
Abstract
In this study, the impact of suggesting that pedophilia is immutable on a man’s specific self-efficacy for modifying his sexual interest in children was examined in 94 men with a sexual interest in children. The participants were selected from differing contexts and included non-forensic patients, forensic patients, and participants from the Internet. Randomly distributed to two conditions, the mutable condition group received the information that experts consider pedophilia to be modifiable, whereas the immutable condition group received the information that experts consider pedophilia to be stable. Afterward, the participants’ levels of specific self-efficacy for modifying their sexual interest in children were assessed. Non-forensic participants in the mutable condition reported higher levels of specific self-efficacy than those in the immutable condition. No differences in specific self-efficacy were revealed for the forensic and Internet participants when comparing the mutable and immutable conditions. It would appear appropriate to avoid generalized and absolute statements about the (im)mutability of sexual interest in children, as scientific research on this topic remains insufficient. Furthermore, given the present results, such statements might have serious consequences for an individual’s belief in being able to change his sexual interest in children.
Keywords
Introduction
Sexual Interest in Children
Within the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), pedophilia is described as recurrent, intense sexually arousing fantasies, sexual urges, or behaviors involving sexual activity with a prepubescent child or children (typically under the age of 13 years). A recent study on 8.718 German males demonstrated that 4.1 % of the total sample reported sexual fantasies including prepubescent children (Dombert et al., 2016). However, only 0.1% of the total sample reported a pedophilic sexual preference (Dombert et al., 2016). Other studies, by contrast, assume a prevalence of 5% for pedophilia in the general population (e.g., Seto, 2012).
The DSM-5 specifies an exclusive type of pedophilic disorder (i.e., sexually attracted only to children), a non-exclusive type (i.e., sexually attracted to children, but also to adults), and an incest type (i.e., sexually attracted only to members of one’s own family; American Psychiatric Association, 2013). Some researchers (e.g., Balon, 2014; Blanchard, 2013; Briken, Fedoroff, & Bradford, 2014; Fedoroff, Gionacchino, & Murphy, 2013; First, 2010; Green, 2010; O’Donohue, 2010) criticized the DSM-5 diagnostic criteria for various reasons, and in particular for the fact that pedophilic disorder has no “in remission” specifier, thus indicating that pedophilia is considered to be a lifelong condition (Briken et al., 2014). In accordance with Balon (2014, p. 1236), the question can again be posed: “Do we have any evidence to support this?” Doubting the changeability of sexual interest in children would appear justifiable, as would assuming a certain level of stability over time (e.g., Beier et al., 2009; Beier, Bosinski, & Loewit, 2005; Cantor, 2012; Seto, 2009). Seto (2012) for instance regarded pedophilia as a sexual age orientation that is—similar to sexual orientation—stable over time. Cantor (2012) was also of this opinion, stating that sexual interest is a lifelong characteristic and thus implying that it cannot change. In 2005, Beier and his colleagues defined sexual responsiveness to pre-, peri-, or postpubertal bodies as part of a “human sexual preference structure” that manifests in puberty and remains from then on unchanged (Beier et al., 2009; Beier et al., 2005). However, it appears that it may also be justifiable to doubt the immutability of sexual interest in children in general and to assume a certain level of flexibility, especially in the non-exclusive and incest types (e.g., Bradford, Fedoroff, & Gulati, 2013; Fedoroff et al., 2014; Marshall, 2008). Marshall (2008) for instance noted that there is evidence indicating that sexual interest in children can change. He refers to results that indicated that a substitutability of sexual interest in children through a stronger sexual interest in adults may emerge during treatment (Marshall, 1997). Moreover, Tozdan and Briken (2015b) examined 75 individuals with a sexual interest in children and assessed the self-perceived mutability of their sexual interest in children using a three-item questionnaire with a maximum score of 15. Results showed that the average mutability was 8.4 (SD = 3.8, range = 3-15) indicating that there may be a spectrum from stable to mutable across which affected individuals are distributed (Tozdan & Briken, 2015b).
With regard to clinical practice, some treatment centers (e.g., Beier et al., 2015; Cantor, 2012) support their clients in accepting their sexual interest in children as immutable (Institute for Sexology and Sexual Medicine of the Charité—University Berlin, 2013), whereas others tend to consider sexual interest in children to be more or less changeable (Fedoroff et al., 2014; Lipp, 2014).
It has always been commonly understood (Marshall, Barbaree, & Butt, 1988) and empirically shown (e.g., Freund & Watson, 1991; Seto, Lalumiére, & Kuban, 1999) that sexual offenses against children are associated, at least in part, with a sexual interest in children. Thus the avoidance of sexual offenses against children can be described as the most important goal when treating pedophilic individuals (e.g., Beier et al., 2009). Marques, Nelson, West, and Day (1994) have shown that individuals who were in treatment consequent to committing a sexual offense against children were at lower risk of committing further sex crimes than individuals in the control group. The contents and therapeutic strategies of a treatment program for individuals with a sexual interest in children can therefore be considered highly relevant in terms of preventing sexual offenses against children.
The present study is associated with a theoretical framework within which sexual interest in children is considered to be more or less flexible and open to change (Tozdan & Briken, 2015a). This does not however mean that this theory promotes a so-called “reparative therapy” for pedophilia, which would try to eliminate any pedophilic desires with the aim of “curing” pedophilia. This framework rather links sexual interest in children with the core principle of the social cognitive theory expounded by Bandura (Bandura, 1977, 1986, 1997, 2001), that is, self-efficacy.
Self-Efficacy and Sexual Interest in Children
Self-efficacy was first postulated by Bandura (1977) and is still considered to be a relevant psychological construct that has been examined intensively in the past (e.g., Kaplan, Ries, Prewitt, & Eakin, 1994; Maddux & Gosselin, 2003). Bandura defines self-efficacy as “the conviction that one can successfully execute the behavior required to produce the outcomes” (p. 193). Research has shown, first, that a higher level of self-efficacy is associated with better mental and physical health (Fuchs & Schwarzer, 1994); second, that self-efficacy appears to be a strong predictor for motivation for change (Schwarzer, 2001); third, that specific self-efficacy beliefs have an impact on corresponding specific experiences and behavior (Ollendick, 1995), and fourth, lower levels of self-efficacy seem to be associated with delinquent behavior (Booxbaum & Burton, 2013; Carroll, Gordon, Haynes, & Houghton, 2013; Tierney & McCabe, 2002). Moreover, a number of randomized controlled trials (RCTs) in various research fields (including nutritional behavior, smoking behavior, drug consumption, and criminal behavior) have shown that experimental manipulations can systematically influence specific self-efficacy beliefs (Marquez, Jerome, McAuley, Snook, & Canaklisova, 2002; Van’t Riet, Ruiter, Smerecnik, & de Vries, 2010; Walsh & Russell, 2010) even so far as to affect mental well-being (Reif, de Vries, Petermann, & Görres, 2013) as well as subsequent behavior (Koring et al., 2012; Luszczynska & Tryburcy, 2008). Therapeutic interventions focusing on specific self-efficacy beliefs were demonstrated to positively affect treatment progress and success for diverse psychological disorders (Ollendick, 1995; Petermann & Noeker, 1991).
It can be reasonably assumed that conveying sexual interest in children as generally immutable correspondingly influences the expectations of affected individuals and may consequently impede change of sexual interest in children in some affected individuals (Briken et al., 2014; Tozdan & Briken, 2015a).
At this point, a brief explanation of the terms immutable/mutable, unchangeable/changeable, and stable/flexible used throughout this article appears necessary. To use established and well-known definitions, we would like to draw a parallel to the literature on risk assessment in sex offenders. Decades of research aimed to identify factors that assess the risk of recidivism among criminals, including sex offenders (for review, cf. Bonta, Law, & Hanson, 1998; Gendreau, Little, & Goggin, 1996). Risk predictors are divided into two main groups: static factors (fixed and unchangeable, for example, the number of prior offenses) and dynamic factors (flexible and changeable, for example, self-regulation problems; Bonta, 1996; Witt & Schneider, 2005). Dynamic factors can be divided again into stable dynamic and acute dynamic factors. The former are enduring changeable characteristics, whereas the latter are rapidly changing changeable characteristics. In risk assessment instruments (e.g., Hanson, Harris, Scott, & Helmus, 2007), deviant sexual preferences such as pedophilia are usually interpreted and measured as stable dynamic factors amenable to change through a process of “effortful intervention” (i.e., treatment or supervision). Pedophilia is not defined as a static (i.e., fixed and unchangeable) factor. When using the terms immutable, unchangeable, or stable, we refer to the term “static” as used in the risk assessment literature and which stands for a fixed and permanently unchangeable state. When using the terms mutable, changeable, or flexible, we refer to the term “dynamic,” which reflects a more or less flexible and changeable state.
Previous research has indicated the existence of specific self-efficacy for modifying sexual interest in children (SSIC; Tozdan, Jakob, Schuhmann, Budde, & Briken, 2015), defined as an individual’s conviction of being able to influence/change their own sexual interest in children as a result of his or her own competencies. Some affected individuals may be convinced that they cannot influence or change their sexual interest in children, which would imply a low SSIC. In contrast, other affected individuals may believe that they are able to influence/change their sexual interest in children, which would imply a high SSIC. Research so far indicates that the SSIC varies across different subsamples of individuals with sexual interest in children and is related to their motivation to change (Tozdan & Briken, 2015b; Tozdan et al., 2015). A general treatment strategy suggesting that sexual interest in children immutable might decrease this SSIC (for detail, cf. Tozdan & Briken, 2015a), leading to a lower motivation for change and consequently hindering certain behavioral patterns required to actually change sexual interest in children. In contrast, suggesting that sexual interest in children is mutable might increase this SSIC, leading to an enhanced motivation for change as well as increasing the probability of behavioral patterns required to actually change sexual interest in children. Thus, if the SSIC of affected individuals, that is, their self-beliefs regarding their ability to change their sexual interest in children, can be influenced (e.g., by verbal information given by clinicians/experts), it seems obvious that clinicians should keep in mind that their statements on the immutability of this sexual interest may have an impact on their clients’ SSIC. In doing so, clinicians may thus indirectly address their clients’ motivation to change their sexual interest in children, which probably has consequences for treatment progress and courses of development.
Aims
The present study mainly aims to investigate the clinically highly relevant question as to whether SSIC can be affected by verbal information. Based on the research outlined above, we generated the following three hypotheses:
Method
Procedure
From March to September 2015, we conducted an online survey using three recruitment paths: (a) German and Swiss outpatient centers which treat individuals who have a self-identified sexual interest in children, who are not registered within the judicial system for sexual offenses against children, and who have started treatment to cope with their sexual interest in children (hereafter named non-forensic participants); (b) German forensic outpatient centers which treat individuals with a self-identified sexual interest in children who are registered by judicial system for at least one sexual offense against children and who have started treatment consequent to a judicial decision (hereafter forensic participants); and (c) an Internet information platform (www.Schicksal-und-Herausforderung.de) addressing individuals with a sexual interest in children. The platform was created by and for affected individuals, and explicitly advocates not acting on a sexual interest in children. It is an exclusively German-language site and information provided for website users concerns sexual interest in children (in particular media reports, reports by affected individuals on their experiences, and current research on pedophilia). The platform also has a guestbook function, enabling users to post their experiences and opinions and to enter into discussion with each other (hereafter Internet participants). The study was approved by the Ethics Committee of the Hamburg Chamber of Psychotherapists. Prior to beginning the survey, an introductory text, information for participants, and the informed consent form were presented to participants. To proceed the survey, individuals had to click three statements confirming that they have (a) read, (b) understood the information for participants, and (c) are giving their consent to participate in the study.
Experimental Design and Main Outcome Measure
In an online study, we focused on the experimental manipulation of the SSIC by suggesting either that sexual interest in children is flexible/changeable or that it is stable/immutable. The study is not a clinical trial involving medication or psychotherapy, and was not registered in any of the publicly accessible registries approved by the World Health Organization (WHO) or International Committee of Medical Journal Editors (ICMJE). A trial registration number can thus not be provided. The online survey was programmed by the first author, using the program “Enterprise Feedback Suite (EFS) Survey” from the company QuestBack AG (http://www.questback.com). The University of Hamburg provides this program for the purposes of scientific research. The randomization of the participants to one of the two conditions was carried out automatically by the survey program while the study was running. The therapists who recruited participants, the website administrators, and the participants were therefore blinded (double-blind experiment). Participants were randomly allocated to one of two experimental conditions: mutable or immutable. In both conditions, participants were presented with information about pedophilia and a supposed current predominant expert’s opinion regarding the changeability or immutability, respectively, of sexual interest in children. Participants within the mutable condition received the key message that the majority of experts assume that sexual interest in children is flexible and changeable, whereas participants within the immutable condition received the key message that the majority of experts assume that sexual interest in children is stable and immutable (for details, see Appendix). Afterward, we assessed the SSIC as the main outcome measure in all participants using the “Self-Efficacy for Modifying Sexual Interest in Children Scale” (SSIC-Scale; validated by Tozdan et al., 2015). Six items on the participant’s conviction regarding being able to change their sexual interest in children (Table 1) were answered on a scale from 1 (do not agree at all) to 5 (totally agree). The maximum score is 30, with higher scores indicating a higher level of self-efficacy. With regard to validation, the SSIC-Scale was investigated within a different sample of 56 men with a self-reported sexual interest in children. The instrument was shown by the results to have good internal consistency, that is reliability (Cronbach’s α = .87). Good construct validity was primarily demonstrated by the expected correlations of the SSIC-Scale with other aspects of sexuality such as sexual self-efficacy (r = .54, p < .01) and by the expected negative correlation with external locus of control (r = −.25, p < 10; Tozdan et al., 2015).
The Six Items of the SSIC-Scale.
Note. SSIC-Scale = Specific Self-Efficacy for Modifying Sexual Interest in Children Scale.
We would like the readership to note that there is intense discussion on the use of short scales in research. Credé, Harms, Niehorster, and Gaye-Valentine (2012) for instance argued that short and long questionnaires have the same claim to validity although they have different numbers of items. Random measurement errors cannot be compensated for so well, which thus reduces reliability and validity values (Credé et al., 2012). Another aspect concerns the construction and validation processes for short scales (Smith, McCarthy, & Anderson, 2000). For example, questionable shortening processes such as the maximization of internal consistency are used (Coste, Guillemin, Pouchot, & Fermanian, 1997). For the SSIC-Scale, however, internal consistency was not used as a shortening process (Tozdan et al., 2015) but rather was reported as a reliability measure. The internal consistency (Cronbach’s α) strongly depends on the number of items, that is, the more the items, the higher the Cronbach’s α (Cortina, 1993). This means that reliability can be increased artificially in large questionnaires. For one-dimensional short scales, such as the SSIC-Scale, Cronbach’s α can therefore be considered suitable because it reduces the risk of reliability being overestimated.
We included two control variables among the demographic variables that might be related to the SSIC to ensure equivalence for the two condition groups: First, we assessed the level of exclusiveness of sexual interest in children, because it has been shown to be related to the SSIC (Tozdan & Briken, 2015b). It was measured on a scale from 1 (interested in children exclusively) to 5 (interested in adults exclusively). Second, we assessed general self-efficacy because specific self-efficacy beliefs have been shown to be related to general self-efficacy (Fuchs & Schwarzer, 1994). It was measured using the General Self-Efficacy Short Scale (ASKU; Beierlein, Kovaleva, Kemper, & Rammstedt, 2012), which consists of three items (e.g., “I am able to solve most problems on my own”) answered on a scale from 1 (doesn’t apply at all) to 5 (applies completely). The maximum score is 15, with higher scores indicating a higher level of self-efficacy. At the end of the study, all the participants were informed that the experts’ opinions on flexibility or immutability that were presented in this study are not based on clear scientific findings and that any clear statement on this issue is not scientifically justified due to the current limited state of knowledge.
Sample
The inclusion criterion for our sample was that the participant has a self-identified sexual interest in children (up to 13 years). We assumed moderate effect sizes of approximately d = .60 for comparison between the two condition groups within the total sample. Given a significance level of α = .05 and a power of 1 − β = .85, an optimal sample size of 82 was calculated a priori.
A total of 105 non-forensic and forensic participants called up the study using the same study link. Of these, 83 started the questionnaire, 73 completed it, and 61 were ultimately included in the analyses. Twelve participants were excluded on the basis of implausible data (e.g., stating that they were female or were exclusively interested in adults). Forty-four were non-forensic (47% of the total sample) and 17 were forensic participants (18% of the total sample). A total of 158 Internet participants called up the study using a different study link. Of these, 65 started the questionnaire, 39 completed it, and 33 were ultimately included in the analyses (35% of the total sample). Six participants were excluded on the basis of implausible data (e.g., stating having recognized their sexual interest in children for the first time at the age of 4 years). The final sample consisted of 94 participants (for sample characteristics, see Table 2) with 55 participants in the mutable and 39 participants in the immutable condition.
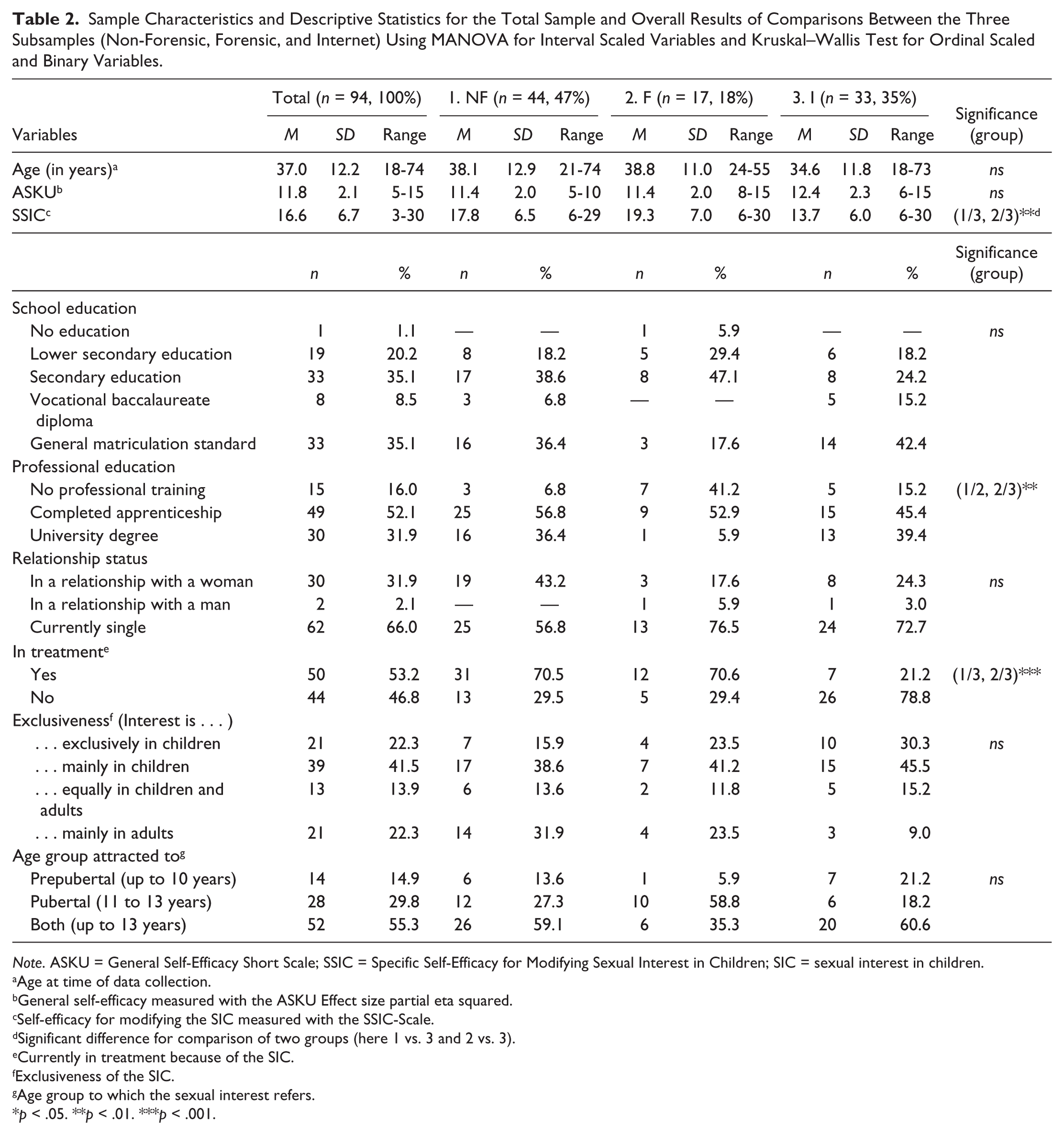
Sample Characteristics and Descriptive Statistics for the Total Sample and Overall Results of Comparisons Between the Three Subsamples (Non-Forensic, Forensic, and Internet) Using MANOVA for Interval Scaled Variables and Kruskal–Wallis Test for Ordinal Scaled and Binary Variables.
Note. ASKU = General Self-Efficacy Short Scale; SSIC = Specific Self-Efficacy for Modifying Sexual Interest in Children; SIC = sexual interest in children.
Age at time of data collection.
General self-efficacy measured with the ASKU Effect size partial eta squared.
Self-efficacy for modifying the SIC measured with the SSIC-Scale.
Significant difference for comparison of two groups (here 1 vs. 3 and 2 vs. 3).
Currently in treatment because of the SIC.
Exclusiveness of the SIC.
Age group to which the sexual interest refers.
p < .05. **p < .01. ***p < .001.
Internet and non-forensic participants reported a higher level of professional training than forensic participants. Non-forensic and forensic participants were more likely to be in treatment currently as a result of their sexual interest in children than were the Internet participants. It should be noted that the outpatient centers also recruited men who had already completed the treatment program or those who had not yet entered the program but were in the diagnostic phase, which explains why not all the non-forensic and forensic participants were currently in treatment.
Statistics
To test overall differences between the three subsamples, we used MANOVA for interval scaled variables and Kruskal–Wallis Tests for ordinal scaled and binary variables. For pairwise post hoc comparisons, we used the Scheffé Test as it is considered suitable for use with differing sample sizes (Rönz, 2001). We used t tests for interval scaled variables, U tests for ordinal scaled, and chi-square tests for nominal scaled and binary variables to ensure equivalence of the two condition groups with regard to demographic and control variables. To test the three hypotheses, we conducted a multifactorial variance analysis (2 × 3 ANOVA) with the factors condition (mutable and immutable) and subsample (non-forensic, forensic, and Internet). According to Hypothesis 1, we expected to find a main effect for condition; according to Hypothesis 2, we expected to find a main effect for subsample; and according to Hypothesis 3, we expected to find an interaction effect between condition and subsample. For subsequent comparisons between the two conditions within the three subsamples, we used the U test to clarify the manipulation effect in detail as it is suitable in samples that are not normally distributed, and/or those that are of different sizes (Conover, 1980). Because multiple testing took place, we adjusted the significance level in accordance with Bonferroni (Abdi, 2007). All statistical analyses were conducted using SPSS v.15.0.1 (IBM SPSS Statistics, IBM Corporation, Armonk, NY, USA).
Results
Descriptive Statistics and MANOVA
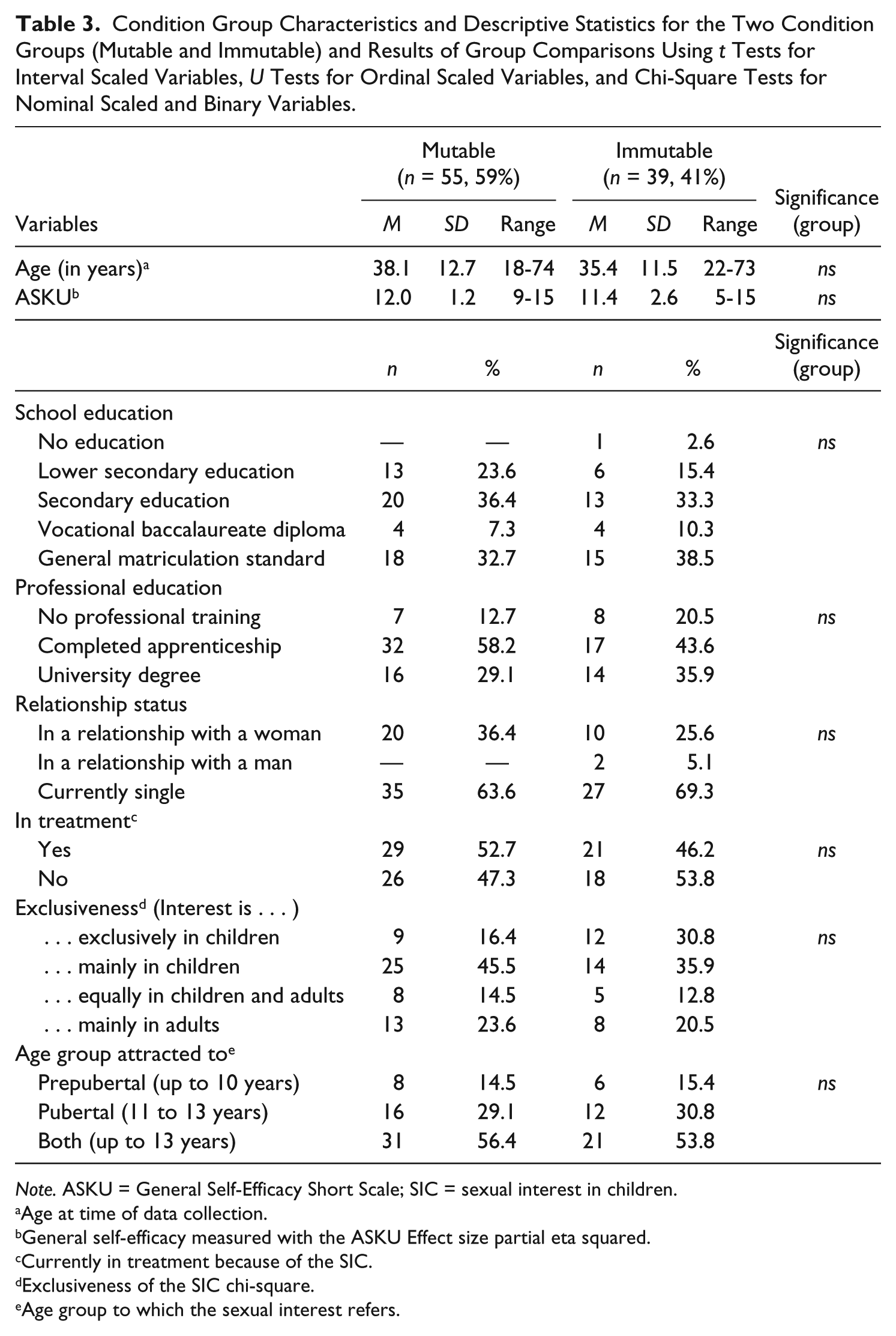
Non-forensic and forensic participants reported significantly higher SSIC scores than the Internet participants (Table 2). The two condition groups showed no differences with regard to demographic and control variables (Table 3).
Condition Group Characteristics and Descriptive Statistics for the Two Condition Groups (Mutable and Immutable) and Results of Group Comparisons Using t Tests for Interval Scaled Variables, U Tests for Ordinal Scaled Variables, and Chi-Square Tests for Nominal Scaled and Binary Variables.
Note. ASKU = General Self-Efficacy Short Scale; SIC = sexual interest in children.
Age at time of data collection.
General self-efficacy measured with the ASKU Effect size partial eta squared.
Currently in treatment because of the SIC.
Exclusiveness of the SIC chi-square.
Age group to which the sexual interest refers.
2 × 3 ANOVA
There was no main effect for the factor condition, which means that the two condition groups did not in general differ in their SSIC score. We also found a significant main effect for the factor subsample, indicating that the three subsamples differ in their SSIC score. This main effect explained 11.7% of the variability in the SSIC scores. Our analysis also revealed a significant interaction between condition and subsample, meaning that whether the two condition groups differ in their SSIC score or not, depended on subsample membership. This effect explained 8.8% of the variability in the SSIC scores (Table 4).
Results of the Multifactorial Variance Analysis (2 × 3 ANOVA) With the Factors Condition (Mutable: n = 55 and Immutable: n = 39) and Subsamples (Non-Forensic: n = 44, Forensic: n = 17 and Internet: n = 33).
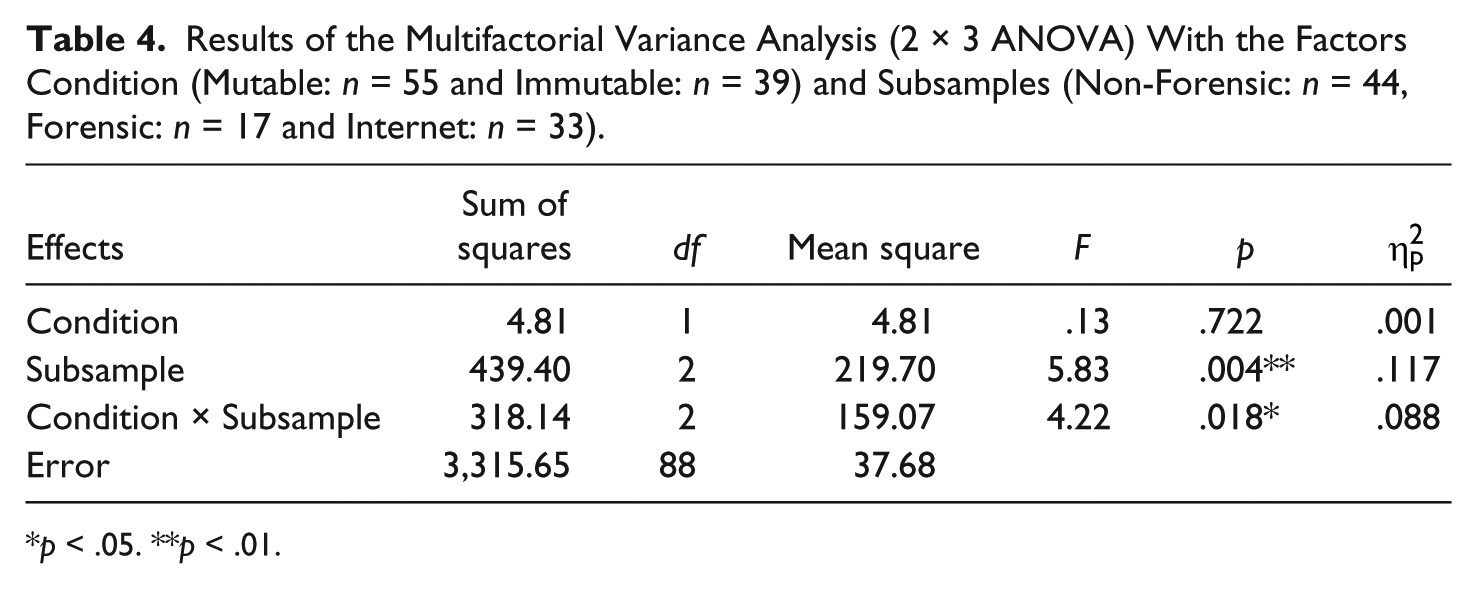
p < .05. **p < .01.
U Tests
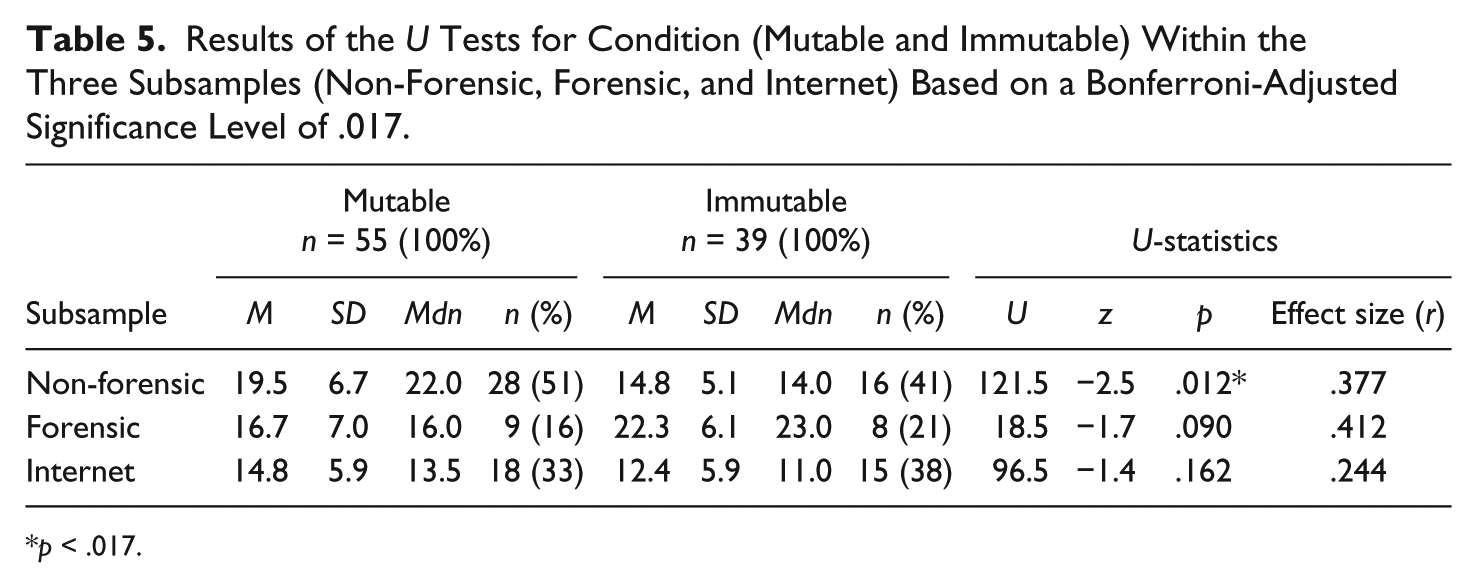
In the mutable condition, non-forensic participants reported significantly higher SSIC scores than in the immutable condition with a moderate effect size of r = .377. Forensic and Internet participants in the mutable condition did not differ in their SSIC scores in comparison with the immutable condition (Table 5).
Results of the U Tests for Condition (Mutable and Immutable) Within the Three Subsamples (Non-Forensic, Forensic, and Internet) Based on a Bonferroni-Adjusted Significance Level of .017.
p < .017.
Discussion
Our results revealed that the experimental manipulation had no overall effect on the SSIC over all three subsamples but showed an important interaction effect with subsample membership. That is, our experimental manipulation had an effect on the SSIC depending on the subsample. Non-forensic participants (n = 44) reported a significantly higher SSIC score in the mutable condition (n = 28) than in the immutable condition (n = 16). Forensic (n = 17) and Internet participants (n = 33) evinced no significant differences in their SSIC between the mutable and the immutable condition.
We assume that one explanation for these results might be the relationship between self-efficacy and motivation to change one’s own SSIC, as indicated by previous results (Tozdan & Briken, 2015b). The conviction that one is able to change something does not necessarily include the motivation to change it. Self-efficacy and motivation have therefore been dealt with separately in the research (e.g., Bandura, 1977, 1997; Schwarzer, 2001). Nowadays, self-efficacy is seen as a key to behavioral motivation (Bandura, 1977), and additionally, it has been shown in general to be a strong predictor for motivation to change (Schwarzer, 2001). The non-forensic participants in our study entered treatment voluntarily, which means that they may have had a stronger intrinsic motivation to change compared with those of the other two subsamples and thus may have responded differently to our experimental manipulation. A second explanation might be the relatively low intensity of the manipulations. We only claimed verbally that the majority of experts either consider pedophilia to be flexible/changeable or to be stable/immutable. Had we included fictive facts and numbers based on scientific research then this might have resulted in stronger effects in forensic and Internet participants as well. A third explanation might be the small subsample sizes: A stronger manipulation effect on the forensic and Internet participants could possibly be visible within larger samples.
We furthermore found that—independent of the condition—the three subsamples significantly differ from each other in their SSIC score: Non-forensic and forensic participants reported a higher level of SSIC than Internet participants. One reason for this might be the fact that the former two subsamples were more likely to be in treatment due to their sexual interest in children. Therapeutic interventions might have an increasing effect on clients’ self-beliefs even if they are not directly addressed within the therapy. With regard to these differences between various subsamples, our results confirm those of previous studies of men from different contexts who have a sexual interest in children (Tozdan & Briken, 2015b; Tozdan et al., 2015).
One further result seems notable, even if not significant. Forensic participants in the mutable condition reported a lower SSIC than in the immutable condition, which was contrary to our expectations. We assume that this could be the result of the fact that the forensic participants had already committed a sexual offense against children and had therefore already been penalized for their crimes by the justice system. Being told that the sexual interest in children that caused them to offend is changeable may suggest that it would have been possible to desist from the offense. This would increase personal responsibility and make it more difficult to justify the offense to oneself. It is possible that this is why they had to report in a direction that shows that their sexual interest in children is not changeable. In contrast, being told that sexual interest in children is immutable suggests that they cannot change in the future and will probably offend again. This would damage their sense of self-determination and predict a negative future that includes being imprisoned again. This is perhaps why they had to state that their sexual interest in children is changeable.
Regarding the assessment of the main outcome with the SSIC-Scale, Credé et al. (2012) stated that short scales might have disadvantages for the inferential statistical testing of a hypothesis, as their reduced psychometric quality might increase the probability of α and β errors (Credé et al., 2012). Seen from this perspective, the use of the SSIC-Scale might have led to higher α and β errors which might in turn explain in particular the non-significant results presented here.
Limitations
The results presented here are limited by the subsample sizes. Furthermore, online studies are limited by a lack of knowledge about participants due to their anonymity. All the measures were based on self-report and were not validated by external assessment, for example, by therapists. However, at least for the non-forensic and forensic subsample, we consider this to be fairly negligible because the participants had been recruited by experienced therapists within an outpatient treatment context.
We used different subsamples (non-forensic, forensic, and Internet participants) and tried to control for a selection bias in the experiment by means of a randomized distribution of participants within the condition groups. However, the sample as a whole is definitely not representative of all men who have a sexual interest in children, and the subsamples are probably biased as a result of other factors such as the willingness to participate in scientific studies or a personal interest in the topic of the study. The forensic subsample in particular may be biased as they were mandated by court to enter treatment and penalized when they refused. They were however not penalized at all if they refused to take part in the study. These participants probably took part in our study more out of a concern relating to negative consequences than as a result of their own motivation, and this might in turn have had an impact on their response behavior.
Although we assessed some control variables (general self-efficacy, exclusiveness of the sexual interest in children), we certainly could not have managed to sufficiently assess all possible confounding variables that are related to sexual interest in children or the SSIC. In some cases, for instance, pedophilia can be associated with hypersexuality (Kafka & Hennen, 2002; Klein, Schmidt, Turner, & Briken, 2015), including extensive and problematic levels of child pornography consumption associated with compulsive masturbation (Kafka, 2010). It may be assumed that the development of a sexual interest in children could be influenced by such hypersexual behavior as a result of interaction effects. Another confounding variable that could have been assessed within the forensic subsample in particular is psychopathy. It was shown to be a reliable predictor of reoffending behavior among sex offenders including child molesters (Hanson & Morton-Bourgon, 2005). Moreover, child molesters with a combination of psychopathy and pedophilia were found to be most likely to reoffend (Seto, 2009). It can be assumed that the levels of psychopathy in the participants within the present study might have an impact on the experimental manipulation effect.
Our experimental design itself can be seen as an additional limitation. We cannot guarantee that our participants believed the information presented to them. It might be possible that participants discovered the experiment while doing their own research into current scientific research questions which suggest study designs like the one presented here. This may be the case with the Internet participants in particular, as the core community of this information platform is involved in a continuing discussion of the question as to the (im)mutability of sexual interest in children. Moreover, we did not establish a typical control group in which participants would have received neutral information not intended to have an impact on the SSIC. The reason for this was the assumption that the sample sizes would be too small if we were to establish a third condition group.
The SSIC, the main outcome measure, was assessed with a short scale consisting of six items. As mentioned earlier, this fact has to be noted as a further limitation as short scales reduce reliability and validity values under certain circumstances (Credé et al., 2012). Having said that, empirical results do exist which demonstrate that losses in psychometric quality are acceptable in some constructs (e.g., Gosling, Rentfrow, & Swann, 2003; Kemper, Lutz, & Neuser, 2011; Wood, Nye, & Saucier, 2010)
Due to these limitations, the validity and generalizability of the present results are probably restricted.
Conclusion
Conclusions for Further Research
A replication of the present study is deemed necessary and should include some modifications according to its limitations. Further research should also examine the relationship between the SSIC and actual sexual interest in children as well as their possible interaction within developmental processes. One research proposal might be the investigation of intervention effects as treatment progresses. Regarding the SSIC and its development, outcome measures of special interest might be the actual extent of the sexual interest in children as well as its development and motivational processes for changing one’s sexual interest in children. Moreover, future research should investigate the different preference age categories: being interested in (peri)pubertal children (aged from 11 to 13 years) may be qualitatively different from being interested in prepubertal children (aged up to 10 years).
Conclusions for the Clinical Practice
Our results indicate that clinicians have to be aware of the possible impact of verbal information relating to the (im)mutability of sexual interest in children. Even if it remains questionable as to whether pedophilic men respond sensitively to such information as this, in our study at least certain participants did, that is, those who do not have a criminal history of sexual offenses against children, are not court mandated, and are maybe motivated to change their sexual interest in children. Presenting these individuals with the simple information that pedophilia is always considered stable and immutable may decrease their self-beliefs regarding their ability to modify their sexual interest in children by means of their own competencies. This might thus decrease their motivation to change their sexual interest in children and might thus also hinder possible actual changes in behaviors and interests. According to the literature on labeling theory (Link, Struening, Cullen, Shrout, & Dohrenwend, 1989), on the effects of a self-labeling process (Walters, 2002) and on self-stigmatization (Pasman, 2011), the assumption of the immutability of one’s sexual interest in children might become a self-fulfilling prophecy. In contrast, presenting the information that pedophilia is considered by experts to be more or less flexible and changeable may increase an affected person’s SSIC. By the same token, the assumption that one’s sexual interest in children is changeable might also become a self-fulfilling prophecy. We therefore suggest avoiding generalized and absolute statements about the (im)mutability of sexual interest in children: such statements might have serious consequences for individuals’ self-beliefs regarding their ability to change their sexual interest in children by means of their own competencies, and the long-term effects are not yet predictable. To be clear on this, we neither recommend telling every pedophilic individual that his or her sexual interest in children is changeable, nor do we recommend the opposite approach. This is because there are individuals who are exclusively interested in sex with children for whom the information that this interest is changeable might also be counterproductive: therapeutic resources could as a result be wasted on unrealizable treatment targets. Clients could also be disappointed because they have been unable to achieve an unrealistic goal. We would instead recommend an open attitude toward the possibility of changes, as scientific research on this question remains insufficient. Where appropriate (e.g., when clients have a non-exclusive sexual interest in children and are motivated to change it), clinicians may support their clients’ attempts to change their sexual interest in children and for example focus on strengthening their sexual interest in adults. Ultimately, the challenge in the future will be to differentiate between and identify what to say to whom and when.
Footnotes
Appendix
Acknowledgements
The authors thank our cooperation partners for supporting the data collection by recruiting clients within their outpatient ambulances. The authors also thank the anonymous web administrators of the information platform ![]() for supporting the data collection by publishing our study link. The platform was created by and for affected individuals and explicitly speaks out against acting on a sexual interest in children. The authors finally thank all participants for their willingness to participate in our study.
for supporting the data collection by publishing our study link. The platform was created by and for affected individuals and explicitly speaks out against acting on a sexual interest in children. The authors finally thank all participants for their willingness to participate in our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Safiye Tozdan is supported by a PhD scholarship from the FAZIT Foundation.