
Abstract
This phenomenological study explores how individuals in long-term recovery from substance use disorders (SUD) cope with problematic music (PM). Semi-structured interviews were conducted with 23 people in sustained recovery after attending treatment centers. Thematic analysis identified three distinct groups. The alternative group received no guidance on music consumption, experiencing three phases: recognizing and avoiding PM’s, adopting alternative music genres, and currently remaining susceptible to PM while exclusively listening to alternative genres. The ambivalent group were told regarding PM’s dangers and went through two phases: informed regarding the danger and avoiding PM, followed by developing ambivalence toward PM. The tolerant group participated in group music therapy, undergoing four phases: recognizing PM’s danger, avoiding PM and adopting alternative genres, developing tolerance by forming new associations with PM, and maintaining this tolerance during recovery. The study highlights the importance of music therapy in addressing musical triggers and supporting sustained recovery in individuals with SUD.
Plain language summary
This study looks at how people who have recovered from drug or alcohol problems deal with “problematic music” (PM) – music that evokes memories and emotions related to past substance use and may trigger cravings and pose risks for individuals in recovery. Researchers talked to 23 people who have been clean for a long time after going through treatment. The study found that people dealt with PM in different ways, and they could be grouped into three types: 1. The Alternative Group – these people didn’t get any advice about music in treatment. At first, they noticed that certain songs were triggering and avoided them. Then, they started listening to other kinds of music instead. Still, they said they are easily affected by old songs, so they stick to the new genres; 2. The Ambivalent Group – these participants were warned about the risks of certain music. At first, they avoided those songs, but over time they started feeling unsure – sometimes avoiding PM, sometimes listening to it; 3. The Tolerant Group – these people had group music therapy sessions as part of their treatment. They learned to recognize the dangers of PM, avoided it for a while, and switched to new music. Later, thanks to the music therapy they received, they were able to listen to PM again without it being a trigger, because they had formed new, healthier connections to that music. The study shows that understanding how different people react to music can help improve treatment programs. Music therapy can help people better manage emotional triggers related to music and support long-term recovery from addiction.
Introduction
Substance use disorders (SUD) have a significant impact on the health, wellbeing, daily life, social relations, and occupation of those who suffer from it (Davidson et al., 2008). Substance use disorder is a physical, psychological, and emotional compulsion to use mood altering substances such as narcotics and alcohol. As substance use continues, tolerance increases, forcing the user to increase quantities to feel the desired “rush,” regardless of the negative consequences (American Psychiatric Association [APA], 2022). According to the World Drug Report 2023 of the UN Office on Drugs and Crime (2023), new data has shown that in 2021, more than 296 million people across the globe use drugs, a gross increase of 23% over the past decade, and the number of people suffering from SUD has grown to 39.5 million, a 45% increase over the previous decade. The report also stated that only one in five people with SUD receive proper treatment, with significant differences across regions. Locally, a report published by the Israeli Center for Addictions (2022) found that one of every seven Israelis suffers from SUD, an increase of 15% since 2018. The report claimed that over half-a-million Israelis across the demographic spectrum are diagnosed with SUD, and 90% of those diagnosed with SUD are left untreated.
Treatment and subsequent recovery from SUD are a complex and difficult process, involving numerous factors (Davidson & White, 2007). Recovery is defined as: “Voluntarily sustained control over substance use, which maximizes health and wellbeing and participation in the rights, roles and responsibilities of society” (UK Drug Policy Commission, 2008, p. 6). Recovery from addiction is determined by several variables that depend on context, circumstance, and resources, such as mental health, socialness, wellbeing, economic independence, self-esteem, empowerment, and self-determination (Dekkers et al., 2020b; Kelly & Hoeppner, 2015; White, 2007). Recovery, therefore, is often seen as a long-term gradual process (Dekkers et al., 2020a; White et al., 2002).
Findings on concurrent use of music and drugs show that it may result in a conditioning effect, named here “problematic music” (PM), whereby merely listening to genres associated with substance use may induce cravings and subsequent relapse (Bensimon, 2024; Lozon & Bensimon, 2025; Silverman et al., 2023). Yet, research on the ability of people with SUD to cope with PM in the long-term is scant. The aim of the current study is to use a phenomenological qualitative approach to understand how people with SUD cope with PM from the start of rehabilitation until their current stage of recovery.
Music and Addiction
The simultaneous use of music and drugs may enhance the experience of both, creating a symbiotic relationship. In a study conducted with people with SUD during sustained recovery, participants reported experiencing a mutual enhancing effect of music and drugs during active use. They knew which combinations of substances and music genres would best enhance their experience. Combined, substance use and music can create a mutual enhancing effect, impacting users’ sensory and emotional abilities, depending on their mood (Lozon & Bensimon, 2024). This finding is supported by research (Dingle et al., 2015; Edri & Bensimon, 2019; Lozon & Bensimon, 2024; Silverman et al., 2023) illustrating that certain music genres and contextual cues can induce cravings for substances such as cannabis, nicotine, and alcohol, resulting in increased substance use.
Problematic Music
It should be noted that music in itself is not inherently problematic nor dangerous, as what is dangerous for one person may not be dangerous for another. Rather, it is the repeated experience of listening to music while consuming drugs that reinforces conditioning that may result in cues to abuse (Silverman et al., 2023). This idea is supported by research demonstrating a neurochemical connection between music-induced and drug-induced euphoria, showing that both experiences activate overlapping regions in the brain (Fachner, 2017). This conditioning of music has been termed “problem music” (PM; Lozon & Bensimon, 2014; North & Hargreaves, 2006) or “dangerous music” (Horesh, 2006), aligning with studies that demonstrate how conditioned associations can make music a trigger for substance use (Bensimon, 2024; Edri & Bensimon, 2019). When substances are not readily available, music may take on the psychological and emotional role of substance use, acting as a buffer against repressed pain or trauma (Horesh, 2010). If music is perceived as dangerous or harmful depends on how frequently specific genres are associated with drug use, creating a strong conditioned link between them for the individual (Silverman et al., 2023).
Music Therapy for SUD Clients
One method of enabling recovery from SUD is through music therapy (MT). MT entails “a structured intervention process in which the therapist assists individuals in fostering health, utilizing music experiences and the resultant relationships as potent catalysts for change” (Bruscia, 1998, p. 20). MT sessions are conducted either individually or in groups, encompassing a diverse range of activities that engage therapists and clients in musical recreation, improvisation, composition, and relaxation (Bruscia, 2014). Systematic reviews studying the efficacy of MT for SUD clients have found music therapy interventions to be beneficial in addressing recovery issues by reducing depressive symptoms, increasing willingness to receive treatment, and changing patterns of active substance use (Carter & Panisch, 2021; C. Ghetti et al., 2022; Hohmann et al., 2017; Megranahan & Lynskey, 2018). For example, Carter & Panisch’s (2021) systematic review demonstrated that MT can be as effective as typical therapeutic treatments in reducing depressive symptoms and enhancing psychosocial well-being, promoting clients’ motivation for treatment and fostering positive behavioral changes related to addiction. Conversely, Megranahan and Lynskey’s (2018) review, highlighted a lack of high-quality evidence supporting creative art therapies for SUD treatment. However, their results showed that MT has a strong positive impact in increasing treatment readiness among individuals with SUD.
MT for SUD clients can accomplish its therapeutic goals by facilitating user participation, equality, and self-agency (Rolvsjord, 2010; Solli & Rolvsjord, 2015). These principles align with strength-based approaches (McCashen, 2005), which highlight clients’ inherent strengths and capacities while recognizing that an exclusive focus on deficits would be limiting. As noted in the literature, within MT, a collaborative relationship is established between the therapist and client, where empowerment is fostered within safe boundaries. This supports the development of self-efficacy and shared responsibility, which are of significance for individuals in recovery from SUD, where rebuilding agency and trust in one’s own capabilities are central therapeutic tenets (Rolvsjord, 2014; Stige, 2002). Thus, by recognizing the clients’ capabilities within the context of MT, therapy reinforces a client’s ability to use music as a tool for empowerment and self-growth (Rolvsjord, 2006).
MT is one of the many methods of treatment used in substance abuse treatment programs (Aletraris et al., 2014; Buino & Simon, 2011). One of MT’s goals for clients with SUD is to address potential musical triggers related to their addiction by introducing problematic music in a safe and contained environment, where clients are supported by the therapist and, if done in a group, by their peers. At the beginning of the process, clients identify their PM by listening to their favorite songs or musical pieces and assessing which constitute triggers and which do not. It may be suggested that triggers can be effectively addressed through cue-exposure therapy, in which clients are deliberately exposed to PM in order to extinguish conditioned responses (Conklin & Tiffany, 2002; Loeber et al., 2006). Alternatively, systematic desensitization may be employed, gradually introducing clients to their triggers until they develop the capacity to manage them more effectively (Stamou et al., 2016, 2017). Subsequently, clients learn how to cope with their PM and how to neutralize its effect (Horesh, 2006). Intervention is typically introduced once clients have developed basic emotional regulation skills, minimizing the risk of relapse. Nonetheless, the precise timing may vary depending on the individual needs and requirements of the client (Bruscia, 2014).
Music therapists specializing in treating SUD clients often employ techniques such as musical improvisation (C. M. Ghetti, 2004), songwriting (Vega, 2017), music-assisted relaxation (Borling, 2011), and group drumming (Gardstrom et al., 2013). These techniques can be utilized within a variety of models, which are frameworks incorporating a set of methods, treatments, and theories aimed toward constructing a framework by which the treatment operates within (McFerran et al., 2023). The most common models employed in MT are: Benenzon music therapy, based on Jungian theory; Behavioral music therapy, based on behavioral-psychology; Nordoff Robbins model/Creative music therapy, based on humanistic psychology; Analytic music therapy, based on Freudian psychoanalytic theory; and, the Bonny method of guided imagery and music, based on transcendental and humanistic psychology (for a review see McFerran et al., 2023). More recent models include, for example, the resource-oriented music therapy, which encompasses positive psychology and empowerment theory, techniques tend to focus on the client’s preferred music and techniques selected by the client (Rolvsjord, 2010). The vocal music psychotherapy model focuses on the use of vocal improvisation, songs, and dialog within a therapist-client relationship, promoting and encouraging inter-personal growth and change (Austin, 2008).
Many rehabilitation centers incorporate MT as a complementary treatment. For instance, the San Diego Detox and Treatment center in the US uses MT in conjunction with art therapy, family systems approach, cognitive behavioral therapy (CBT), and dialectical behavioral therapy (DBT) to engage clients in music-related activities (Sandiegodetox, n.d). Similarly, the UK Addiction Treatment Centers utilize MT alongside CBT and DBT, encouraging emotional expression through music (Hari, 2023). In Israel, Kfar Izun offers MT as part of its therapeutic arts approach, which includes psychodrama and art therapy (Izun, n.d). A recent study on music-based interventions for formerly incarcerated individuals with substance use disorder found that MT helped participants develop essential recovery resources, improve interpersonal relationships, and become aware of triggers (Bensimon, 2024).
The Current Study
Studies on the effect of PM on people coping with SUD primarily focus on short-term effects of MT in rehabilitation programs and its capacity to assist clients in attaining rehabilitative goals and maintenance (Hohmann et al., 2017; Megranahan & Lynskey, 2018; Silverman et al., 2023). Research examining how people with SUD cope with PM over the long term remains limited. Given that recovery is a long-term and often non-linear process (Keith et al., 2022), it poses challenges for quantitative or short-term research methodologies (Bjornestad et al., 2020). While large-scale longitudinal studies could offer valuable insights into long-term coping strategies, they are presently limited in number, possibly due to their resource-intensive nature or limited ability to follow up with participants (Kellett et al., 2019). The current study thus serves as a foundational step in addressing this gap in understanding the adverse effects of PM among individuals with SUD. Employing a phenomenological qualitative approach, it focuses on the lived experiences of individuals with SUD, retrospectively exploring their journey from active use to sustained recovery. Thus, the current study has the potential to contribute foundational insights that may inform future research within established developmental frameworks and research models in SUD research.
Method
Participants
As can be seen in Table 1, 23 Israelis (16 males and seven females), aged 26 to 65 (M = 40), participated in the study. Of the participants, 52% were married. Attending treatment centers (TCs) included methadone treatment (9%), mental health facilities (17%), and residential treatments (74%). The mean duration of sustained recovery was 10 years (SD = 8.1). Participants attended TCs with an average duration of 5 months (SD = 0.2). Of the 23 participants, six received group MT tailored toward SUD treatment during their stay, while the remaining 17 did not receive any form of MT. Eligibility criteria for participation in the study were, at least, 1 year of drug-free period prior to the interview date, attending a residential TC in the past, and self-identification as recovering addicts. The minimum 1-year drug-free period was set based on research indicating that 1-year of sustained recovery significantly decreases risk of relapse (El-Guebaly, 2012; Inanlou et al., 2020). Considering the difficulty in defining addiction, the current study relied on participants’ self-definition, a recognized valid method for defining this condition (Anderson & Mott, 1998; McIntosh & McKeganey, 2000).
Participants’ Demographic Information.
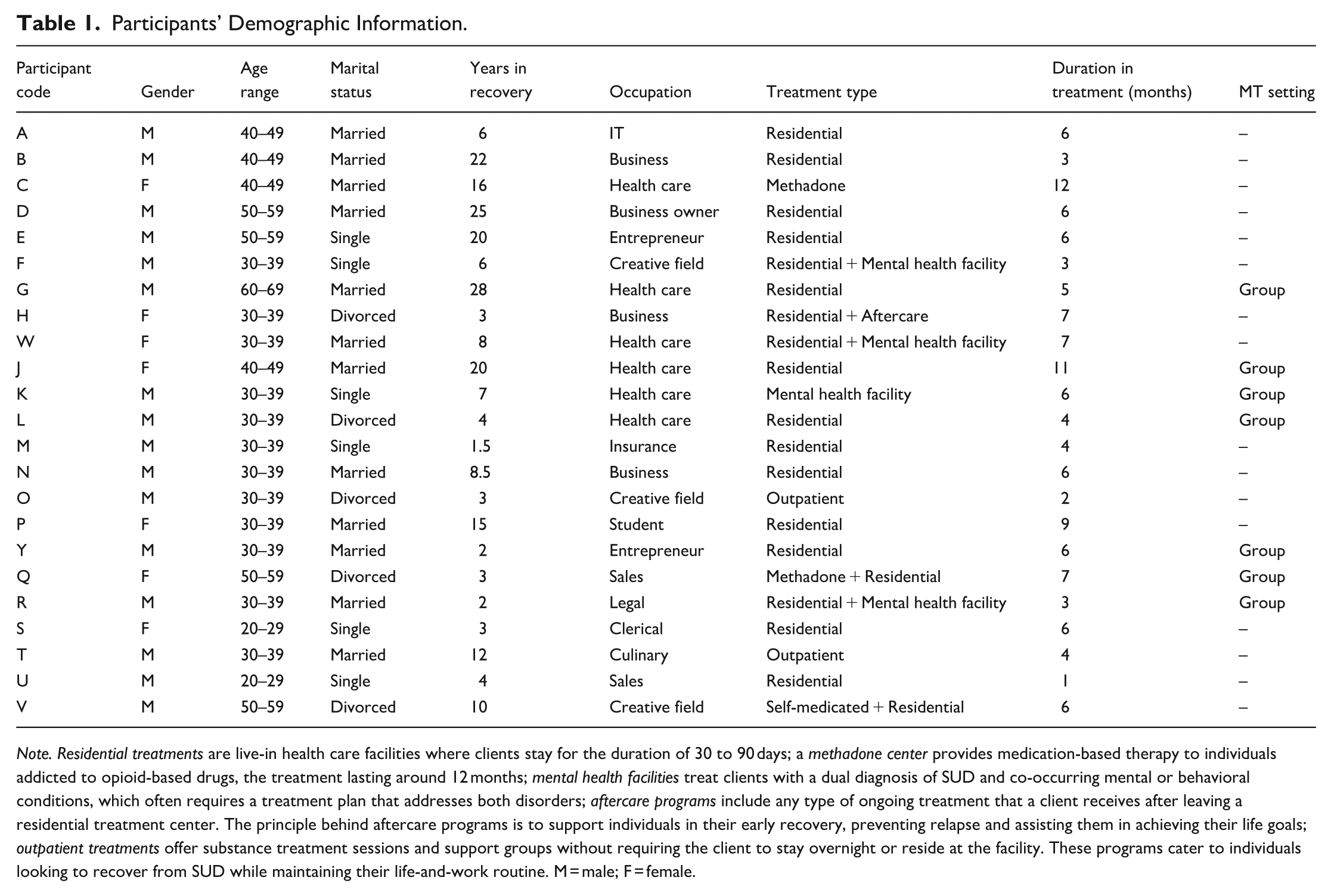
Note. Residential treatments are live-in health care facilities where clients stay for the duration of 30 to 90 days; a methadone center provides medication-based therapy to individuals addicted to opioid-based drugs, the treatment lasting around 12 months; mental health facilities treat clients with a dual diagnosis of SUD and co-occurring mental or behavioral conditions, which often requires a treatment plan that addresses both disorders; aftercare programs include any type of ongoing treatment that a client receives after leaving a residential treatment center. The principle behind aftercare programs is to support individuals in their early recovery, preventing relapse and assisting them in achieving their life goals; outpatient treatments offer substance treatment sessions and support groups without requiring the client to stay overnight or reside at the facility. These programs cater to individuals looking to recover from SUD while maintaining their life-and-work routine. M = male; F = female.
Procedure
Participants were initially recruited through snowball sampling (Cohen & Arieli, 2011). Further recruiting was done by posting notices at Narcotics Anonymous (N.A.) and rehabilitative centers to achieve data saturation. In the current study, snowball sampling involved the first researcher physically attending open AA and NA groups and asking the group leaders to suggest individuals who might fit the study’s criteria. None of the groups actively facilitated the study as representatives of NA or AA. Rather, they assisted out of willingness and desire to help others by sharing their stories and experiences. Those initial participants then recommended others who met the criteria and were willing to discuss the study’s topics. When no additional participants were being suggested, no more individuals were willing to be interviewed, and the first researcher could no longer attend in-person meetings due to the COVID-19 pandemic, an alternative approach was required. Colleagues in the field, such as those working in TCs, were approached and asked if they or their staff knew anyone who might qualify or be able to suggest potential participants. Those who were suitable and wished to participate then, in turn, suggested others. Despite its effectiveness in accessing hard-to-reach populations, snowball sampling also could have limited the diversity of the interviewee pool. By restricting interviews to a homogeneous population, snowball sampling may have facilitated over-representation of specific participants’ characteristics (Parker et al., 2019). This may have resulted in the exclusion of individuals with smaller social networks, as they were less likely to be recommended for inclusion in the sample (Daniel, 2012; Shaghaghi et al., 2011). Interviews lasted between 45 min to 2 hr. Eight interviews were conducted face-to-face, while 15 were conducted via Zoom due to COVID-19 restrictions and following research showing the Zoom platform to be a legitimate tool for establishing and sustaining rapport during interviews (Oliffe et al., 2021).
An ethical approval was obtained from the Ethics Review Board of Bar-Ilan University. Before the interview itself, an initial conversation was held with each participant where the research topic and the nature of the study were explained. Then, participants signed an informed consent form and gave their permission to record the meeting, all while guaranteeing anonymity. For anonymity purposes, participants were given pseudonyms, and all identifying details, including ethnic background, country of origin, and specific music genres, were either generalized or omitted, unless it was important to note it. Additionally, digital information was saved on a separate drive, while physical information on sheets, such as demographic and personal information, was stored in a nondescript folder in a safe location away from other research material. Given the sensitivity of the discussed issue and the potential evocation of negative emotions, participants were provided contact details of TCs and self-help groups such as Narcotics Anonymous for emotional support.
Data Collection
Semi-structured interviews (Cunningham et al., 2011) were conducted in Hebrew by the first author, allowing for deeper exploration and clarification of participants’ experiences. This approach was chosen to allow participants to elaborate on their experiences and generate novel insights (Heath & Cowley, 2004). The key questions in the interview guide focused on participants’ personal and social musical encounters during their rehabilitation at TCs. Questions were designed to elicit comprehensive responses and included: Describe your musical habits during rehabilitation; If you listened to your PM during rehabilitation, how was it like?; What led you to listen to PM after rehabilitation?; Describe what you feel today when exposed to PM; Describe your current musical tastes and habits.
Data Analysis
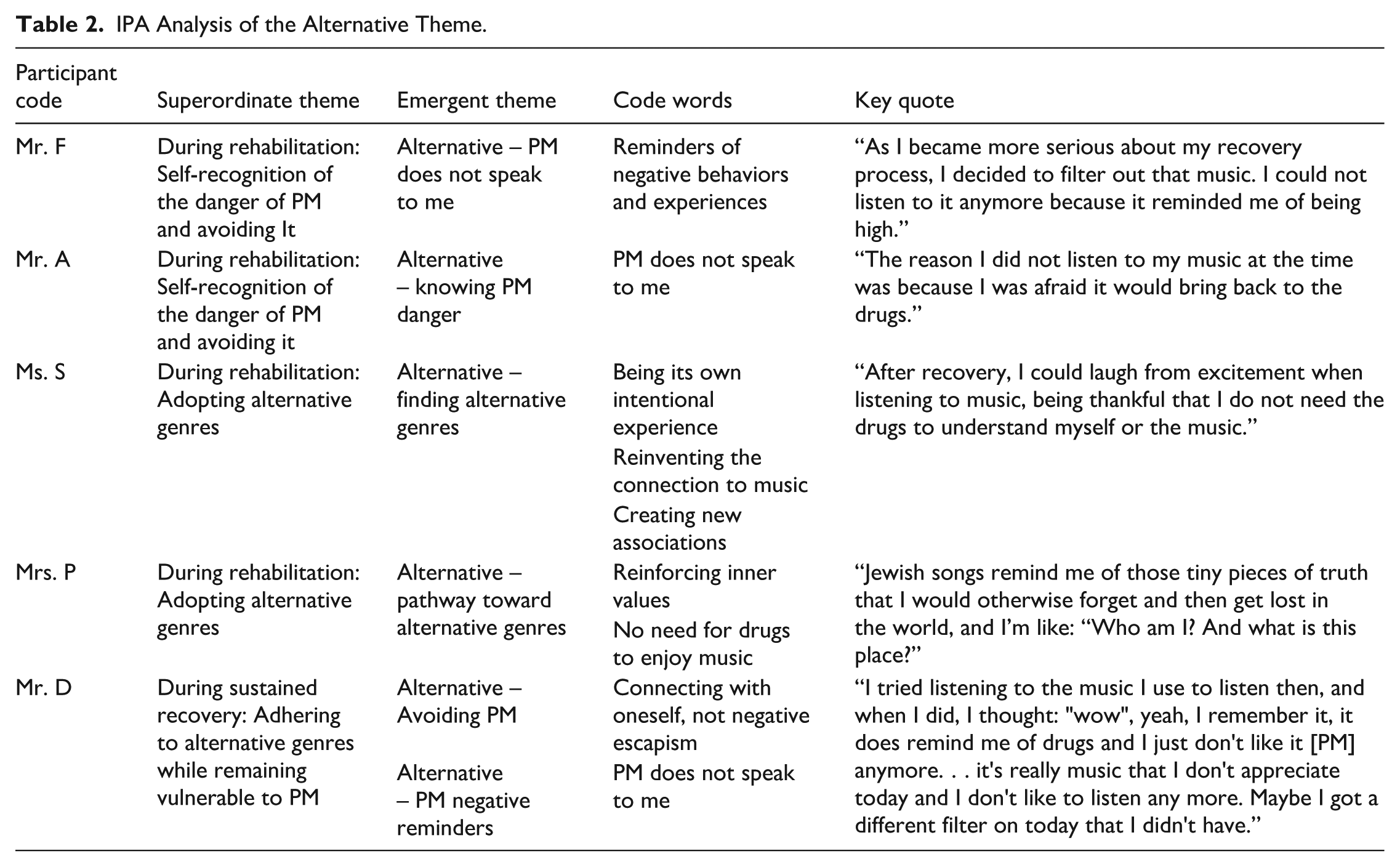
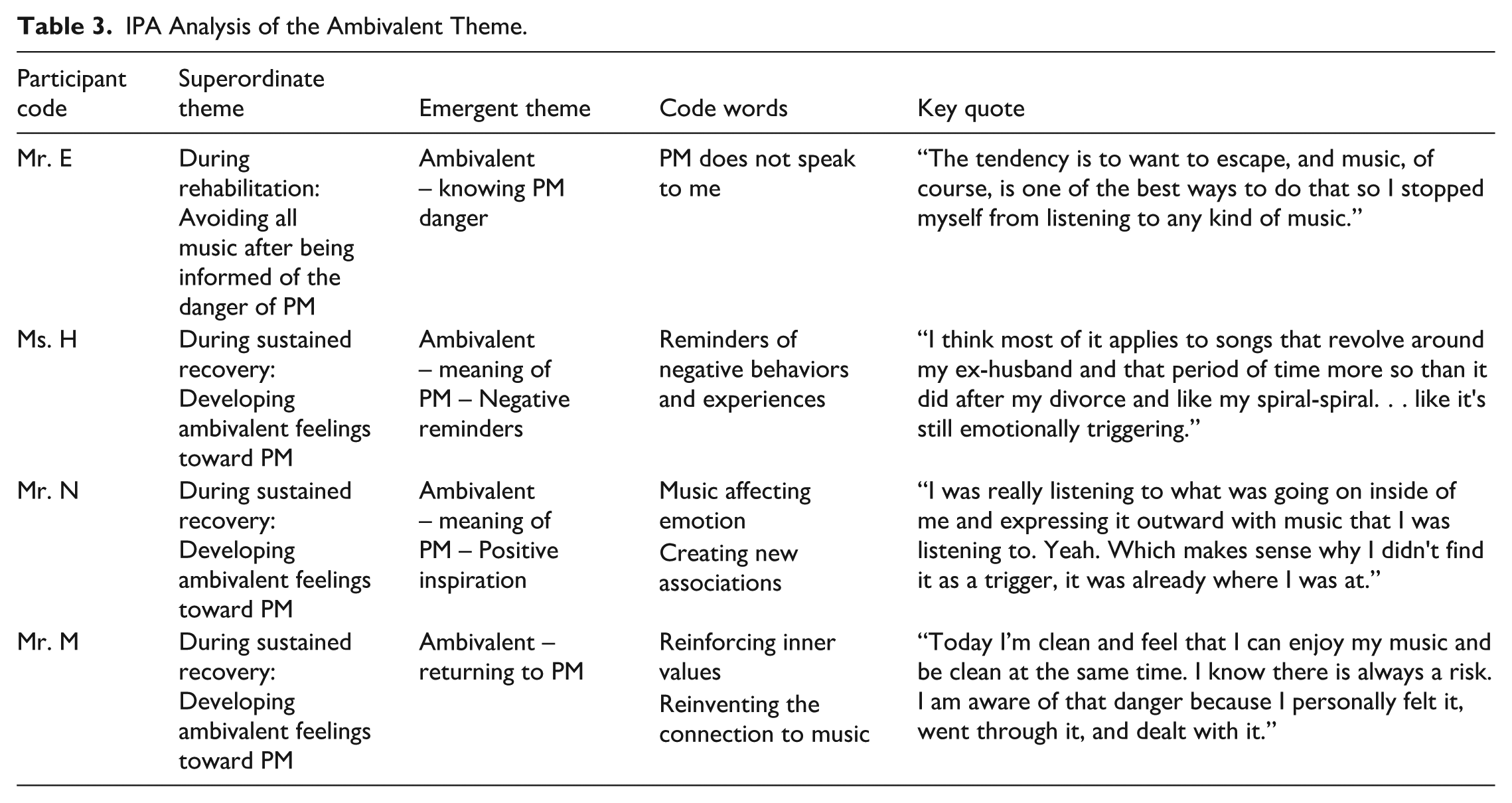
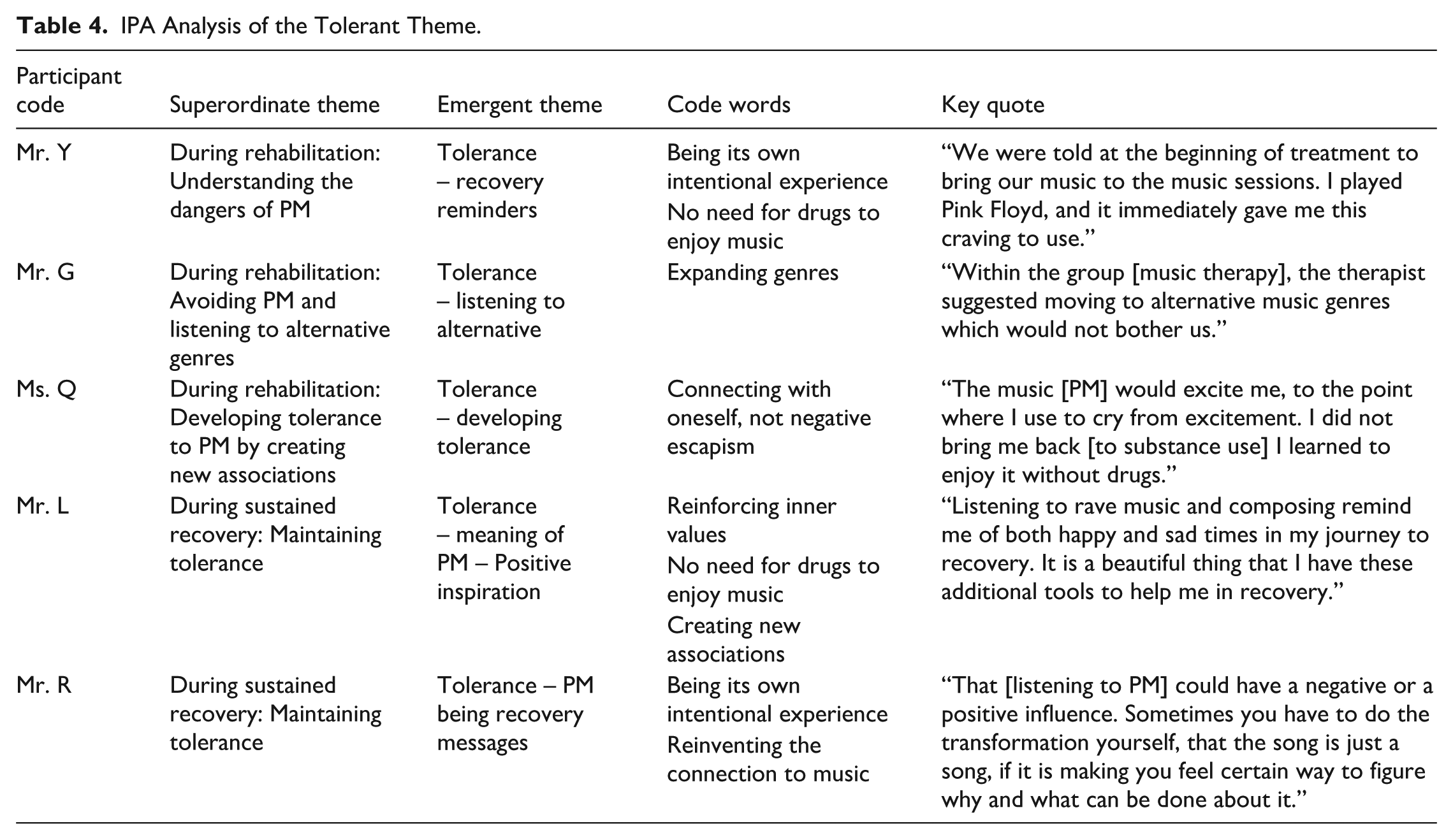
Data analysis was conducted by the first author using the following seven-step process of interpretative phenomenological analysis as delineated by Smith et al. (2021): (1) Interview transcripts were read multiple times to ensure immersion in and familiarity with the data. This was accomplished by listening to the recorded interviews and reading alongside the transcripts; (2) Exploratory comments were documented in the margins of the interviews, encompassing descriptive, linguistic, and conceptual observations. Numerous personal comments were added where it felt relevant, noting significance to any ideas and topics of interest; (3) Notes served as the basis for identifying emergent themes; (4) Data was subsequently grouped together and refined through a process of thematic integration, yielding, for example, the following initial theme: “Music, from past-to-present,” noting any changes of participants’ perception of music from their time in active substance use to currently, in sustained recovery; (5) The analysis proceeded to further refine the emergent themes by bracketing them while remaining receptive to new meanings emerging from each subsequent interview. For example, data from “music, from past-to-present” became “music reminders, from past-to-present,” with the following subthemes: “Music is a reminder of negative behaviors and experiences” and “PM does not speak to me”; (6) Patterns and divergences were then explored across the data, continuously editing the data until the final themes were created. Following the categorization and creation of multiple subthemes, three distinct groups were created, where participants were placed in groups based on their approach to music during rehabilitation: (1) Avoidance, (2) Ambivalent, and (3) Tolerance (for an expanded review of the Data Analysis see Tables 2–4; for a flowchart illustrating the data analysis process from main themes to subthemes and emergent themes, see Figure 1); (7) Lastely, relevant theoretical frameworks were considered to enable a deeper understanding of participants’ experiences, rooting the findings within broader conceptual contexts, such as DeNora (2000) for the Avoidance group or the Good lives Model (Ward & Brown, 2004) for the Tolerance group.
IPA Analysis of the Alternative Theme.
IPA Analysis of the Ambivalent Theme.
IPA Analysis of the Tolerant Theme.
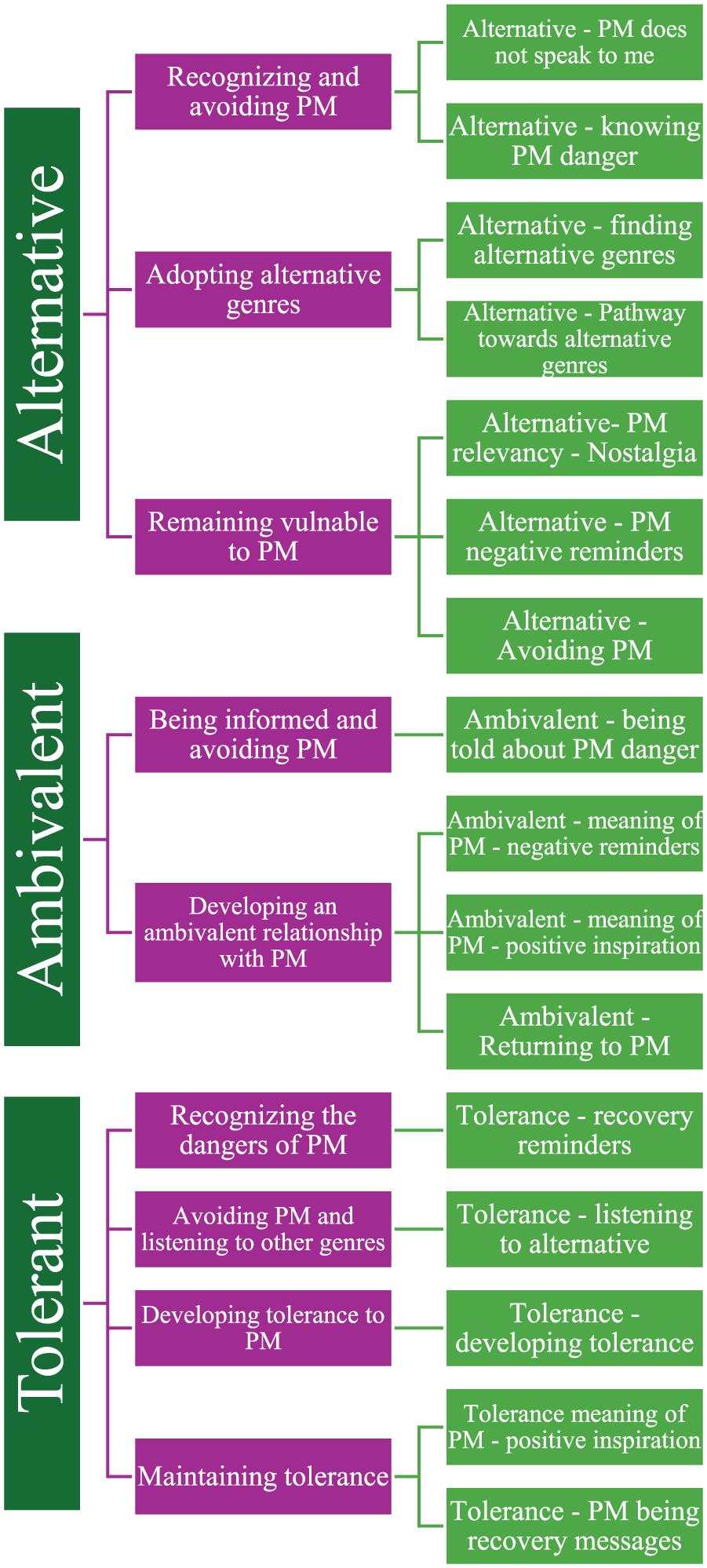
Data analysis from main themes to subthemes to emergent themes.
Reliability
Peer Debriefing
To ensure trustworthiness, peer debriefing was employed as suggested by Denzin and Lincoln (2008). The first author sent the interview transcriptions to the second author, who reviewed the analysis meticulously, offered feedback, and together with the first author, reached an agreed upon interpretation of the interviews. Both authors repeatedly examined the data and adjusted categories as needed to achieve a more comprehensive representation of the information (Morse et al., 2002). Thus, during the coding process, the analysis of the third, fifth, and eighth interviews were sent for review to a Ph.D. researcher, who specializes in qualitative research and was unaffiliated with the current study, to examine the development of the analysis. Disparities found between the two analyses were reconciled in the compilation of the final output.
Reflexivity
Since the authors’ prior views on the subject could have created bias during the interviews and analysis of the findings, a policy of reflexivity was employed to mediate the research process (Palaganas et al., 2017). At the outset of the study, the first author, who conducted the interviews, had limited direct experience with individuals living with SUD. Nonetheless, his prior research on the intersections of music, crime, and addiction – examining both its effects and applications – offered valuable insight into the profound influence music can exert on individuals. This perspective allowed him to assist interviewees in reflecting on connections between their substance use and music’s role in their lives. The participants’ insights played a pivotal role in deepening the author’s understanding of addiction and its complexities. The second author is a rehabilitative criminologist who has in-depth therapeutic understanding of SUD and the Narcotics Anonymous 12-step program. He served as a PhD supervisor of the first author and met with him regularly at different stages of the research to reflect on thoughts and feelings that had surfaced, thus increasing awareness of possible bias.
Results
The findings expanded on the experiences, resources, and processes that enabled participants to cope with PM. Data analysis revealed three distinct groups of participants, each using a different coping strategy regarding PM. The alternative group (n = 12) were not offered information regarding PM during their stay at their TC, yet recognized the danger of listening to PM on their own. The findings show this group went through a three-phase process – the first and second during rehabilitation and the third during sustained recovery: (a) recognizing and avoiding the danger of PM; (b) adopting alternative genres; and (c) as still feeling vulnerable to PM exposure, continuing to abstain from it and exclusively listening to alternative genres.
Participants in the ambivalent group (n = 5) were informed at their TCs about PM triggers. The ambivalent group described a two-phase process in the coping process, the first during rehabilitation and the second during sustained recovery: (a) being informed and thus avoiding the danger of PM; and (b) developing an ambivalent relationship with their PM.
Participants in the tolerant group (n = 6) received group MT at their TC, undergoing a four-phase process, the first three during rehabilitation and the last one during sustained recovery: (a) recognizing the danger of their PM; (b) avoiding PM and listening to alternative genres; (c) developing tolerance to PM by creating new associations; and (d) maintaining tolerance. Due to the paper’s limited scope, the findings are exemplified by selected representative quotations.
The Alternative Group
Twelve participants adopted the strategy of alternative music and acted on their own volition. Participants in this group were not informed by their respective TCs about the danger of PM, and none received MT. The process of adopting alternative music included three phases, two during rehabilitation and one during sustained recovery.
During Rehabilitation: Self-Recognition of the Danger of PM and Avoiding It
At the beginning of the rehabilitation process, participants recognized on their own the danger of listening to music genres associated with their drug use period. Ms. S recognized on her own during her time in treatment that it was imperative for her rehabilitation to be present in the moment. Despite being allowed to listen to PM, a mix of rave and rock, she abstained from it at the TC because she recognized it as a means of escapism: I chose on my own not to listen to my music, ignoring it completely. Listening to my music pulled me back into my former world since it was my recorded past. It was important for me to be in the present and cope with it, not escape back to the past.
For Ms. S, her PM, and by extension her drug abuse, served as a coping mechanism to manage her problems in life. Listening to her PM would be a reminder of her time in active substance abuse, with each lyric and beat echoing that period in her life. To avoid it, then, was more than abstaining from a soundtrack or playlist; it was a choice to anchor herself in the present and confront her current reality without any illusions or external escapism.
Mr. F’s music, a mix of rock and electronic, played a significant role in his life, as due to his occupation he engaged with music on a daily occurrence. Beyond being the soundtrack to his active addiction, his music was the means by which he supported himself. His PM was intertwined with his identity and livelihood, making his relationship with it particularly complex within the context of recovery, as the very medium that sustained him also carried powerful associations with his addictive past. When he eventually began his recovery process, at the TC, Mr. F was allowed an MP3, and in an attempt to recreate the feelings he had felt during his active addiction, he listened to his PM. Yet, during the early stages of his recovery, Mr. F understood, through self-experimentation, that the old songs impeded his recovery process, thus avoiding them: I brought an MP3 to rehab and tried to listen to songs I would hear when I was taking drugs, when I was high. I wanted to experience the same feelings. However, as I became more serious about my recovery process, I decided to filter out that music. I could not listen to it anymore because it reminded me of being high.
If, in the past, Mr. F employed his PM as a companion to his drug use, facilitating his addiction, it was only natural for him to assume that his PM would serve the same purpose for his recovery. Yet, he soon realized that instead of supporting his treatment, his PM was undermining it. In response, he chose to step away from PM, dedicating himself toward the long and demanding path of recovery.
Thus, participants gradually developed self-recognition of PM as a relapse trigger within the rehabilitative framework. However, this strategy arose not from clinical direction but from personal reflection and experimentation, leading them to identify avoidance as the most adaptive coping strategy. As they were not offered any structured guidance regarding their music, avoidance became the default option. Nonetheless, through their determination and intent towards recovery, PM became a lens through which participants negotiated the boundaries between their addiction to their emerging recovery, highlighting the role of agency and self-efficacy in sustaining treatment.
During Rehabilitation: Adopting Alternative Genres as a Personal Path to Recovery
With PM being shunned, participants sought alternative genres to fill in the musical vacuum. They selected musical pieces based on their content, focusing on those containing positive recovery messages inherent to their well-being and sustained recovery, such as being in a state of calmness and relaxation; meditating and focusing on the self; being in a state of happiness; and not allowing daily events to spiral out of control. Ms. P’s alternative genre was Jewish songs. She chose songs containing messages she identified with such as maintaining a positive perspective of the world. This kept her from spiraling into depression when life became difficult. Jewish songs, therefore, served as a tool to remind her of the positives in her life: Jewish songs remind me of those tiny pieces of truth that I would otherwise forget and then get lost in the world, and I’m like: “Who am I? And what is this place?” It became a downhill spiral towards nihilism when I stopped listening to Jewish songs. These songs reinforced the message of truth that addressed my questions. So, my music served as a lovely way of looking at the world.
Jewish songs were not a mere substitute or background noise to fill the silence left by her PM, they were a deliberate, proactive message – this is who she is. Consequently, for the past 15 years of sustained recovery, each of her songs serves as a constant reminder of her identity, a musical signpost grounding her to the self she chose to be and chooses to be every day.
As a new immigrant in Israel, Mrs. W decided to embrace Middle Eastern songs as an alternative genre (a genre resembling Turkish arabesque music). The strong connection that she felt with those songs helped her connect deeply with herself: My past identity was all based on electronic music, raves, and clubs. When I joined a treatment center here in Israel, I remember having serious questions, like, how do I listen to my usual music without running away from myself. At that point, I decided to only listen to Middle Eastern songs, which instead of making me want to run away from who I was, helped me develop a deep, inner connection with myself.
Echoing Ms. S’s experience regarding escapism, Mrs. W’s PM, and the drug use that accompanied it, functioned as a defense mechanism, shielding her from confronting her reality. By relating to a new genre, one intertwined with her present and new environment, Mrs. W was doing more than changing her playlist, she was actively committing to recovery and to herself. Thus, she would no longer flee from who she was, but begin, instead, to embrace herself fully. By selecting new genres, participants began shaping a musical identity that was increasingly distanced from their active addiction. At this stage of rehabilitation, music was no longer tied primarily to relapse triggers but was becoming interwoven with their emerging sense of recovery, reflecting both their new-found agency and the construction of new coping resources.
During Sustained Recovery: Adhering to Alternative Genres While Remaining Vulnerable to PM
Despite the elapsed time in sustained recovery, participants continued to avoid their PM, reporting that listening to it felt uncomfortable and triggered negative emotions and behaviors. This is partially attributed due to a lack of structured guidance in regards to their PM, as noted in the first subtheme. Without a positive means of resolving their musical triggers, participants persisted in the same strategy that they developed from the onset, avoidance. Mr. T initially expected to enjoy his PM, a blend of psychedelic and hip-hop. However, over the past 12 years, he has recognized that his PM elicits negative feelings and makes him feel emotionally unwell. Despite the distance and stability gained in sustained recovery, including a family and steady employment, Mr. T remains wary of his PM and the memories it stirs, reminders of his addiction that time alone cannot erase. For Mr. T, some associations run too deep; there are certain things, it seems, that even time cannot fully heal. His wariness reflects an ongoing awareness of how deeply embedded such associations can be, even within the context of a seemingly stable and structured life. Therefore, he now seeks to avoid it whenever he can, and instead listens to subgenres of rave music that are not connected to his drug use: I do not like to hear that type of [problem] music anymore. Even at work, when people put on any of these songs [from his PM] on high volume, I feel emotional pain, and ask them to lower the volume or change the song. Nowadays, I listen to subgenres of rave, like minimal techno and underground artists. I even began listening to classical music. When I listen to these new genres, I experience new feelings and connections that are not associated with drugs.
Given Mr. K’s professional background in the healthcare field, he maintains a heightened level of vigilance and self-awareness regarding his behavior. His daily experiences related to mental health and addiction treatment contribute to his sensitivity to any subtle changes that could signal a potential relapse. This continuous attentiveness reflects both his personal commitment to sustained recovery and the influence of his professional role, shaping a proactive approach to self-regulation. Thus, Mr. K acknowledges that even today, 7 years into sustained recovery, his PM, Portuguese and heavy metal, can trigger cravings. This happens when he fails to work the 12-step program, for example, when he was between sponsors. When Mr. K begins to listen to his PM rather than his current alternative genre of soft pop, a chain of events occurs which may result in a relapse: Today I listen to soft pop music. I do not typically listen to heavy metal or Portuguese music because it triggers negative behaviors, such as obsessively seeking drugs. Listening to my [problematic] music typically happens when I do not work the [12] steps. One time I neglected working the steps because I was in between sponsors, and as I was talking with my new sponsor over the phone, I caught myself listening to heavy metal, and I was like: “What the hell am I listening to?” When I listen to heavy metal or Portuguese music, I get anxious and act out. Then I feel guilty and ashamed, which can push me towards using again.
Without actively engaging in his personal work through the 12 steps, Mr. K risks slipping back into PM, which can trigger a chain of emotional and physical reactions resulting in relapse. Even with the structure of the steps, he may succeed in avoiding the music itself, but struggles to manage its effects on him. Thus, remaining vulnerable to his PM.
Participants are able to distance themselves from their musical triggers, by maintaining avoidance as their primary coping strategy. However, this strategy required them to remain constantly vigilant, lest exposure to their PM provoke a relapse. Although participants learned to manage their PM, it also left them at risk, as they never fully developed positive strategies to process or integrate their PM within their sustained recovery.
The Ambivalent Group
Five participants developed ambivalence toward their PM. Participants in this group were informed by their respective TCs about the danger of PM, but none received MT. The ambivalent group went through a two-phase process, the first phase during rehabilitation and the second during sustained recovery.
During Rehabilitation: Avoiding All Music After Being Informed of the Danger of PM
In rehabilitation, participants were informed by their respective TCs about the dangers of “people, places and things,” which refers to triggers that are connected to addicts’ social circle, milieu, and actions or items, including music. Unlike the participants in the previous group, the participants in this group were apprised of the inherent risks associated with PM, where their apprehension extended to encompass all music genres during their treatment period, fearing that music in any form might trigger cravings. Mr. E’s treatment center implemented a ban on all music on the assumption that it is a form of escapism. Despite the ban (and ethical issues that may arise from it), Mr. E remained in rehabilitation and, consequently, abstained from listening to music during his treatment, perceiving it as an obstacle to rehabilitation: They [at the residential TC] did not let me listen to music on purpose, so that I could not escape reality. They wanted me to face it. In hindsight, the hardest thing for addicts is to stay in reality. The tendency is to want to escape, and music, of course, is one of the best ways to do that so I stopped myself from listening to any kind of music.
Mr. E’s TC reinforced the very idea noted by the alternative group, PM serves as a vehicle of escapism. Yet his experience touches on a nuanced insight: people struggling with SUD often find it difficult to stay grounded in reality. His TC sought to counter this by preventing all forms of unauthorized escape, music included, in an effort to keep residents present and accountable. By doing so, these TCs fostered a fear of all music, regardless of its association to participants’ musical triggers. A fear that participants will carry throughout their rehabilitation and sustained recovery.
Mr. V’s path toward rehabilitation initially began through attempts at self-medication, as he sought to manage his recovery without a TC. However, these efforts repeatedly led him to relapse, creating a cyclical pattern in which brief periods of recovery were followed by prolonged returns to substance abuse. Confronted with the persistent nature of this relapsing and the limitations of his self-medicated efforts, Mr. V made the decision to enter a TC, seeking a more stable and supportive environment to break the cycle. In the TC, Mr. V’s rehabilitation was characterized by a highly regulated environment to the point that he was informed that music must be avoided, otherwise it can lead to drug use: “We were told that once you’re clean, you should not be in touch with certain people, not do certain things, and not visit certain places. Listening to music was definitely on that not-to-do list.” Recalling his own previous attempts at recovery, and determined to remain steadfast in his current efforts, despite and because of the ban on music, Mr. V avoided playing and listening to music while working his way toward maintaining recovery: When I was in rehab this last time, I understood things differently and became fanatical about staying clean. I avoided places where people were using [drugs] and didn’t do things that reminded me of using. So, I did everything I was told, including staying away from playing and listening to music.
Mr. V’s experience was characterized by an unwavering commitment to the principles of the TC, shaped in part by the lessons and challenges of his earlier recovery attempts. If that meant relinquishing music, due to its association with his PM, then so be it. It was a sacrifice he was willing to make in service to his recovery.
During Sustained Recovery: Developing Ambivalent Feelings Toward PM
In the months and years following treatment, participants tried returning to their PM, feeling that enough time had passed, and they developed resilience toward their PM. Participants’ accounts revealed that at first, they felt they were succeeding in reimplementing PM in their lives. However, at the time of the study, during sustained recovery, findings show that PM still aroused strong emotions similar to those evoked during active use. Several participants reported several relapses, all occurring after exposure to PM. Thus, exposure to PM seemed to pose a threat to the recovery process.
Ms. H invested a lot of effort over the past 3 years to maintain her recovery. At the same time, she worked on reinventing her connection to her PM, house music, imbuing it with fresh experiences and a new state of mind. However, Ms. H described how she sometimes still uses her PM as she did during active addiction – to numb and disassociate herself: I sometimes listen to Chainsmokers and Kygo’s music. I think I use it like a numbing agent, to get outside of myself, to numb my feelings and disassociate myself emotionally. This music evokes feelings I had when I was fucked up with Molly [MDMA] and Coke. Now, when I’m in a different state of mind and I’m happy, I hope I can handle this music without relapsing.
Ms. H embodies the dichotomy at the heart of the ambivalent group. On one hand, she attempts to reinvent her PM, forging new associations that align with her recovery and developing sense of self. On the other, she continues to use that same music as a form of escapism, a means to dull her emotions and disassociate from reality. Her experience, once again, echoes the recurring theme of music as a tool for emotional escape found throughout the findings.
Mr. M went back to listening to his PM, rave music, after finishing treatment, and experienced a reoccurring cycle of recovery-and-relapse. Mr. M could not let go of his PM because he felt it was central to his core identity. Today, one and a half years into recovery, Mr. M is struggling to maintain recovery while consciously exposing himself to PM: For many years after treatment, it was hard for me to shut the door on drugs because I couldn’t let go of my music. It was my life. Giving it up was relinquishing my image, my identity. I couldn’t do it. There were also temptations where I would go to parties and tell myself I wouldn’t use, but then I would fail and use. Today I’m clean and feel that I can enjoy my music and be clean at the same time. I know there is always a risk. I am aware of that danger because I personally felt it, went through it, and dealt with it.
Mr. M’s ambivalence characterizes itself in stark black-and-white terms. Despite his awareness and desire to sustain his recovery, he remains unable to part with his PM, though it serves as a trigger to his people, places, and things. His experiences became a part of the learning process, shaping his awareness of both the risks and the enduring pull of his PM. Yet it is an uncertain path, as his PM still holds power over him, threatening his recovery. Without the tools to effectively manage his PM, Mr. M remains vulnerable to its effects and the relapse it could trigger.
Unlike the previous group, these participants were explicitly instructed to avoid music, and only returned to their PM once they felt secure enough in recovery. The difference lies in the way each group understood the risk posed by music: those left to experiment alone avoided PM out of ongoing insecurity and concern that it might serve as a trigger, while those guided to abstain did so until they perceived the danger had passed. Yet in both cases, PM was never fully reclaimed as a positive resource, leaving participants vulnerable to its effects.
The Tolerant Group
All six participants in the tolerant group attended group MT during rehabilitation, where the risks and dangers of PM were brought up and discussed. Achieving tolerance to PM through MT included three phases during rehabilitation and one during sustained recovery.
During Rehabilitation: Understanding the Dangers of PM
Within the secure confines of MT, participants were led to recognize the risks posed by PM. At the beginning of group MT, within its safe confines, Mr. L was asked to analyze his PM, Rave. Through this process, he realized that his PM was more than just a musical preference – it served as a conduit to painful memories of past drug use and deeply rooted emotions tied to his divorce and the fear of losing his son. This realization illuminated the emotional danger his PM posed to his recovery: “I remember that we selected a song from our past, and I chose a rave song. I remember being suddenly hurled back to the past and to the familiar feelings of hopelessness and negativity. It was scary.”
Mr. Y was asked at the TC to present his PM, psychedelic rock. Mr. Y tried it out, and found it to be an immediate trigger: “We were told at the beginning of treatment to bring our music to the music sessions. I played Pink Floyd, and it immediately gave me this craving to use.” Through his experimentation within MT, Mr. Y recognized the hidden risk his PM posed to his recovery. PM revealed itself as a potential threat, a trigger capable of undermining his treatment. Acknowledging this risk marked a pivotal step in his self-awareness and healing.
Within the protected milieu of MT, participants were able to experiment with their PM while receiving structured guidance. This process allowed them to confront and reflect on the risks of their music without feeling left to face them alone. Much like an infant taking their first steps under careful observation, participants were provided the safety of understanding the dangers their PM embodied.
During Rehabilitation: Avoiding PM and Listening to Alternative Genres
Once participants recognized the risks posed by their PM, they avoided it and listened to alternative genres that created new music experiences and did not act as triggers. During MT sessions, Mr. G avoided his PM, a mix of psychedelic and mediterranean music, and instead listened to Yemenite and meditation music as alternative genres: Within the group [music therapy], the therapist suggested moving to alternative music genres which would not bother us. The therapist brought this Yemenite guy from Holland. He accompanied his music by wailing and waving his hands. I really connected to him and his music, so I copied him, waving my hands and shouting. It was fun. Or, the therapist would ask us to lie down and do breathing exercises as some sort of meditation, with calm music playing in the background. I hadn’t listened to those genres before, but after hearing them during exercise, I really connected to the music.
With the guided support of his therapist, Mr. G was introduced to unfamiliar musical genres, sounds that once lay outside the purview of his musical world. As he connected with these new genres, Mr. G began to cultivate new, meaningful experiences, ones that were drug-free and embedded in his recovery journey.
Ms. Q began listening to meditative music as an alternative genre through guided meditation exercises in MT sessions, where music such as New Age was played. Thus, she actively connected to this music, forming new associations through a new genre: At first, when I got into rehab, I completely stopped listening to music. The first time I went back to it was when I joined music therapy sessions. There was one exercise, where we would lie down on a mat and do breathing exercises in tempo with meditative music the therapist put on. After several sessions, I started feeling a connection with that music, even when I was not doing the exercises. I started enjoying it and getting really emotional when listening to it.
Through guided breathing exercises and meditative music, a genre unrelated to her history of drug use, Ms. Q found her way back to music. Similar to Mr. G, she began to nurture a new relationship with music, approaching it from a place of joy and renewal. Thus, she uncovered a fresh meaning in music, no longer as a trigger, but cultivating the seeds of what will eventually become a source of healing and vitality.
Neither participant immediately returned to their PM, rather, like the Alternative group, they needed a respite from their PM. Within group MT, exposure to other genres fostered new associations, offering participants recovery-oriented triggers instead of relapse-related ones. Accordingly, they were shown that music could be re-encountered and enjoyed on its own terms, separate from the weight of their addictive past.
During Rehabilitation: Developing Tolerance to PM by Creating New Associations
As the group MT process progressed and participants became familiar with their new alternative genres, they were ready to develop tolerance toward their PM within the safe and supportive environment of group MT. The sessions sought to neutralize the potency of PM by creating new associations through experiences that were not related to the participants’ world of addiction. When Mrs. J returned to her PM, ska music, in group MT sessions, she created new associations such as dancing to her PM, to reflect on her new place in recovery. Mrs. J’s PM was reemployed to express her joy and freedom from drugs: Music was a huge thing for me in rehab. There was a computer in the therapy room, where I would go, put my [problematic] music on and dance around. Looking back, by dancing to that music, I gave new meaning to something familiar. It was about finding those familiar lyrics, that familiar tune, but infusing it with what I was feeling at the time, the elation of no longer using.
Within the supportive space of MT, Mrs. J revisited her PM, consciously reshaping its meaning and purpose. In the past, during her active addiction, she had been a passive listener to ska music, where its upbeat rhythms a background noise to her substance use, offering distraction rather than connection. In this point in her rehabilitation, however, she actively engaged with the music, dancing to its beats, feeling the energy in her body, and transforming it into a source of joy and self-agency. By reclaiming the familiar and the comforting under new and sober circumstances, she effectively disarmed PM’s emotional potency, turning it into something both distinct and familiar – a tool of her recovery.
Mr. R introduced his PM, alternative rock, in MT group sessions, where he discovered its therapeutic properties. During active use, music and drugs had acted as a form of escapism. Through MT, he learned that he could create new associations to problematic lyrics by focusing on their connection to positive recovery. Mr. R expanded his emotional horizons, using his PM as a tool for emotional regulation. By disentangling it from its past association with drug use, he was able to set aside the latter and engage with the music on its own terms, allowing it to support and shape his emotional experience in a healthier and more intentional manner: My music used to be a form of escapism with earphones in my ears and a joint in my hand. In the group [MT], I became aware that the same music could also act as a force towards recovery, a therapeutic tool. The lyrics that I used to listen to while I was using are the same as those in recovery, but my existence as a person has changed, where I relate differently to the meaning and context of the songs. My emotional spectrum has expanded, allowing me to feel positive emotions such as joy and pleasure without drugs.
As illustrated in the prior subtheme, participants’ engagement with alternative genres provided the foundation for reintroducing their PM in a safe context. As they progressed in their recovery, within group MT, they learned to create new associations, allowing them to experience their PM differently. Although PM could still evoke cravings, their recovery-oriented identity enabled them to tolerate it, transforming it into a source of joy, emotional engagement, and a positive element of their recovery.
During Sustained Recovery: Maintaining Tolerance
Although participants had already established new and positive connections to PM, currently, participants also employ their PM as positive reminders and warning signs to maintain their rehabilitation. Through group MT, participants re-engaged with their PM in a way that supported their recovery, transforming it into a tool for reflection and emotional regulation. They expanded their use of music more broadly, drawing on the full spectrum of genres to manage their musical triggers, experiencing it with confidence rather than avoidance or uncertainty. Ms. Q, who has been in sustained recovery for 3 years, still listens and enjoys her PM, rave music. She is able to find great joy in listening to it, and no longer worries about triggers. Yet, listening to her PM also acts as a reminder of everything she went through during active abuse – a constant warning to stay on the straight path: Today, listening to rave music is amazing because I don’t need external substances to enjoy it. Hearing tracks while driving is like flying on the road. I’m clean. Clean. Clean. So, I have these fun moments, but there are also a lot of crappy ones. They remind me of how much it is not worth going back. Drugs are an illusion. You feel good for an hour or two but then you are sucked into a black hole where you simply want to die. I make sure not to forget those awful times. That way, I will never want to go back, and I will be able to continue enjoying my music without drugs.
For Ms. Q, her PM has become an additional resource in her recovery, serving a dual role: both educator and emotional facilitator. She hasn’t merely neutralized its power as a trigger – she has altered it into a resource that actively supports and sustains her sustained recovery.
For the past 4 years in sustained recovery, Mr. L has found new joy and appreciation in his PM, rave music. Through music analysis exercises at MT sessions, he opened-up emotionally and related to his PM on a personal level. This enabled him to separate the joy of listening from its connection to substance use. Currently, Mr. L utilizes his music as what may be termed a “recovery sign,” reminding him of the rehabilitation process and helping him stay on the right path of recovery. It stands as a signpost, a clear marker that he has reached a meaningful milestone in his recovery journey. A goal he once set for himself, now realized, reinforces his sense of progress and solidifies his place within sustained recovery. Within his social life, he has taken meaningful steps toward healing, most notably by making peace with his ex-wife. This reconciliation has also opened the door to a more consistent and fulfilling relationship with his son. By confronting and working through the fears that initially held him back, he has claimed a sense of stability and presence in his family life, reflecting his commitment to recovery and personal growth. Mr. L’s PM is thus a sign of growth, strengthening his confidence and reaffirms his ability to keep moving forward. For Mr. L, rave music now represents the joy of existence, entirely detached from dependence on substances: Listening to rave music and composing remind me of both happy and sad times in my journey to recovery. It is a beautiful thing that I have these additional tools to help me in recovery. Today I can just sit, listen to a good rave song, and enjoy myself and my life without using or wishing to use drugs.
Discussion
The goal of the present research was to explore the retrospective and current outlook of individuals in sustained recovery from SUD, examining their approach toward their musical triggers from the onset of rehabilitation until current state of sustained recovery. The alternative group consisted of participants who, at the time of the study, still abstained from PM and exclusively listened to music genres they had specifically chosen as an alternative; the ambivalent group consisted of participants who had developed mixed feelings toward PM; and the tolerant group consisted of participants who had developed resilience to PM through group MT. Each group went through a different process in developing mechanisms to cope with PM.
The Alternative Group
In the first phase, the alternative group achieved self-recognition of PM risks. The coping mechanism used was total abstinence from PM in order to avoid cues and safeguard rehabilitation. Studies show that recognizing the source of drug cues is vital for successful rehabilitation, as awareness plays a significant role in the likelihood or unlikelihood of relapse (Beaulieu et al., 2024; Stewart et al., 2019; Suzuki & Kober, 2018). More specifically, an analysis of interviews with released prisoners suffering from SUD illustrated that participants who became aware of their musical triggers, stopped listening to their PM as a coping strategy, to avoid cravings (Bensimon, 2024).
In the second phase, the alternative group listened to alternative genres, filling the void left by avoiding PM. They purposefully selected new musical genres that could strengthen their motivation to maintain recovery and intensify emotions they wished to express. This aligns with DeNora’s (2000) findings on how music can temper, interpret, and enrich emotions in daily life, demonstrating how individuals use music to meet their emotional needs by choosing specific songs and genres. By actively selecting music, participants became their own DJs. By choosing alternative genres, participants exercised agency over their emotional environment, demonstrating a self-regulated approach to recovery. Past studies (Greasley & Lamont, 2011; Sloboda & O’Neill, 2001) support DeNora’s research, showing that people are generally aware of music’s influence on their mood and behavior, using it to regulate their emotions and actions. Recent research further supports this perspective. Kahn et al. (2025), employing a mixed-methods approach, found that college students reported music to serve as a tool for distraction, empowerment, the cultivation of shared experiences, the evocation of memories, and as a means of emotional facilitation and regulation. These findings align with DeNora’s central thesis where individuals are consciously aware of music’s impact on their emotional and social lives and employ it intentionally. Accordingly, participants functioned as their own music therapists, curating playlists that supported their recovery. This approach to music, as a self-guided tool, highlights how individuals can actively engage with music to foster their self-resilience and manage their recovery journey.
In the third phase, at the time of the study, participants remained susceptible to their PM, exclusively listening to their alternative genres while avoiding their PM. Although participants had already been in sustained recovery for a significant amount of time, PM still constituted a trigger that should be avoided to maintain recovery. Findings have illustrated that people in sustained recovery from SUD safeguard their recovery by taking a proactive stance against their triggers, typically exemplified via physical distance (Pettersen et al., 2023). Yet, despite the elapsed time since the end of rehabilitation, tolerance to PM had not been achieved.
The strategies employed by participants in the alternative group can be meaningfully interpreted through the lens of the Risk-Need-Responsivity (RNR) model, a widely recognized framework for the assessment and treatment of offenders. The RNR model comprises three core principles: (1) the Risk principle, which emphasizes aligning the intensity of intervention with the individual’s risk of reoffending; (2) the Need principle, which focuses on identifying and targeting criminogenic needs within treatment; (3) the Responsivity principle, which calls for tailoring interventions to the individual’s abilities, learning styles, and motivation (Bonta & Andrews, 2023). Within this framework, the actions of the alternative group can be seen as following a phased application of the RNR principles. In the first phase, by deliberately avoiding their PM, participants engaged with the Risk principle: minimizing exposure to a recognized trigger and thus reducing the likelihood of cravings and relapse. In the second phase, their shift toward alternative music genres reflects the Need principle: while acknowledging their psychological and emotional need for music, they consciously redirected that need toward safer and non-triggering musical alternatives. In the third phase, participants exhibited the Responsivity principle by adapting their behavior to their current capacity and readiness: lacking the tools to manage the emotional impact of PM, they chose to exclude it entirely. Nonetheless, this avoidance underscores a continued vulnerability, suggesting that while the strategy reduced immediate risk, the underlying triggers remained unaddressed.
The Ambivalent Group
The first phase of the ambivalent group was similar to that of the first phase of the alternative group, characterized by participants being told about the risks of their PM and avoiding it. However, unlike the alternative group members, once the ambivalent group members started feeling comfortable within their sustained recovery, they returned to their PM, yet lacked the appropriate tools to cope with musical triggers. As a result, participants developed an ambivalent relationship with their PM, which remained a possible risk factor to abuse. This finding is supported by a study showing that self-administered music rehabilitation without proper education or training, can result in involuntary cravings when listening to PM, despite the best intentions to the contrary (Silverman et al., 2020). Unlike unstructured listening, which may reinforce maladaptive behaviors or emotional states, research suggests that structured music therapy provides a more sustainable and clinically supported pathway for recovery, reducing cravings (Megranahan & Lynskey, 2018; Silverman, 2021).
A few structured interventions are designed to neutralize potential triggers and cultivate healthier coping mechanisms. In the Music Therapy Anger Management, musical situations are constructed collaboratively with clients to enable them to practice new skills in a positive environment. Music is employed as a positive reinforcer during challenging tasks, facilitating the development of adaptive coping strategies through improvisational exercises (Compton-Dickinson & Hakvoort, 2017; Marshall & Serran, 2004; Ross et al., 2008). Similarly, Group Cognitive Analytic Music Therapy, which can be implemented in both group and individual settings, reduces risk by promoting mindfulness and emotional self-reflection through active music creation (Compton Dickinson, 2006; Compton-Dickinson & Hakvoort, 2017). By integrating music within a structured therapeutic framework, these approaches support not just momentary relief, but long-term recovery, emotional regulation, and reintegration into society. Therefore, unless rehabilitation centers incorporate MT group programs specifically designed to address the unique needs of individuals with SUD, equipping clients with tools to neutralize their musical triggers (Horesh, 2010), such triggers will continue to pose challenges, including ambivalence, to sustained recovery.
The Tolerant Group
Participants in the tolerant group received group focused MT during rehabilitation and were able to develop tolerance to PM. In the first phase, participants recognized the risks of their PM while attending group MT. In the second phase, participants avoided PM and were encouraged to listen to alternative genres. It has been proposed that listening to alternative music within the framework of MT can serve as a temporary replacement until clients are able to develop enough confidence to address cues evoked by their PM (White, 1996). In the third phase of rehabilitation, participants developed new and significant connections with PM through MT, eventually reintegrating it back into their lives, not as a trigger, but as music to enjoy in the last phase.
The study found that participants recognized the important role of MT in neutralizing musical triggers. MT’s lasting impact on PM is significant, as it transforms PM from a potential relapse trigger into a tool for evoking positive emotions or serving as a reminder to avoid past behaviors. Research highlights the overarching benefits of MT for individuals with SUD, showing it can help reintegrate musical triggers and enable clients to express their emotions constructively, verbally and nonverbally, without relying on substances (Baker et al., 2007; Lin et al., 2011; Shuman et al., 2016). MT for SUD clients provides various methods to address their musical triggers (for a review see Aldridge & Fachner, 2010), helping them enjoy their PM beyond rehabilitation (Gardstrom et al., 2013; Silverman, 2021). Techniques like listening (Bensimon, 2024), playing, (Ghetti et al., 2022), singing (Silverman, 2016), and composing (Silverman, 2021) are used, along with guided discussions to explore the underlying sources of triggers (Dijkstra & Hakvoort, 2004; Horesh, 2010). MT fosters a safe and supportive environment for reintroducing PM, aligned with qualitative research showing that clients felt more secure and confident in engaging with PM during sustained recovery (van de Ree, 2016). As a result, MT plays a crucial role in promoting emotional regulation, enhancing positive mood and reducing negative emotions. This has been demonstrated in studies that examined the effectiveness of MT in both inpatient settings (Albornoz, 2011; Huang & Chen, 2021; Hwang & Oh, 2013) and outpatient programs for individuals with SUD or substance abuse treatment (Oklan & Henderson, 2014; Yun & Gallant, 2010). Although the MT groups were conducted in Israel, research has illustrated the prevalence of MT on a global scale, indicating its capacity to transcend cultural barriers (Carter & Panisch, 2021; Hohmann et al., 2017). Nonetheless, MT in Israel has been shown to be a success and instrumental in the therapeutic process across a range of clients with a history of drug abuse (Bensimon, 2024; Bensimon & Gilboa, 2010; Lozon & Bensimon, 2025).
An additional factor to consider is the relationship between the music therapist and the client, which can assist in sustained recovery from SUD. As illustrated in the findings, participants benefited from a therapist who accommodated their musical and personal needs, fostering trust and emotional connection. Research shows that clients often recognize the significance of this relationship, noting that it provides stability, encouragement, and a sense of being heard (Lindvig et al., 2022; Topor & Denhov, 2015). Through key relational components – hopefulness, concern, commitment, honesty, positive regard, and engagement – therapists help clients develop trust, which is essential for the treatment (Brekke et al., 2018; Skånland & Trondalen, 2024).
Furthermore, in group-focused MT for SUD, shared musical experiences facilitate mutual recognition and emotional regulation, helping clients engage in treatment without the pressure of verbal expression (Wilhelmsen & Fuhr, 2018). Techniques such as lyric analysis, songwriting, and improvisation allow clients to process emotions and strengthen coping mechanisms in a supportive therapeutic environment (Solli & Rolvsjord, 2015). This is particularly beneficial for individuals who struggle with social interactions, as the therapeutic relationship nurtures confidence and trust, both in themselves and in others, which are crucial for reintegration into society and maintaining recovery (Ansdell, 2015).
To better understand how the tolerant group used PM as a tool for rehabilitation and sustained recovery, the Good Lives Model (GLM) is proposed as a theoretical rehabilitation framework. This is a strengths-based rehabilitation model, whose purpose is to first identify aspirations, fundamental values, and strengths of individuals within the criminal justice system, and then develop the knowledge, skills, opportunities and resources to reduce the risk of recidivism. This rehabilitation model assists individuals in meeting their needs, pursuing their interests, and eventually living meaningful and productive lives (Ward & Brown, 2004). In the current study, the tolerant group used both PM and alternative music to achieve the following GLM goals:
Life – utilizing music as one of the means for achieving sustained recovery and living a healthy and productive life.
Knowledge – the process of first being made aware of the dangers of PM and only then listening to it, made participants understand that they could turn PM into a cue for maintaining recovery.
Excellence in agency – participants became masters of their own choices by selecting songs and musical genres based on how they felt or how they wanted to feel.
Inner peace – during rehabilitation, participants learned to neutralize musical triggers. They reshaped their PM through new experiences and events that focused on recovery, thus finding moments of peace and comfort in their PM.
Pleasure – after the inherent dangers of PM had been neutralized, PM turned into a means of feeling content and deriving pleasure from current surroundings and experiences.
Creativity – instead of being limited to specific genres and experiences due to past drug use, participants could now explore curated songs and genres that evoked moments and emotions from the entire spectrum of their life.
By reintroducing PM during rehabilitation, the tolerant group achieved GLM goals with new and old genres. They learned how to cope with musical triggers in a safe environment and how to transform those triggers into positive constructs that strengthen sustained recovery. Participants neither abstained from PM nor developed ambivalence toward it. They successfully navigated their musical stressors while fostering a balanced and positive connection with their PM.
Limitations and Future Studies
The present study has several limitations. First, the groups were unbalanced in the number of participants. Future studies will greatly benefit from having an equal number of participants per group to yield more significant insights. This is particularly important, as the current study could not determine if participants in the tolerant group, who received MT, were already more inclined toward treatment and, consequently, more likely to benefit from it, compared to the other groups. Second, the ambivalent and tolerant groups consisted of only five and six participants respectively, numbers that may pose a problem for reaching saturation. This situation occurred because groups were identified through content analysis and were not chosen in advance, during research planning. Future studies should recruit a larger number of participants per group. Third, the number of male participants was significantly larger than the number of female participants. Research has shown that gender differences exist regarding recovery issues (Gueta & Chen, 2019) and music processing during rehabilitation (Gardstrom & Hiller, 2016). Future studies should strive to include a more diverse population, examining possible gender differences that may affect the role of music in their lives. Fourth, future studies should examine the impact of MT on long-term recovery when given to participants from ambivalent and alternative groups during their sustained recovery. Fifth, the study did not consider the participants’ cultural backgrounds, nor other key factors involved in recovery, such as mental health, social well-being, economic independence, and self-esteem (Fardone et al., 2023; Kim & Elefant, 2016; Zhang & Wu, 2025), all of which may have influenced their perspectives and experiences. Future research could benefit from considering these aspects and their potential impact on the findings. Additionally, data on co-morbidity was not collected, as it fell outside the purview of the present study. However, this remains a compelling avenue for future research. Considering the added complexity that co-morbid conditions may introduce (Ghetti et al., 2022; Silverman et al., 2023), it is plausible that such factors could significantly influence individuals’ relationships with their music, potentially altering how music is experienced, utilized, or avoided in the context of substance use and recovery. Finally, while MT can integrate a broader multidisciplinary treatment framework (Aletraris et al., 2014), this study did not account for the specific treatment model each participant received. Future research should aim to conduct a mixed methodology combining qualitative insights with measurable and documented outcomes, fully detailing specific MT approaches, models and protocols, including dance and movement, allowing for a more exact understanding of the role MT in contributing to positive change and sustained recovery. These steps could provide the foundation for subsequent studies and randomized controlled trials, with procedural matched demographic groups across conditions, establishing a framework for the development of complex rehabilitative interventions for people with SUD.
Conclusions
The findings revealed three groups of participants, each with a unique approach to managing PM during rehabilitation and sustained recovery. The alternative group replaced PM with other music genres to avoid triggers for relapse. They abstained from all music during rehabilitation, later embracing and integrating alternative genres into their lives. However, PM remained a trigger for negative emotions and potential relapse even during sustained recovery. The ambivalent group had conflicting feelings about PM. Although they initially avoided their PM during rehabilitation due to fear of relapse, afterward they returned to PM as they felt more confident in their recovery. However, without the proper skills to manage musical triggers, PM continued to provoke cravings and relapse risk. Of the three groups, the tolerant group developed resilience to PM. In rehabilitation, they initially abstained from PM, exploring alternative music genres instead. Over time, within group-focused MT sessions, PM was reintroduced in a supportive environment, allowing participants to neutralize their triggers by forming positive new associations. This process equipped them with the skills to manage PM effectively, transforming it from a drug-use reminder into a positive part of their recovery journey.
Footnotes
Acknowledgements
We are grateful to each one of the research participants for their willingness to share with us personal aspects of their lives. This article is part of the lead author’s dissertation to be submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Criminology department of Bar-Ilan University, Ramat-Gan, Israel.
Ethical Considerations
All study procedures were approved by the university Institutional Review Board.
Consent to Participate
Participants completed written informed consent forms explaining the nature of the study, the potential risks and benefits of their participation, and that they would withdraw their participation at any time without penalty.
Consent for Publication
Participants gave their consent for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this qualitative study include interview transcripts and are not publicly available because of participant identifying information included in the transcripts. Upon request, the corresponding author can provide blinded interview transcript excerpts that are not already included in the manuscript Results section.