
Abstract
Depression is one the most common mental disorders in prisons. People living with HIV are more likely to develop psychological difficulties when compared with the general population. This study aims to determine the efficacy of cognitive group therapy based on schema-focused approach in reducing depression in prisoners living with HIV. The design of this study was between-groups (or “independent measures”). It was conducted with pretest, posttest, and waiting list control group. The research population comprised all prisoners living with HIV in a men’s prison in Iran. Based on voluntary desire, screening, and inclusion criteria, 42 prisoners living with HIV participated in this study. They were randomly assigned to an experimental group (21 prisoners) and waiting list control group (21 prisoners). The experimental group received 11 sessions of schema-focused cognitive group therapy, while the waiting list control group received the treatment after the completion of the study. The various groups were evaluated in terms of depression. ANCOVA models were employed to test the study hypotheses. Collated results indicated that depression was reduced among prisoners in the experimental group. Schema therapy (ST) could reduce depression among prisoners living with HIV/AIDS.
Introduction
Prisoner populations comprise some of the most disadvantaged and stigmatized individuals in society and mental disorders are overrepresented in prisoners (Fazel, Hayes, Bartellas, Clerici, & Trestman, 2016). A recent meta-analysis of 62 prison mental health surveys found that inmates were substantially more likely to have a psychotic illness, major depression, and a personality disorder than the general population (Fazel & Danesh, 2002).
On the contrary, the HIV epidemic has struck prisons and other places of detention around the world with particular severity. In numerous countries around the world, HIV prevalence among inmates is higher than that in the general population (Jürgens, Nowak, & Day, 2011). Jahani et al. (2009) in a review article on the prevalence of HIV/AIDS among Iranian prisoners reported that HIV prevalence during admission time and annual rate of HIV were 24.4% and 16.8%, respectively. HIV/AIDS is a considerable cause of death and disability. AIDS is a stigmatized and progressive disease that is associated with psychological difficulties (Whetten, Reif, Whetten, & Murphy-McMillan, 2008). Similarly, patients with psychological difficulties are at high risk of HIV infection (Yehia et al., 2014). In addition, people living with HIV are more likely to develop psychological difficulties when compared with the general population (Fernandez & Ruiz, 2006). Mental health problems in people living with HIV have a negative impact on treatment, allegiance to treatment, and prognosis of AIDS (Chander, Himelhoch, & Moore, 2006; Horberg et al., 2008). Awareness of being HIV positive can lead to psychological difficulties such as anxiety and depression as well as social isolation (Gitterman, 2001). Several studies have demonstrated that about half of HIV-positive people experience a variety of psychological difficulties of which depression is the most common (Jeffrey et al., 2008; Patterson et al., 2006). The likelihood of developing depression is 2 times higher in HIV-positive people than in HIV-negative comparison participants (Ciesla & Roberts, 2001).
According to the above, the connection between HIV infection and psychological difficulties is twofold. On one side, people living with HIV experience problems such as shame, stigma, and discrimination, which can cause psychological difficulties (Collins et al., 2008; Paudel & Baral, 2015). On the other, psychological difficulties such as depression and problematic substance abuse can increase risky sexual behavior, thereby increasing the chances of spreading HIV (Lee, Salman, & Fitzpatrick, 2009). A study by Adewuya et al. (2008) revealed that poorer health-related quality of life (QOL) in Nigerian participants with HIV was associated with depression. Early maladaptive schemas (EMSs) are patterns that have been formed in childhood. These patterns are emotional and cognitive and have a self-defeating theme (Young, Klosko, & Weishaar, 2003). Schema therapy (ST) is based on traditional cognitive-behavioral therapy (CBT; Young et al., 2003). The specific condition of people living with HIV/AIDS, especially in prisons, considering the initial negative experiences and failure to satisfy their basic needs, provide a favorable field for triggering of EMSs. In fact, people living with HIV/AIDS are vulnerable to harm or illness schemas (Young et al., 2003). Several studies showed that EMSs in prisoners, offenders, and HIV infected individuals are common (Baker & Beech, 2004; Chakhssi, de Ruiter, & Bernstein, 2013; Levy, 2005; Nikmanesh, Kazemi, Khosravi, & Bahonar, 2015; Pellerone, Craparo, & Tornabuoni, 2016). Reducing the activation of EMSs and developing more adaptive coping can reduce depression (Calvete, Orue, & Hankin, 2013; Orue, Calvete, & Padilla, 2014; Shimotsu & Horikawa, 2016). Cognitive therapy model (Beck, 1983) and schema theory (Young et al., 2003) are two models for explaining the development and maintenance of psychopathology including depression by integrating Beck’s (1983) cognitive model and Bowlby (1980), Young et al. (2003) identified a variety of EMSs that are hypothesized to underline several psychological disorders, including depression.In fact, Bowlby (1980) believes disorders that occurred in the early stages of life can effect on information-processing in the later stages of life. ST is an integrative form of psychotherapy developed for complex, chronic psychological disorders with a character logical underpinning and it was designed for clients for whom traditional CBT was not helpful. Young (1990; Young et al., 2003) developed ST to treat patients with chronic psychological disorders. “Early Maladaptive Schemas” are the most important elements in ST, penetrating background or personal and social patterns, formed during childhood and adolescence and affecting the individual throughout adulthood.
Some studies have shown the effectiveness of ST for depression in various groups such as patient with chronic depression and chronic disease with depression (Carter et al., 2013; Heilemann, Pieters, Kehoe, & Yang, 2011; Malogiannis et al., 2014; Renner, Arntz, Peeters, Lobbestael, & Huibers, 2016). Also, several studies indicated the efficacy of other psychotherapies (interpersonal psychotherapy, art therapy, and group interpersonal therapy) for depression reduction for HIV-positive inmates and prisoners (Gussak, 2007; Johnson & Zlotnick, 2008, 2012; Pardini et al., 2014). However, the effect of ST for depression in prisoners living with HIV was not examined.
Considering the above mentioned theoretical and research basis, this study aims to survey the effectiveness of cognitive group therapy based on schema-focused approach for reducing depression in prisoners living with HIV.
Hypothesis
It is predicted that cognitive therapy based on schema-focused approach has a different effect on depression in the experimental group as compared with the waiting list control group.
Method
Design
The design of this study was between-groups (or “independent measures”). It was conducted with pretest, posttest, and waiting list control groups (Field & Hole, 2002). It should be noted that depression is a dependent variable and ST is an independent variable.
Participants
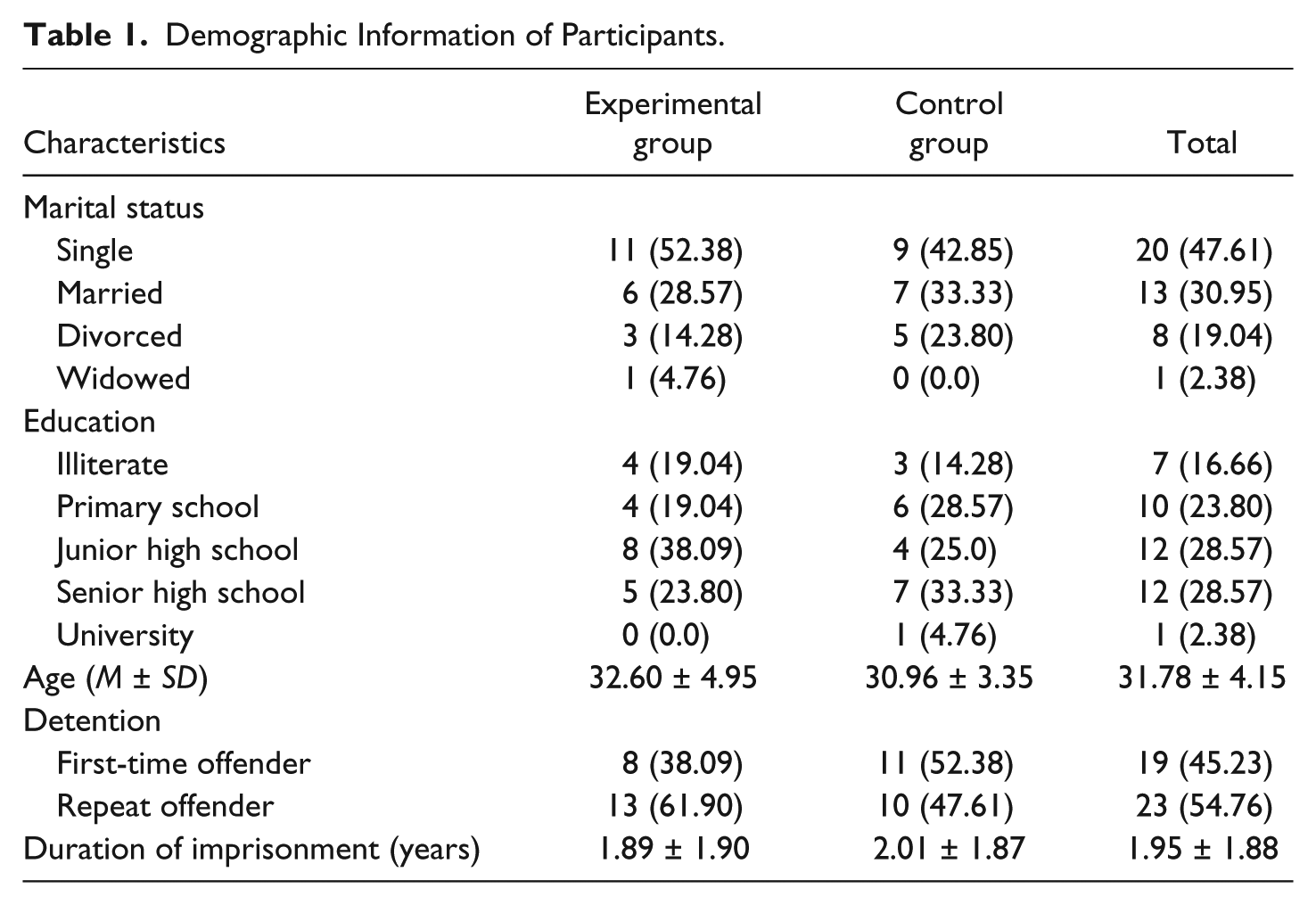
The study population included all male prisoners living with HIV in Mashhad Central Prison (67 individuals). All participants participated voluntarily in the study in response to the call for research. Based on baseline assessments including inclusion criteria, interview, and Beck Depression Inventory, 42 male prisoners living with HIV/AIDS were eligible to enter the study. They were randomly divided into two groups: an experimental group (21 prisoners) and a waiting list control group (21 prisoners). Inclusion criteria to participate in this study were (a) lack of concurrent psychotherapy; (b) the absence of psychosis; (c) lack of medical conditions that could affect depression such as thyroid dysfunction, diabetes mellitus, multiple sclerosis, and so on; (d) a lack of substance abuse when entered into the study; (e) a positive Western blot test; (f) length of incarceration more than 6 months; and (g) the absence of depression before HIV infection and imprisonment (No clinical depression diagnosis before HIV infection). Demographic information of participants such as marital status, education, age, detention, and length of incarceration is presented in Table 1.
Demographic Information of Participants.
Measures
Beck Depression Inventory (BDI-II)
The BDI-II is a 21-items self-report version of a questionnaire for depression in adults and adolescents older than the age of 13 years. Scores are based on four options (0-3). The questionnaire is a self-evaluation test and takes 5 to 10 min to finish. The scores range from 0 to 63. According to this questionnaire, depression levels placed into four groups: 0 to 13 = no or minimal depression; 14 to 19 = mild depression; 20 to 28 = moderate depression; 29 to 63 = severe depression (Mohammadkhani et al, 2010). One measure of an instrument’s usefulness is to see how intimately it concurs with another similar tool that has been accredited against information from a clinical interview carried out by an expert clinician. In this regard, the BDI-II is positively correlated with the Hamilton Depression Rating Scale with a Pearson’s coefficient (r) of .71, showing good agreement. The test also indicated a high 1-week test–retest reliability (r = .93), showing that it was not extremely sensitive to daily changes in mood (Beck, Steer, & Brown, 1996). In addition, this test showed a high internal consistency (α = .91; Beck, Steer, Ball, & Ranieri, 1996).
Schema Questionnaire–Short Form (SQ-SF)
The SQ-SF (Young, 1999) is a 75-item self-report instrument created to recognize 15 EMSs (abandonment/instability, mistrust/abuse, emotional deprivation, defectiveness/shame, social isolation, dependence, vulnerability to harm, enmeshment, failure, entitlement, insufficient self-control, subjugation, self-sacrifice, emotional inhibition, and unrelenting standards). Items are graded on a 6-point Likert-type scale ranging from completely untrue of me to describe me perfectly. Some studies have shown the reliability and validity of the SQ-SF (e.g., Hoffart et al., 2005).
Procedure
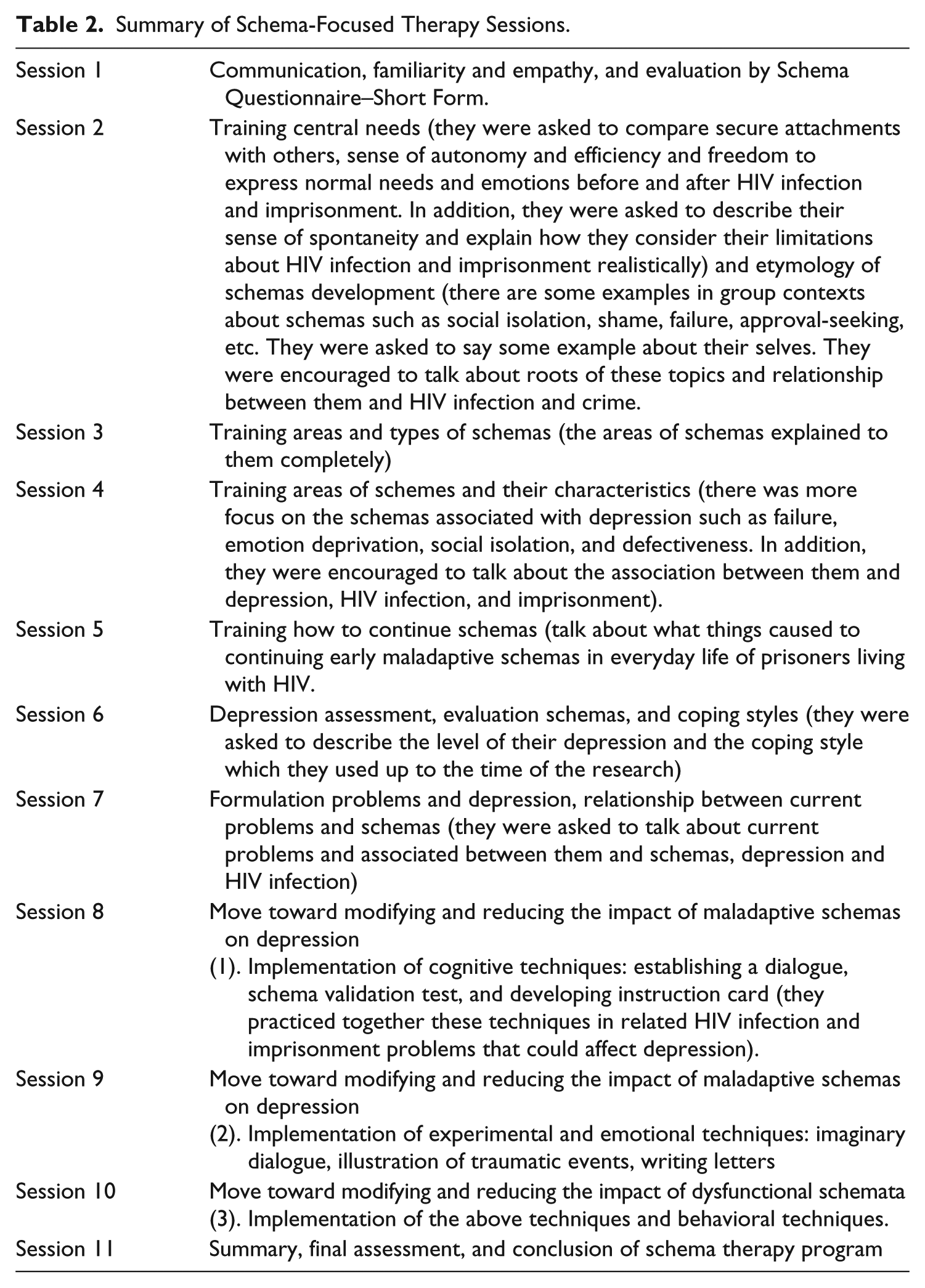
The study was conducted in “Positive Club.” This club provides clinical, psychological, and social support for people living with HIV/AIDS referred from Mashhad Central Prison. Prisoners living with HIV use the services of positive club voluntarily. Study participants completed a two-stage screening process. At the baseline assessment, interviews focused on maladaptive schemas and depression symptoms were conducted. In the next stage, they participants were asked to fill out the BDI-II questionnaire to quantify the level of depression. According to the inclusion criteria, clinical interview, and the level of depression (scores higher than 14), 42 male prisoners living with HIV/AIDS were eligible to enter to the study. They were randomly assigned to an experimental group (21 people) and a waiting list control group (21 people). The experimental group received 11 sessions of schema-focused group therapy for 90 min every week, while the waiting list control group by the end of the study received no treatment. Both groups at the end of the intervention process filled out questionnaires again, as a posttest stage. It should be noted that in the end of the study process, the waiting list control group received 11 sessions of schema-focused group therapy as well. Group therapy sessions were held without the presence of a guard, so as to maintain patient privacy, and to develop a therapeutic alliance. Group therapy was directed by two certified schema therapists. Two participating counselors received additional training hours in ST. These two counselors showed good proficiency during the training course and entered the study. It should be noted that the schema-focused group intervention can be separated into three stages. The first phase comprises four sessions of psychoeducation. In addition, clients express their problems and recall their past life events. The second phase comprises three sessions in which mostly cognitive techniques are used. Each person introduces their schemas and current problems associated with the scheme are discussed. The third phase lasts for four sessions and is mainly focused on recognizing schema-triggering events and interdiction of schema triggering in the future (Young et al., 2003). To inform the schema-focused sessions, we used from the book by Young titled Schema Therapy: A Practical Guide. Summary of therapy session used in this study is presented in Table 2.
Summary of Schema-Focused Therapy Sessions.
It should be noted that all of the levels of this study were conducted according to the Helsinki Statement on Health. In addition, all of participants filled out a consent form.
Data analysis
The data gathered from implementing BDI-II in pretest and posttest were analyzed using descriptive statistics to show demographic properties. For data inference, ANCOVA was used to test the assumption and control the effect of pretest. All stages of analyzing the data were done by SPSS-21.
Results
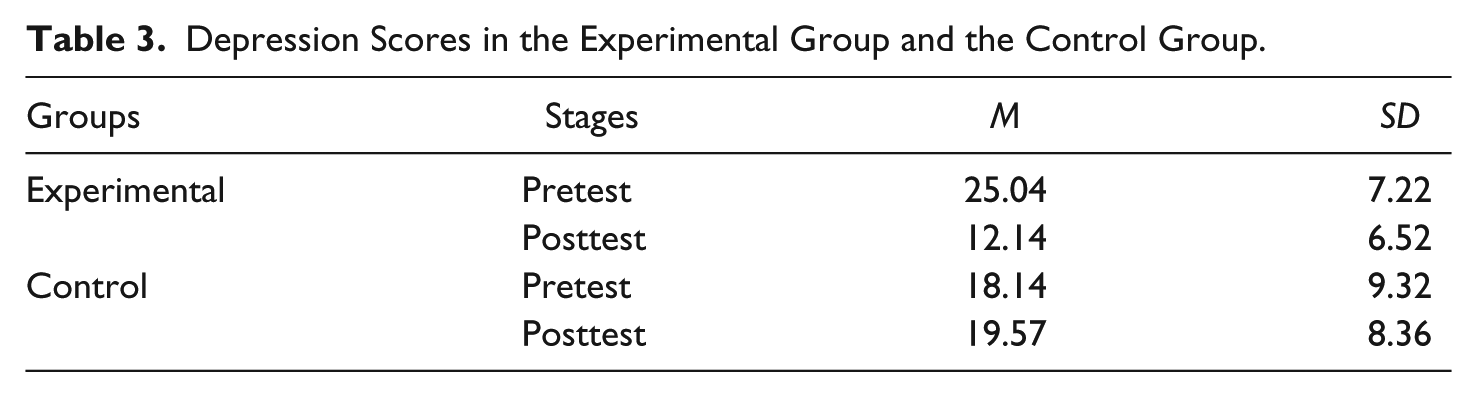
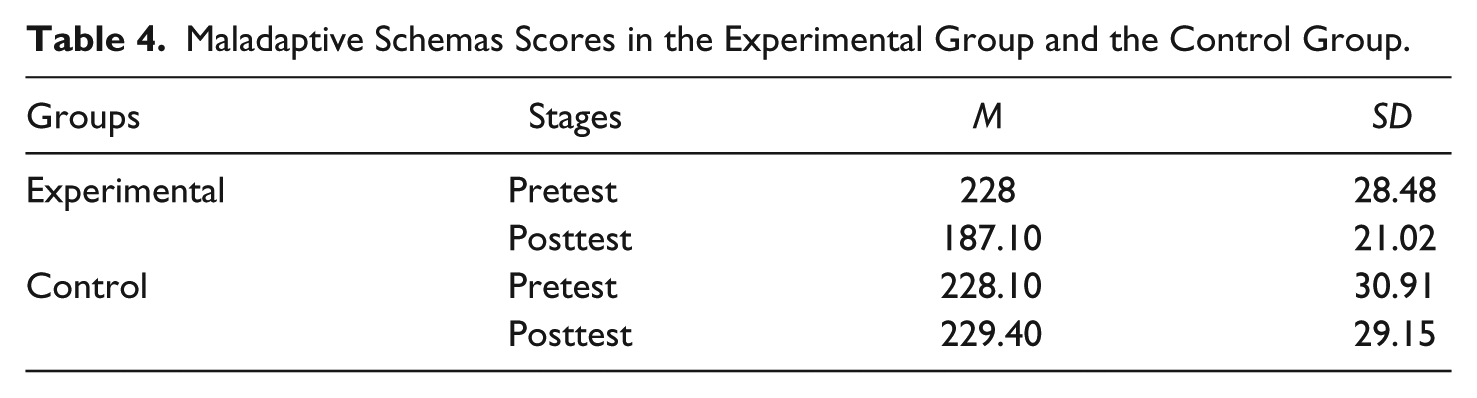
As seen from Tables 3 and 4, general information description such as mean scores and standard deviation presented in pretest and posttest are divided into experimental group and the waiting list control group in BDI-II and SQ-SF.
Depression Scores in the Experimental Group and the Control Group.
Maladaptive Schemas Scores in the Experimental Group and the Control Group.
Before presenting the results of ANCOVA to compare experimental and waiting list control groups in overall depression and maladaptive schemas scores, it should be noted that the data met all assumption of normality as indicated by the results of the Kolmogorov–Smirnov test. The results of the Levene’s test were not significant. Therefore, the homogeneity of variance assumption was supported. Also, the homogeneity of regression slopes assumption was observed for relationships between depression and pretest.
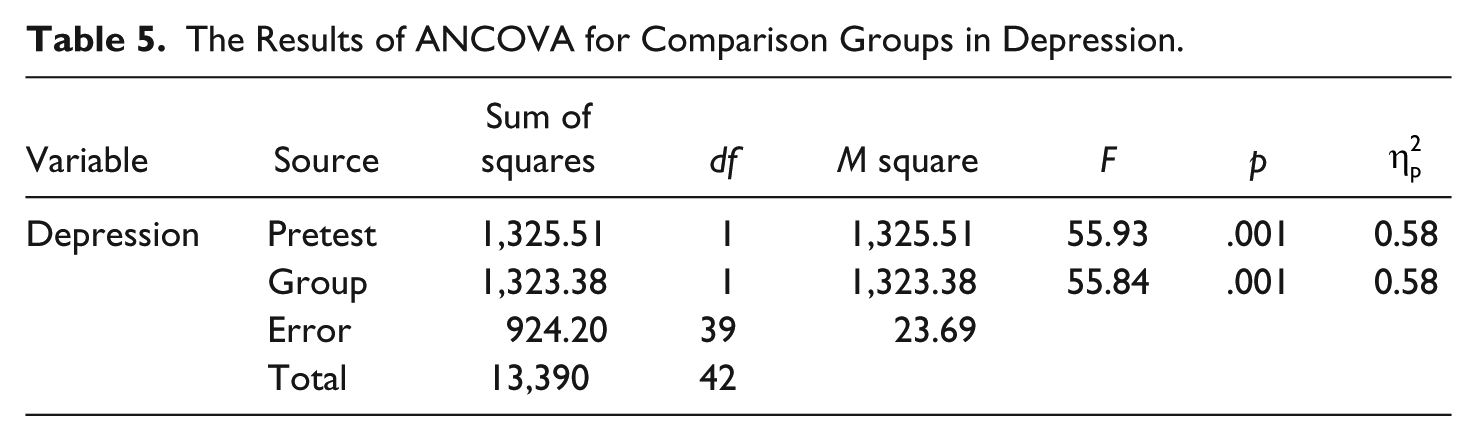
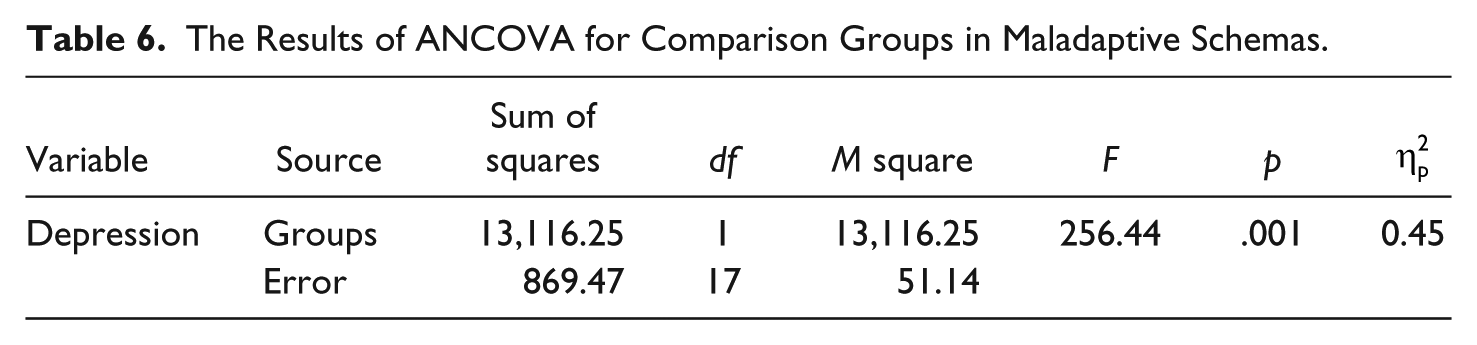
As can be seen from Tables 5 and 6, there is a significant difference in terms of depression (F = 55.84, p = .001) and maladaptive schemas (F = 256.44, p = .001) between experimental group and waiting list control group.
The Results of ANCOVA for Comparison Groups in Depression.
The Results of ANCOVA for Comparison Groups in Maladaptive Schemas.
Discussion
This study examined the effectiveness of cognitive group therapy based on schema-focused approach in reducing depression in prisoners living with HIV. As the results show, the intervention had a positive effect in reducing depression.
The results of this study are in line with the studies of Renner et al. (2016) and Malogiannis et al. (2014). They demonstrated that ST might be an effective treatment for patients with chronic depression. It should be noted that AIDS is a chronic disease (Knoll, Lassmann, & Temesgen, 2007) and chronic depression is associated with chronic disease (Audrey, 1988; Boing et al., 2012). In other studies, Carter et al. (2013) and Heilemann et al. (2011) demonstrated that ST may be an effective alternative therapy for depression.
Cognitive group therapy based on schema-focused approach was an effective strategy for reducing depression in this particular group. The ultimate goal of ST is to improve schemas. Each ST technique plays a role in reaching this therapeutic target (Young et al., 2003). Schema therapists believe that therapeutic alliance is an essential component in changing schemas. It provides a tool that allows changes (Young et al., 2003). Therapeutic alliance has been considered in all therapy session of this intervention. Cognitive, experiential, behavioral, and interpersonal strategies are other components of ST.
Cognitive strategies increase the rational awareness of patients (Young et al., 2003). Cognitive techniques which were used in this study to improve maladaptive schemas and reduce depression among prisoners living with HIV/AIDS consisted of testing the validity of schemas, reframing of schema confirmation evidence, listing pros and cons of patient’s coping strategies, conducting dialogue between the “schema side” and the “healthy side,” construction and compilation of flash cards, and schema diary (Fassbinder, Schweiger, Martius, Brand-de Wilde, & Arntz, 2016; Young et al., 2003). In addition, using experiential techniques is one of the key features in ST. Experiential techniques focus on the experience and expression of emotion that are related to past situations, which in turn leads to the maintenance of maladaptive schemas (Safran, Greenberg, & Rice, 1988). Experiential techniques help prisoners living with HIV/AIDS recognize their schemas at the emotional level. The aim of these techniques was to help patients to strengthen the rational understanding of schemas through an emotional comprehension (Fassbinder et al., 2016). Experiential techniques which we used in this intervention were Gestalt therapy psychodrama and imagery techniques and writing a letter to parents (van Vreeswijk, Broersen, & Nadort, 2015; Young et al., 2003). Empirical techniques in ST helped prisoners living with HIV/AIDS to become aware about their emotions and accept them. These techniques such as emotion reorganization, new self-learning, regulating interpersonal emotions, and relaxation helped to improve schemas. The using of mental imagery by inmates allowed them become aware of the main maladaptive schemas, understand the roots of their evolution, and relate these roots to their current life (Dadomo, Panzeri, Caponcello, Carmelita, & Grecucci, 2018). Also, imagery techniques help the inmates to not use inefficient coping styles such as avoidance and excessive compensation (Fassbinder et al., 2016). By using the writing letter technique, inmates found an opportunity to express their rights and recognize their feelings. Based on the Yang’s view (Young et al., 2003), one of the purposes of ST is helping to satisfy the patient’s unsatisfied emotions. Satisfying emotional needs during the therapy process provides conditions that improve maladaptive schemas. Maladaptive schemas come from the failure to satisfy emotional needs (Gojani, Masjedi, Khaleghipour, & Behzadi, 2017). Also, behavioral pattern-breaking is the longest and most sensitive part of schema. This part helps inmates replace consistent behavioral patterns. In fact, the target behavioral patterns are maladaptive coping styles. These maladaptive coping styles are overcompensation, avoidance, and surrender (Arntz, Bernstein, & Jacob, 2012; Young et al., 2003). All of these techniques were used in this study and they led to reduced depression in prisoners living with HIV.
Negative self-schemas were related to HIV/AIDS stigma (Varni, Miller, McCuin, & Solomon, 2012). As demonstrated by Eller et al. (2014), negative self-schemas are significantly higher in people living with HIV. Self-schemas include evaluation of self-worth (self-esteem), perceived self-efficacy in managing HIV symptoms (HIV symptom self-efficacy), and feelings related to nonjudgmental treatment for oneself (self-comparison). Generally, several EMSs are more associated with depression such as emotion deprivation, dependency, defect, failure, and social isolation (Nordahl, Holthe, & Haugum, 2005).
In addition to all these, prisoners living with HIV/AIDS benefited from Positive Club services voluntarily. Therapy sessions were also conducted in the form of group therapy. Group therapy based on a Youngian schema approach appears to be effective in reducing depression symptoms in service users who are HIV positive. Group therapy provides a context for prisoners living with HIV/AIDS who are supported and encouraged by other members. Each member can be a pattern for other members and receive the correct feedback from others (Yalom & leszcz, 2008). Therefore, voluntary participation and benefiting from group form were other factors that helped to success of this clinical trial.
This study has several limitations. Most notably, small sample size, the use of a convenience sampling technique, the loss of participants in both the experimental group and control group, a lack of follow-up, and no inclusion of covariates/confounding variables.
Conclusion
In conclusion, this study examined the effectiveness of ST for depression among prisoners living with HIV/AIDS. Based on results, it appears that using principles of ST and group therapy helps to reduce depression among prisoners living with HIV in the experimental group when compared with the waiting list control group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.