
Abstract
Introduction
Dementia affects cognitive functions and has a direct impact on the ability to perform activities of daily living. Studies have focused on the impact of cognition-focused interventions on cognitive functions, but less on the daily functionality of people with dementia. The aim of this study was to review systematically evidence of the effectiveness of cognition-focused interventions on the ability of people with dementia to perform activities of daily living.
Method
A search of randomised controlled trials was performed in 10 databases to find all available evidence on the subject. Two reviewers independently selected articles based on predetermined inclusion criteria. The articles had to describe randomised controlled trials involving cognition-focused interventions in people with some form of dementia, aged 65 years or over, and specify their score on the Mini-Mental State Examination or the Clinical Dementia Rating. Eleven articles met the inclusion criteria for the review.
Results
Cognitive rehabilitation through functional tasks led to maintenance or improvement in everyday tasks in some cases. In cognitive stimulation studies the subjects maintained their performance in activities of daily living with respect to the control condition, but this was not the case in reminiscence stimulation groups. Subjects who underwent cognitive training of cognitive functions did not show significant improvements in activities of daily living.
Conclusion
The evidence on the effectiveness of cognition-focused interventions suggests that multi-component programmes that include cognitive rehabilitation or cognitive stimulation could maintain or improve functionality in people with dementia.
Introduction
Dementia is a syndrome that involves the progressive loss of cognitive functions in one or more cognitive domains: complex attention, executive functions, learning and memory, language, perceptual-motor ability and social cognition. These cognitive deficits affect the ability to perform daily tasks, emotional control and social behaviour (McKhann et al., 2011).
Worldwide epidemiological studies indicate that 47.5 million people have dementia, and there are 7.7 million new cases every year. It is estimated that this number will progressively increase to reach 75.6 million people with dementia in 2030 (Prince et al., 2015).
Cognitive functions are required to plan, manage and execute daily tasks satisfactorily. There is a clear relationship between the degree of cognitive impairment and loss of functional abilities related to daily activities, which interferes directly with the autonomy of the person with dementia (Fuentes, 2008; Helvik et al., 2015; Rockwood and Middleton, 2007). Involvement in tasks is essential to enable older adults to remain autonomous in the community (Baum, 1995). When autonomy in activities of daily living (ADL) declines, people with dementia must rely on others to perform these tasks, which increases their risk of institutionalisation (Brodaty et al., 2014). ADL are defined as the activities required to take care of one’s own body. These include basic ADL (BADL), which are basic individual tasks related to caring for your body, and instrumental ADL (IADL), which are activities of daily life at home and in the community (Liu et al., 2007).
Traditionally, drug therapy has been used to improve cognitive and behavioural symptoms in people with dementia and to slow and stabilise the impairment (Chen et al., 2014; Di Santo et al., 2014; Gauthier and Molinuevo, 2013). Some studies show that patient benefits could be increased when interventions combine pharmacological and non-pharmacological methods as complementary approaches (Chapman et al., 2004; Onder et al., 2005). The earliest reference to non-pharmacological interventions that we could find was a case study by Taulbee and Folsom (1966). They showed that changing the environment or facilitating temporary space orientation in a hospital could improve the behaviour and cognitive functions of people with dementia. Since then, non-pharmacological therapies (NPTs) have been used mainly to improve cognition, but have also been reported to improve quality of life, and in some cases the performance of daily living activities (Olazarán et al., 2010).
NPTs include cognition-focused interventions (C-FI) which are centred on cognitive tasks (Bahar-Fuchs et al., 2013), and can be grouped into three categories as follows (Choi and Twamley, 2013; Clare and Woods, 2004; Kim, 2015; Spector et al., 2012; Woods B et al., 2012):
Cognitive stimulation (CS): engagement in activities designed to improve general cognitive performance and social functioning, involving the person in tasks that stimulate mental activity (activities or discussion, usually in a group).
Cognitive training (CT): guided practice of standard tasks to practise specific cognitive functions such as memory, attention, reasoning or executive functions (that is, focused on cognitive functions like crossing out a specific letter from a text to stimulate the person’s attention). A range of difficulty levels may be available. Practice in isolation of any specific cognitive skill has the potential to improve or maintain performance in a specific domain. Tasks may be performed using paper and pencil, computers or other media, and exercises for specific cognitive domains are repeated. This technique can be combined with psychoeducation and strategy training (activities may be offered in individual or group sessions).
Cognitive rehabilitation (CR): an individualised approach focused on reducing functional decline and maximising social participation and performance in ADL. This approach focuses on improving daily functioning through compensatory or restorative strategies, rather than on cognitive tests. Cognitive rehabilitation tends to be used in real-world settings, and benefits may be generalised to other settings. It is important to understand these terms, because they have sometimes been used interchangeably.
Previous reviews have specifically examined the effectiveness of C-FI trials in people with dementia. In particular, they have focused on the CS approach, and reported benefits in cognition and in wellbeing and quality of life (Aguirre et al., 2013; Cooper et al., 2012; Woods B et al., 2012; Yuill and Hollis, 2011). A systematic review focused on the benefits of non-pharmacological interventions (Olazarán et al., 2010) reported positive results in some studies on ADL performance. However, this review did not specifically assess evidence of benefits of NPTs that target ADL performance.
In general, there is a significant lack of studies assessing performance in daily activities compared with the number of studies on cognition or quality of life benefits (Cooper et al., 2012; Woods B et al., 2012). There is controversy about the benefits of C-FI on the ability to perform ADL. Some authors have found improvement (Aguirre et al., 2013; Olazarán et al., 2010), whilst others have found no benefits (Kim, 2015; Letts et al., 2011; Miranda-Castillo et al., 2013).
This systematic review aimed to identify and analyse the available evidence regarding C-FI benefits on functional abilities in people with dementia.
Method
PRISMA guidelines methodology (Moher et al., 2009) was followed to conduct the systematic review. All of the trials included were also critically assessed using the 11-item PEDro scale (De Morton, 2009; Maher et al., 2003).
Literature search
Ten databases were consulted: PubMed, Web of Science, Scopus, PsycINFO, CENTRAL (Cochrane), SciELO, LILACS OTseeker, CINHAL and ALOIS. The search was performed between November 2014 and March 2015. The keywords used in the search strategy were (free term and MeSH), ‘cognitive therapy’ OR ‘cognitive training’ OR ‘cognitive stimulation’ OR ‘cognitive rehabilitation’ OR ‘memory therapy’; AND ‘activities of daily living’; AND ‘dementia’. The title and summary of a total of 3442 articles were reviewed to confirm that they met the predetermined inclusion criteria. In these articles, the Mendeley reference manager was used to look for duplicated items. To attain additional eligible articles, reference lists of the selected studies were also checked.
Selection criteria
Only randomised controlled trials (RCTs) published in peer-reviewed journals and written in Spanish or English were included in the study. Study protocols were not included.
Participants
Participants had a clinical diagnosis of dementia according to DSM-IV criteria, including Alzheimer’s disease, mild to moderate dementia, mixed dementia, vascular dementia or mild cognitive impairment. Studies reported the Mini-Mental State Examination (MMSE) or the Clinical Dementia Rating (CDR) score. Participants were older than 65 years. Participants were either living in the community or in residential care centres.
Types of interventions
The experimental group (EG) had to perform one of the C-FI approaches described above. Studies using new technologies such as CS interventions were dismissed, because the method was different from conventional C-FI. The EG and a control group (CG) were compared.
Types of outcome measures
Studies had to assess functionality in ADL.
Quality assessment
All of the trials were critically assessed using the 11-item PEDro scale (De Morton, 2009; Maher et al., 2003). This tool is used to determine the rigour of clinical trials. The final score is the sum of all the items. A study was designated ‘high quality’ if it scored 10 to 6, ‘fair quality’ if it scored 4 to 5, and ‘poor quality’ if it scored 3 to 0. Only trials with ‘high’ or ‘fair’ quality scores were included in the review. If the RCT met all the following criteria it was considered high quality: randomisation, blinding (allocation, subjects, therapists and assessors), similar groups at baseline, application of intention-to-treat principles, between-groups statistical comparison and provision of point measures.
Quality assessment scores (PEDro scale).
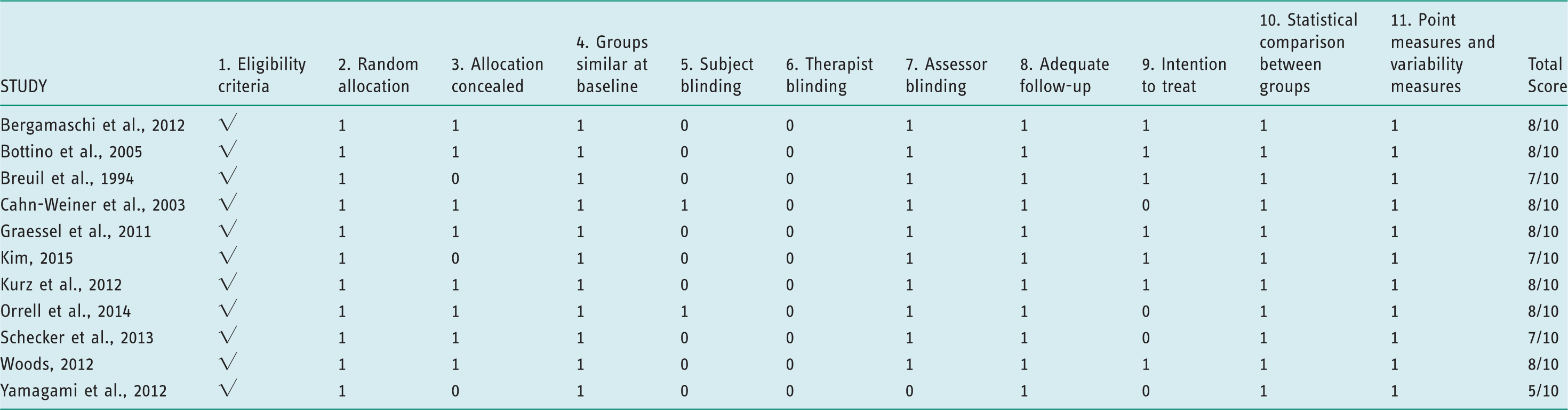
1. Elegibility criteria were specified; 2. Subjects were randomly allocated to groups; 3. Allocation was concealed; 4. The groups were similar at baseline; 5. There was blinding of all subjects; 6. There was blinding of all therapists who administered the therapy; 7. There was blinding of all assessors who measured at least one key outcome; 8. Measures were obtained from more than 85% of the subjects initially allocated to groups; 9. All subjects data for at least one key outcome was analysed by ‘intention to treat’; 10. The results of between-group statistical comparisons are reported; 11. The study provides both point measures and measures of variability.
√ yes (not scored) high quality = PEDro score 6–10
1 yes (scored) fair quality = PEDro score 4–5
0 no poor quality = PEDro score ≤3
Data extraction
Descriptive characteristics (age, sex, education, cognitive level assessed with MMSE, and place of living), source (authors, year), participants, study design, methods (such as time of intervention) and sample were extracted. The study description and intervention results that were gathered were the study objectives, intervention type, control condition, outcome measures to evaluate the ability to carry out ADL, results, conclusions and limitations of the study.
Results
Study selection
The initial screening was conducted by two reviewers. They screened titles and abstracts against the inclusion criteria to identify potentially relevant studies. Disagreements in the screening were resolved by a third reviewer. A total of 158 relevant abstracts were selected in this first step. Records that were out of scope were then excluded, which left 36 studies. The full papers of these studies were obtained, and the two reviewers independently assessed their eligibility. Twenty-five studies were excluded in this step, which left a total of 11 studies that met the inclusion criteria and were included in the review (see Figure 1, PRISMA flow diagram).
PRISMA flow diagram of articles identified (based on Moher et al., 2009).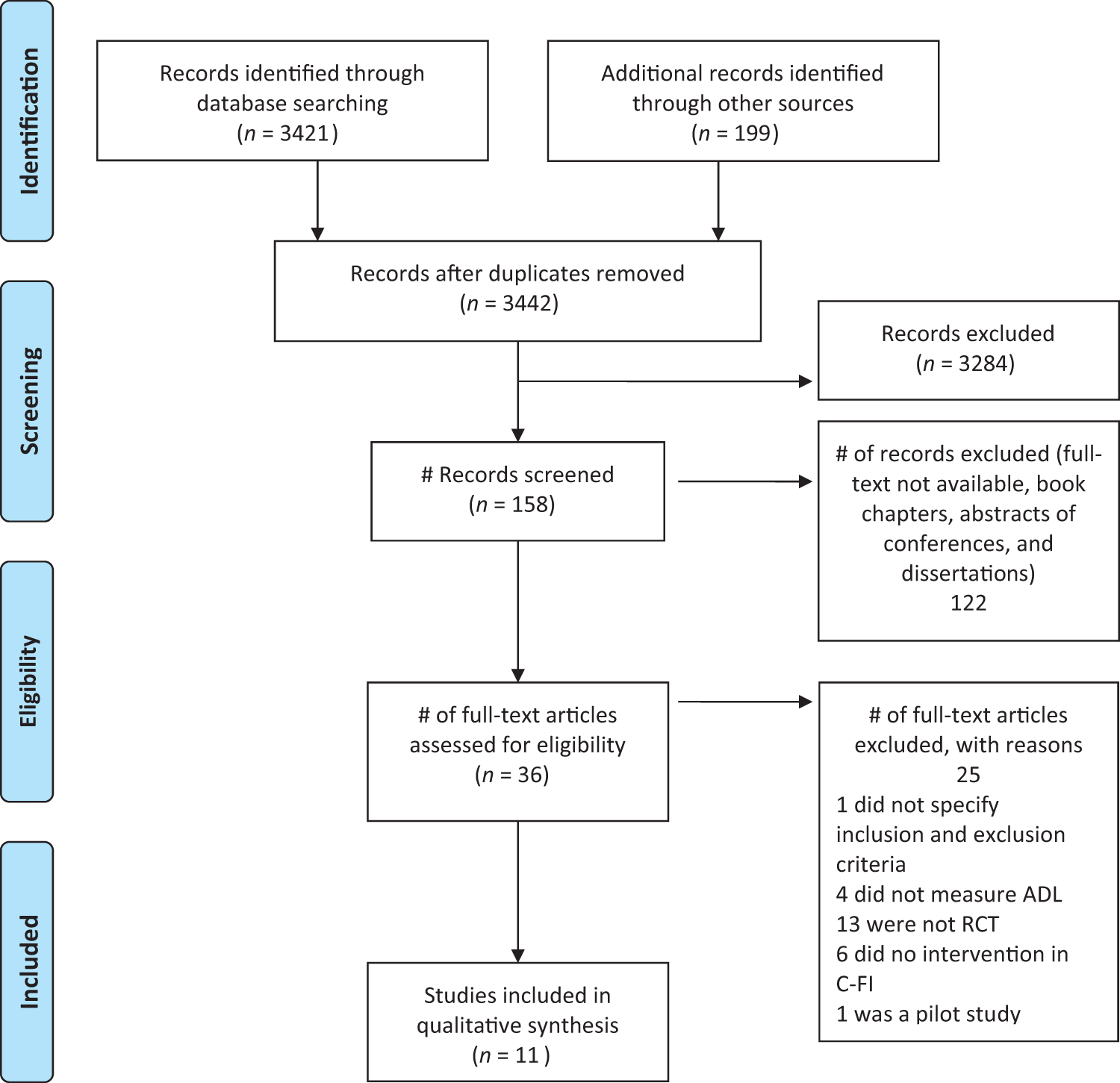
Paper characteristics
Summary of included studies.

CG: Control Group; IG: Intervention Group; C-FI: Cognition-Focused Intervention; CT: Cognitive Training; CS: Cognitive Stimulation; CR: Cognitive Rehabilitation. AChE-I: Acetylcholinesterase inhibitor; ADL: Activities of Daily Living; AD: Alzheimer disease; MMSE: Mini-Mental State Examination; RCT: Randomised Controlled Trial; CDR: Clinical Dementia Rating; ECA: Échelle Comportamentale Adaptative; E-ADL test: Erlangen Test of ADL; AFIB: Aachen Functional Item Inventory; Bayer ADL: Bayer Activities of Daily Living; MOSES: Multidimensional Observation scale for Elderly Subjects; COPM: Canadian Occupational Performance Measure; MBI: Modified Barthel Index.
Intervention characteristics
Nine studies used group interventions (Bergamaschi et al., 2013; Bottino et al., 2005; Breuil et al., 1994; Cahn-Weiner et al., 2003; Graessel et al., 2011; Orrell et al., 2014; Schecker et al., 2013; Woods RT et al., 2012; Yamagami et al., 2012). One study was organised into thematic modules and based on individual interventions (Kurz et al., 2012). Only one study combined group and individual interventions (Kim, 2015).
The intervention time in the C-FI studies ranged from a minimum of five weeks (Breuil et al., 1994) to a maximum of 12 months (Graessel et al., 2011). The intensity (hours per session) and frequency (times a week) of interventions ranged widely from 45 (Orrell et al., 2014 ) to 120 minutes (Bergamaschi et al., 2012; Graessel et al., 2011) and from once a week (Bottino et al., 2005; Cahn-Weiner et al., 2003; Kim, 2015; Orrell, 2014; Woods RT et al., 2012) to six sessions per week (Graessel et al., 2011).
Outcome measures
The measures used in the studies were the Activities of Daily Living Scale (ADLS) (Bergamaschi et al., 2013; Bottino et al., 2005; Cahn-Weiner et al., 2003), the Adaptive Behavior Échelle (ECA) (Breuil et al., 1994), the Erlangen Test of ADL (E-ADL test) (Graessel et al., 2011), the Instrumental ADL Scale (IADL) (Bergamaschi et al., 2013), the Multidimensional Observation Scale for Elderly Subjects (MOSES), specifically the Self-Care Scale (Yamagami et al., 2012), the Bristol ADL Scale (Woods RT et al., 2012) and the Alzheimer’s Disease Cooperative Study-ADL (ADCS-ADL) (Orrell et al., 2014). From all these measures described, the most frequently used to assess the functionality was the ADLS, which was applied in three studies (Bergamaschi et al., 2013; Bottino et al., 2005; Cahn-Weiner et al., 2003).
Some trials used more than one scale. For instance, the Bayer ADL (B-ADL) was used with the Aachen Functional Item Inventory (AFIB) (Kurz et al., 2012). Another study combined the Barthel Index (BI), the IADL, the B-ADL and the ADL and IADL subscales of the Nosger scale (Schecker et al., 2013), whereas Kim (2015) used the Canadian Occupational Performance Measure (COPM) combined with the modified BI (MBI).
Summary of cognition-focused interventions on ADL
Cognitive training
In a comparison of a five-week CS programme, which used paper and pencil tasks, and a CG that did not undergo stimulation, the researchers found no significant improvements in ADL, tested with the ADLS (Breuil et al., 1994). Another study used a specific CT programme, through the practice of mnemonic strategies (organisation of stimuli into significant categories, organisation of ideas to recall information from daily tasks, and visualisation and association of items to remember). A weekly session was conducted for six weeks. The CG only received educational information on ageing and dementia. In this study, neither group reported significant changes in the ADL questionnaire (Cahn-Weiner et al., 2003). A study with one year of training using paper and pencil tasks (stimulation of spatial orientation, memory, attention, perception and visual analysis, as well as recognition of emotional expressions), compared with a CG that did not perform CT-specific tasks, showed no significant differences in the IADL test in the post-intervention period. One ADL test showed a decline in ADL performance in the CG compared with the EG (Bergamaschi et al., 2013).
Cognitive stimulation
In a multicentric study, cognitive functions were stimulated in structured sessions in which a specific topic or activity was discussed (daily tasks, life history and puns). Orientation activities based on time and space information were also performed, and subjects were reminded of the previous sessions. The CG followed the usual treatment, which varied according to the centre. Participants in the EG improved slightly in the ADCS-ADL test after three months of intervention (a very small standardised difference) (Orrell et al., 2014).
Another study established two EGs with different interventions carried out over six months (Schecker et al., 2013). The first intervention group performed a training CS programme that involved both working memory and processing speed tasks. The second EG intervention focused on metacognitive training through the use of self. In this focus group, personal issues were brought up to stimulate discussion with users (for example, sex before marriage or having children at an advanced age). The non-intervention group only followed the usual drug treatment. Both EGs showed better results than the CG. Significant improvements in functionality were observed in the group that trained working memory and executive processes by CS. This group obtained better results in the BI and IADL than the focus group.
Cognitive stimulation through reminiscence
In one multicentre study, reminiscence was used as a CS tool for people with dementia and their carers. The CG followed the same treatment as usual. ADL benefits were not obtained, and the BADLS did not report significant differences in any group (Woods RT et al., 2012). However, another 12-week trial that used brain-activating rehabilitation, a sort of CS programme that combined reality orientation techniques with reminiscence of everyday events that were significant to the subject, showed that the intervention group maintained daily life functions in ADL compared with the non-intervention that did not participate in an intervention. The intervention group had lower scores than the CG after the intervention, as measured on the self-care subscale of MOSES (Yamagami et al., 2012).
Cognitive rehabilitation in multi-component programmes
A five-month CR programme was designed that consisted of reality simulation sessions of simple daily activities (making a purchase in a supermarket or writing a message to someone); advice on the use of external aids for memory deficits (such as diaries and calendars); training caregivers on verbal instructions; and support sessions to prevent stress in users. The CG had regular appointments with their doctors to follow-up the pharmacological treatment and answer caregivers’ questions about patient management. Improvements in ADL test score were obtained in the EG, but not in the CG (Bottino et al., 2005).
A second study organised multi-component group therapy into three categories: motor stimulation (bowling and croquet); CR through ADL performance (preparing a snack, creative tasks or gardening) and CT (paper and pencil tasks). The non-intervention group followed the usual treatment (CT, exercise, cooking groups, among others). After intervention for six days per week for a year, the intervention group managed to maintain functional abilities (the scores remained unchanged), whereas the CG showed a decrease in the E-ADL test score (Graessel et al., 2011).
A third multicentric study focused on an individual intervention that lasted 12 weeks and was based on CR and cognitive behavioural therapy. This intervention consisted of a programme of thematic modules based on a neurorehabilitation (external memory aids and introduction to daily routines) and psychotherapy approach (daily structure, planning activities and reminiscence). The CG continued with the standard drug therapy. No statistically significant differences in ADL were obtained in any group, but the B-ADL scores declined slightly in both groups after the intervention (Kurz et al., 2012).
One of the studies was designed to investigate the effect of CR on the performance of ADL in people with mild dementia. It used individual sessions focused on significant targets for the person with dementia, offering strategies and support to manage stress and improve performance during activities. In addition, group sessions were conducted with reality orientation techniques, CT, paper and pencil tasks and training in the use of external aids (timing and agenda). The CG only participated in unstructured conversations and watched health-related videos. After eight weeks of intervention, there were improvements in COPM performance and satisfaction ratings in the EG, but no significant differences were observed in MBI scores after the intervention in any group (Kim, 2015).
Discussion
This review is focused on the effects of C-FI on functional capabilities, which deteriorate considerably in people with dementia.
In total, 11 RCTs with 1259 participants (667 in the EG, 592 in the CG), met the inclusion criteria for the review. Previous reviews reporting the benefits of CS programmes showed significant positive effects on cognition. Therefore, this approach is strongly recommended in people with dementia (Aguirre et al., 2013; Woods B et al., 2012; Yuill and Hollis, 2011). In the World Alzheimer Report, Prince et al. (2015) reported the strongest evidence of the impact of CS interventions on cognition. This review suggests that short-term improvements in cognitive functions could be produced or cognitive decline could be reduced in people with dementia, which would also improve wellbeing and quality of life. However, there is a lack of evidence of C-FI benefits on functional performance. The present review provides a comprehensive appraisal of C-FI effectiveness for ADL performance in people with dementia, and also provides evidence of the benefits of C-FI approaches. Olazarán et al. (2010) described NPTs and their benefits in different areas in people with dementia. This review reported positive results of NPTs on performance in daily activities, but not all the interventions were specifically C-FI, and the review was not focused on functionality benefits specifically. The present review provides evidence of the benefits of CS groups (for example: training working memory, daily tasks topics, reminiscence about everyday materials) in maintaining ADL performance. Moreover, multi-component programmes of CR that use functional tasks reported maintenance or improvement of functional abilities if simulation of daily tasks was used or external aids were offered. Training on external aids in isolation was not associated with ADL benefits. Activities in these approaches that were associated with ADL maintenance or improvement included some of the following tasks: simulated daily tasks, training compensatory strategies or external aids for ADL, reminiscence about or recognition of everyday tasks, and involvement of CT tasks (Bottino et al., 2005; Graessel et al., 2011; Kim, 2015; Orrell et al., 2014; Schecker et al., 2013; Yamagami et al., 2012). However, in the present review isolated CT interventions did not show any benefits related to functionality. This finding is consistent with the World Alzheimer Report (Prince et al., 2011), which suggests that CT is not effective in cognitive function or subjective memory. Also Clare et al. (2004) did not provide evidence supporting the use of CT interventions.
The outcome measures used to assess the ability to perform ADLs differed across the studies. Therefore, it is difficult to determine which functional assessment tool should be used.
There is no evidence on the optimal length of interventions, as there was great variability between the trials. Most studies conducted interventions for less than six months, with an average of one or two sessions per week. The relationship between application time and the benefits of therapy is not clear. However, the longest studies showed that ADL were maintained in the EG with respect to the CG (Bergamaschi et al., 2012; Graessel et al., 2011).
The only study that used individual intervention (Kurz et al., 2012) did not show an improvement in the participants’ ability to perform ADL. However, the study that combined a group and individual approach showed enhanced performance and satisfaction in ADL when measured with COPM, but did not report significant differences in MBI (Kim, 2015). The rest of the studies used group interventions and obtained different functionality results.
Some studies were not included in this review because they did not meet the inclusion criteria, although the results showed improvements in the ability to perform ADL. As in the study by Graessel et al. (2011), Ávila et al. (2004) used a C-FI programme in people at a moderate stage of Alzheimer’s disease. They implemented a multi-component programme with motor training, CT and ADL training (CR). A support group was organised for caregivers to reduce stress. They found a significant improvement in functionality. However, this study had some methodological limitations: no CG and small sample size. In a study published by Farina et al. (2002), ADL training was provided to stimulate procedural memory (as a CR approach) related to the performance of a previously learned activity. Benefits resulted in the ability to perform daily tasks. These findings are consistent with other studies in which training was provided based on the principle of procedural memory stimulation (Zanetti et al., 1997). In this review, the studies that used CR to stimulate ADL as a C-FI also reported positive functionality results (Bottino et al., 2005; Graessel et al., 2011; Kim, 2015; Kurz et al., 2012).
Regarding the limitations of the present review, the samples in most studies were small, which made them unrepresentative. There was no consensus on appropriate ADL assessment tools. None of the studies considered the application of personalised activities adapted to the needs of every individual. Not all studies took into consideration the participation of the family in the intervention, although it would be important to practise learned strategies at home (Bottino et al., 2005; Kurz et al., 2012). Some studies only compared the experimental condition with the non-training control.
The team that has carried out this work includes people from different disciplines and although not all members are experts in the subject of the review, they are all involved in healthcare-related work. We view this as a strength in our team, since it provides a multidisciplinary aspect to our work, bringing together many viewpoints.
It is important to note that the classification of the studies into the different categories was made under the consensus of different team members. It is possible that there was a bias in this classification if the study interventions have not been well described.
Implications for the practice of occupational therapy
The present review has some implications for occupational therapy practice, in terms of C-FI best practice. Multi-component C-FI should be developed combining CS and CR techniques, not only cognitive programmes that involve CT (stimulation of cognitive functions in isolation). Furthermore, the provision of compensatory strategies and external aids, such as a CR tool, seems to reduce difficulties in everyday tasks (Olazarán et al., 2010). These recommendations appear to maintain and even improve functionality in the daily life of people with dementia, reduce caregivers’ stress (Chew et al., 2015) and even cut the economic costs of associated care (Knapp et al., 2006).
Conclusion
The findings suggest that multi-component C-FI programmes that include CR through functional tasks and some kinds of CS interventions are promising for maintaining or improving ADL performance in people with dementia. Functional skill training through functional tasks has shown some promising functionality results, and can be generalised to other settings. The studies included in this review do not provide evidence of the benefits of CT on performance in ADL.
Further research is needed to develop cognition-focused interventions to improve and maintain the ADL performance of people with dementia, as well as studies to assess the effect of individualised CR interventions at home. In addition, it may be necessary to develop a sensitive evaluation tool to assess functionality performance. There is also a need for awareness about optimum interventions in terms of length, frequency, type of C-FI, and differences between the clinical and home setting.
Key findings
Multi-component cognition-focused intervention programmes have a positive effect, as they can improve or maintain functional capabilities. The effects of the therapy are significant when cognitive interventions use directly functional tasks through everyday activities.
What the study has added
This review suggests that C-FI based on CR or CS may help to preserve cognitive functions and obtain optimum levels of participation in daily activities.
Footnotes
Acknowledgements
The authors thank Rosa M. Piqué and M. Àngels Pujols, librarians of the Escola Universitària d’Infermeria i Teràpia Ocupacional de Terrassa, Universitat Autònoma de Barcelona, for facilitating access to articles.
Research ethics
Ethical approval was not required for this research.
Declaration of conflicting of interests
The authors confirm that there is no conflict of interest.
Funding
This research received no specific grant support from any funding agency in the public, commercial, or not-for-profit sectors.