
Abstract
Introduction
Ethical tensions are an unavoidable part of occupational therapy practice. Given the significance of this, and the divergent nature of the literature, a need was identified for a systematic examination of the published literature on this topic. The purpose of this scoping review therefore was to identify, summarize, and describe existing literature on ethical tensions in occupational therapy practice.
Method
A comprehensive scoping review was conducted. In the initial search, 459 articles, spanning a 13-year time frame, were retrieved from six databases; 32 articles met the criteria for full review.
Results
Seven themes were identified that highlighted ethical tensions related to: (a) resource and systemic issues; (b) upholding ethical principles and values; (c) client safety; (d) working with vulnerable clients; (e) interpersonal conflicts; (f) upholding professional standards and (g) practice management.
Conclusion
This scoping review highlights a breadth of ethical tensions that have implications for practice, education, policy and research. It represents an important first step in mapping knowledge about ethical tensions in occupational therapy practice, and lays a foundation for future research directions.
The moral complexity of professional practice is an undeniable challenge in contemporary times (Kinsella and Pitman, 2012). Such complexity frequently leads to ethical tensions that have become an unavoidable part of practice for all health care professionals. Three types of ethical tensions have been identified in the ethics literature (Jameton, 1984) and taken up in occupational therapy (Kinsella et al., 2008; Opacich, 1996). Ethical uncertainty occurs when an individual is uncertain about which moral principles apply or whether a situation is indeed a moral problem. Ethical distress occurs when an individual knows the right course of action but feels constrained to act otherwise by institutional or organization rules. Ethical dilemmas occur when an individual faces two or more equally pleasant or unpleasant situations that are mutually exclusive. In this study we use the broad term ‘ethical tensions’ to encompass all three of these types of tensions. Ethical tensions are defined as: events in professional life that raise morally troubling concerns that involve practitioner uncertainty, distress or dilemma (Kinsella et al., 2014).
Further, we assume that implicit within what are identified as ethical issues in the literature are ethical tensions. Given our interest in ethical tensions that are widely and collectively experienced by occupational therapists, we chose to use the term ‘ethical tensions’, rather than ‘moral tensions’, which we viewed as depicting a more personal or individualistic orientation. Nonetheless, we acknowledge that conceptions of ethics and morality, and of ethical tensions and moral tensions, are frequently used interchangeably in the literature (Seedhouse, 2009).
Scholarly literature about ethical tensions in occupational therapy practice is limited (Kinsella et al., 2008; Kumas-Tan and Beagan, 2003), interspersed, and has yet to be systematically examined. Although there is little research that examines the nature and extent of ethical tensions, there is an emerging body of literature that identifies the types of ethical tensions reported in practice settings. These include ethical tensions related to: discharge planning (Atwal and Caldwell, 2003; Durocher and Gibson, 2010); decision-making (Horowitz, 2002); implementing client-centred care (Kyler, 2008); accepting gifts (Grisbrooke and Barnitt, 2002) and goal-setting (Levack, 2009). In a phenomenological study examining the ethical tensions that students experience or witness in educational practice, Kinsella et al. (2008) reported four major themes: systemic constraints, conflicting values, witnessing questionable behaviour, and failure to speak up. Hence, ethical tensions are seen to permeate both occupational therapists' and occupational therapy students' domains of practice and education.
Ethical tensions have been identified as a concern that has important consequences for different stakeholders. Ethical tensions are linked to negative consequences such as burnout (Severinsson, 2003; Sundin-Huard and Fahy, 1999) and have implications for satisfaction, recruitment, and retention of health care providers (Pauly et al., 2012). In the field of nursing, ethical tensions have been negatively linked to working relationships with colleagues (Radzvin, 2011). Decreases in quality of patient care and patient outcome were identified by Aiken et al. (2001) as potential impacts of unresolved ethical tensions within hospitals. Other disciplines such as medicine have identified ethical tensions related to emotional exhaustion, depersonalization, and low personal accomplishment (Grassi and Magnani, 2000). Conversely, ethical tensions can result in positive consequences that may concern opportunities for change. For example, Bell and Breslin (2008) assert that establishing a positive ethical climate in response to ethical tensions is linked to an increase in health care professionals' level of job satisfaction and retention. Buelow et al. (2010) point out that the results of studies into ethical tensions can assist educators in developing more effective and relevant ethics education programmes.
A review of the literature conducted by Dieruf (2003) found little research that examines the ethical tensions that occupational therapists and students encounter in practice and practice education. In addition, the knowledge base regarding the nature of ethical tensions arising in the relatively young profession of occupational therapy is not well developed compared to other disciplines such as medicine and nursing (Barnitt, 1998; Kinsella et al., 2008). This problem is compounded given that the ethics material used in health professional education is often primarily drawn from biomedical or health care ethics literature (Barnitt, 1998). Yet, it is unknown to what extent the ethical tensions that arise in occupational therapy are unique from those of other health professions. Frequent examples of ethical tensions in medicine, such as euthanasia, while of interest to occupational therapists are infrequently their primary domain of concern or influence, while ethical tensions such as issues around discharge planning (Durocher and Gibson, 2010) may be more regularly encountered by therapists.
Given these challenges, the primary purpose of this scoping study was to identify, summarize, and describe existing literature on ethical tensions in occupational therapy practice. The study addressed the following research question: What is the current state of knowledge as depicted in the peer-reviewed literature regarding ethical tensions in the field of occupational therapy?
Method
Scoping reviews are used to map ‘key concepts underpinning a research area … especially where an area is complex or has not been reviewed comprehensively before’ (Mays et al., 2001: 194). The current review adopted Arksey and O’Malley's (2005) five-stage methodological framework, which involves: (1) identification of the research question; (2) identification of relevant studies; (3) study selection; (4) data extraction; and (5) data synthesis.
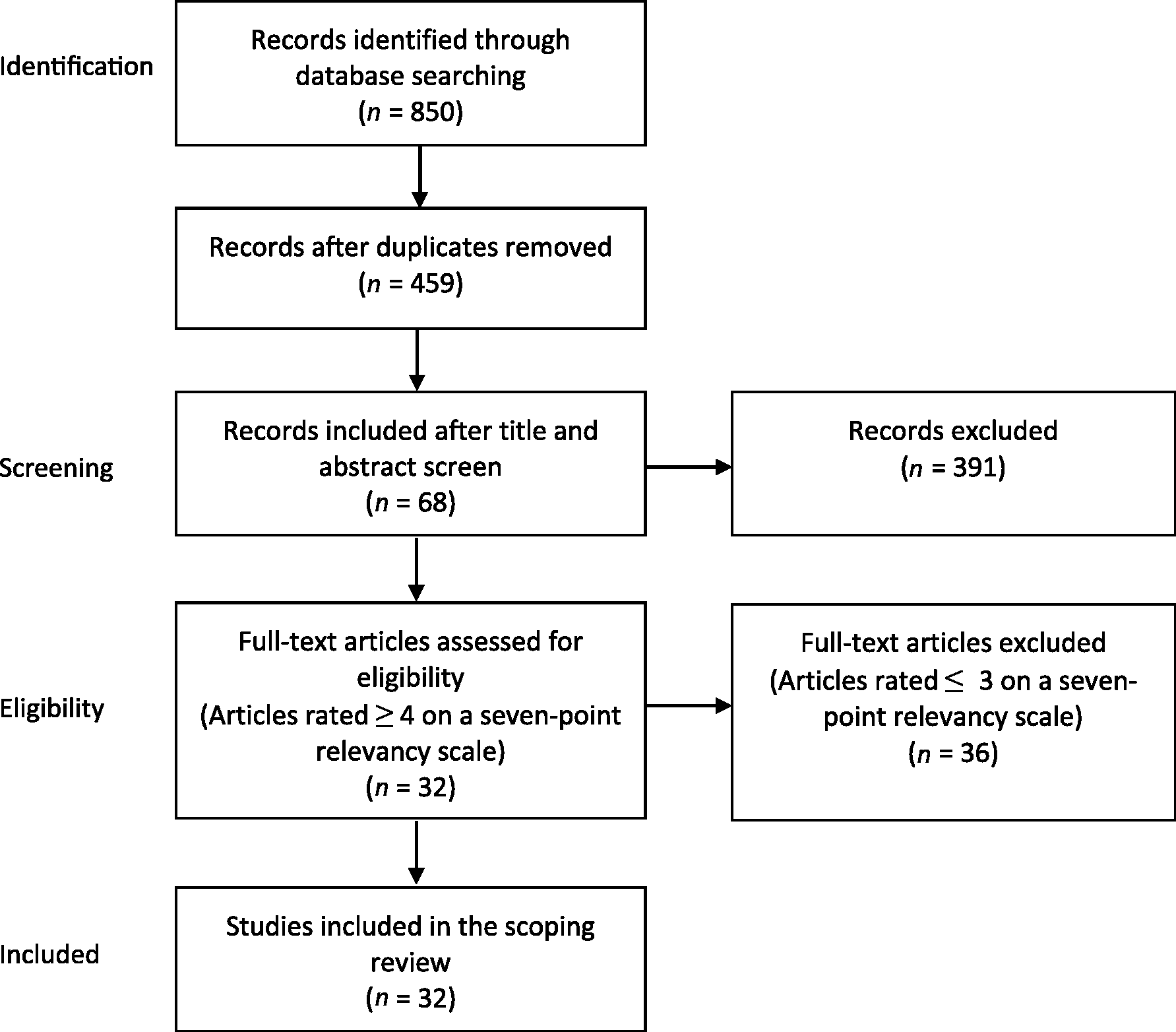
An extensive database search involved consultation with a reference librarian, and an electronic search in the following databases: CINAHL, EMBASE, Scopus, PsychINFO, PubMed, and ProQuest Nursing & Allied Health. Key words used for the search included: ethical tension or ethical issue or ethical dilemma or ethical distress or ethical uncertainty or ethic, and occupational therapy. The search was limited to articles that were peer-reviewed and published between January 2000 and March 2013. The initial search process yielded 850 articles, which were imported into RefWorks, where duplicates were deleted, for a total of 459 articles.
Inclusion and exclusion criteria were identified to further screen the articles by titles and abstracts. Articles were included if they met the following inclusion criteria:
The article addresses ethical tensions in occupational therapy practice. The article addresses ethical tensions pertaining to practising occupational therapists or occupational therapy students. The article includes the terms ‘ethics’ and/or ‘ethical’ and/or describes an ethical tension. The article includes the terms ‘occupational therapy’ and/or ‘occupational therapist’. The article was published between 2000 and 2013. The article was published in English. The article was peer-reviewed. The reference to ethics related to research ethics. The article was not available in English. The article was grey literature. Flowchart of study retrieval and selection process (adapted from PRISMA, Moher et al., 2009).
Exclusion criteria were:
Each of the 459 abstracts was reviewed to determine eligibility. If an abstract was not available, the full article was reviewed. A total of 68 articles met the inclusion criteria. Each article was reviewed and independently rated for relevancy by two researchers, from 0 (no mention of ethical tensions) to 6 (explicitly addresses ethical tensions in occupational therapy practice; ethical tensions were the major focus. Thirty-two articles were rated either 6 (18), 5 (eight), or 4 (six), and included in the final analysis (refer to Figure 1).
The final 32 articles were read in full. Data were extracted according to: title of the study; author(s); publication date; journal; location of study; research objectives/purpose statement/research question; type of population; research setting; article type; methodology; methods; main findings; ethical tensions identified; and comments/queries.
The data was first analysed numerically according to the categories identified above. Second, the data was analysed thematically to map the ethical tensions in occupational therapy practice identified. The development of themes was an iterative process. First, each researcher independently created a map of themes and subthemes that emerged from analysis of the data. Mind mapping is a technique that uses lines, colours, pictures and diagrams to form associations and relationships between ideas (Davies, 2011). The researchers met on three occasions to discuss the emerging findings, refine mind maps, themes and subthemes, integrate ideas, and to collaboratively generate a thematic map of the findings.
Results
Descriptive numerical summary
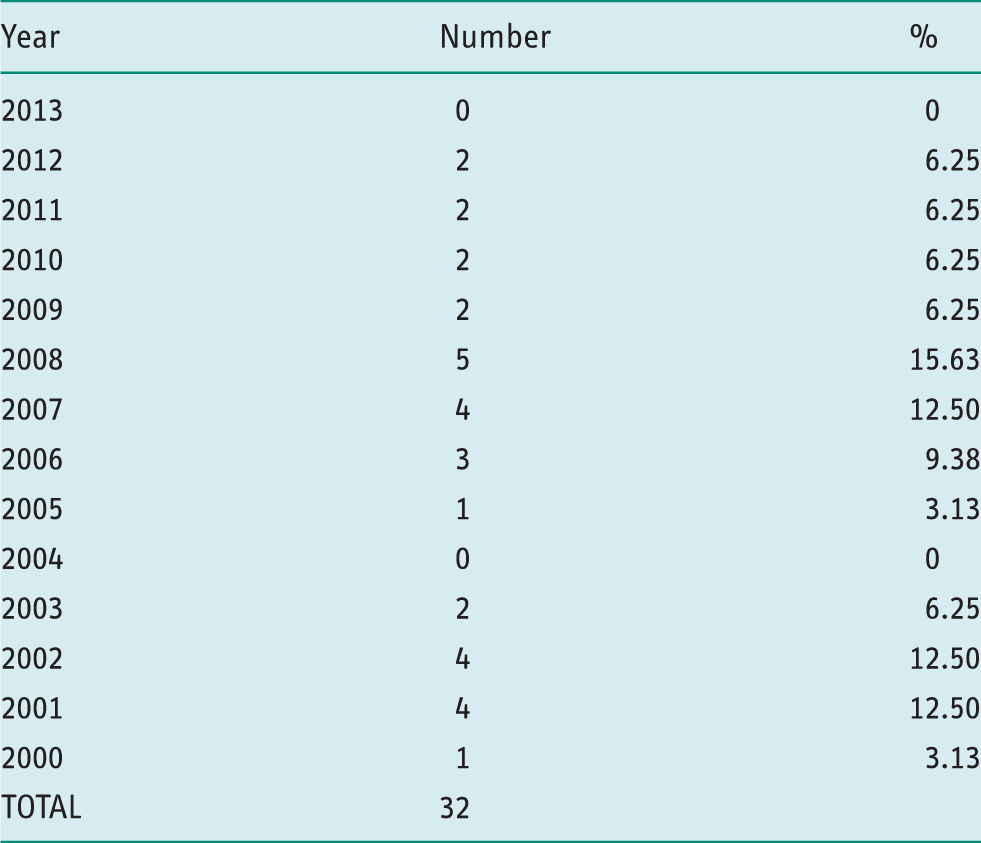
Year of publication.
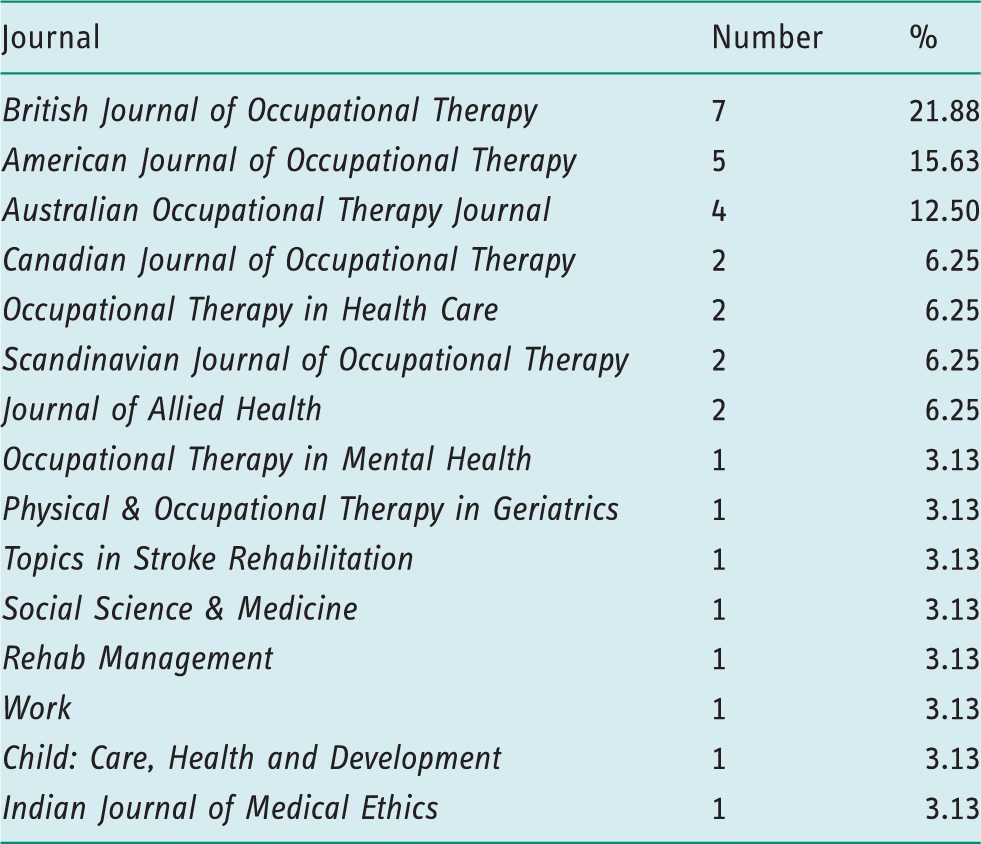
Journal of publication.
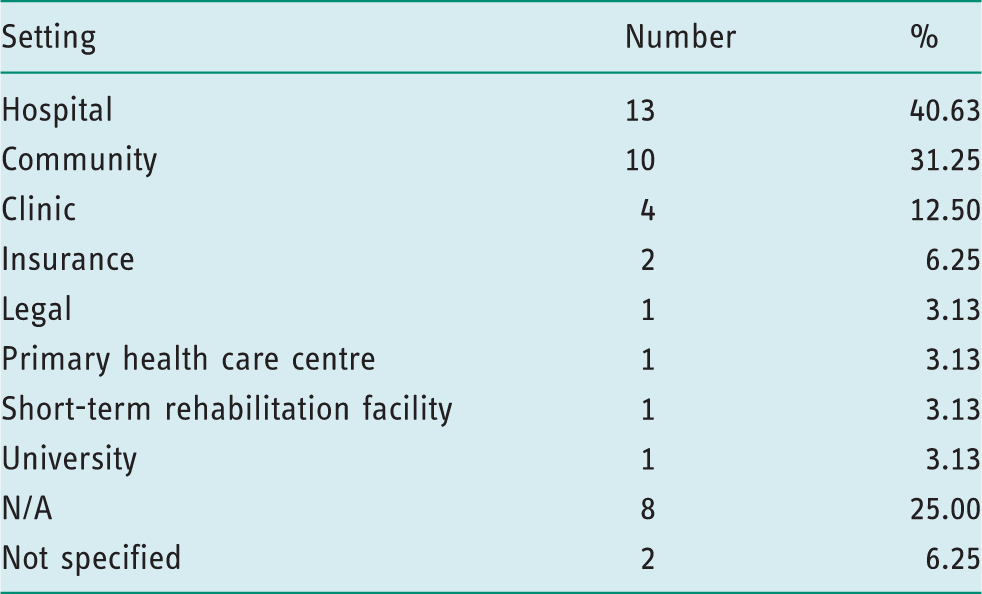
Research setting.
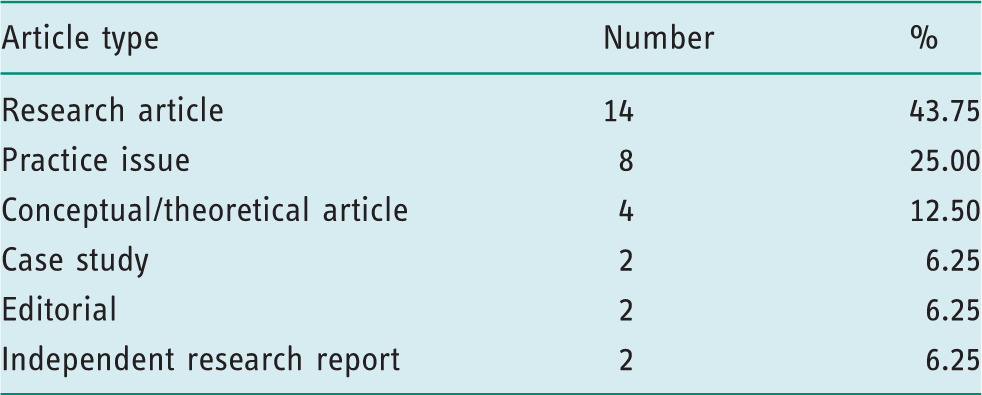
Article type.
Thematic analysis
Seven major themes were identified, including: resource and systemic issues; upholding ethical principles and values; client safety; working with vulnerable clients; interpersonal conflicts; upholding professional standards; and practice management.
Resource and systemic issues
Ethical tensions arising from resource and systemic issues was the predominant theme. Limited resources in occupational therapy were identified as: inadequate time for quality practice (Carrier et al., 2010; Kinsella et al., 2008; Walker, 2001); challenges to implementing interventions with insufficient economic resources (Kassberg and Skär, 2008); therapists needing to fight for funding; and delays in receiving equipment (Walker, 2001). Other systemic issues included insufficient staff, excessive caseloads, and lack of resources to inform practice.
Tensions surrounding access to services was another issue identified. Carrier et al. (2010) highlight a gap between the demand for occupational therapy community services and the resources available. They identified four elements that shape access: subjective criteria to prioritize who gains access; partial responses to clients' needs due to waiting lists; delegation of occupational therapy tasks to other professionals; and inordinate waiting times for some populations. Carrier et al. (2010) further suggest that resources are determined by political priorities, raising questions regarding how many resources and services should be provided and to whom. The pressure for cost containment was another ethical tension. American occupational therapists described how adjustments to managed health care affected their practice (Walker, 2001). They expressed frustration about insufficient therapy sessions due to cost containment, and at case managers who made reimbursement decisions based on cost containment. In another study, therapists identified client needs for multiple prostheses that were not met due to cost containment measures (Shivji, 2009).
The pressure of productivity measures was also found in instances of over-referral of patients for monetary gain and under-referral of ‘difficult’ clients to increase productivity (Walker, 2001). Therapists reported having to compromise therapeutic regimes, use abbreviated assessment tools to meet productivity quotas, and struggles to ‘distinguish between resourcefulness in manipulating therapy activities within reimbursement rules and compromise of professional values to conform to monetary values’ (Walker, 2001: 134).
In another study, Foye et al. (2002) reported group treatment being used despite the lack of evidence supporting outcomes equal to individualized therapy (Foye et al., 2002). Walker (2001) noted ethical tensions in group treatment related to client access to therapists, and when clients are charged while waiting to see the therapist.
Upholding ethical principles and values
Ethical tensions surrounding upholding ethical principles and values was a major theme identified in the review. Brown and Griffiths (2000) identified confidentiality dilemmas involving the principle of autonomy when students withhold or disclose their own disabilities in education contexts. Truth telling (veracity) was another prevalent ethical tension identified in a survey of 38 occupational therapists in a rehabilitation hospital (Foye et al., 2002). Examples included the disclosure of a patient's prognosis and the efficacy of group therapies. Another issue was identified when working with people with cognitive issues regarding whether it is better to tell the truth and contribute to a client's distress or to tell a lie (Lohman et al., 2003). Scarce resources pose challenges ‘often with resulting conflicts between principles of justice and equity … principles of fidelity (faithfulness) to colleagues and employers and the principles of veracity (honesty) and beneficence (bringing about good) in relationships with patients and families’ (Horowitz, 2002: 10). A case study by Wells (2007) identified ethical principles of autonomy veracity, justice, fidelity, and beneficence as being at risk in clinical decision-making.
Atwal and Caldwell (2003) identified ethical tensions in discharge planning related to the ethical principles of respect for autonomy, beneficence, non-maleficence and justice. For instance, the principle of non-maleficence is raised when a therapist's opinion about discharge differs from the team; a tension between acting for the client and being perceived as delaying discharge arises. Moats and Doble (2006) found that either discharge planning focused solely on risk avoidance or autonomy was inadequate, proposing a more balanced approach.
Client safety
Ethical tensions concerning client safety were identified with respect to discharge planning, knowledge of unsafe behaviour, practice errors, clinical education, and involvement in research. In discharge planning, Durocher and Gibson identified challenges as therapists ‘balance commitment to client safety with the client's values and priorities’ (Durocher and Gibson, 2010: 2). In their case study, the team was concerned that discharge would place the client ‘at risk of declining medically and sustaining another fall’ while the client stated that ‘living elsewhere would make him unhappy and be “meaningless”’ (3). Further, ethical tensions were identified when therapists had knowledge of unsafe client behaviour, for example knowledge of drug use or clients who continued to drive despite being unsafe (Foye et al., 2002).
A second area of concern was practice errors (Lohman et al., 2003; Lohman et al., 2008; Mu et al., 2006). Lohman et al. (2008) identified different categories of practice errors including misjudgement, lack of treatment preparation, error from lack of experience, and insufficient communication. As examples, therapists misjudged how long to leave a hot pack on their client; a client fell and injured himself because a therapist did not prepare protective mats for treatment; therapists failed to refer their clients to appropriate outpatient services; an occupational therapist mistreated bicipital tendonitis leading to prolonged shoulder pain; a therapist failed to communicate that specific clients were on bed rest and the clients were taken for daily walks.
Lohman et al. (2003) found that therapists frequently responded either by learning from their errors, responding emotionally, or seeking support. Sometimes therapists avoided facing the error. Mu et al. (2006) found that errors can cause emotional distress and physical harm to clients and therapists. They indicated that therapists who disclose their practice errors cope in a more constructive way.
Concerns about safety also occur during student placements and research settings in occupational therapy. Brown and Griffiths (2000) described a student being paired with another student (who confided a medical condition) who was not handling clients safely. In another study, Atkinson (2005) highlights issues of safety that arise when research participants open up about emotional issues; while it can be therapeutic it also has the potential to cause emotional harm.
Working with vulnerable clients
Another theme was ethical tensions that arise when working with vulnerable clients. In a study by Foye et al. (2002), occupational therapists identified the questionable decision-making capacity of clients as an ethical issue. Durocher and Gibson (2010) describe a case study involving an older adult who wanted to be discharged home; however, the client's decision-making capacity could not be determined. Further, Kassberg and Skär (2008) discussed tensions that can arise when working with individuals with developmental disabilities, highlighting challenges when clients are partly competent to make their own choices, and when they were not involved in their own health related decision-making.
Further examples arose in a study by Kinsella et al. (2008). Occupational therapy students described ethical tensions when team members did not respect patient confidentiality; when disrespectful attitudes were conveyed; or when practitioners discussed ‘clients in negative ways, by labeling and stereotyping clients, making inappropriate comments … or referring to clients only by their diagnosis’ (179). Foye et al. (2002) identified tensions when therapists were unsure if they should speak about their client to family members, or disclose personal medical information (such as HIV) to the health care team.
Ethical tensions were also identified when working in dementia care. Plastow (2006) discusses the use of tagging and tracking technology (GPS bracelets), and its potential uses to assess wandering behaviour. Such technology may allow people to live longer at home, but is negatively associated with tracking prisoners and animals, and can threaten personhood and violate human rights. Another tension is the use of restraints to manage challenging behaviours. In addition to overt use of restraints, Cotterill (2012) points out that restraints can be subtle such as seating a client in a low chair that prevents transfer out of the chair.
Interpersonal conflicts
Ethical tensions involving interpersonal conflicts were identified as occurring between occupational therapists, clients, family members, other health care providers, and institutions. Walker (2001) reported on an occupational therapist's frustration with having to justify why a patient may require a splint for longer than the six-week protocol. Tensions and conflicts may be generated when the clinical opinions of therapists are not respected. Another conflict involves goal-setting. In a survey of occupational therapists in a rehabilitation setting, Foye et al. (2002) found that conflicts around goal-setting were frequently mentioned. They highlight challenges within multidisciplinary teams when attempting to set ‘appropriate rehabilitation goals for patients’ (Foye et al., 2002: 93). Tensions were seen when patients were considered poor candidates for rehabilitation, including those no longer interested, or in the final stage of life.
Challenges were reported when patients or family members had goals that conflicted with what the therapist considered as therapeutically appropriate. Foye et al. (2002) reported examples of patients and families wanting therapy when the person has plateaued, or wanting equipment that is inappropriate for their needs. Similarly, Kassberg and Skär (2008) found that ‘clients who asked for special technological interventions such as advanced electric wheelchairs and lifts created ethical dilemmas because clients and relatives often had an opinion contrary to that of the occupational therapist’ (208). Further, Foye et al. (2002) describe the challenge that arises when a client or caregiver refuses to follow treatment recommendations. Flecky (2001) considered the case of an uncooperative patient, suggesting that this patient's ‘refusal to participate in therapy may reflect a value conflict around the question of who establishes therapeutic goals and how these goals should be implemented’ (22), thus highlighting the unequal power inherent in patient–therapist relationships as creating tensions.
Kinsella et al. (2008) found that value conflicts were an ethical tension identified by occupational therapy students. A student described a conflict between an occupational therapist and client regarding the best course of treatment: … the practice of occupational therapy looks at … making people more independent in life. She wasn't into being more independent; she was fine with being dependent on her family, but the occupational therapist didn't feel that way. She felt that she wasn't holding up her practice (179).
Upholding professional standards
Ethical tensions related to upholding professional standards such as implementing client-centred practice, evidence-based practice, competency of occupational therapists, and failure to speak up were identified in the literature. Ethical tensions relating to client-centred practice were identified by Hammell (2007), who noted tensions between therapists’ attempts to be client-centred, while needing to serve the system in which they are employed. She offers the example of an occupational therapist who believes it is in the best interest of the client to order a specialized wheelchair, while the service providing funding enforces a policy that people entering nursing homes are not eligible to receive wheelchairs. Hammell (2007) argues that upholding client-centred practice would require the therapist to advocate for the wheelchair and for provisions regarding policies for specialized wheelchairs in nursing homes. However, she notes that therapists frequently feel powerless, not wanting to ‘rock the boat’, or threaten job security.
Kyler (2008) also contends that occupational therapists are not able to implement client-centred care due to: inadequate workplace support; lack of understanding of what client-centred really means; relationships of power between clients and therapists; and questions concerning who to include, and when, in decision-making. Pollard and Sakellariou (2007) argue that part of being client-centred means that the area of sexual health must be explored with people living with disabilities. They assert that failure to attend to this area creates ethical tensions by compromising the quality of care, and putting clients at risk of adopting precarious approaches to pursue their sexual needs.
Another professional standard that was identified as important yet difficult to uphold was evidence-based practice (Rodger et al., 2012). Christiansen and Lou (2001) note that the primary reason for implementing evidence-based practice is a moral one. Nonetheless, they caution that while it is important, we may overlook its limits: ‘we may forget that clinical decision making, at its core, is an ethical matter, and we may lose sight of the ethical dilemmas hidden beneath our efforts to produce the most effective … outcomes’ (Christiansen and Lou, 2001: 345). Furthermore, limited evidence for complex practices presents an ethical challenge to occupational therapists. They point out that context is important in the application of research, and that instances exist for which objective measures may not apply, or where other values, such as patient autonomy, may be more important.
Ethical tensions were also related to issues of competency. Kinsella et al. (2008) found that occupational therapy students experienced ethical tensions related to speaking up and advocating for clients. For working therapists, Murray and Lawry (2011) indicate the importance of maintaining ‘professional currency’ or participation in activities for professional development and practice competency. They noted a tension in that although therapists recognize the professional and ethical obligations to maintain professional currency, some do not for various reasons such as not knowing where to start with unfamiliar activities. Unfamiliar activities identified by participants included implementing evidence-based practice, undertaking research, and critiquing and exhibiting resource constraints.
Practice management
Ethical tensions around practice management also emerged related to professional boundaries, caseload management, dual roles, documentation, and professional accountability. Tensions with professional boundaries are raised in questions concerning whether or not therapists should accept gifts (Grisbrooke and Barnitt, 2002). Further, Kassberg and Skär (2008) point out those social relations do develop over time, to the point where therapists can be regarded as a friend. They note that ethical tensions can occur when therapists find themselves being invited to clients' birthday parties, given gifts, or invited to meet a client at a café outside of work time. Foye et al. (2002) identified dating patients as another ethical issue that could arise.
Ethical tensions with respect to caseloads were also identified. Kolehmainen et al. (2011) assert that tensions can occur when perceived moral duties are not in line with the duties defined by the service policies. For example, policies may indicate that if a child does not attend appointments then they should be discharged, whereas a therapist's moral duty may suggest otherwise. Flecky (2001) highlights a tension when patients refuse participation in therapy, and therapists feel in conflict with their duty to care.
Van Denend and Finlayson (2007) identified ethical tensions that occur when the responsibilities of being a researcher diverge with those of an occupational therapist. For instance, when a research participant discloses information that suggests elder abuse during a research interview. Further, Atkinson (2005) noted a role conflict between maintaining duty of care as an occupational therapist and best practice as a researcher. For example, when a participant asked the researcher to help install a bath seat, the therapist reported finding it difficult not to help (Conneeley, 2002).
Ethical tensions related to documentation and accountability also emerged. Lundgren (2001) discussed therapists' hesitation to document intimate personal matters, and uncertainty about whether or not to document psychological issues. Freeman et al. (2009) further identified tensions with upholding professional accountability obligations when they were seen to conflict with the ideal of professional autonomy.
Discussion and implications
The findings of this study have important implications for occupational therapy practice, policy, research and education.
Implications for practice
Understanding the ethical tensions that occur in occupational therapy practice, and making them explicit, is important in preparing practitioners to think about and negotiate such tensions in their practices. For instance, awareness of ethical tensions that may occur between therapists and clients can better inform client-centred practice and quality of care, and enable therapists to be pro-active in their approaches to such tensions. Further, ethical tensions have been linked to negative consequences such as burnout (Severinsson, 2003), while their positive resolution can result in increased job satisfaction and retention of practitioners (Bell and Breslin, 2008).
Given the finding that many of the ethical tensions arose from systemic and resource issues, the effort to negotiate ethical tensions may be seen as extending beyond individual practitioners. Awareness that organizational environments, policies and cultures may be implicated in the generation of ethical tensions, their prevention, and resolution is important knowledge for front line practitioners and administrators.
Implications for policy
While ethical tensions are frequently thought of as occurring at the individual level, it is important to consider how factors outside of therapists’ control, such as working within policy-dependent systems, shapes ethical tensions (Kinsella et al., 2008). Ethical tensions arising from resource tensions were identified in the study, as were systemic issues that interfered with the operationalization of professional standards such as evidence-based and client-centred practice. Resource policies developed at governmental and institutional levels shape the front line practices of therapists, which ultimately affect client care. Therefore, these findings reiterate Kinsella et al.’s suggestion of a ‘need for greater attention to the ways in which macro-level policies can shape micro-level practices, and thus raise ethical issues for occupational therapists’ (Kinsella et al., 2008: 180–181). It is important that the roots of such tensions are made explicit, so that therapists are not ‘blamed’ for issues beyond their individual control, and so that dialogue about such issues may be engaged with in the discipline, and at institutional, policy, and professional levels.
Implications for education
By contributing to knowledge about types of ethical tensions in occupational therapy practice, this review has the potential to contribute to the education of future and currently practising occupational therapists. Knowledge about ethical tensions that may arise in practice, and discussions concerning how to navigate such tensions, has the potential to better prepare students to face ethical tensions they encounter in their clinical placements and as they enter the workplace.
Advocacy can be an important response when dealing with ethical tensions. For example, Hammell (2007) explains that advocating for wheelchairs in nursing homes is a way in which occupational therapists can uphold client-centred practice. Educating future and practising occupational therapists about how to advocate regarding ethical tensions in the workplace may be an important dimension of professional preparation. Moreover, Kinsella et al. (2008) found that occupational therapy students experienced ethical tensions when speaking up and advocating for what they believe to be the right course of action. The educational implications of learning about ethical tensions in clinical and classroom settings may extend to learning about appropriate means of advocating for positive change.
Implications for research
The findings of the review also have significant implications for future research. By identifying, summarizing, and describing the existing literature on ethical tensions in occupational therapy practice, this review lays the foundation for future programmes of research into ethical tensions in occupational therapy practice. There is a paucity of strong empirical research on this topic. Of the 32 papers, only 14 were research papers. The majority of papers were discussions of practice issues, or small-scale case studies. More empirical research that examines the types of ethical tensions that occupational therapists encounter in their practices is highly recommended. Future research that examines whether empirical research parallels the cases and issues identified in this review is recommended. Further research that examines how often and in what contexts occupational therapists experience ethical tensions is also recommended. In addition, no research was found that examined how therapists ‘negotiate’ the ethical tensions they encounter, suggesting that research in this area is of pressing concern. Furthermore, research that examines how policies and systemic issues shape the ethical tensions that practitioners encounter is highly recommended. It is suggested that a general investigation of ethical tensions in occupational therapy practice, and their negotiation, would be fruitful in laying the foundation for more in depth research in distinct practice areas, and in interdisciplinary team contexts in the future.
Gaps in the literature
Gaps in the literature were also identified. A major ethical tension reported in an unpublished study by Kumas-Tan and Beagan (2003) was related to social differences. Social differences included fear of stereotyping clients, lack of understanding people with differences, and power differentials because of differences such as socioeconomic status or skin colour. Other important bodies of literature relate to occupational justice (Townsend and Wilcox, 2004) and political practice (Pollard et al., 2008). While ‘justice’ is a major principle in ethics, and political practice is inherently related to ethical tensions, these domains were not explicitly captured in this review. Nonetheless, the principle of justice may be reflected in practice in other bodies of grey literature such as codes of ethics. In addition, practitioner-based knowledge and the work of regulatory and professional bodies on ethical tensions is another important area that was not captured in the review. The language used to theorize in these areas may not make explicit links to ethics, or may be represented in grey literature. Further scholarship that examines ethical tensions related to social difference, occupational injustice, and political practice is warranted.
Strengths and limitations
The strengths of the study include the systematic nature of the review, the adoption of rigorous methods, the quantity and range of papers included, and the study's potential contributions to practice, policy, education, and future research. Limitations may include the exclusion of studies published in languages other than English, the decision not to include grey literature (due to the size of the review), and the decision not to use the specific term ‘moral’ in the database search. The decision not to include grey literature precluded the inclusion of potentially relevant documents such as codes of ethics and literature from regulatory colleges. In regards to the latter limitation, including ‘moral’ as a search term could have been beneficial given that other professions have used the term and derivations of it when discussing ethical tensions. Ethics refers to the formal study of moral standards or conduct (Purtilo and Doherty, 2011); however, the difference between ethics and morals can be ambiguous.
Conclusion
The discussion of ethical tensions has been limited in the occupational therapy literature. This scoping review was undertaken to address this gap. The results identified seven major themes that reflect different types of ethical tensions encountered by occupational therapists and students in practice. The findings draw attention not only to a range of ethical tensions identified in the literature but also have implications for practice, policy, education and research. In view of the results, it is suggested that knowledge about ethical tensions in occupational therapy is in the early stages, and further empirical research on this topic is required. Further explicit attention to ethical tensions related to systemic issues, the organization of occupational therapy services, social difference and occupational injustice is suggested. The study lays a foundation for future empirical investigation that examines whether the issues identified align with what contemporary therapists report. In addition, research that attends to how therapists negotiate ethical tensions once they are encountered is highly recommended.
Key findings
Themes of ethical tensions identified in the study included; • resource and systemic issues • upholding ethical principles and values • client safety • working with vulnerable clients • interpersonal conflicts • upholding professional standards • practice management
What the study has added
This study has mapped the current state of the peer-reviewed literature on ethical tensions in occupational therapy practice, and has implications for practice, policy, education and research.
Footnotes
Research ethics
Ethics approval was not required for this study given that the work is a scoping review of the literature and no human subjects were involved.
Declaration of conflicting interests
None declared.
Funding
This research was funded in part by a development grant from the Faculty of Health Sciences, Western University, Canada.