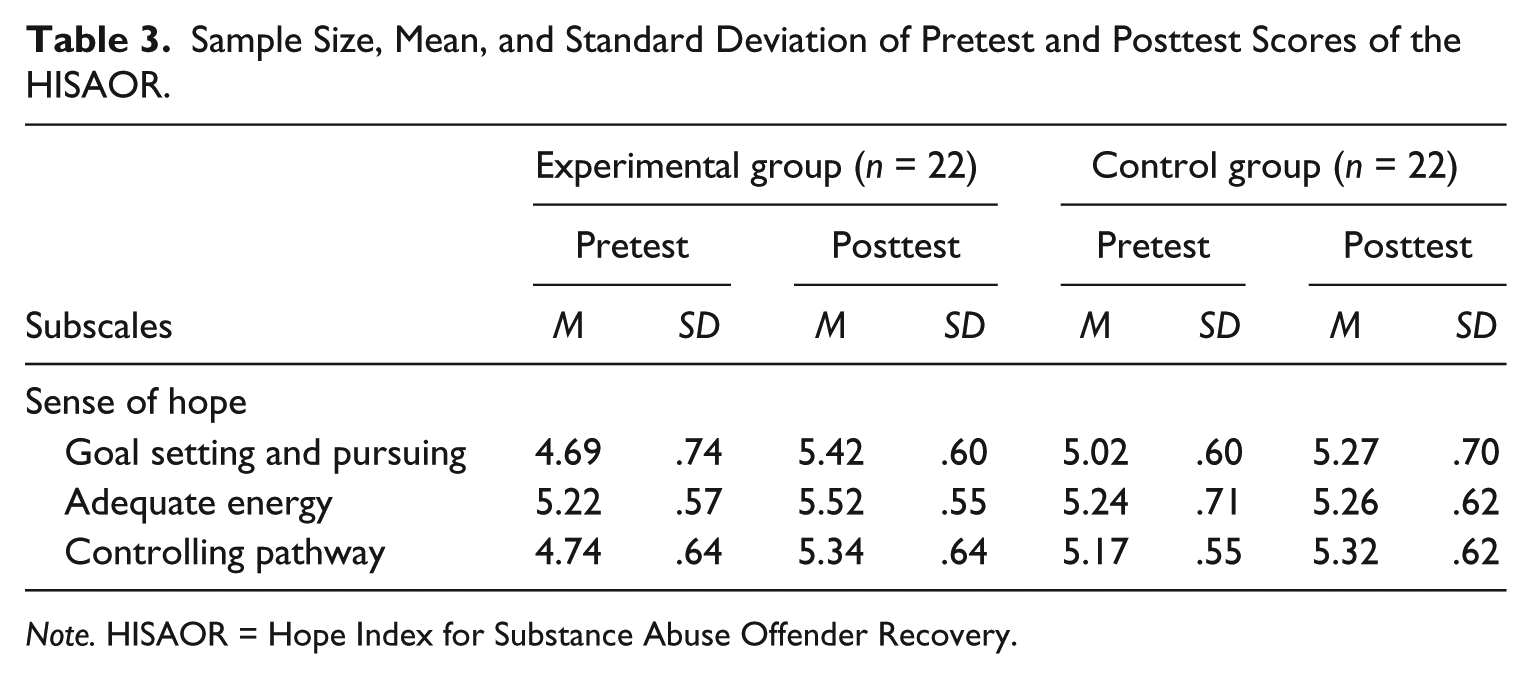
Note. HISAOR = Hope Index for Substance Abuse Offender Recovery.
Prior to analysis with ANCOVA, the homogeneity within the regression coefficient was tested for each subscale of the HISAOR; the results showed that there was no significant interaction between the groups in the pretest scores for Goal Setting and Pursuing (F = 3.183, p > .05, partial η2 = .074), Adequate Energy (F = .015, p > .05, partial η2 = .000), or Controlling Pathway (F = .677, p > .05, partial η2 = .017; see Table 4). This was an indication that the data met the requirement for homogeneity within the regression coefficient so that ANCOVA was appropriate for use in further analysis. The results of ANCOVA for the three subscales of the HISAOR and estimates of effect size by partial eta square are shown in Table 5.
ANCOVA Summary for Homogeneity Within the Regression Coefficient of the HISAOR.
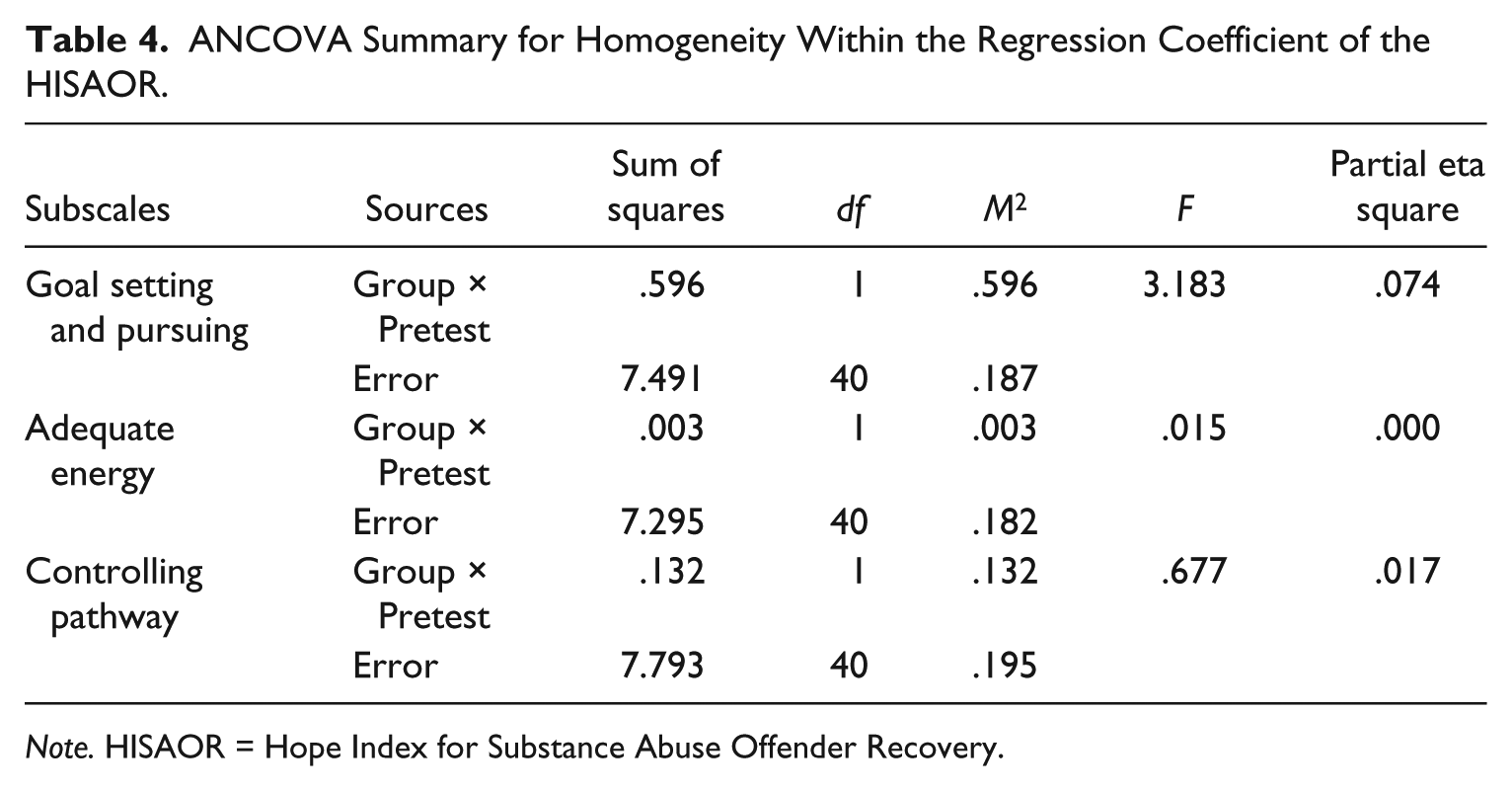
Note. HISAOR = Hope Index for Substance Abuse Offender Recovery.
Results of ANCOVA for the Three Subscales of the HISAOR.
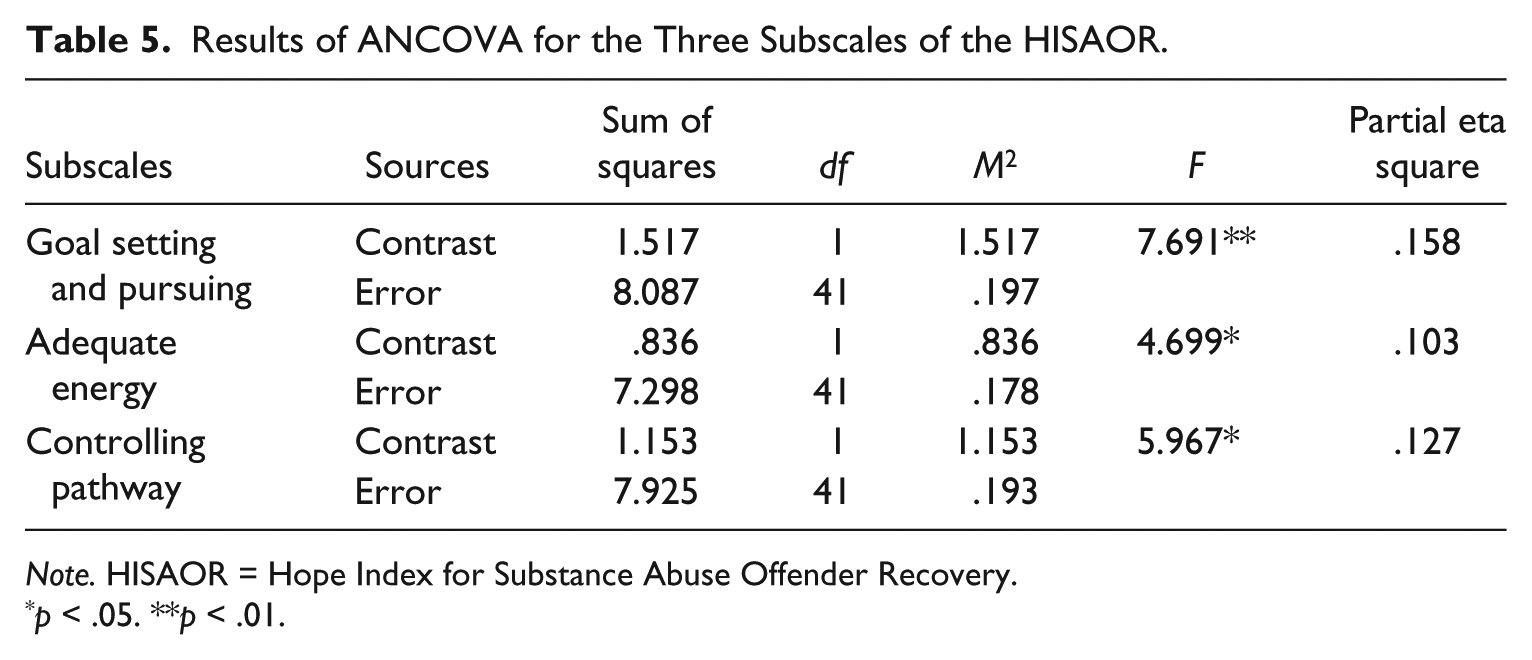
Note. HISAOR = Hope Index for Substance Abuse Offender Recovery.
p < .05. **p < .01.
As the results in Table 5 indicate, after significant adjustment by the covariates of the pretest scores for the three variables, there were significant differences between the members of the two groups in the posttest scores for Goal Setting and Pursuing (F = 7.691, p < .01, partial η2 = .158), Adequate Energy (F = 4.699, p < .05, partial η2 = .103), and Controlling Pathway (F = 5.967, p < .05, partial η2 = .127). The experimental group had significantly higher scores for Goal Setting and Pursuing, estimated marginal means = 5.532; Adequate Energy, estimated marginal means = 5.530; and Controlling Pathway, estimated marginal means = 5.501, as compared with the control group’s scores of estimated marginal means = 5.150, 5.254, and 5.156, respectively. These results suggest that, compared with those participants who had not received treatment, the participants who had received choice-based reality substance involvement treatment had higher levels of hope, as reflected in their scores in Goal Setting and Pursuing, Adequate Energy, and Controlling Pathway, for working toward their recovery. Furthermore, effect size values (η2 = .158, .103, and .127) suggested a moderate practical significance.
Discussion
Hope theory emphasizes that setting up a goal is essential in promoting recovery (Guo & Law, 2013; Law & Guo, 2011, 2012; Snyder, 1989, 1994, 1995, 2000, 2002; Snyder, Harris, et al., 1991; Snyder, Irving, et al., 1991; Snyder et al., 2006). The theory behind choice-based reality therapy stresses that, through clarifying and prioritizing their wants, clients will be able to make better choices and set up workable goals (Corey, 2013; Glasser, 1965, 1990, 1998; Wubbolding, 1990, 2000, 2011a, 2011b; Wubbolding & Brickell, 2009a, 2009b). Empirical evidence from a study by Law and Guo (2014) revealed that in contrast to members of the control group, women convicted of drug offences in the group that received choice-based reality treatment showed a significantly clearer understanding of their needs and future goals for recovery. Based on these principles and the corroborating evidence, two sessions of the choice-based reality treatment program we developed were designed to help Taiwanese women convicted of drug offences learn to make healthy choices for their life and recovery goals. It was hypothesized that this treatment program would strengthen the participants’ hope by increasing their capacity in setting up and pursuing goals. In line with previous research from Taiwan (Law & Guo, 2014), the evidence provided in the present study indicates that this expectation was fulfilled. The Taiwanese women convicted of drug offences who completed the treatment program reported that their levels of hope, as measured in their ability in setting goals and their persistence in pursuing the goals they had set up and overcoming obstacles in the process, had significantly increased compared with the levels of hope of participants who had not yet had treatment.
Having motivation and a belief that they are in control of the effort to reach the goal is another important element of hope (Guo & Law, 2013; Law & Guo, 2011, 2012; Snyder, 1989, 1994, 1995, 2000, 2002; Snyder, Harris, et al., 1991; Snyder, Irving, et al., 1991; Snyder et al., 2006). Choice-based reality therapy emphasizes that helping clients become aware of what are they doing and encouraging them to evaluate how their actions and choices affect their total behavior will enable them to make more effective decisions, and this, in turn, may have an impact on their goal attainment (Corey, 2013; Wubbolding, 1990, 2000, 2011a, 2011b; Wubbolding & Brickell, 2009a, 2009b). Accordingly, four sessions of our choice-based treatment program were designed to enhance Taiwanese women convicted of drug offences’ sense of self-control in choosing and creating behavior that would promote recovery. Corresponding to these sessions, it was hypothesized that after treatment the participants’ hope, as measured in the adequacy of their energy to pursue recovery goals, would be significantly increased. Consistent with previous research from Taiwan (Law & Guo, 2014), this expectation was fulfilled in the evidence provided by the present study. Compared with the responses of those who had not yet attended the program, upon completion of the choice-based reality therapy for substance involvement, Taiwanese women convicted of drug offences reported a significantly higher level of energy for recovery.
Building up a workable pathway is essential for enhancing the sense of hope (Guo & Law, 2013; Law & Guo, 2011, 2012; Snyder, 1989, 1994, 1995, 2000, 2002; Snyder, Harris, et al., 1991; Snyder, Irving, et al., 1991; Snyder et al., 2006). Choice-based reality therapy emphasizes the importance of encouraging clients to develop a plan to fulfill their wants and needs (Corey, 2013; Wubbolding, 1990, 2000, 2011a, 2011b; Wubbolding & Brickell, 2009a, 2009b) and empowering their sense of self-confidence in carrying out the plan (Law & Guo, 2015). Based on this perspective, the aim of six sessions in the choice-based reality substance involvement treatment is to encourage clients to explore how they can exercise control over their goals and to develop and modify an action plan. Consistent with previous research from Taiwan (Law & Guo, 2014), the women convicted of drug offences who completed the choice-based reality treatment program reported significantly greater hope, as measured in their ability to set up pathways based on their goals, than those who had not yet attended the program.
Conclusion
As this is a pioneering study in this line of investigation, the findings are a useful contribution to the practical framework and literature supporting choice-based reality treatment for women convicted of drug offences, especially in Taiwan. However, there are several limitations of the study that deserve mention. In addition, some recommendations for further research that would address these limitations are offered.
Limitations and Recommendations for Further Study
The first limitation is that, due to the lack of empirical evidence in this line of research, the literature review and framework building relied heavily on supporting studies from the theoretical perspective. Although the findings of the present study comprise a significant contribution to the drug treatment field in Taiwan, further study in related areas will be necessary. The second limitation, regarding the sampling, is that because the participants were selected from only one institution, the sample cannot be said to be representative of the nationwide population of women convicted of drug offences in Taiwan. More studies applying this model to female substance-involved inmates who have been convicted of other offences and women convicted of drug offences in different institutions would provide important confirmation of the results. Likewise, additional studies involving application of the same treatment model to male substance-involved offenders could be conducted to assess the relevance of this treatment program for them. The third limitation is in regard to sample size. For group counseling, a small number of participants have been strongly recommended (Corey, 2012), and this is the general practice in substance-involved treatment programs in correctional settings (Pearson & Lipton, 1999). Nevertheless, the purpose of this study was to detect the significant differences between experimental and control groups, and there is some concern that the small group size may diminish the statistical power of the results. For future study, an increased sample size would be desirable if the appropriate counselor/client ratio can be maintained (Sheppard, 1999). Furthermore, the complexity of the substance-related recovery experience might be difficult to capture through an objective scale; therefore, use of objective scales to collect behavioral data related to changes in knowledge, cognition, and action might be considered another limitation of this study.
To maximize the accuracy of the data, adding qualitative strategies such as open-ended questions, face-to-face interview, observation records, and so on, for data collection in further study would be desirable. Furthermore, as the study was conducted in a correctional setting, it may have been difficult for inmates to display their true insights as they may have felt embarrassed about admitting weakness or been concerned that their personal information could be used against them in court. Thus, self-report bias could be considered a potential limitation of this study. To maximize the accuracy of the responses, the participants’ self-report data were handled in a confidential manner, participants were randomly assigned into two groups, a pretest and posttest control group design was used, and ANCOVA was used for data analysis. It is our hope that through this effort, the self-report bias was minimized. Nevertheless, overall, the effect size values suggest a moderate practical significance, and interpreting and generalizing the results to the wider population should be viewed with caution.
Policy Implications
Hopelessness has been identified as a potential factor contributing to substance-involved behavior among females (Hiebert-Murphy & Woylkiw, 2000; Hien et al., 2005; Koenig, 2004; Najavits et al., 2004; Nyamathi et al., 2001; Peterson et al., 2002; Wu et al., 2003); related research has shown that hopelessness blocks confidence in recovery and puts recovering users at greater risk of relapse after treatment (Grella et al., 2003). Furthermore, a tendency toward overreliance on substances can prohibit substance-involved females from developing positive pathways for coping and assuming responsibility for their actions (Pelissier & Jones, 2006; Washington, 2001). However, despite the potential for more successful treatment suggested by this line of research and the rising number of women convicted of drug-related crimes, only a few treatment programs have been focused specifically on empowering hope in the treatment of female drug-related offenders. The findings of this preliminary study highlight the value of choice-based reality therapy in enhancing hope of recovery for women convicted of drug offences.
Regarding the problem of recidivism among drug offenders, Ryan et al. (1995) discovered that, even when women convicted of drug offences were under mandatory treatment, enhancing internal motivation was the key to better retention in treatment. Although there is no empirical evidence to support a predictive role for hope in regard to recidivism of drug offenders, a study of domestic violence offenders by Lee, Uken, & Sebold (2007) highlighted the value of setting self-determined goals through prioritization of wants in predicting reduced recidivism. It will be necessary to continue from this pioneering investigation with further research in related areas, but the findings of the present study comprise a significant contribution to the establishment of a substance abuse treatment program for women convicted of drug offences in the correctional system of Taiwan. Upon attainment of appropriate confirmation for this approach, the authors recommend use of choice-based reality treatment programs for rehabilitation of this population that focus on empowering women’s sense of hope in terms of goal setting and pursuing, adequate energy, and controlling pathway as a means of alleviating strain on the criminal justice system by reducing relapse and recidivism rates. Moreover, implementation of this program would mean constructive attention for a population which has had limited resources and would have other potentially beneficial short- and long-term outcomes, such as reduced drug usage and enhancement of the recovery and well-being of women who have been convicted of drug offences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.