
Abstract
Introduction
The objectives of this study are to determine (1) the ability of the Montreal Cognitive Assessment to predict on-road driving performance in drivers with a neurological condition and elderly drivers with suspected cognitive decline, and (2) the association between the performance on the Useful Field of View and the performance on the Montreal Cognitive Assessment.
Method
This study used a retrospective design. Clients were included who had completed the Montreal Cognitive Assessment and the on-road driving evaluation from November 2006 to May 2009 (n = 154) in a driving rehabilitation program in the Montreal Area. Total scores on the Montreal Cognitive Assessment, Useful Field of View risk categories, pass or fail outcomes from an on-road evaluation, as well as demographic and clinical characteristics were recorded from participants’ medical charts.
Results
The Montreal Cognitive Assessment was found to have a sensitivity of 84.5% and a specificity of 50% with a cut-off of ≤25. It was significantly associated with the Useful Field of View risk category.
Conclusion
The Montreal Cognitive Assessment could be a valuable screening tool. However, its predictive validity is not strong enough to recommend its use as the sole instrument for identifying unfit drivers.
Introduction
Driving is a complex activity requiring the integration of physical, perceptual, and cognitive skills (Mazer et al., 2004). It constitutes a major factor toward community reintegration for individuals following a neurological event (Marshall et al., 2007), and is an important life skill for seniors with mild age-related impairments to maintain their functional autonomy (Man-Son-Hing et al., 2007). Among the possible deficits observed within each of the clienteles, cognitive impairments are deemed to have a significant impact on driving ability (Man-Son-Hing et al., 2007).
Several cognitive screening tests have been evaluated to determine their ability to discriminate safe from unsafe drivers. Although there is no consensus to date regarding which test best identifies at-risk drivers, some screening tools have been shown to be predictive of on-road performance. One cognitive screen, which is being increasingly used by occupational therapists, is the Montreal Cognitive Assessment (MoCA). A recent survey of assessment practices to evaluate medically at-risk drivers across Canada revealed that the MOCA was among the most used tests by occupational therapists as part of their off-road assessment (Vrkljan et al., 2013). Despite its growing use in clinical practice, the MoCA has not yet been investigated as a screening tool for identifying at-risk drivers (Vrkljan et al., 2011).
The primary objective of this study was to determine the ability of the MoCA to predict on-road driving performance. As the Useful Field of View (UFOV) test has demonstrated a predictive ability to detect at-risk drivers (Duchek et al., 1998; Goode et al., 1998), the secondary objective was to determine the association between the UFOV risk category outcomes with the MoCA score.
The study’s primary hypothesis was that the MoCA score might be an important predictor of on-road performance of drivers with possible cognitive deficits. It was also hypothesized that the UFOV performance would be significantly associated with the MoCA score.
Literature review
Screening for at-risk drivers is an area that is a major source of concern for individuals, families, professionals, institutions, and society. As a result, occupational therapists are increasingly being asked to screen for fitness to drive. Through quick examination of driving specific skills, screening aims to distinguish those who require further evaluation from those who are most likely safe drivers (Korner-Bitensky et al., 2005). It is recommended that occupational therapists use a multifactorial-based assessment approach including physical, cognitive, and visual-perceptual components (Vrkljan et al., 2011). The cognitive component typically represents a crucial part of the assessment when conducted with drivers with a neurological condition or elderly drivers with suspected cognitive decline.
Recent literature reviews have investigated the ability of a variety of cognitive tests available for use in clinical practice to predict on-road performance with specific populations (Unsworth et al., 2005; Vrkljan et al., 2011). Unsworth and collaborators (2005) reviewed 20 assessments commonly found in the driving literature. The cognitive assessments that obtained the highest ranking and were recommended for inclusion to screen clients in the clinic included the Mini Mental State Examination (MMSE), the Rey-Osterrieth Complex Figure test, and the Trail Making test (TMT) A and B. More recently, Vrkljan and colleagues (2011) critically reviewed various off-road cognitive assessments with regards to their psychometric properties and predictive ability for fitness to drive. The MMSE, TMT A and B, clock-drawing test (CDT), Motor-Free Visual Perception Test (MVPT), and UFOV were found to have adequate to excellent psychometric properties, while the Traffic Recognition Test, Money Road Map Test, Bell’s test, and Single-letter cancellation were weaker. The UFOV was the only cognitive test reviewed which has demonstrated excellent predictive ability for crash history, future crashes, or performance on the road test. This test, which requires the use of a computer, is, however, recommended for more comprehensive driving assessment rather than for screening purposes. The TMT A and B, the CDT, and the MVPT were rated as adequate, as there is some evidence supporting their predictive ability. The MMSE was found to lack the necessary evidence to predict on-road performance. The authors indicated that there is no evidence available regarding the predictive ability of the MoCA for screening at-risk drivers, although therapists identified using it for that purpose.
The increasing interest from occupational therapists in using the MoCA for screening purposes is, in part, because it provides a global cognitive screen compared with other tools that are rather specific. In addition, the MoCA has demonstrated excellent sensitivity (90%) and specificity (87%) in identifying those with Mild Cognitive Impairment (MCI), unlike the MMSE (Nasreddine et al., 2005). Its use has been investigated in populations other than MCI, including Parkinson’s disease (Gill et al., 2008), dementia (Nasreddine et al., 2005; Smith et al., 2007), patients with brain metastases (Olson et al., 2008), and cerebrovascular disease (Popovic et al., 2007). The time to administer this test is short and thus comparable with the MMSE (10–15 minutes). In addition, the MoCA is standardized and accessible in several languages via the Internet. Finally, the MoCA includes an abbreviated TMT B and a clock drawing subtest. Both of these tests in their complete version have been shown to be associated with poor driving performance (Freund et al., 2005; Mazer et al., 1998; Ott et al., 2008; Vrkljan et al., 2011).
However, as suggested by Vrkljan and colleagues (2011), there is a need to investigate this tool further before supporting its use for driver screening.
Methods
Participants
This study used a historical cohort. We reviewed the charts of drivers who were evaluated in an outpatient driving evaluation program at a rehabilitation center in Montreal between November 2006 and May 2009. Participants were included if they had completed the MoCA and the on-road evaluation. To be admitted into the program, the participants had to meet the medical eligibility requirements for driving established by the provincial licensing body (Société de l’Assurance Automobile du Québec), be referred with a medical diagnosis, and have a neurological and/or musculoskeletal condition resulting in significant deficits.
The research ethics board of the Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal approved the protocol.
Measures
Demographic and clinical variables including age, sex, diagnosis, total years of education, presence of driving-related physical disability, and use of adaptive aids during the on-road test were recorded. Information on driving history (years of experience, class of permit, and typical driving habits) was also obtained from the participants’ medical charts.
Cognitive tests
The cognitive tests were administered by the occupational therapist as part of the off-road assessment prior to the on-road test.
The MoCA screens higher mental functions including visuospatial and executive functions, denomination, memory, attention, mental flexibility, abstraction, language, and orientation. It incorporates an abbreviated form of TMT B and the CDT, both of which have been shown to be valid tests in their original form with respect to driving screening (Freund et al., 2008). The MoCA yields a score of 30, with a cut-off of 26/30 indicating possible mild cognitive impairment (Nasreddine et al., 2005). One point is added to the score for those with an education level below 12 years (Nasreddine et al., 2005). The MoCA was found to have high test–retest reliability (r = 0.92, p > 0.001) and good internal consistency (Cronbach’s alpha 0.83). Validity was established through correlation with MMSE (Nasreddine et al., 2005).
The UFOV touch and mouse PC version is a computerized test composed of three subtests including processing speed, divided attention, and selective attention (Langford, 2008). Each subtest yields a numerical score and the overall performance on the test is classified into risk categories with respect to driving ranging from 1 (very low risk for crash) to 5 (very high risk). Those with a score of 3 or higher are considered at increased risk of crash (Ball and Owsley, 1992; Rubin et al., 2007). It has been shown to have high test–retest reliability (r = 0.884 for mouse and 0.735 for touch screen) and validity (Edward et al., 2005), as well as excellent predictive validity with crash history (Norvack et al., 2006), future crashes (Owsley, 1994), and performance on road test (Myers et al., 2000; Norvack et al., 2006; Stav et al., 2008)
On-road test
Although on-road evaluations are inherently diverse in their administration given varying traffic and weather conditions, a recent survey of driver rehabilitation specialists identifies the behind-the-wheel component of the assessment protocol as ‘by far the primary factor in making a decision regarding fitness-to-drive’ (Dickerson, 2013). In this study, the determination of driving performance was based on the client’s outcome in the behind-the-wheel assessment. This assessment meets the requirements indicated in the literature to have a valid and reliable on-road test (that is, standardized route with pre-determined observation, scoring criteria, range of traffic conditions, self-directed section, trained assessors) (Di Stefano and Macdonald, 2003; Justiss et al., 2006; Mallon and Wood, 2004).
The on-road test takes approximately 55 minutes and follows a standardized route. It is performed in the presence of an occupational therapist specializing in driving rehabilitation (the same occupational therapist who administered the off-road test) and a driving instructor experienced in evaluating drivers with medical conditions. The driving circuit progresses gradually from residential areas to busy urban boulevards. It also includes two highway segments and a non-directed portion where the client must find his own way to return to a specified location. All assessments were carried out in the same test vehicle, equipped with a dual brake on the passenger side and basic adaptive driving equipment (that is, left foot accelerator, hand-controls, and steering devices) utilized as needed. When pertinent, clients are introduced to adaptive driving equipment to compensate for a functional limitation (that is, a stroke survivor with right side hemiparesis who can no longer activate the vehicle pedals with his right foot). In these cases, driver training is provided prior to performing the on-road evaluation. The hours of driver training vary according to each client’s learning ability, but the on-road evaluation is only undertaken once the driver has integrated the new adaptive driving devices to his driving habits. During the on-road evaluation, the driving instructor sits in the front of the vehicle and is responsible for guiding the client through the standard route and ensuring the safety of participants during the assessment. The occupational therapist sits in the rear of the vehicle and fills out a grid to record driving performance and driving behavior. Each lane change to the right or left is recorded, including whether it was properly performed with advance signaling and adequate visual verification or blind-spot checks. The numbers of intersections properly or improperly managed are also noted, as are the number of merges properly/improperly performed and specific vehicle speeds in distinct zones (that is, school versus city versus highway). Observations of the client’s performance in unpredictable situations (that is, parked delivery trucks blocking a lane, cyclists not obeying traffic rules, detours because of construction, etc.) are also detailed to gather information regarding the client’s ability to anticipate, plan, initiate, and problem solve. The recording of these behaviors helps to quantify the road test and provides the evaluators with objective data on which to base the result of the on-road test.
Once the driving evaluation is completed, the occupational therapist and driving instructor discuss the driver’s strengths and weaknesses to determine the recommendation on the outcome of the on-road test. The recommendation is one of three possibilities: (1) safe to drive (pass), (2) unsafe to drive (fail), or (3) unsafe to drive at the moment but the client shows potential for pursuing with driver training (fail with potential). Driver training is considered an appropriate recommendation for clients demonstrating good insight into their limitations and a good learning potential (that is sufficient memory abilities to recall and implement strategies suggested by the driving instructor). The validity of using global ratings as an outcome measure for assessing on-road performance has been demonstrated (Justiss et al., 2006) The joint decision-making process (occupational therapist and driving instructor) regarding the outcome of the on-road test helps to decrease subjectivity in the final recommendations to the client.
Procedure
The medical charts of participants satisfying the inclusion criteria were reviewed. The results of the MoCA, the road test outcome, as well as information regarding driving history, demographics, and clinical characteristics were recorded. The scores of those who had completed the UFOV were also documented. Data were retrieved from the occupational therapist’s report for the driving legislation authority.
Data analysis
Descriptive statistics, as well as chi-square and one-way analysis of variance (ANOVA), were carried out to highlight main demographic, clinical and driving characteristics, MoCA, and UFOV scores by the categories of the on-road test (pass, fail with potential, or fail).
The Receiver Operating Characteristic (ROC) curve was used to examine the discriminative power of the MoCA score in predicting on-road performance as well as to find the best cut-offs for the MoCA score in identifying the drivers who failed the on-road test. For this analysis, the outcome of the on-road test was dichotomized to pass and fail. Drivers who failed included both those whose outcome is unsafe to drive (definite fail) and those whose outcome is unsafe to drive for the moment but had shown potential for pursuing with driver training (fail with potential). According to Streiner and Norman (2008), the discriminative power of a tool is considered to be low if the area is between 0.5 and 0.7; moderate between 0.7 and 0.9; and high when it is above 0.9. Sets of best cut-offs for the MoCA score were determined based on the most optimal combination of sensitivity and specificity. Additionally, positive and negative predictive values were examined. Each of these analyses provides different information regarding the ability of the MoCA to identify a pass/fail on the road test. Sensitivity is the probability that the MoCA identifies a person as failing in the road test when they do fail the on-road evaluation, whereas the specificity is the probability that the MoCA identifies a person as passing the on-road test when they do succeed during the on-road evaluation. As it is most important to identify individuals who will fail an on-road evaluation, priority was given to obtaining high sensitivity. All participants who had completed the MoCA and the on-road test were included in this analysis.
To further investigate the association of the MoCA score with the probability of failing the on-road test, a multivariable ordinal logistic regression analysis was carried out, adjusting for age and overall driving-related physical disability. For the multivariable ordinal logistic regression analysis, the on-road performance was analyzed with three levels (pass, definite fail, and fail with potential). The overall physical ability rating of normal/sufficient for driving or insufficient for driving was developed by combining the ratings (normal, sufficient for driving, and insufficient for driving) from the occupational therapist’s report on the mobility of the neck, the trunk, the right and left upper limbs, and the right and left lower limbs.
To explore the relationship between the MoCA score and the UFOV risk categories, a multivariable ordinal logistic regression was carried out, adjusting for age and overall driving-related physical disability. As the UFOV was not administered for some participants (39 persons did not complete the UFOV), the analysis was done with the sample of participants who completed the MoCA, the UFOV, and the on-road test. The characteristics of the 39 subjects for whom UFOV data were missing were further examined. An independent t-test and chi-square analysis were performed to compare the two groups (UFOV score missing versus available) with regard to age, sex, diagnosis, overall physical ability, on-road performance outcome, and MoCA total score.
All data analyses were performed using the statistical analysis system SAS 9.3.
Results
A total of 336 individuals were referred to the driving department for an evaluation between November 2006 and June 2009. Of these, 154 individuals were assessed using both the MoCA and the on-road test. Among these, 115 completed all three subtests of the UFOV. A total of 182 individuals were not included in this study, because they were not tested with the MoCA (n = 168), had incomplete MoCA because of aphasia (n = 5), were not tested on-road (n = 5), or the medical chart was not found (n = 4).
The average age of the participants was 68.8 ± 16.6 years (range 18.6–92). The group was composed mostly of males (79.2%). The most frequent diagnosis was neurovascular disease (50%) followed by neurological diseases (31.8%). Most of the participants had normal or sufficient physical abilities to drive (85.1%) The average number of years of driving experience was 44.2 ± 16.5 years (range 0–77). Most participants drove with an automatic transmission (94.7%) and did not use adaptive equipment in their vehicle prior to the driving evaluation (93.3%). The average time between the MoCA and the on-road test was about 10 ± 15.2 days in both the passing and the failing groups.
Sociodemographic and clinical characteristics of participants (n=154).
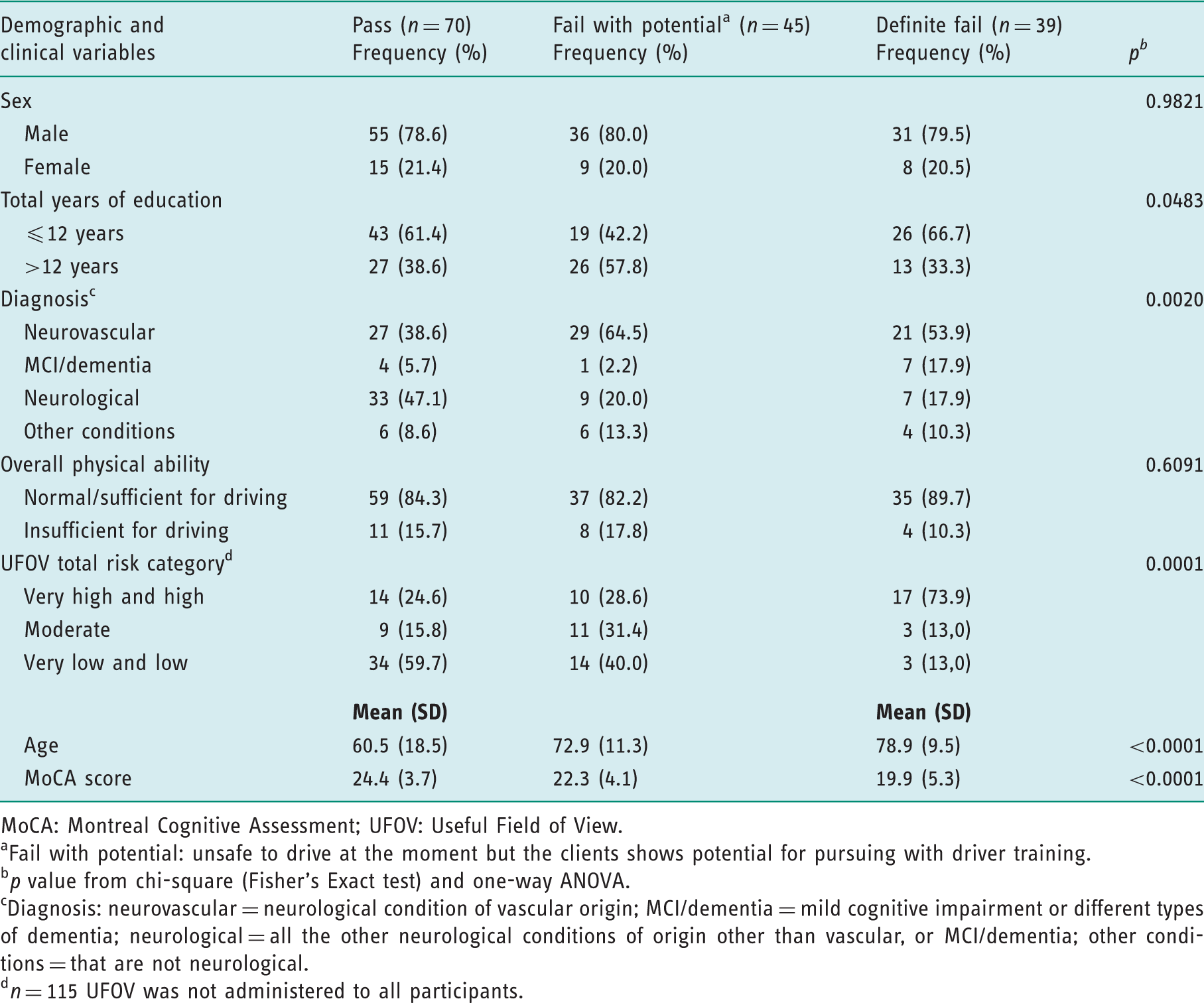
MoCA: Montreal Cognitive Assessment; UFOV: Useful Field of View.
Fail with potential: unsafe to drive at the moment but the clients shows potential for pursuing with driver training.
p value from chi-square (Fisher’s Exact test) and one-way ANOVA.
Diagnosis: neurovascular = neurological condition of vascular origin; MCI/dementia = mild cognitive impairment or different types of dementia; neurological = all the other neurological conditions of origin other than vascular, or MCI/dementia; other conditions = that are not neurological.
n = 115 UFOV was not administered to all participants.
Predictive validity of the MoCA test
Sensitivity, specificity, and predictive values according to MoCA cut-off values.
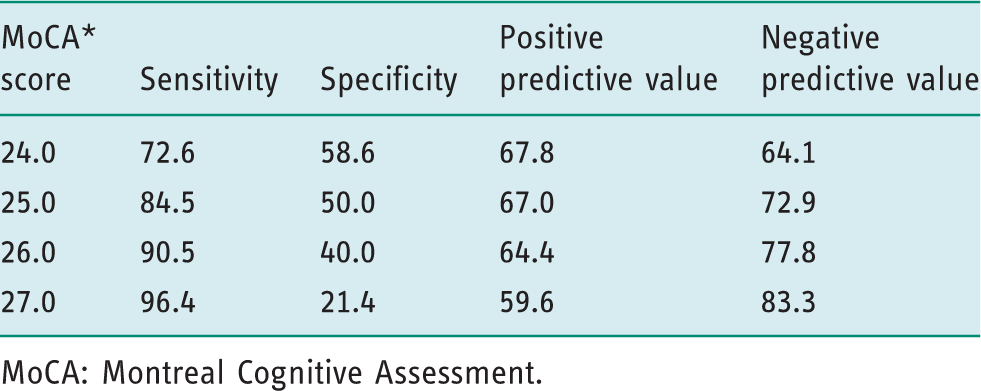
MoCA: Montreal Cognitive Assessment.
Multivariable ordinal logistic regression modeling the probability of failing on the road test (n = 154).
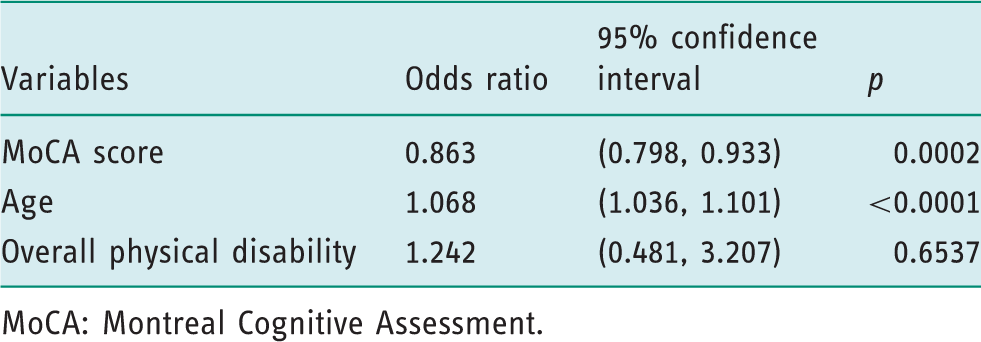
MoCA: Montreal Cognitive Assessment.
Association between UFOV performance and MoCA scores
Multivariable ordinal logistic regression modeling the probability of being at high risk on the UFOV test (n = 115).
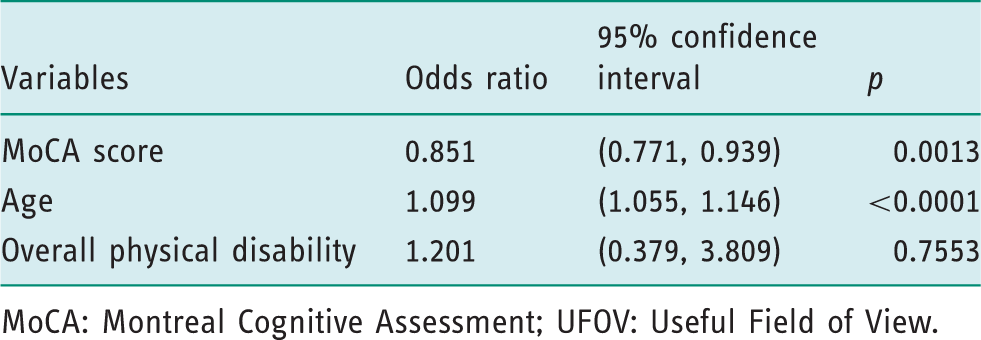
MoCA: Montreal Cognitive Assessment; UFOV: Useful Field of View.
The comparison of subjects with UFOV missing and non-missing data highlighted statistically significant MoCA total score and on-road performance test differences. The analyses revealed that subjects who had missing data on UFOV had lower average MoCA total scores compared with those who completed the UFOV, 20.4 versus 23.1 (p = 0.0017). Furthermore, the relationship between UFOV missing groups and the on-road performance test was statistically significant at p = 0.0302, with about 41% of subjects with missing UFOV compared with 20% of subjects who completed the UFOV more likely to fail on the on-road performance test. No other significant differences were found for the remaining demographic and clinical characteristics.
Discussion and implication
The main objective of this study was to determine the value of the MoCA in predicting driving performance in clients with a medical condition. In addition, the relationship between the MoCA score was compared with the UFOV results.
The MoCA was found to have an optimal predictive ability with a sensitivity of 84.5% and a specificity of 50% when a cut-off of ≤25 was used. This cut-off was chosen over the 26 point cut-off as it represents the most optimal combination of sensitivity and specificity. The chosen cut-off score of ≤25 in predicting failing the on-road test is very close to the MoCA original cut-off score of 26 with respect to screening for mild cognitive impairment (Nasreddine et al., 2005). This cut-off score for predicting on-road performance is not surprising as driving is a high-level task, which relies on well-preserved higher cognitive skills. In selecting this cut-off, higher sensitivity was favored over specificity. Because the objective of the screening tool in this context is to identify those that should be further tested, it is imperative that all those who are not safe to drive be identified with a higher sensitivity. However, the lower specificity of 50% implies that a significant proportion of truly safe drivers will also be targeted for further testing by requiring an on-road test, thus undergoing an unnecessary evaluation procedure.
The moderate discriminative ability for predicting on-road performance of the MoCA found in this study might be explained by the complexity of the driving task and the fact that the MoCA does not cover all of the skills that are required for driving. Thus, clinicians should not base their decision-making solely on the MoCA, but use it in combination with other assessments during the screening procedure.
The findings revealed a significant association between the MoCA score and the risk categories on the UFOV. The UFOV is a test that has been widely adopted in clinical practice by occupational therapists based on the evidence supporting its use. Research conducted with the UFOV has indicated an association between poor performance on the test and greater risk of vehicle accidents (Owsley et al., 1998). However, the UFOV test is not as practical for screening as the MoCA and it has been recommended for use in the comprehensive driving assessment (Vrkljan et al., 2011). Considering the results obtained in this study, it would be interesting to explore further the association between these two measures in relation to the on-road performance to determine whether both are necessary for inclusion in a screening battery.
Another interesting observation was the significant difference in the mean MoCA score and UFOV risk categories in the groups of fail and fail with potential on the road test. The fail group had a lower MoCA mean score and higher proportion of subjects with high-risk UFOV category compared with the group who failed with potential. Thus, clinically it could be useful to identify those who have potential to be referred to driver retraining programs, given the existing evidence of the effectiveness of driver retraining programs in improving driving awareness and driving behavior in older adults (Korner-Bitensky et al., 2009)
There are some limitations in this study. A historical cohort with clinical data was used, and the occupational therapist of the on-road test was not blind to the MoCA score, or to the diagnosis of the participants. However, the fact that there are two evaluators (the occupational therapist and the driving instructor) who were involved in the decision-making process with regard to the result of the on-road test should have reduced potential bias. There are also some known limitations to the use of the on-road test as an outcome measure (such as uncontrollable environmental factors, driver experience, driver intrinsic factors, assessor differences) (Ott et al., 2012), although it is still considered the gold standard in evaluating fitness to drive (Korner-Bitensky et al., 2005). In our sample, some of the participants had a physical disability in addition to cognitive impairments, which may have influenced the results of the on-road tests. However, the presence of physical disability and use of adaptive equipment for driving were a factor for only a small number of participants (n = 23). In addition, the potential influence of physical disability and age were taken into consideration in the analyses to decrease such potential bias in the result. Another limitation pertained to the analyses performed with the UFOV test as only subjects who completed all three subtests were included. Not including those who could only partially complete the UFOV because of cognitive impairments and who would obtain lower scores on the MoCA could have biased the results. Finally, the results of this study may be limited in the ability to generalize to other populations that are not targeted by the specialized driving evaluation program in rehabilitation centers.
This study has important clinical implications. As the MoCA has been shown to be more predictive than the MMSE in detecting mild cognitive impairment (Nasreddine et al., 2005), it is increasingly being used by clinicians working with individuals with potential cognitive impairment. Given the cognitive demands of the driving task, these individuals may be at risk for driving. In the current study, the MoCA demonstrated a sensitivity of 84.5% with a cut-off score of ≤25, which makes it especially useful for identifying those who are at risk. However, its lower specificity (50%) implies that a proportion of safe drivers may be asked to undergo more in-depth testing. Clinicians should take this into consideration when using this assessment and should not use it as the sole tool to make a recommendation with regards to driving safety. Compared with other tools, such as the UFOV, the MoCA has the advantages of being inexpensive, transportable, quick to administer, and readily available in several languages.
Conclusion
The MoCA is a brief and accessible test that was developed to screen MCI. This study showed that the MoCA has moderate predictive abilities and therefore, although it can be a valuable instrument for screening at-risk drivers, it should not be used as the sole tool for identifying those who are likely to fail the on-road driving test. The findings also revealed that the MoCA is related to the UFOV, which has demonstrated a predictive ability to detect at-risk drivers. Further studies investigating the predictive ability of the MoCA for detecting at-risk drivers with specific population groups such as MCI or other neurodegenerative conditions are recommended. Early detection of at-risk drivers is important to identify those who need further evaluation or, for those who may be too impaired, to identify those who should prepare for driving cessation.
Key findings
The MoCA showed a moderate discriminative ability for predicting on-road performance in persons presenting with a medical condition. The MoCA was significantly associated with the UFOV risk categories.
What the study has added
The MoCA is an accessible and valuable screening tool for on-road driving performance. However, it should not be used as the sole measure for identifying at-risk drivers.
Footnotes
Ethics
Ethics approval was obtained from the Comité d’éthique de la recherche des établissements du Centre de recherche interdisciplinaire en réadaptation du Montréal métropolitain (CRIR), 23 July 2009, with the following reference number: CRIR-436-0609.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant support from any funding agency in the public, commercial, or not-for-profit sectors.