
Abstract
The present study aims at validating the German version of the Structured Assessment of PROtective Factors (SAPROF) for violence risk in a representative sample of incarcerated adult male sexual offenders. Sexual offenders (n = 450) were rated retrospectively with the SAPROF using the database of the Federal Evaluation Centre for Violent and Sexual Offenders (FECVSO) in the Austrian Prison System. Interrater reliability and predictive validity of the SAPROF scores concerning desistance from recidivism were calculated. Concurrent and incremental validity were tested using the combination of the SAPROF and the Sexual Violence Risk–20 (SVR-20). Interrater reliability was moderate to excellent, and predictive accuracy for various types of recidivism was rather small to moderate. There was a clear negative relationship between the SAPROF and the SVR-20 risk factors. Whereas the SAPROF revealed itself as a significant predictor for various recidivism categories, it did not add any predictive value beyond the SVR-20. Although the SAPROF itself can predict desistance from recidivism, it seems to contribute to the risk assessment in convicted sexual offenders only to a limited extent, once customary risk assessment tools have been applied. Implications for clinical use and further studies are discussed.
Although standardized approaches of assessing risk for recidivism in sexual offenders have made great progress during the last two decades, most assessment tools still focus on risk factors, and thus neglect protective factors, which might be important for risk management as well. Rogers (2000), therefore, argued that an enumeration of risk factors alone would not only be insufficient but also biased because such an approach ignores the effect of protective factors. Furthermore, focusing on protective factors might not only improve risk assessment but could also help clients to achieve desistance from reoffending and improve their own quality of life (Marshall, Marshall, Serran, & Fernandez, 2006). In their Good Lives Model (GLM) of rehabilitation, Ward and colleagues (Ward & Brown, 2004; Ward, Mann, & Gannon, 2007; Ward & Stewart, 2003) suggested that the goal of any treatment should be to provide offenders with constructive suggestions for a fulfilling life and to explore personal needs and goals in their lives rather than to solely focus on the deficits of an individual. Therefore, identifying empirically supported risk and protective factors in the individual might be beneficial for successful interventions in offenders.
Starting with Clayton, Leukefeld, Donohew, Bardo, and Harrington (1995), researchers have emphasized the importance of an empirical evaluation of changeable and treatment-oriented factors, which could counteract risk factors (Gendreau, Little, & Goggin, 1996; Quinsey, Jones, Book, & Barr, 2006; Rogers, 2000). The definition of protective factors, however, still varies markedly among different researchers. Some studies have conceptualized protective factors as absent risk factors (Zagar, Busch, Grove, & Hughes, 2009) or as the opposite end of risk factors (Webster, Martin, Brink, Nicholls, & Desmarais, 2009). However, other researchers have argued that any factors with risk-reducing effects should be considered as protective (de Vogel, de Ruiter, Bouman, & de Vries Robbé, 2009). Moreover, some researchers seem to agree that protective factors either function as predictors for desistance from recidivism by themselves or by reducing the impact of risk factors (Loeber & Farrington, 2012), whereas other researchers rather consider protective factors as the opposite side of risk factors (Harris & Rice, 2015). The interaction between risk and protective factors has, nevertheless, not been empirically investigated yet.
Considering these suggested conceptualizations, previous studies on protective factors have mainly been focused on juvenile offenders and most of the longitudinal studies published regarding protective factors of juveniles drive from nondelinquent school populations (e.g., Loeber, Farrington, Stouthamer-Loeber, Moffitt, & Caspi, 1998; Stouthamer-Loeber et al., 1993). These studies have found that factors like school achievement, presence of a positive peer group, psychosocial health, residential treatment, and social integration level seem to be relevant protective factors that predicted desistance from criminal and/or violent behavior in adolescents (e.g., Borowsky, Hogan, & Ireland, 1997; Calley, 2012; Hall & Barongan, 1997; Hoge, Andrews, & Leschied, 1996; Stouthamer-Loeber, Wei, Loeber, & Mastenb, 2004; Zagar et al., 2009).
The number of studies investigating protective factors against reoffending in adults is small. However, factors such as self-regulation, empathy, coping skills, compliance, vocational training, employment status, living situation, and social network are suggested to be personal and environmental resources against recidivism (Brown, Harkins, & Beech, 2012; DeMatteo, Heilbrun, & Marczyk, 2005; Gendreau, Goggin, & Gray, 2000; Miller, 2006; Ullrich & Coid, 2011). Recent studies also found risk-reducing effects for treatment programs, reintegration plan quality, and a positive relationship to correction officers as well (Beggs & Grace, 2010; Kennealy, Skeem, Manchak, & Eno Louden, 2012; Marques, Wiederanders, Day, Nelson, & van Ommeren, 2005; Olver, Stockdale, & Wormith, 2011; Scoones, Willis, & Grace, 2012; Willis & Grace, 2008). As these factors appear to overlap with the risk factors identified in large meta-analyses (Hanson & Morton-Bourgon, 2005; Mann, Hanson, & Thornton, 2010), the construct of protective factors remains unclear.
Similar to the course of this debate, several Structured Professional Judgment (SPJ; Douglas & Reeves, 2010) instruments with different conceptualizations for the assessment of protective and risk factors have been developed during the last years. For instance, the Structured Assessment of Violence Risk in Youth (SAVRY; Borum, Bartel, & Forth, 2006) assesses six protective factors against juvenile violence in addition to 24 risk factors. On the contrary, within the Short-Term Assessment of Risk and Treatability (START; Webster, Martin, Brink, Nicholls, & Middleton, 2004; Webster et al., 2009), all included factors can be assessed either positively (protective) or negatively (risk) related to possible adverse outcomes for adult forensic patients on a 3-month basis. An official German version of the START was recently published in spring 2015 (Webster, Martin, Brink, Nicholls, & Desmarais, 2009/2015). However, the currently existing instruments capturing protective factors were criticized for not considering the medium-term (e.g., over 1 year) treatment-related aspects in adult forensic populations (de Vries Robbé, de Vogel, & de Spa, 2011). To overcome these limitations, the Structured Assessment of PROtective Factors (SAPROF) for violence risk (de Vogel et al., 2009) was developed as a structured assessment guideline for protective factors against future violent (including sexually violent) behavior in criminal offenders and forensic-psychiatric patients. The SAPROF defines protective factors in a broader sense: “any characteristic of a person, his/her environment or situation which reduces the risk of future violent behavior” (de Vogel et al., 2009, p. 25). The initial sample used in the development process of the SAPROF consisted of violent offenders, though the authors assumed that the found protective factors could be valid for sexual violence as well. The authors suggested to use the SAPROF in combination with another well-validated SPJ risk assessment tool (e.g., Sexual Violence Risk–20 [SVR-20] for sexual offenders; Boer, Hart, Kropp, & Webster, 1997) because the purpose of assessing protective factors is to achieve a balanced view on a broader spectrum of recidivism-related factors of an individual (de Vogel et al., 2009). The initial validation study of the SAPROF revealed good to excellent predictive validity for desistance from reoffending in violent and sexual offenders (de Vries Robbé et al., 2011; de Vries Robbe, de Vogel, Koster, & Bogaerts, 2015). Both total scores and final protection judgments indicated a large effect size of the instrument in 126 violent offenders after 1 year (area under the curve [AUC] = .82-.85, p < .01), 2 years (AUC = .77-.80, p < .01), and 3 years (AUC = .71-.74, p < .01) after release from a forensic-psychiatric institution. In sexual offenders (n = 83), the AUC values of the SAPROF total scores were slightly lower for the follow-up period of 3 years (AUC = .76, p < .05) and after 15 years (AUC = .71, p < .01). The final protection judgments turned out to be nonsignificant (both AUCs = .65, p = ns). Another recently published study found strong predictive power of the SAPROF regarding absence of violence (AUC = .85) within a follow-up period of 6 months in a sample of 98 patients in a secure forensic hospital setting (Abidin et al., 2013). In a sample of juveniles alleged for sexual offending (n = 71), the sum scores of the German version of the SAPROF predicted desistance from violent recidivism (AUC = .65, p < .05) but failed to achieve any incremental predictability beyond the SAVRY in a mean follow-up period of 47.84 months (Klein, Rettenberger, Yoon, Kohler, & Briken, 2015).
Except for the above-mentioned initial validation study by the developers of the SAPROF in a hospitalized sexual offender sample in the Netherlands (de Vries Robbe, de Vogel, Koster, et al., 2015), there exist no published data about the influence of protective factors on the risk of recidivism in adult sexual offenders. Preliminary results of the German SAPROF version tested in a pilot study with 30 sexual offenders (Yoon, Spehr, & Briken, 2011), which were currently integrated in an outpatient treatment program, revealed a significant negative correlation between the SAPROF and the risk measured with the SVR-20 (Boer et al., 1997). However, no correlation was found between the SAPROF and the risk measured with the Static-99 (Hanson & Thornton, 1999). The German version of the SAPROF exhibited negative correlations with the actuarial risk measured by the Screening Tool for the Assessment of Young Sexual Offenders’ Risk (STAYSOR; Klein et al., 2012) and the SAVRY risk factors in another sample of accused juveniles (n = 66) who have sexually offended (Klein et al., 2012). These results might indicate that the SAPROF corresponds better with SPJ instruments measuring clinical, supposedly dynamic risk factors rather than certain actuarial instruments with more historical factors, in accordance with the background of its development.
Apart from the above-mentioned studies, however, there is a lack of assessment tools for protective factors in general and their validation in German-speaking countries. Furthermore, previous studies do not provide sufficient information regarding the influence of protective factors on recidivism in adult sexual offender populations. Although the debate regarding the overlap in risk and protective factors cannot be resolved, the utility and a possible additional benefit of the SAPROF upon existing risk assessment are worth examining. The current study therefore aims at testing the predictive relevance of protective factors as captured by the SAPROF in a representative correctional sample of sexual offenders. Therefore, assessing predictive validity of the SAPROF factors regarding various types of recidivism after release was the main focus of this study. Given the comprehensive definition of protective factors within the SAPROF, this study premised that the SAPROF would predict desistance from various types of recidivism. Furthermore, another focus of interest was to investigate whether the protective factors add predictive power beyond the risk factors. For this purpose, we tested concurrent validity of the protective factors measured by the SAPROF against the risk factors measured by the SVR-20 and incremental validity of the SAPROF above and beyond the SVR-20 regarding various types of recidivism.
Method
Sample
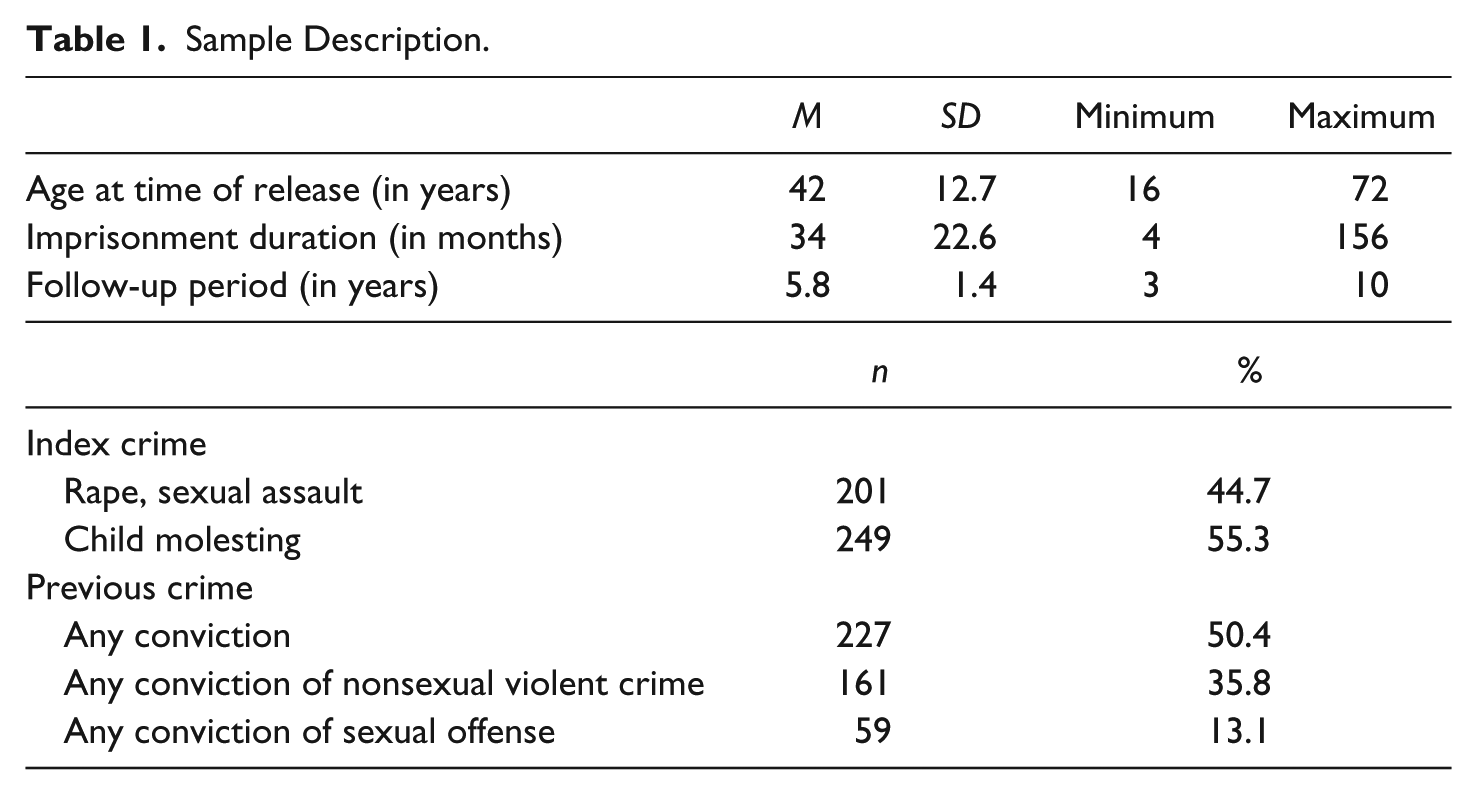
The sample of the current study is part of a larger sample of an ongoing research project using inmate evaluation reports of the Federal Evaluation Centre for Violent and Sexual Offenders (FECVSO; Eher, Matthes, Schilling, Haubner-Maclean, & Rettenberger, 2012; Mokros, Schilling, Weiss, Nitschke, & Eher, 2014) in the Austrian Prison System, a department within the Austrian Ministry of Justice. The FECVSO collects and evaluates data of all incarcerated sexual offenders in the Austrian Prison System. The SAPROF, however, is not part of the routine assessment. It was coded retrospectively based on file analyses in 467 sexual offenders who had undergone clinical diagnostics and forensic risk assessment between 2001 and 2007 at the FECVSO. This sample represents approximately 60% of all offenders reported to the FECVSO and referred to further clinical assessment due to one of following criteria: (a) Static-99 total score of more than 5, (b) age younger than 25, (c) prison sentence of more than 4 years, (d) conviction for a child abuse offense with a nonrelated victim, or (e) reconviction for a sexual crime. However, because the SAPROF was originally developed to assess protective factors regarding desistance from violent (including sexual) recidivism, 17 individuals with noncontact offenses only (e.g., exhibitionism, child pornography abuse) were excluded, and a final count of 450 cases was included into further analyses (see Table 1).
Sample Description.
Measures
Recidivism
To enhance objectivity of the outcome measure, recidivism was defined as any official reconviction after discharge. Reconviction data were collected in four different recidivism categories: general, nonsexual violent, sexual, and violent (including sexual) recidivism. These recidivism categories were generated adopting the definitions of the most commonly used risk assessment tools, such as the Historical Clinical Risk–20 (HCR-20; Webster, Douglas, Eaves, & Hart, 1997), the SVR-20 or the Sexual Offender Risk Appraisal Guide (SORAG; Quinsey, Grant, Rice, & Cormier, 2006). In the present study, general recidivism was defined as any conviction of a new criminal offense, nonsexual violent recidivism as any new conviction of an offense causing physical harm or threat to a person with no sexual intention, and sexual recidivism as any new conviction of an offense involving sexual contact with a nonconsenting person. Violent (including sexual) recidivism comprises both nonsexual and sexual violent recidivism. In other words, while the sexual recidivism category contains only crimes with a sexual component, the violent (including sexual) recidivism category consists of any violent crime with or without a sexual component. The average follow-up time was 5.8 years after release from prison (SD = 1.4; see Table 1). The base rates for recidivism were as follows: 34.2% for general recidivism (n = 154), 16.9% for nonsexual violent recidivism (n = 76), 8.4% for sexual recidivism (n = 38), and 22.2% for violent (including sexual) recidivism (n = 100). The follow-up period refers to the time after release and not to the time after the assessment.
SAPROF
The 17 items of the SAPROF are categorized into three subscales: Internal Items (intelligence, secure attachment in childhood, empathy, coping, and self-control), Motivational Items (work, leisure activities, financial management, motivation for treatment, attitudes toward authority, life goals, and medication), and External Items (social network, intimate relationship, professional care, living circumstances, and external control). Except for the first two internal items (intelligence, secure attachment in childhood), all other SAPROF items are dynamic by definition. In the present study, the SAPROF items were coded retrospectively based on the assessment reports of the FECVSO. The case reports were approximately 20 to 30 pages and were evaluated by three of the authors all with different professional backgrounds (criminology, medicine, and psychology). The raters had extensive experience and trainings in risk assessment as well as in the SAPROF and treatment of sexual offenders. All three raters were blinded concerning the recidivism outcome. Because the file information was insufficient for coding certain SAPROF items—Item 7 “leisure activities” and Item 8 “financial management”—these items were coded as missing in many cases (see Table 2). Other three items of the SAPROF were excluded from reliability and validity analyses on the item level—Item 12 “medication” due to the rarity of medication in this prison sample, Item 16 “living circumstances,” and Item 17 “external control”—since by item definition, these items have to be coded with “2 (clearly present)” for an incarcerated person. The items can be briefly described as follows:
Overview on the SAPROF Item Values and Interrater Reliability Measures.
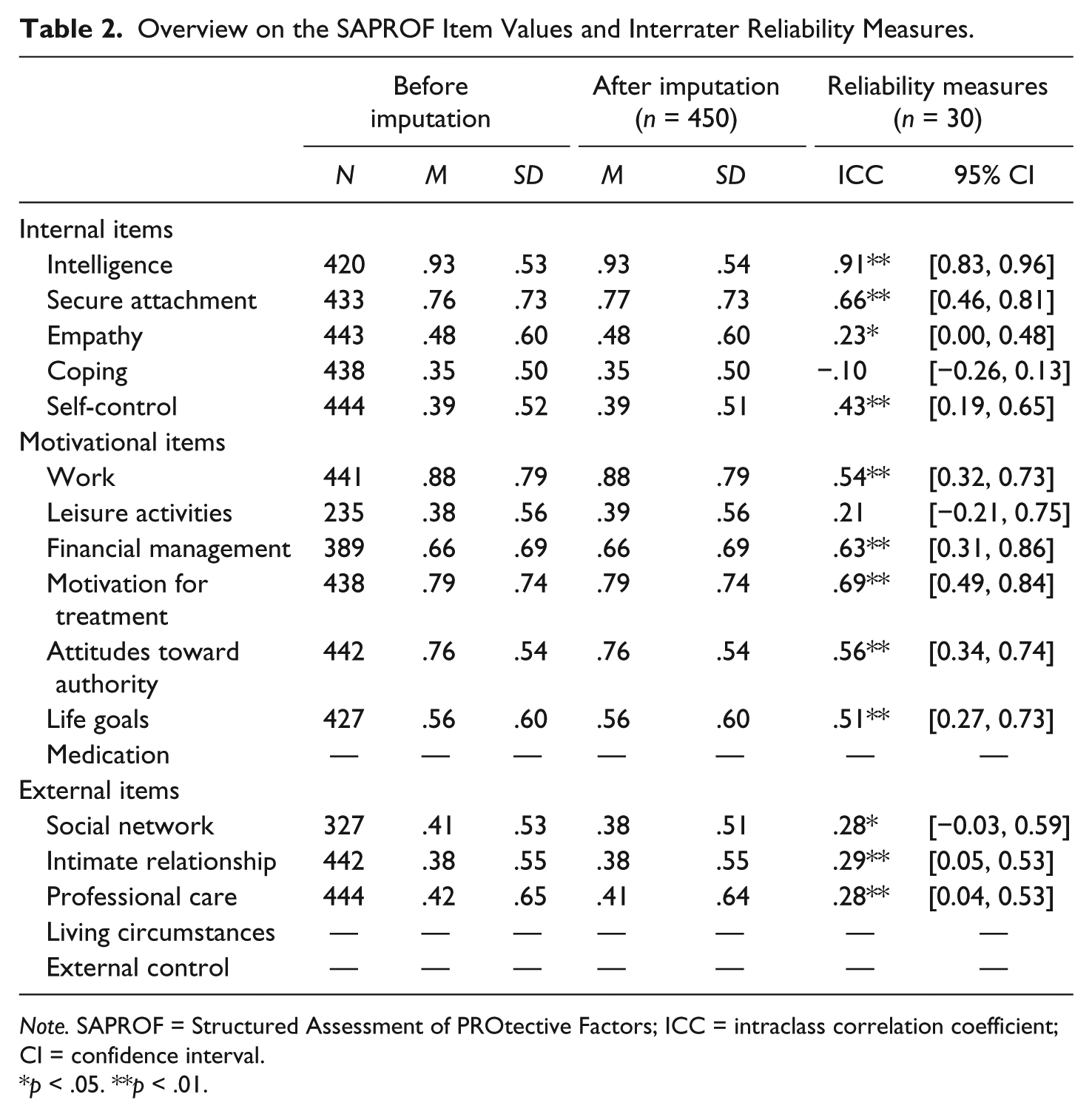
Note. SAPROF = Structured Assessment of PROtective Factors; ICC = intraclass correlation coefficient; CI = confidence interval.
p < .05. **p < .01.
Intelligence: IQ based on the results of a reliable and valid instrument. If the file ruled out IQ testing as it was not indicated, an average intelligence was assumed.
Secure attachment in childhood: A close bond with at least one prosocial adult before the age of 18. The biography was provided in all case files for rating any prosocial role models in childhood.
Empathy: Cognitive and emotional empathic ability in reaction to others and their situations. This item is considered as a dynamic factor in the SAPROF and coded based on behavioral and emotional responses of offenders toward other people and their situations, particularly toward past and potential victims.
Coping: Effective coping skills and strategies to appropriately manage stressful situations in daily life and risk-related circumstances. Reports on behaviors within an inmate community, therapeutic group, or external social networks were used to code the level of coping with stressful circumstance.
Self-control: Behavioral and emotional controls to reach goals and/or meet expectations. Similar to the coping item, the self-control was coded based on reports on behavioral aspects. Furthermore, institutional misconducts were also evaluated as a possible indicator for self-control and self-discipline.
Work: Regular and suitable occupation regardless of payment.Consistency and responsible work behavior in work history and intramural vocational status were evaluated for coding this item.
Leisure activities: Structured use of leisure activities not only within social contacts but also within inmate communities was evaluated for coding this item.
Financial management: Steady income and sound financial management regardless of the source of income were documented in the files and evaluated for the coding.
Motivation for treatment: Positive attitudes toward treatment and compliance. Because attitudes toward therapeutic intervention were elaborated in detail in the file, the openness toward treatment and motivation for changes in own behavior were used for coding motivation for treatment.
Attitudes toward authority:Acceptance and tolerance toward authority figures. This item refers to accepting decision by authority figures, including rule-obeying behaviors. Thus, complying with prison regulations was also evaluated next to the attitudes toward own convictions.
Life goals: Prosocial life goals provide positive meaning of life. Positive life goals were assumed when an individual has clear resources providing meaning of life such as religion, ideology, being a parent, or pursuing social or cultural ambitions.
Medication: Motivation for intake and responsiveness of primarily psychopharmacological medication. Medications are not frequently indicated in German correctional settings. In case of indicated or prescribed medications, acceptance of side effects, compliant intake, and responsiveness documented in the file were evaluated.
Social network: Prosocial, supportive, and stable social network (friends or relatives). As all visitors are documented in prisoner’s files, the characteristics of the networks were described in the case reports.
Intimate relationship: Stable intimate relationship of good quality for at least 1 year. Similar to the social network, relationship status was elaborated in the case reports.
Professional care: Availability and the intensity of appropriate treatment measures. History of treatment and current treatment status in the case reports were evaluated for the rating.
Living circumstances: Living circumstances that are intensively supervised by mental health care professionals. As mentioned above, this item was coded with “2 (definitely present)” according to the item definition.
External control: Mandatory treatment order, probation, or other institutional monitoring measures. As mentioned above, this item was coded with “2 (definitely present)” according to the item definition.
As in most other SPJ instruments, the items can be rated on a 3-point scale reaching from 0 (clearly absent) to 2 (clearly present). It was recommended to rather use the total scores for research purposes than for any clinical decision making because “scores are not related to norms or criteria” similar to other SPJ instruments such as the HCR-20 (de Vogel et al., 2009, p. 24; Webster et al., 1997). In a clinical context, after all items are rated and weighted concerning their relevance for the treatment planning process, a final judgment for protection can be made. An integrative judgment about the recidivism risk counterbalanced by the protective factors should be made as the final step. These two clinical judgments were not included into this study because the file analyses did not provide sufficient information to make an overall clinical judgment.
SVR-20
The SVR-20 was constructed to assess the clinical risk of sexual violence in adult sexual offenders. The instrument consists of 20 items and is divided into three subsections: psychosocial adjustment (sexual deviation, victim of child abuse, psychopathy, major mental illness, substance use problems, suicidal/homicidal ideation [ideas], relationship problems, employment problems, past nonsexual violent offenses, past nonviolent offenses, past supervision failure), sexual offenses (high-density sex offenses, multiple sex offense types, physical harm to victim(s) in sex offenses, use of weapons or threats of death during sex offenses, escalation in frequency or severity of sex offenses, extreme minimization or denial of sex offenses, attitudes that support or condone sex offenses), and future plans (lacks realistic plans, negative attitude toward intervention). According to the survey of Archer et al. (2006), the SVR-20 is one of the most frequently used instruments for risk assessment in adult sexual offenders in North American and European countries. Also in the German-speaking part of Europe, the SVR-20 is commonly used in different forensic settings. There are recent cross-validation studies from Germany, Austria, and Switzerland (Dietiker, Dittmann, & Graf, 2007; Rettenberger, Boer, & Eher, 2011; Rettenberger, Hucker, Boer, & Eher, 2009; Stadtland et al., 2005).
The SVR-20 was part of the initial diagnostic and risk assessment process and was rated prospectively during the offenders’ stay at the FECVSO (Rettenberger et al., 2011). An excellent interrater reliability of the sum score of the SVR-20 in this sample was reported elsewhere for an overlapping sample (Rettenberger et al., 2011; intraclass correlation coefficient [ICC] = .84, p < .001). The AUC values of the SVR-20 sum scores ranged from .68 (p < .01) regarding violent recidivism to .72 (p < .01) regarding sexual recidivism in the aforementioned study.
Statistical Analyses
The first part of analyses was conducted to offer descriptive information concerning the distribution of the SAPROF ratings within the present sample of incarcerated male sexual offenders. To measure interrater reliability, single ICCs with a two-way random effects model for absolute agreements in sum scores as well as in each item were calculated. All three above-mentioned raters independently coded 30 randomly selected cases. These 30 cases were included into the further analyses after being recoded with the average scores of the three raters. For further analyses, the sum scores of the SAPROF were calculated after adjusting the missing values via multiple imputation procedures using SPSS (IBM SPSS Statistics 22.0.0 for Windows, SPSS, Inc., Chicago, IL, USA). In other words, the missing item values were filled with estimates based on present values.
Predictive accuracy of the SAPROF and its items regarding absence of recidivism was analyzed by calculating the AUC based on the receiver operating characteristics (ROC; Hanley & McNeil, 1982). A number of researchers have suggested ROC analyses as a standard measure of testing predictive accuracy in the field of forensic research (Hanson, 2009; Mossman, 1994; Rice & Harris, 1995). ROC analyses provide information on the discriminative performance of a test for each possible cutoff score. The level of accuracy of the test performance is revealed by the AUC values. An AUC value of 1 represents a perfect predictive performance, while a value of .5 indicates a prediction at chance level and a value below .5 indicates negative accuracy (i.e., the variable is related to the outcome in the direction opposite of what was anticipated).
The convergent validity of the SAPROF was tested against the SVR-20 by Pearson product–moment correlation analyses with two-tailed test of significance.
For the calculation of the incremental validity, sequential regression models are generally the method of choice (e.g., Hunsley & Meyer, 2003). Because of the substantial variability in the follow-up periods due to unequal follow-up time periods, we calculated Cox regression models. Cox regression estimates hazard ratios which are similar to risk ratios associated with one or more predictor variables from data with unequal follow-up times (Allison, 1984; Hanson, 2006). For the purposes of the present study, sequential Cox regression models with the SAPROF and the SVR-20 as independent variables, and the dichotomous recidivism criteria as the dependent variable were calculated to observe if the SAPROF protective factors add predictive power above and beyond the SVR risk factors. For this purpose, the SVR-20 was entered as a covariate in the first block to control for risk, followed by the SAPROF in a second block. All statistical analyses were conducted using SPSS version 22.0.0.
Results
Risk and Protection Scores
The average total score of the SVR-20 was M = 19.01 (SD = 6.78, range = 2-36; possible total sum = 40), the average total score of the SAPROF was M = 12.95 (SD = 4.11, range = 4-25; possible total sum = 34). The average item values before and after the imputation procedures are demonstrated in Table 2.
Interrater Reliability
The ICC single measure for the SAPROF total scores was ICC = .72** (95% confidence interval [CI] = .[56, .85]). According to the critical values proposed by Fleiss (1986; ICC ≥ .75 = excellent; .60 ≤ ICC < .75 = good; .40 ≤ ICC < .60 = moderate; ICC < .40 = poor), this number indicates a good interrater reliability. Both Internal and Motivational subscales revealed good to excellent reliabilities as well (Internal subscale: ICC = .73** and Motivational subscale: ICC = .79**), whereas the ICC for the External subscale was rather poor (ICC = .31**). Although eight of 14 analyzed items showed at least moderate reliability values, six items showed rather weak reliability values. Only intelligence showed an excellent interrater reliability and secure attachment, financial management, motivation for treatment revealed good interrater reliability. ICC values for self-control, work, attitudes toward authority, and life goals were moderate. Empathy, social network, intimate relationship, and professional care showed rather poor ICC values. ICC measures for coping and leisure activities were not significant, and interrater reliability for the Coping item was even lower than chance. The ICC values of each item are displayed in Table 2 next to the average item values.
Predictive Validity
Table 3 shows the predictive accuracy of the SAPROF items, the total score and the subscales’ scores in terms of the AUC values. According to the critical values proposed by several researchers (Cohen, 1992; Dahle, Schneider, & Ziethen, 2007; Rice & Harris, 2005; AUC ≥ .72 = large effect size; .64 ≤ AUC ≤ .71 = moderate; .56 < AUC < .64 = small), the results showed overall a rather small to moderate predictive accuracy of the SAPROF concerning the prediction of desistance from various forms of recidivism. Two items showed significant moderate AUC values for general, nonsexual violent, and violent including sexual violent recidivism: work and financial management (AUC = .64**-.71**). There were two items with small but significant AUC values: self-control and life goals for the same recidivism categories (AUC = .58*-.63**). However, only secure attachment in childhood was significantly linked to sexual recidivism (AUC = .61*). The item life goals also approached statistical significance (AUC = .59; p = .62) for sexual recidivism. The rest of the items did not predict sexual recidivism and overall, nine of the 13 items examined did not significantly predict any of the four recidivism outcomes. On the subscale level, small predictive powers of the internal scores (AUC = .57*-.58*) and small to moderate predictive powers of the motivational scores (AUC = .63**-.67**) were observed for the three above-mentioned recidivism types. External scores could not predict any recidivism category. The total scores of the SAPROF predicted desistance from the three aforementioned recidivism categories but with small effect sizes (AUC = .61*-.63**). Neither the total score nor the scores of the subscales could significantly predict desistance from sexual recidivism.
Summary of ROC Analyses.
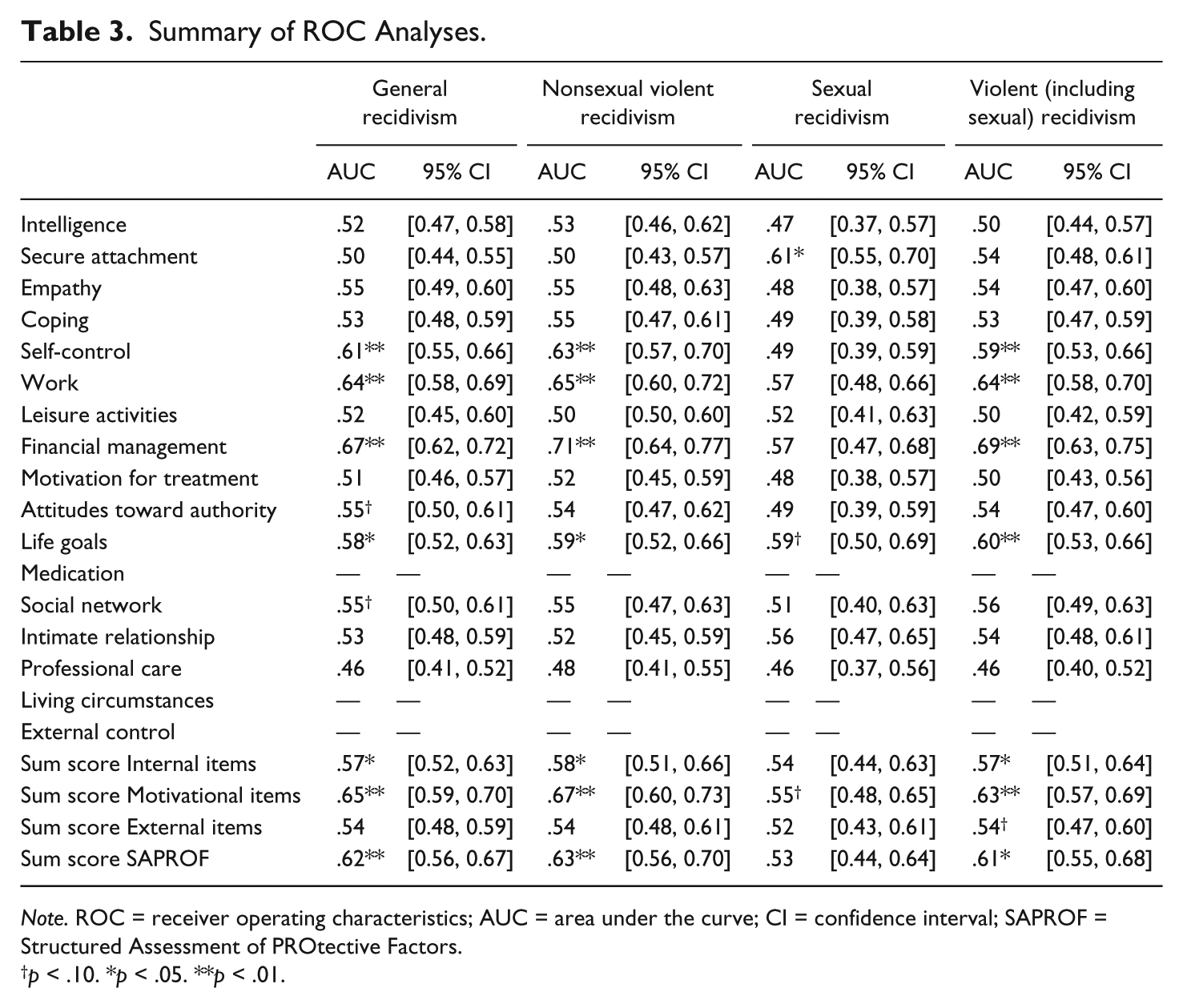
Note. ROC = receiver operating characteristics; AUC = area under the curve; CI = confidence interval; SAPROF = Structured Assessment of PROtective Factors.
p < .10. *p < .05. **p < .01.
Criterion-Related Validity
The SAPROF total score was negatively correlated with the SVR-20 total score with a Pearson’s r of −.66** (p < .01), which represents a large effect size according to the Cohen convention (Cohen, 1992).
Incremental Validity
Cox regression analyses revealed that the SAPROF scores did not add any predictive power above and beyond the SVR-20 scores (see Table 4). The hierarchical analyses revealed that in the first block, the SVR-20 contributed significantly to the prediction of all recidivism categories with hazard ratios of 1.09-1.12 (p < .01), which means that an increase of each 1 point in the SVR-20 was associated with an increase of 9% to 12% in the rates of recidivism. However, adding the SAPROF into the model to test whether decreases of SAPROF scores become a unique predictor of recidivism after controlling for the SVR-20 scores, the model did not explain additional variation in recidivism.
Summary of Cox Survival Analyses at Instrument Level.
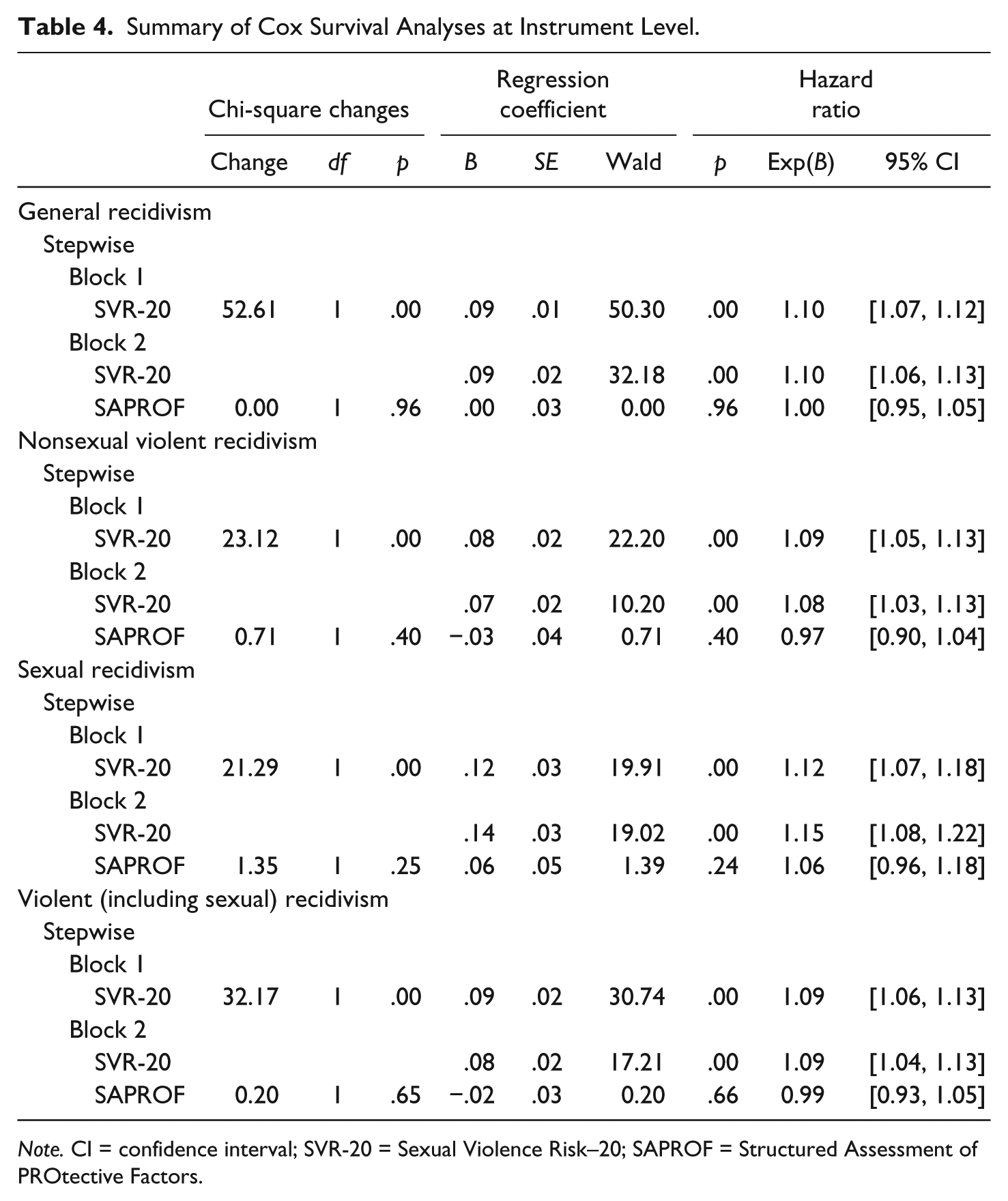
Note. CI = confidence interval; SVR-20 = Sexual Violence Risk–20; SAPROF = Structured Assessment of PROtective Factors.
Discussion
The present study represents the first empirical evaluation of the reliability and validity of the German version of the SAPROF in a correctional sample of adult male sexual offenders.
The offenders in the present study varied considerably from the German-speaking populations assessed in previous studies concerning the presence of protective factors (M = 12.95, SD = 4.11). For example, an outpatient community sample of sexual offenders (Tozdan, Briken, Yoon, & von Franqué, 2015; Yoon et al., 2011) revealed substantially more protective factors as measured with the SAPROF (M = 14.60, SD = 5.06; M = 17.35, SD = 5.64). The results of the present study might resemble the fact that offenders of this study were (a) higher on risk in general and (b) evaluated in their early stage of incarceration by the FECVSO, which usually is accompanied by lower level of protection. However, the samples might also differ on various other issues (e.g., incarcerated vs. outpatient setting). On the contrary, the SAPROF mean scores of the present study were comparable to a sexual offender sample (M = 12.25, SD = 5.91) of a forensic mental health hospital in the Netherlands (de Vries Robbe, de Vogel, Koster, et al., 2015).
Despite the multidisciplinary composition of the rater team, the ICC measures on the total scores and scores for the Internal and Motivational subscales indicated a reasonable raters’ agreement (ICC = .72-.79**). However, two of five internal items (empathy, coping), one motivational item (leisure activities) and all the external items (social network, intimate relationship, professional care) noticeably varied among raters showing poor or nonsignificant interrater reliability. Coping revealed the weakest reliability that was even below chance level. A possible explanation could be that the archival data were insufficient to code this item properly because the manual suggests “to include information from the individual’s daily life” (de Vogel et al., 2009, p. 43), which was not available in most cases. However, it is possible that this item gives leeway to raters to evaluate certain behavioral observation as an effective coping mechanism or not. Regarding the items “leisure activities” and “social network,” it should be noted that these items had the most missing values. It can be assumed that these items are difficult to rate in an early stage of incarceration because the inmates were removed from their social contexts. Further prospective studies are warranted to address the interrater reliability issue within a setting that allows more intensive case information including daily behavioral observations.
Taking one of the first validation studies from Utrecht into account, which yielded a good to excellent predictive validity of the SAPROF total scores for violent and sexual recidivism in sexual offenders (de Vries Robbe, de Vogel, Koster, et al., 2015), the present study found only small to moderate predictive validity indices for the instrument. The sum score of protective factors was, nevertheless, found to be a reasonable predictor for desistance from at least general, nonsexual, and sexual violent recidivism in sexual offenders. The predictive power for the sexual recidivism category was not significant. These results at least partially correspond with the results of the initial sexual offender validation study conducted by the Utrecht research group showing that the SAPROF predicts violent recidivism better than sexual recidivism (de Vries Robbe, de Vogel, Koster, et al., 2015). This finding might originate from the general characteristics of the SAPROF items, which are primarily related to general and violent criminality and less to sexual criminality (cf. Babchishin, Hanson, & Helmus, 2012). As Seto and Fernandez (2011) postulated distinctive dynamic risk groups depending on sexual deviance and criminogenic needs, it is possible that the SAPROF might perform better in violent sexual offenders with high antisociality than in sexually deviant offenders. Some subscales of the SAPROF exhibited significant predictive power. In particular, Internal and Motivational subscales predicted general, nonsexual violent, and violent recidivism. None of the subscales predicted sexual recidivism, and, external factors did not predict any recidivism category. Corresponding to this result, some of the individual items of the SAPROF showed meaningful predictive accuracy: “self-control,” “work,” and “financial management” were the most precise predictors with small to moderate effect sizes in all recidivism categories except for sexual recidivism. These factors were also identified in the Dutch validation study as the strongest predictors for violent recidivism (de Vries Robbé et al., 2011). The “secure attachment in childhood” was the only item that significantly predicted desistance from sexual recidivism. In the SAPROF, secure attachment in childhood refers to being attached to at least one prosocial role model before adulthood rather than indicating a secure or insecure attachment type as described by Bowlby (Bowlby, 1969, 1973; de Vogel et al., 2009). The association of this item with desistance from sexual recidivism might indicate that the risk of sexual (re)offending might be reduced by keeping bonds toward others with prosocial characteristics over developmental periods. However, as running 13 analyses might yield in a significant result by chance from the default Type I error rate (.05), the significance of this finding needs to be considered with caution. The predictive power of “life goals” might reflect the positive motivation for a satisfying life being a strong protective factor against recidivism risk. Although the offenders only partially showed explicit motivation for treatment (see Table 2), those willing to reach distinct meaningful goals were found to be lower on risk for recidivism in this study.
Although the above-mentioned results indicated that the SAPROF scores themselves showed significant predictive power for several recidivism categories, the SAPROF did not exhibit any incremental validity above and beyond the SVR-20 for any of the recidivism criteria. The overall results parallel those from the German validation study of the SAPROF in a juvenile sample by Klein et al. (2015). Following the conceptualization of Loeber and Farrington (2012), it could be assumed that the SAPROF factors represent protective factors by themselves predicting desistance from criminal behaviors and/or lower probability of recidivism, but do not outweigh the effect of risk factors measured by the SVR-20. One of the most obvious explanations for the lack of incremental effect of the SAPROF is that the SAPROF might not measure unique constructs that are not contained in the SVR-20, which was also indicated by the highly significant correlation between the two instruments (r = .66**) in the present study.
One of the strongest limitations and a possible explanation for the low predictive accuracy found in our study might be the fact that the SAPROF ratings were based on archival information, which did not include treatment-relevant information. The SAPROF is described as an instrument, which is helpful for observing treatment changes of clients and for predicting recidivism risk when used in combination with other (SPJ) risk assessment tools. The positive values in the 15 dynamic factors of the SAPROF might require at least some progress within the therapeutic intervention. Overall, the current study examined the reliability and the validity of the SAPROF using the item and total scores and therefore cannot claim that it reflects a clinical setting in which the usual SPJ assessment is administered. Thus, it can be assumed that applying the SAPROF for posttreatment ratings or during treatment might lead to a higher predictive accuracy than in the present study (e.g., de Vogel et al., 2009). Furthermore, the present study tested an instrument originally developed for forensic hospital populations in a correctional offender sample. Therefore, it cannot be ruled out that there exist specific factors that can only be applied in correctional populations. In the same context, the SAPROF was developed primarily within a violent offender pool and was designed to assess factors against future violence including sexual violence and not specifically sexual violence. Thus, the low predictive accuracy of the tool particularly for sexual recidivism seems to have a plausible background. However, it is also possible that the SAPROF is missing certain factors relevant for desistance from recidivism in sexual offenders. For instance, Willis and Grace (Willis & Grace, 2008) underlined the importance of the quality of reintegration planning in sexual offender risk management. Another study suggested that victim-specific empathy is a stronger predictor for sexual recidivism than general empathy (Brown et al., 2012). A more recent review regarding protective factors in sexual offending has identified healthy sexual interests as possible protective factors against sexual offending (de Vries Robbe, Mann, Maruna, & Thornton, 2015). As the SAPROF items do not contain these specific aspects, it is possible that the items need further clarifications for certain sexual offenders, whose nature of offending is rather deviant than violent (Seto & Fernandez, 2011).
Overall, the significant predictive power of the SAPROF as an instrument and certain factors of the SAPROF might indicate that the inclusion of positive aspects in individuals in risk assessment procedures could be beneficial. The SAPROF factors seem to have protective effects regarding general, nonsexual violent, and sexual violent criminality. As sexual offenders are very heterogeneous in nature, further analyses in various risk groups are needed to differentiate their risk traits and strengths, which could be helpful to provide indications for more appropriate intervention programs for specific types of sexual offenders. Also, items with lower interrater reliability need further examination for the usage in the correctional population, especially in a prospective setting with a more sufficient information basis for the rating. Discrepancies between this study using a correctional admission sample and previous forensic posttreatment samples need to be addressed in further studies. A prospective design with more sufficient information to code the SAPROF items in a clinical setting, which would correspond with the development purpose, might result in a stronger validity of the instrument. Moreover, as recently examined in their studies (de Vries Robbe, de Vogel, Douglas, & Nijman, 2015; Tozdan et al., 2015), an examination regarding the relationship between therapeutic changes and posttreatment scores measured by the SAPROF with desistance from various recidivism types in a representative correctional sexual offender sample is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was realized within the MiKADO project, funded by the German Federal Ministry of Family Affairs, Senior Citizens, Women and Youth.