
Abstract
Statement of context
Unilateral neglect is a complex impairment that is common after stroke and limits occupational performance. Sensitive assessment of unilateral neglect is critical for planning treatment and ensuring safe community discharge.
Critical reflection on practice
This reflection describes unexpected findings in the assessment of neglect with two individuals in the acute phase of recovery post-stroke. When trialing a new activity-based test battery, we observed few neglect behaviors during test tasks despite observation of multiple neglect behaviors outside of the testing situation. Upon reflection, we better understood how simplification and structuring of test items and environments could impact the observation and assessment of neglect behaviors.
Implications for practice
This practice analysis further supports the use of multiple assessments when evaluating unilateral neglect and specifically encourages the inclusion of assessment methods that maintain the complexity of everyday tasks and environments.
Statement of context
Unilateral neglect is a challenging impairment associated with stroke. The contralateral decrease or absence of attention seen in unilateral neglect can have a profound effect on occupational performance (Kortte and Hillis, 2009). Unilateral neglect often results in longer lengths of rehabilitation stay and decreased functional outcomes (Cherney et al., 2001). Understanding the nature of unilateral neglect and its impact on everyday activities is complicated by variations in the presentation of this complex impairment. Unilateral neglect can affect one or more sensory systems and/or the motor system (Plummer et al., 2003). It can present as allocentric, egocentric, or object-centered (Kerkhoff, 2001). There can also be variations in the affected space (Plummer et al., 2003) with the neglected input within the person’s body (personal), within arm’s reach (peri-personal), and/or beyond arm’s reach (extra personal). The complexity of this impairment is further reflected in the terminology that has been used over the years, with some authors using terms that emphasize the neglect of information (that is, unilateral neglect, unilateral spatial neglect, hemi-neglect) and others, the attentional aspect of the disorder (that is, hemi-inattention, inattention).
Unilateral neglect occurs after both right- and left-sided stroke; however, impairments after right-sided stroke are more common and tend to be more severe (Stone et al., 1993). Prevalence estimates vary widely from 18–23% of persons at some time post-stroke to as high as 72%, 3 days after stroke (Marshall, 2009; Stone et al., 1991). Differences in anatomical location of the underlying lesion, extent of impairment, and timing of assessment in relation to recovery are thought to contribute to the variability seen in these estimates.
While valid and reliable assessments are critical in making treatment and discharge decisions (Singh-Curry and Husain, 2010), assessing unilateral neglect can be challenging. Recently, there has been a shift from the sole use of paper/pencil tasks to considering measures that focus on functional task performance. In some instances, the functional tasks are simulated as in the behavioral inattention test (BIT) (Wilson et al., 1987), and Eschenbeck et al.’s activities of daily living (ADL) scale (Eschenbeck et al., 2010), while others, such as the Catherine Bergego scale (CBS) (Azouvi et al., 2003; Azouvi et al., 2006), use naturalistic observation. While most authors (for example, Plummer et al., 2003) recommend using multiple assessments, there is no universally agreed-upon approach. In one study, only 27% (n = 67) of occupational therapists working in stroke rehabilitation used any specific unilateral neglect assessments (Menon-Nair et al., 2007). Of the 28 assessments available at that time, only seven were being used with paper/pencil tests named as the top two choices.
Functional measures of unilateral neglect.
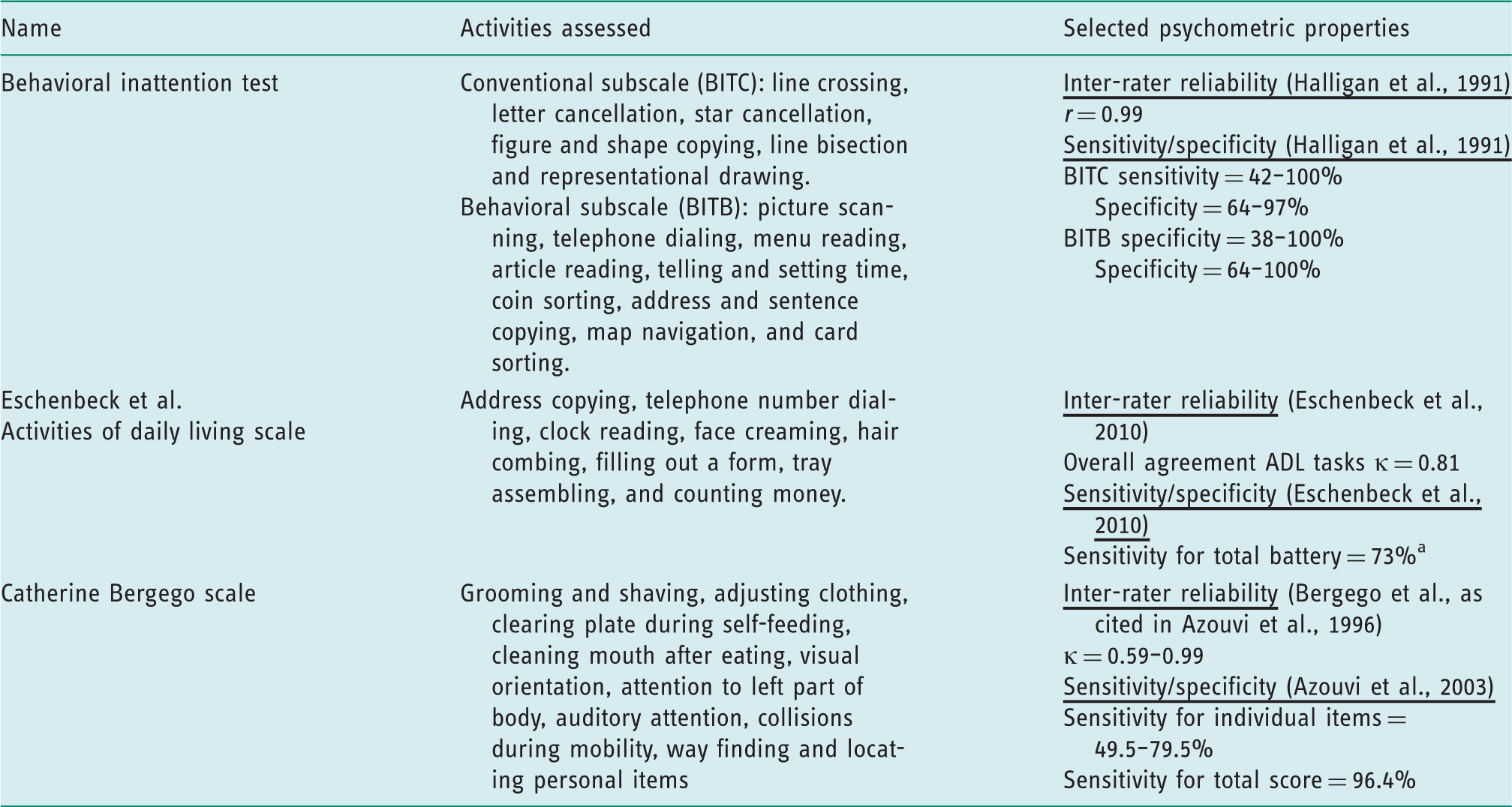
This value was derived from information presented in the article that the total battery detected 17 persons out of the 23 identified as having neglect (total sample = 68).
Critical reflection on practice
This practice analysis presents a critical reflection on the assessment of unilateral neglect following stroke. It is based on our observations of two individuals who were the sole participants in a pilot study aimed at developing measures of unilateral neglect for use in single-subject research (unpublished data). We were quite surprised by the differences between their performance during the research protocols compared to performance outside of testing. As a result, we ceased test development after these two participants and focused our efforts on exploring the reasons for the unexpected performance. Our subsequent analysis gives additional insight into possible reasons for differences in performance on various types of unilateral neglect assessments. It also highlights the importance of using occupation-based, naturalistic methods to assess the presence and extent of unilateral neglect and determine its impact on occupational performance.
Background
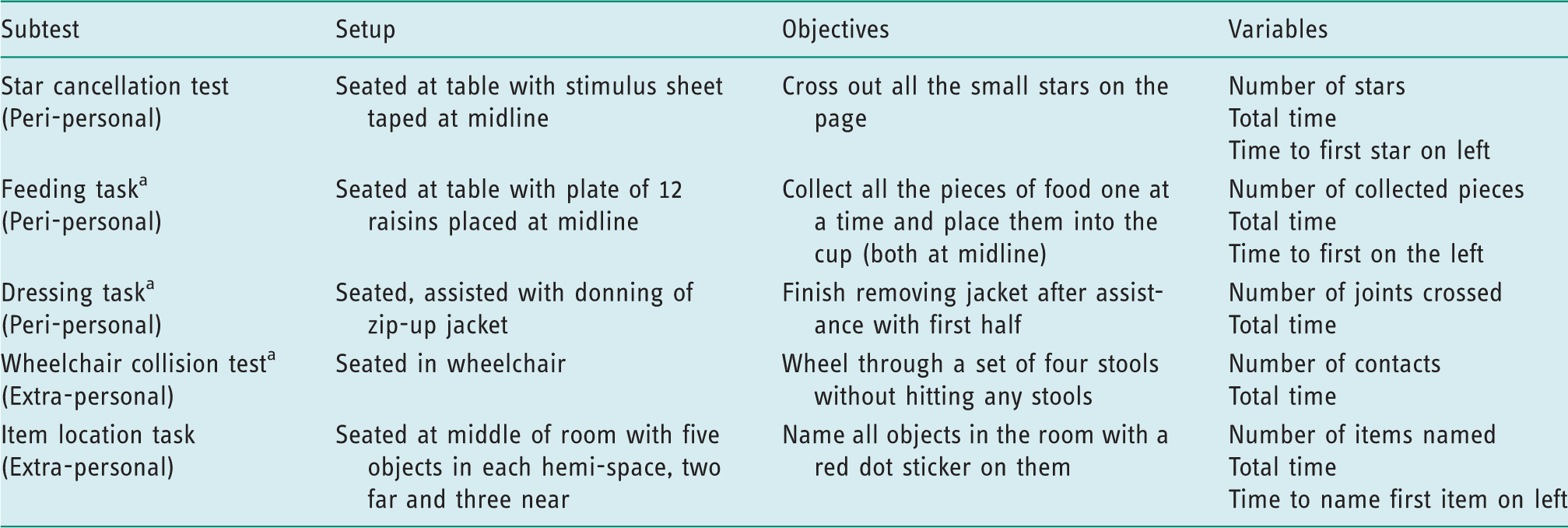
Pilot assessment battery subtests.
Summarized across all data collection points.
We developed standardized administration guidelines for the feeding, dressing, and item location tasks while tests that had previously been standardized (that is, the wheelchair collision test and the star cancellation test) were administered according to established protocols. However, we modified the feeding and dressing tasks from what are typically used in clinical settings to help ensure that factors outside of neglect did not impact a person’s performance, to ensure the safety of participants, and to allow for measurement by timing or counting. For example, we originally planned to observe the person eating a full lunch for the feeding task. However, since appetite, food preference, and fatigue could play a factor in how much and what someone eats and due to concerns about swallowing safety, we, instead, designed a simulated feeding task in which the person was instructed to pick up, bring to the mouth, and then place in a cup at midline 12 raisins evenly distributed across all four quadrants of the plate. Similarly, in the dressing task, we originally planned to observe the person completely removing his or her jacket. Yet, in order to reduce the potential impact of motor function, we decided to assist with the initial removal of the right arm from the jacket sleeve and only assess neglect during the last part of this task (that is, pulling the sleeve off the left arm).
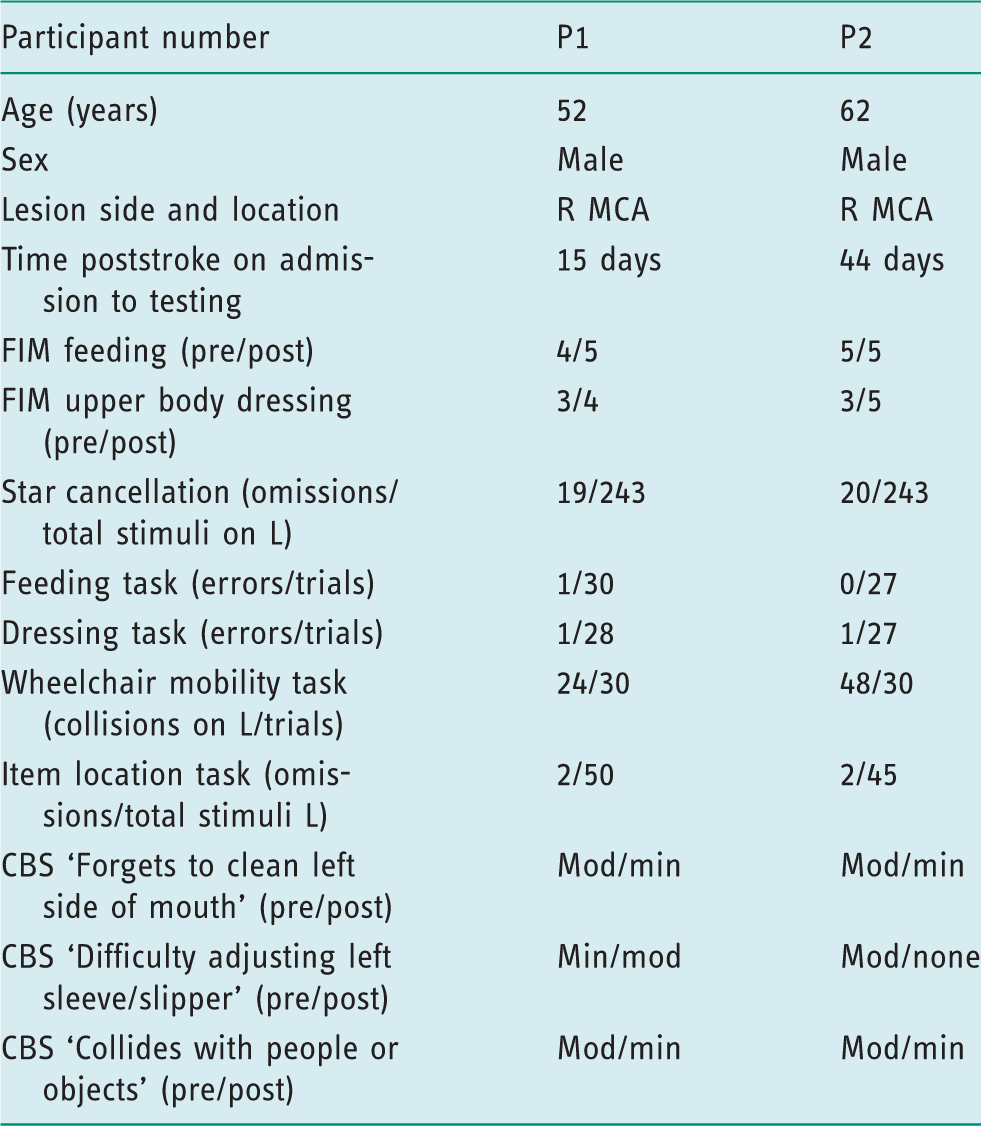
Participant characteristics and results. a
Summarized across all data collection points.
Findings
Based on our previous experience, we anticipated that individuals with unilateral neglect would miss almost all of the targets on the left or take longer to reach the left targets in all of the measures. However, despite having been identified by the rehabilitation team as having unilateral neglect based on clinical observations in order to qualify for the study, both P1 and P2 demonstrated little to no unilateral neglect on the feeding, dressing, and item location subtests and tested within the normal range on the initial star cancellation test (see Table 3). This performance was in contrast to the CBS subtest scores both before and at the end of study participation when both individuals exhibited behaviors indicative of unilateral neglect when observed performing dressing and other ADL activities on the rehabilitation unit (with the exception of P2 on the sleeve/slipper adjustment and finding food at the second time period). We also saw differences in how participants performed during and immediately before and/or after the testing situation. For example, one participant would remove the jacket from the left sleeve without difficulty, but would need verbal cueing to notice the examiner standing with the jacket on the left for the next trial. Similarly, on some trials, participants who had just completed the wheelchair collision test with few or no collisions were observed bumping into objects on the left as they left the testing area.
These unexpected findings led us to cease the development of the assessment battery and critically analyze all aspects of this experience. We wanted to understand better why the identification of unilateral neglect varied for the different measures and why performance was worse outside of the study procedures. We first considered the possible impact of motor and cognitive impairments. We ruled those out as major factors given our screening procedures and the relatively constant task demands of the assessment battery, which were designed to control for these variables.
We next considered what was different between the CBS and the tasks that we had developed. Through this reflection, we began to wonder if our simplification of the test activities might have played a critical role. We realized that we had inadvertently employed three key simplification strategies in developing the assessment tasks in order to improve reliability. We had reduced task demands by using only part of a task, decreasing the number of task elements, and limiting the space in which the task was to be completed. For example, as described above, we reduced the task demands in the dressing task by only assessing neglect during the last part of jacket removal. We had reduced the number of task elements in the feeding task by only using 12 raisins and no distractor items. In choosing the wheelchair collision test (Qiang et al., 2005) for wheelchair mobility, we had limited the space that was available to maneuver a wheelchair as per the assessment protocol. On reflection, we realized that the steps we took to simplify the tasks likely resulted in fewer visual stimuli (including competing stimuli on the ipsilesional side) when compared to the non-test environments and the more naturalistic assessment of the CBS, thus possibly leading to improved performance on our test battery.
In addition to simplification, it was also noted that we provided a substantial amount of structure through the administration procedures. Our standardized administration guidelines had resulted in each task having a clear beginning and end, with participants given highly specific directions each time the task was performed. We also specifically structured the testing environment to decrease distractions during testing sessions by scheduling the assessment when activity in the rehabilitation gym was minimal and not speaking to participants while they were performing the tasks. These structural elements, which are typical of most standardized procedures and assessments, may have made it possible for participants to utilize potentially preserved top-down attentional networks better, which possibly allowed them to perform better on our measures than on the CBS as well as outside the direct test environment.
Our reflections regarding the impact of simplification and structure in neglect assessment have support in the neuroscience literature. For example, when evaluating performance on peri-personal search tasks, it has been found that individuals with neglect perform better when fewer search stimuli are present or when stimuli have been arranged in an organized pattern (Gorgoraptis and Husain, 2011; Weintraub and Mesulam, 1988). In addition, there have been recent studies from neuropsychology in which dual task computer-based assessments (that is, increased task demands) have been shown to be more sensitive indicators of neglect, especially in persons whose neglect was not detected by standard paper/pencil tests (Bonato, 2012). Furthermore, Duncan et al. (1999) found that during targeted, search tasks persons with unilateral neglect performed similarly to controls, suggesting a preservation of top-down attentional control under certain testing parameters.
Our observations support previous work on the variable nature of unilateral neglect and how people may be able to compensate for their impairment in controlled testing environments. These findings provide additional support for the use of occupation-based naturalistic observation in unilateral neglect assessment. It is possible that tools such as the CBS have greater ecological value than paper/pencil tasks or those assessments that use simulated functional activities, with the demands present during naturalistic assessment more consistent with those that occur in daily occupations at home or in the community. Furthermore, it is possible that individuals are able to compensate more effectively on paper/pencil and simulated functional tasks out of context or that the task demands in these assessments may not be great enough to elicit unilateral neglect behaviors (Bonato, 2012). However, these possibilities should be considered with caution as this practice analysis is based on two patients, both of whom were in the acute stage of recovery and had moderate neglect. Stroke survivors in a more chronic phase of recovery, as well as those with milder or more severe neglect, may show different patterns of performance during assessments. In addition, while screenings were in place to reduce the potential effect of confounding factors, it is not possible to rule out completely the full impact of other impairments on performance.
Summary
In order to ensure accurate identification of those persons with unilateral neglect and determine the effect of remedial and compensatory interventions and recovery over time, it is important for occupational therapists and others to consider incorporating tools that assess performance through occupation-based naturalistic observation (Chen et al., 2012). While this type of assessment approach is in keeping with current thinking in occupational therapy, it will require that clinicians develop experience and confidence in these approaches in order to move beyond the long-standing reliance on paper/pencil tests (Menon-Nair et al., 2007). Similar considerations related to structure and complexity may also apply to the treatment of unilateral neglect with compensatory strategies practised in a structured, supportive hospital setting perhaps not generalizing when patients return to more complex, natural environments. Finally, when reviewing the literature, clinicians and researchers should consider how participants are screened for inclusion in studies with the use of multiple measures likely indicating a broader range of impairment than those studies that rely solely on paper/pencil assessments to identify participants. Our ability to measure this complex and variable condition accurately in the context of occupations is important, both for identifying appropriate interventions, as well as being able to prepare patients with unilateral neglect for safe discharge to the community.
Key findings
Unilateral neglect assessments using simple structured tasks may not identify neglect-related challenges in everyday occupations. Assessments based on skilled observations of performance in occupations within ecologically (contextually and environmentally) relevant settings may better support effective intervention and safe community discharge.
Footnotes
Acknowledgments
The authors would like to thank Drs Deborah Kartin and Sarah W. McCoy for their support in the design of the initial study and Ms Elizabeth K. Wise an occupational therapist who assisted in the participant recruitment and data collection.
Dr Donoso Brown completed data collection for this project while she was a doctoral student at the University of Washington.
Research ethics
This investigation received review and approval from the University of Washington Human Subjects Division. The project number was 37391, 2010. The institutional review board has closed the monitoring of this study as all remaining data are de-identified. All participants provided written informed consent.
Declaration of conflicting interests
The authors confirm that there are no conflicts of interest.
Funding
This investigation was supported as part of a training grant that Dr Donoso Brown held while she was a doctoral student at the University of Washington. NIH, NICHD (NCMRR: 5T32HD007424).