
Abstract
Introduction
The aim of this scoping review was to examine and synthesise literature on adaptive equipment use for personal care and mobility after stroke.
Method
We searched databases including Medline, EMBASE, AMED, CINAHL and Scopus to February 2016. Two authors independently screened 789 titles, identifying 28 studies for inclusion in the review.
Results
Findings were grouped into four themes: (1) stroke-specific impairments and consequences for equipment use and training; (2) meaning of equipment for people with stroke; (3) cost of equipment after stroke; and (4) conflicts between equipment provision and models of stroke rehabilitation.
Conclusion
The wide range of impairments after stroke increases complexity of how people use equipment. Nonetheless, training needs and the relationship between social context, identity and equipment use are increasingly better understood,. The findings highlight a tension between practice that seeks to re-train function by ‘normal’ movement without equipment and restoration of function by using compensation strategies involving use of equipment. However, there is no evidence that compensation strategies impede recovery of physical abilities. High-quality evidence about costs of equipment after stroke, which could inform policy decisions, is urgently needed.
Introduction
The number of people who survive a stroke is growing, and improving quality of life for this group is an increasingly urgent issue, alongside reducing the financial burden of stroke on healthcare systems (Feigin et al., 2014). In the United Kingdom (UK), the cost of stroke per year is estimated at over UK£7b (Wolfe et al., 2014). In New Zealand, the country of origin for this paper, annual costs due to stroke are now estimated to be NZ$700m (Stroke Foundation of New Zealand, 2010).
Providing adaptive equipment for people after stroke can be an effective means of reducing the burden of stroke. Adaptive equipment is defined as ‘equipment that enables an individual, who requires assistance, to perform the daily activities essential to maintain health and autonomy and to live as full a life as possible’ (World Health Organization (WHO), 2004: 10). Equipment provision is often a substantial component of occupational therapy practice for people with stroke, and fits with the objective of achieving client-centred occupational-focused goals, such as being able to have a shower or move around one's house (Gelderblom and de Witte, 2002). Equipment provision can be expensive. Consequently, public health services have established systems to manage costs, such as criteria for funding particular equipment and therapists specialising in certain types of equipment assessment. The administration of equipment provision policies and processes can be time-consuming, requiring the completion of extensive paperwork, and potentially lead to challenging interactions for therapists with clients, their family or health service funder. The time spent on these activities can itself lead to additional cost to the health service.
People who use equipment after stroke present with unique challenges, with many being discharged from rehabilitation with ongoing impairments and an expectation from family and healthcare staff that the abilities of the person with the stroke will continue to improve following community-based rehabilitation interventions (Pollock et al., 2014). As a result, the equipment needs of people with stroke can be expected to change over time, and the risk of adaptive equipment use inhibiting opportunities for further recovery of unaided physical function could be queried.
Furthermore, whether or not equipment will be used as a health professional intended, or used at all, is an important consideration when prescribing it. Equipment use after stroke has been associated with personal factors (Scherer et al., 2011) and the timing of the introduction of equipment. For instance, three distinct stages of equipment use have been proposed in relation to the optimal timing of powered mobility aids: reluctant use, strategic use and essential use (Mortenson et al., 2015). It has also been suggested that the relationship between how someone with a disability views themselves and their abilities, as well as their equipment, impacts on equipment use (Lund and Nygard, 2003).
There is increasing demand on occupational therapists to justify how they spend their time with people in stroke rehabilitation (Whitehead et al., 2014). Concurrently, clients’ loss of access to social interaction and life roles – areas that can be enabled by equipment provision – remain substantial issues for stroke rehabilitation services (Woodman et al., 2014). It is timely therefore to explore what research exists on optimising use of adaptive equipment by people who have experienced stroke. To address this, we conducted a scoping review to identify and synthesise research on the provision and use of adaptive equipment after stroke. A scoping review is a type of critical review that involves mapping key concepts underpinning an area in order to identify where gaps exist and to summarise findings (Arksey and O’Malley, 2005; Levac et al., 2010). Scoping reviews are more focal than general literature reviews, and are suited when the aim is to address broad research questions, where the work involves synthesis of studies of differing methodological design, or where key concepts of an area need to be clarified (Joanna Briggs Institute, 2015). In this review, we chose to focus solely on equipment for mobility or personal care after stroke, as research and reviews on equipment use have been criticised in the past for lack of attention to the clinical characteristics and needs of specific user groups (Auger et al., 2008). The key question addressed by this review was ‘what is known about the uptake and use of equipment for mobility and personal care by people after stroke?’
Method
Selection of studies
To be included in this review, articles needed to describe the findings from a study on equipment use involving people 16 years or older who had experienced a stroke, and be published in an English-language peer-reviewed journal. Included studies also needed to focus on adaptive equipment used for activities of daily living in the home (such as making a meal, using the toilet or bathing) or for mobility in either the home or community, and needed to report on the effectiveness or utility of this equipment from the perspectives of either equipment users or providers.
Articles were excluded if they focused primarily on equipment that was deemed highly unlikely to be routinely funded by public health systems in New Zealand for personal use. Decisions regarding what equipment a public health system might not fund was based on the authors' combined experiences of working in healthcare systems in New Zealand, Australia, the UK and Ireland. We excluded studies on robotics, housing modifications, communication devices (such as iPad and speech-enhancing devices), virtual reality technology, functional electrical stimulation, orthotics and prostheses, hearing aids or glasses, personal electronic devices, personal alarms and computers. We also excluded studies that focused primarily on the engineering, product design or the biomechanics of adaptive equipment. Finally, we excluded studies involving people who experienced transient ischaemic attacks without stroke. Year of publication, study methodology or study quality were not used to exclude articles.
Search strategy and article selection
Overview of search terms.
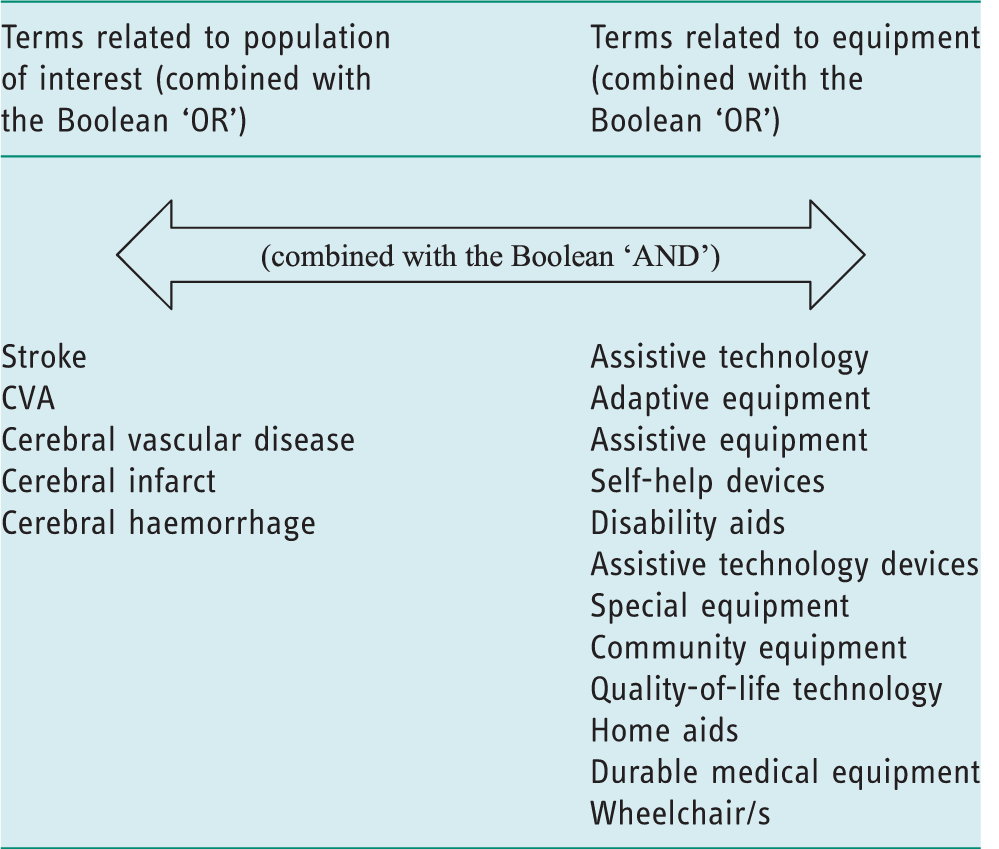
CVA, cerebral vascular accident.
Summary of study characteristics, analysis and results organised according to theme: stroke-specific impairments predicting use and related assessment and training considerations.

Fall Efficacy Scale is a self-report questionnaire that measures the perceived confidence of participants in task performance.
Summary of study characteristics, analysis and results organised according to theme: meaning and acceptance of equipment.

ICF, International Classification of Function.
Summary of study characteristics, analysis and results organised according to theme: cost of equipment.
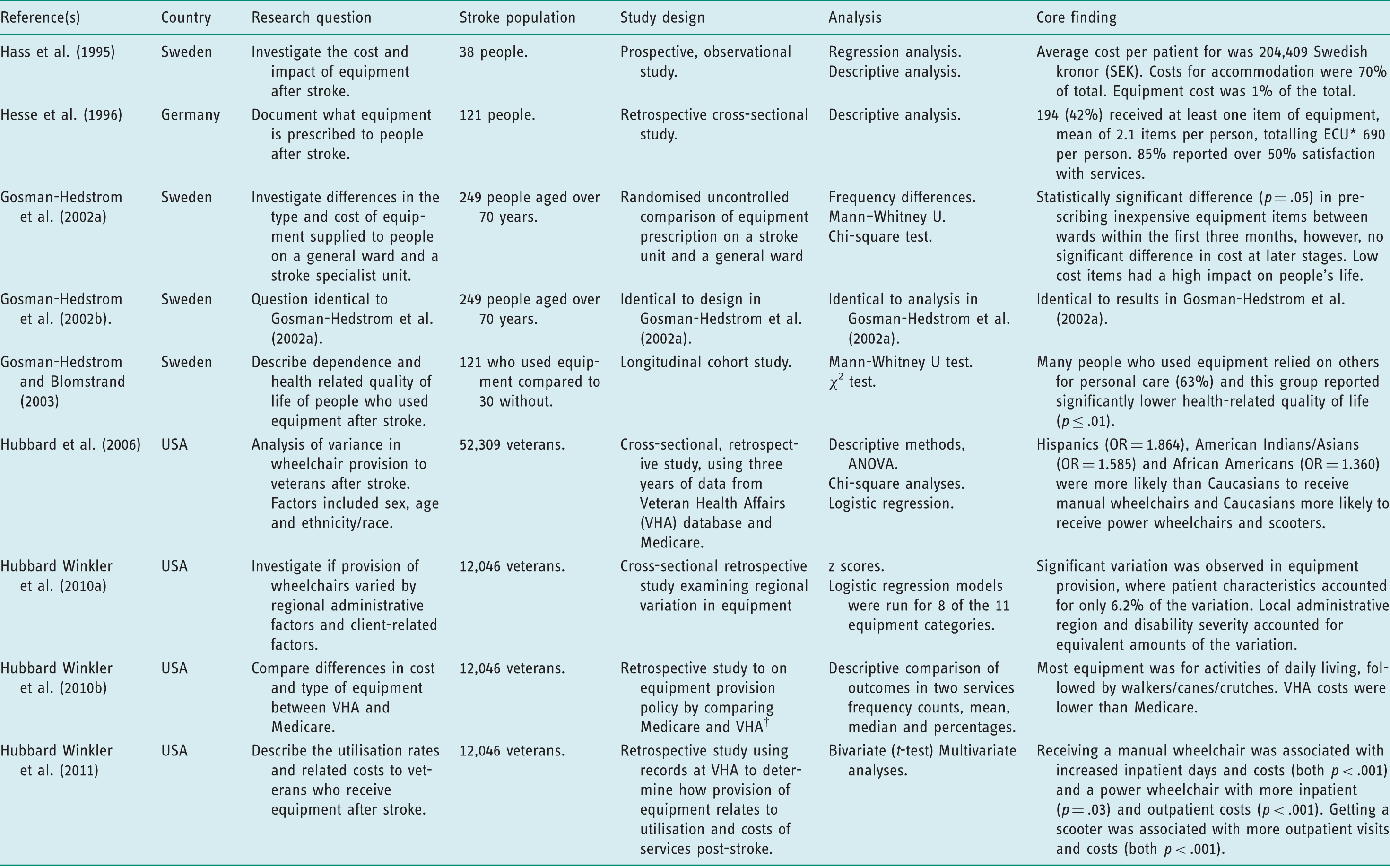
*European Currency Unit – used as the unit of account of the European Community before being replaced by the Euro on 1 January 1999. †VHA does not limit provision of equipment to in-home use only whereas Medicare has this restriction.
The titles and abstracts of all articles from these database searches were screened independently by two authors. The first author screened all articles, while the co-authors provided a second independent opinion on the inclusion or exclusion of articles by screening a third of all articles each. Differences of opinion regarding inclusion of articles were resolved by discussion. Full text articles were sought when further information was required to make a selection decision.
Data extraction and synthesis
The full text of each included article was read and key messages were noted. Descriptive data from included studies were tabulated to compare content. Data were extracted on the research question(s), country of origin, methodology, population, key findings and how the results related to the scope of this review. As formal assessment of methodological quality is not performed in a scoping review (Joanna Briggs Institute, 2015), this process was not included as part of the selection or synthesis of literature. Similarities in the aims and results of studies were noted and grouped together to form themes, and a narrative synthesis of this literature arranged around these themes was completed to summarise the review findings.
Results
Study characteristics
Our search resulted in the identification of 789 potentially relevant articles after removing duplicate citations. On screening titles and abstracts, we excluded 724 papers, identifying 65 papers for full text retrieval. On review of these full text papers, we excluded another 27 articles, leaving 38 for inclusion in the review. Most studies were excluded because the equipment being studied was not specific to mobility or personal care. No studies were excluded at the screening stage because the technology was deemed unlikely to be funded by a public health system. A flow diagram for the selection of articles for inclusion is present in Figure 1 based on PRISMA guidelines (Moher et al., 2009). These 38 articles presented findings from 28 discrete research projects, with data from seven individual studies being presented across more than one publication.
PRISMA flow diagram (Moher et al., 2009).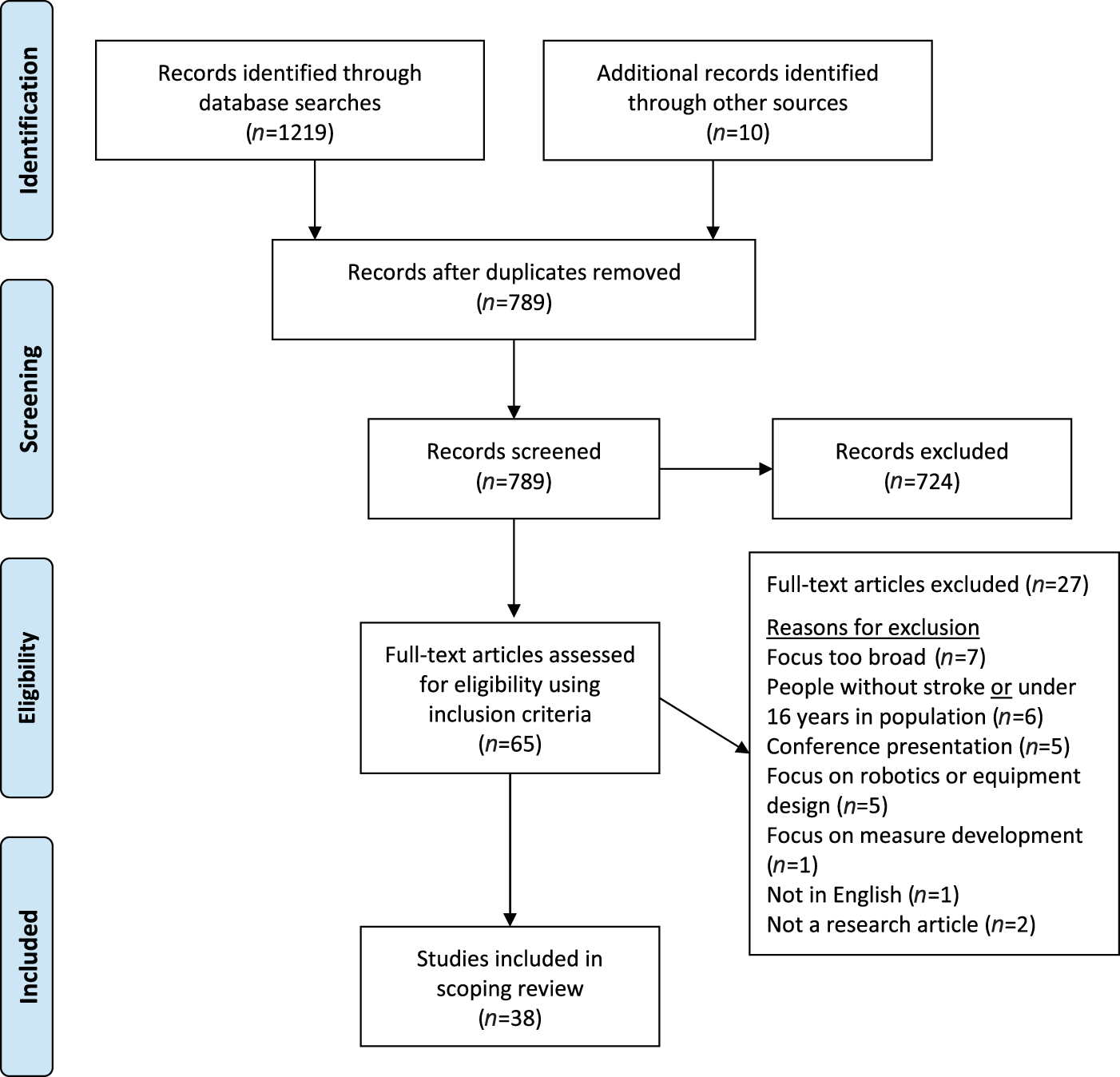
Of the included studies, 10 were conducted in the United States (USA) (Garber et al., 2002; Gitlin, 1998; Hubbard et al., 2006; Hubbard Winkler et al., 2010a, 2010b, 2011; Mann et al., 1995; Mountain et al., 2010a, 2010b, 2014; Prangrat et al., 2000; Skolarus et al., 2014), five in the UK (Barrett et al., 2001; Lennon, 1991; Punt et al., 2008, 2011; Turton et al., 2009; Tyson and Rogerson, 2009), three in Sweden (Gosman-Hedstrom and Blomstrand, 2003; Gosman-Hedstrom et al., 2002a, 2002b; Pettersson et al., 2006, 2007b, 2007a), three in Canada (Barker et al., 2004, 2006; Jutai et al., 2007; Reid et al., 2001; Rudman et al., 2006), and one each in Hong Kong (Chiu and Man, 2004), Switzerland (Allet et al., 2009), Germany (Hesse et al., 1996), Denmark (Sorensen et al., 2003), Israel (Laufer, 2003) and Korea (Kim and Kim, 2015). Four studies were randomised control led trials (RCTs) (Barrett et al., 2001; Chiu and Man, 2004; Mountain et al., 2014; Tyson and Rogerson, 2009), while others primarily used either descriptive designs such as cross-sectional or cohort frameworks, at times in combination with economic evaluations, or they consisted of qualitative research. No systematic reviews specific to adaptive equipment use for people after stroke were found.
Overview of review findings
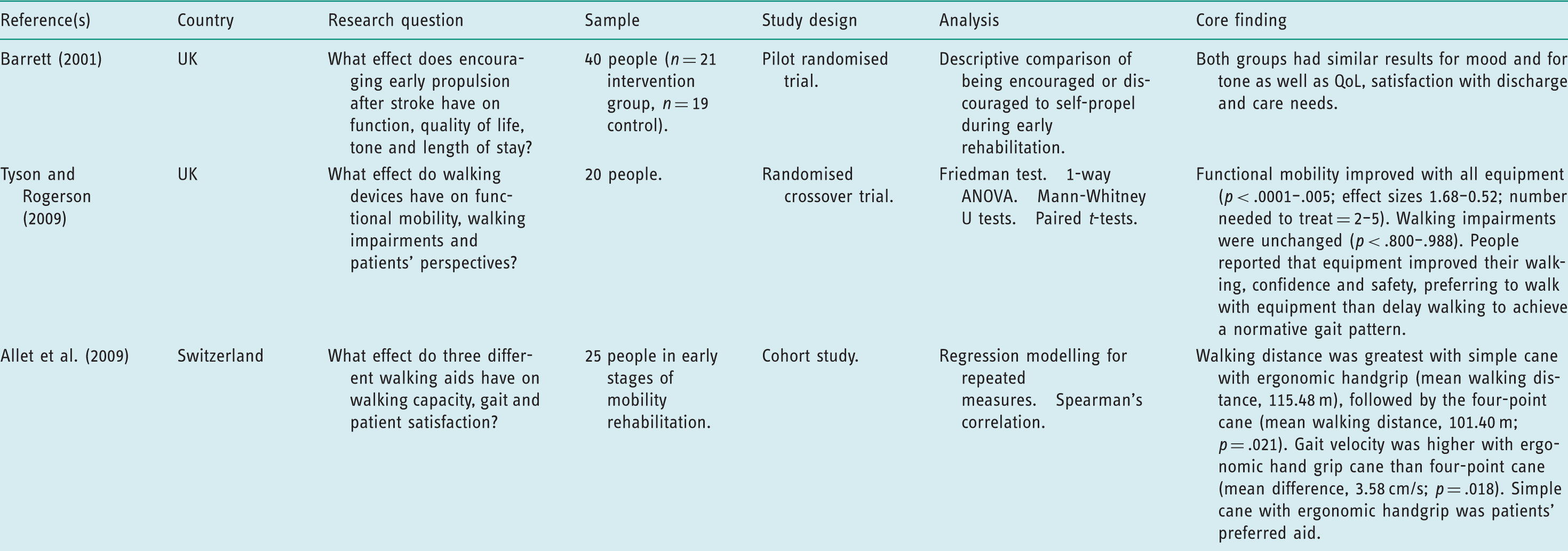
Summary of study characteristics, analysis and results organised according to theme: equipment use conflicting with stroke rehabilitation approaches.
Stroke-specific impairments and consequences for equipment use and training
The impairments that result from stroke are complex and broadly influence the extent and type of equipment used (Garber et al., 2002). Many who use equipment have poor balance and are at high risk of injury from falls (Kim and Kim, 2015); and people with stroke who need equipment can have difficulties getting out of their house (12.4%), as well as moving around inside their house (11.9%) (Skolarus et al., 2014). People often experience cognitive difficulties after stroke though one longitudinal study reported that having better cognition after stroke was reliably associated with equipment use (OR = 1.46; 95% CI, 1.03–2.07) (Jutai et al., 2007). From this literature, it appears that the wide range of impairments that can be associated with having a stroke increase the complexity of how people interact with equipment.
In one of the few longitudinal studies of equipment use after stroke, Sorensen et al. (2003) reported that 75% of 155 consecutive clients discharged from a Danish hospital with stroke had received equipment. Almost all of those followed up at 6 months and between 3 and 5 years were using assistive equipment or environmental modifications (93%; 71/76). The mean number of items of equipment provided was 4.4 (SD = 2.39). A total of 83% (96/116) were prescribed mobility aids, and 63% (73/116) rated bathing and mobility aids as their most valued items, though many (37.9%; 44/116) had equipment prior to stroke. These researchers also noted, similarly to others (Mann et al., 1995), that the amount of adaptive equipment owned can increase in the years post stroke.
Perceptual impairments that result in visual–spatial neglect commonly occur when people have a right hemisphere stroke, and introduce a significant and often poorly understood challenge when it comes to equipment provision (Prangrat et al., 2000). People with neglect tend to use the equipment they are issued less (Prangrat et al., 2000), have more wheelchair collisions (Turton et al., 2009), and have more difficulties navigating obstacles when using their mobility equipment, than those without neglect (Punt et al., 2008; Punt et al., 2011). People with left-hemisphere stroke are more likely to receive a wheelchair at discharge from hospital than those with right-hemisphere stroke (OR = 3.33; 95% CI, 1.33–8.33) (Mountain et al., 2010b). The presence of neglect, therefore, may impact on the provision and uptake of equipment.
Several studies have examined the training needs of people with neglect after stroke to establish how to maximise benefits from equipment for this group. In a small cohort study exploring the outcome of a wheelchair skills training programme for 10 people with stroke, Mountain et al. (2010a) found that even though people with neglect scored lower on a powered wheelchair skills test before and after training compared to the group without neglect, the scores of both groups improved – and improved to the same extent. Similarly, Dawson and Thornton (2003) found that driving accuracy improved for two people with stroke after practice navigating a wheelchair obstacle course over 2 weeks, while Punt et al. (2011) demonstrated that simply changing the position of a power chair joystick from one side to the other had a significantly positive effect for four people with neglect in terms of their ability to navigate with their wheelchair (p < .025).
Home-based training also appears to improve ability and satisfaction with equipment use. In a RCT in Hong Kong, Chiu and Man (2004) compared additional (2–3 visits) home-based training in equipment use (n = 30) to hospital-based training only (n = 27) for people after stroke. A significant increase in both the users' functional abilities (t = 3.89; df = 51; p = .01) and their satisfaction with the equipment (t = 69.8; df = 29; p = .01) was observed. Similarly, other studies also found that more in-home training, in the form of pre-discharge visits, increased the uptake of equipment use by people with stroke (Hesse et al., 1996; Sorensen et al., 2003). Finally, people with stroke who receive formal powered wheelchair skills training appear to improve their wheelchair skills to a greater extent than those who do not (Mountain et al., 2014). Other suggested strategies have included encouraging self-cueing rather than therapist-led prompting when practising transfers to and from a wheelchair (Lennon, 1991) and provision of a four-point cane to reduce postural sway in people mobilising (Laufer, 2003).
Meaning of equipment for people with stroke
Since the mid-1990s, researchers began including data on the experiences of users of equipment, often as an adjunct to other study objectives such as exploring perceptions of life after stroke (Hass et al., 1996; Mann et al., 1995). Later, the question of experiences of equipment users after stroke became a more central concern. In one of the first qualitative studies to explore the meaning of equipment use for people after stroke (n = 103), Gitlin (1998) identified six dimensions of client concerns, namely: (1) the operation of devices; (2) the utility of devices; (3) transitional perspective (equipment offering an adapted way of doing a task); (4) the learning curve associated with device use; (5) the emotional response to using a device; and (6) value dilemmas evoked by equipment. This study also suggested that perceptions of equipment could be culturally related.
Exploration of the relationship between social context and consequences of equipment use have since been expanded upon, particularly in the area of wheelchair use after stroke (Barker et al., 2004; Pettersson et al., 2007b; Rudman et al., 2006). A key finding is that people with stroke appear to rank the value and use of a piece of equipment more highly when the equipment is explicitly linked to a social interaction or occupational performance goal (Pettersson et al., 2007a; Reid et al., 2001). Ongoing use and development of measures such as the Canadian Occupational Performance Measure (Reid et al., 2001) and the Psychosocial Impact of Assistive Devices Scale (Pettersson et al., 2007a) have been discussed in the publications in this review as being useful to evaluate the personal meaningfulness of adaptive equipment.
Cost of equipment after stroke
There is little published information on the actual cost of providing adaptive equipment to people after stroke and no research was found on cost-effectiveness of equipment for people with stroke specifically. While we identified some studies that reported on the cost of equipment after stroke in individual countries, it was difficult to generalise from these studies because of differences in the value of currency between countries and over time, differences in the relative value of costs compared to local economies, and differences in the cost of this equipment compared to overall healthcare or rehabilitation costs. However, one Swedish study indicated that equipment contributed approximately 1% of total healthcare cost following stroke, with an average of 2,307 Swedish kronor (being spent per person on adaptive equipment in the first year of stroke recovery (Hass et al., 1995)). Higher costs of equipment were associated with greater disability. In a retrospective study of people discharged with equipment from a stroke unit in Germany, Hesse et al. (1996) reported that 690 European Currency Units 1 were spent per person with stroke receiving equipment. In another Swedish study, no difference was found between the cost of equipment issued on a specialist stroke ward compared to a general medical ward, and the overall cost of equipment was reported as low compared to other stroke-related costs (Gosman-Hedstrom et al., 2002a). The authors of this study concluded that health-related quality of life was lower for people who used equipment, however this was attributed to having increased dependency on others, rather than being caused by the presence of equipment (Gosman-Hedstrom and Blomstrand, 2003).
One large cross-sectional cohort study explored the cost and funding policies regarding assistive devices for 12,046 people entitled to support from Veteran's Affairs and/or Medicare in the USA (Hubbard Winkler et al., 2010a). Equipment provision varied significantly by administrative region and by disability severity (Hubbard Winkler et al., 2010b), and funding for in-home equipment alone (as opposed to funding for equipment for outside the house) did not necessarily lead to decreased costs (Hubbard Winkler et al., 2010b). This variation in equipment provision suggests that administration policies and processes have influence over provision of equipment at a clinical level. Earlier research by Hubbard et al. (2006) strongly indicated that there was inequity with wheelchair provision attributable to ethnic background, where Hispanics (OR = 1.864), African Americans (OR = 1.360) and American Indians/Asians (OR = 1.585) were more likely than Caucasians to receive standard wheelchairs, rather than powered wheelchairs or scooters. With the exception of research conducted by Hubbard Winkler et al. (2011) in recent years, the lack of high-quality evidence about the cost of equipment after stroke makes policy decisions in this area challenging, and means it is difficult to quantify the degree of unmet need (Skolarus et al., 2014).
Conflicts between equipment provision and models of stroke rehabilitation
This theme was identified in just three of the articles reviewed, but was significant in that these studies used experimental designs and include two of the four RCTs identified and included in this review. Barrett et al. (2001) examined whether encouraging people to self-propel a wheelchair in the acute phase (generally within the first month) of stroke rehabilitation risked worsening their spasticity. In their pilot RCT (n = 21 intervention group, n = 19 control group), they found that there was no evidence that early self-propelling increased spasticity. In an observational study with 25 participants, Allet et al. (2009) found that use of a standard walking stick resulted in greater walking distance on a 6 minute walking test compared to the same patient walking with a Nordic walking pole or a four-point cane.
Relatedly, in a multi-site crossover RCT with 20 non-ambulant clients undergoing mobility retraining after stroke, Tyson and Rogerson (2009) found that participants preferred to walk as soon as possible rather than work on what might be considered normal gait patterns, irrespective of the walking device used. Significant improvement in mobility was observed with all assistive devices (p > .0001–.005; effect sizes: 1.68–0.52). This finding supported the idea that the benefits of providing adaptive equipment early after stroke to increase a person's function outweighs potential disadvantages that may or may not actually exist related to impeding recovery of ‘normal’ movement patterns.
Discussion
This scoping review examined and synthesised concepts from published research on equipment provision for personal care and mobility when people have had a stroke. Broadly speaking, research to the present day has focused on estimating the frequency of equipment use and non-use (Gosman-Hedstrom et al., 2002b; Hass et al., 1995; Sorensen et al., 2003), and on exploring patient experiences of equipment provision and use (Barker et al., 2006; Gitlin, 1998; Pettersson et al., 2006), contributing to better understanding of the utility of equipment after stroke. The methods used to address research questions in this field have become ever more sophisticated, including analysis of large datasets to develop models to predict equipment use according to demographic characteristics (Hubbard Winkler et al., 2011) and the importance of the perspective of equipment users has been increasingly explored (Barker et al., 2004; Pettersson et al., 2007b; Rudman et al., 2006). An indication of the development of interest in this area is the emergence over the last 15 years of academic journals dedicated to the design and implementation of assistive technology.
Visual–spatial neglect, in particular, increases the complexity of how people interact with equipment; however, studies on this topic demonstrate that even in the presence of neglect people can learn to use adaptive equipment with adequate training. Home visits with the purpose of training in equipment use were particularly highlighted as valuable, enhancing users' understanding of equipment and improving the fit of equipment for users' needs (Chiu and Man, 2004; Skolarus et al., 2014). Learning happens best in an ecologically meaningful environment such as one's home and neighbourhood (Jones et al., 2013; Logan et al., 2004). However, findings from this scoping review indicate that most training on equipment use (reported empirically) tends to occur in hospital settings (Mountain et al., 2014; Punt et al., 2011). Although an economic analysis on the efficacy of home visits in relation to equipment provision is warranted, current research suggests that home visits (Sorensen et al., 2003) or home-based training on equipment after discharge (Chiu and Man, 2004) are beneficial.
The relationship between social context and consequences of equipment use have been a major focus of research, particularly in the area of wheelchair use after stroke. The findings of this review suggest that it may be important to relate equipment use to personally meaningful roles and occupations, which can only occur when therapists have a clear understanding of what these are from clients' perspectives. When a goal is established regarding social interaction or occupational performance, people are more likely to overcome initial negative feelings towards equipment (Pettersson et al., 2007a; Reid et al., 2001). The ambivalence that people can go through about accepting or using equipment is nuanced. Nevertheless, when health professionals pay attention to social and occupational contexts in order to recommend equipment best suited to client goals, consider the timeliness of introducing equipment, and are aware of the connection between equipment and valued social and cultural activities, use and satisfaction with equipment is likely to be enhanced.
Research findings identified in this review add clarity to the long-running debate on whether to introduce equipment early in stroke rehabilitation. Several studies have concluded that providing equipment for mobility early after stroke and during the impairment reduction phase of rehabilitation, at a minimum, does no harm (Barrett et al., 2001) and possibly improves functional gain during rehabilitation (Allet et al., 2009; Tyson and Rogerson, 2009), a position endorsed by other research (Pollock et al., 2014; Zorowitz, 2011). These findings challenge the assertion that recovery of ‘normal’ movement after stroke is preferable over achievement of functional outcomes such as speed and distance when walking, which is promoted in some approaches to rehabilitation for stroke (Pollock et al., 2014). Such approaches can explicitly advocate minimal use of equipment, based on the assumption that it may limit recovery of normal movement (Lennon et al., 2001). A tension for all rehabilitation professionals has been the issue of whether to focus therapy on retraining of physical abilities after stroke or on pursuit of functional outcomes by providing compensatory strategies, with the concern that the compensatory strategy may impede physical recovery (Ferrarello et al., 2011). Findings from this review highlight the small but growing body of evidence supporting the view that early mobilisation with equipment does not appear to be detrimental to physical recovery, and may even facilitate it. This finding suggests that therapists can have confidence using rehabilitation and compensatory strategies alongside each other in practice.
Scoping reviews are subject to the limitations of all reviews, where pertinent research may be missed during the search process, and where the conclusions of the review are dependent on the relevance and usefulness of the underlying research studies. Furthermore, as no rating of quality or risk of bias occurs in a scoping review, recommendations for practice cannot be graded (Joanna Briggs Institute, 2015). The heterogeneity of the literature in this area was unsurprising, though this feature did make comparisons difficult, meaning that decisions on synthesis were therefore narrative and pragmatic. Some populations received greater attention across studies, such as veterans (Garber et al., 2002; Hubbard Winkler et al., 2011), which may impact on the generalizability of these findings to other populations. Our review process also did not involve consultation with end-users of equipment – a recommended step to further enhance the value of review findings (Levac et al., 2010). Most research studies in this review excluded people with moderate and severe cognitive and communication difficulties, meaning that the findings may not apply to this group.
The purpose of a scoping review is to map a body of literature on a topic (Pham et al., 2014) and this review achieved that purpose. The search terms, search strategy and data extraction were conducted using an iterative and team approach, and findings have been related to policy and further research, as advocated by Levac et al. (2010). The search terms were tested and changed to ensure breadth and accuracy in the search strategy. No other review specific to equipment use and stroke was identified, and the findings, particularly about tailored training enhancing recovery after stroke and taking a pragmatic approach to when and how equipment is introduced to people, appear to be congruent with current literature on stroke rehabilitation approaches (Pollock et al., 2014).
Experimental studies are required to test emerging ideas about the best approaches to equipment prescription and use after stroke. Questions that could be addressed by such studies include assessing the impact of the preference of users on uptake of equipment and testing the extent to which contextualised training with equipment affects functional outcomes. Large, population-based surveys are also required to gather basic information on the current state of play regarding who uses adaptive equipment after stroke, at what cost and to what ends. Alongside this type of evidence, information on the environmental and occupational factors affecting equipment use is required. Based on findings from this scoping review the current research in this area would not be compatible with a systematic review approach to research synthesis at this point as there are not enough studies involving sufficiently similar and precise research questions to enable such a review. There would also be inadequate data to conduct a meta-analysis on any topic related to equipment use after stroke.
Adaptive equipment prescription can be meaningfully modelled with clinical and socio-demographic variables (such as income and ethnicity) to predict provision and use of equipment (Hubbard Winkler et al., 2010a; Jutai et al., 2007; Skolarus et al., 2014) and this approach to identifying inequities and addressing gaps is likely to continue to evolve, with electronic data management processes increasingly providing greater opportunities for this to happen. The lack of high-quality evidence about cost of equipment after stroke means that policy decisions in this area tend to be based on ideology rather than evidence. Thus, further economic analyses are recommended. Future research on how to optimise the timing and conditions for training on equipment use after stroke is also warranted, and use of outcome measures that focus on the meaning of equipment to the user may also help with furthering clinical knowledge and establishing the impact of equipment use after stroke.
Conclusion
Providing adaptive equipment early in stroke rehabilitation appears to have more advantages than disadvantages, and there are some specific techniques being developed to maximise how people with stroke receive training to use equipment. Receiving support in one's own home environment appears to encourage uptake of equipment, possibly as therapists' assessing in the home setting enables them to have a greater understanding of a client's valued roles and routines. Having a positive self-image of themselves using equipment and awareness of the social context and occupational goals of their clients were indicated in this review as possibly important influences on whether people will use equipment after stroke. It appears that providing equipment provides more opportunities during rehabilitation than not and, finally, the cost of equipment in relation to stroke care remains unclear, making it difficult to address important questions about cost-effectiveness of supplying equipment in a public health system.
Key findings
Equipment after stroke may be most useful and used when tailored to people's participation or occupational goals; More work is required to understand the best conditions to optimise equipment training; Equipment in stroke rehabilitation probably provides more advantages for recovery than disadvantages.
What the study has added
Equipment appears to promote quality of life for people after stroke when linked to participation or occupational goals. Lack of information on how equipment affects people's occupational performance, as well as cost to the health service, makes evidence based recommendations challenging.
Footnotes
Research ethics
No ethical approval was required for this study
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
This work was supported by a Publishing Bursary from the University of Otago, Postgraduate services and a University of Otago PhD scholarship grant.