
Abstract
Introduction
Anxiety is a common non-motor symptom of Parkinson’s and is an important consideration for occupational therapists working with this population. Little is known about how people with Parkinson’s experience anxiety. A pragmatic inquiry framework and inductive approach were used to perform a patient and public consultation round to inform future occupational therapy research exploring anxiety in people with Parkinson’s.
Method
Seven telephone and two Skype interviews were conducted with people with Parkinson’s, who were accessed and recruited through the charity Parkinson’s UK. They were selected on the basis of their previous experience and training to participate in a consultation exercise. Thematic analysis was used to develop codes using an inductive approach.
Findings
Three key themes emerged: experiences of anxiety in Parkinson’s; coping with anxiety in Parkinson’s; and considerations for future research. These include timing with regards to medication ‘wearing-off’ phenomena, easy access to medications, and providing a safe, sensitive research environment. Occupational therapists need to take these findings into account when designing intervention studies.
Conclusion
This patient and public involvement consultation round proved valuable and the participants’ contributions will directly improve the design of future occupational therapy research exploring the lived experience of anxiety for people with Parkinson’s.
Introduction
Occupational therapists working with people with Parkinson’s (PWPs) often encounter anxiety, which acts as a barrier towards effective treatment. Developing an intervention that takes into account a condition with several interacting components requires a rigorous scientific process as outlined by the Medical Research Council guidance for developing complex interventions (Craig et al., 2008). Beginning the journey towards developing a more holistic, complex intervention for PWPs experiencing anxiety, it is crucial to lay a strong scientific foundation. Putting the experiences of PWPs at the centre of such a process ensures future work to develop the intervention is less influenced by researcher or healthcare professional assumptions. Occupational therapists are ideally placed to fulfil this role, with holism and person-centred practice being central concepts of the profession’s philosophy.
Patient and public involvement
Patient and public involvement (PPI) in research has been shown to have positive benefits in terms of participant recruitment, feasibility, study design, and dissemination of findings (Whitstock, 2003). It has been stated that PPI provides a cornerstone to a truly patient-led national health service (NHS) in the United Kingdom (UK) (Hogg, 2007). Patient and public contributions can provide alternate views from those of researchers and the workforce (NIHR, 2014). Those involved are able to form judgements and recommendations based on experiences of their condition. They may have differing aims and opinions about health which researchers and healthcare professionals have not considered (NIHR, 2014; Whitstock, 2003). As well as increasing representation and equity in public services, PPI contributes towards health services that are more accessible and acceptable to the public (Hogg, 2007). Improvements in the overall quality and relevance of health research have also been highlighted, as well as a perception of increased patient acceptance of research findings (Whitstock, 2003). However, there is a view that the impact of PPI in individual projects is weak and supported by methodologically poor research (Staniszewska et al., 2008). Despite this, service users involved in PPI report increased feelings of empowerment and value (Brett et al., 2014), which echoes the philosophical underpinnings of occupational therapy. Research funders, such as the National Institute for Health Research (NIHR) in the UK, now consider PPI an essential requirement of funding applications (NIHR, 2014).
Literature review
In the UK there are approximately 127,000 people with Parkinson’s (Parkinson’s UK, 2014), and 98.6% experience non-motor symptoms that can be defined as a collection of neuropsychiatric symptoms specifically linked with Parkinson’s (Barone et al., 2009). These can include gastrointestinal issues, cognitive problems, and mental health issues (Barone et al., 2009). Of those people experiencing these non-motor symptoms, 43–56% live with stress and anxiety (Barone et al., 2009; Breen and Drutyte, 2013). Whilst there is evidence that briefly touches upon anxiety, multiple references in the literature refer to the lack of anxiety-specific research in Parkinson’s (Barone et al., 2009; Breen and Drutyte, 2013).
Stress and anxiety are terms often used either together or interchangeably in relation to Parkinson’s, yet these terms need clarification. Bystritsky and Kronemyer (2014) emphasise that stress is an external process that arises from an individual’s environment. In contrast, Sylvers et al. (2011) define anxiety as an ever-present internal feeling of excessive fear and worry that is invasive in everyday existence, often having a negative impact on one’s quality of life. It is appropriate to focus solely on anxiety, rather than a combination of the terms, because it focuses on the individual and their experience rather than the wider external environment over which they may have little control. The presence of anxiety is linked to decreased quality of life and an increase in motor symptoms in PWPs, yet authors have noted a lack of anxiety-specific research in Parkinson’s (such as Barone et al., 2009 or Breen and Drutyte, 2013). Wressle et al. (2007) interviewed seven older PWPs (64–77 years) in a qualitative study to identify factors affecting their quality of life. Consistent reports of increased emotional sensitivity leading to higher anxiety emerged. For example, PWPs experienced anxiety about being unable to care for their partner should they become unwell. These experiences resulted in people planning to avoid stress wherever possible. Sunvisson (2006) interviewed a single PWP using a phenomenological approach at intervals over a 5-year period. This paper identified similar themes to Wressle et al. (2007), such as experiencing a fear of the future, increased sensitivity to stress, and increased anxiety associated with the unexpected. These themes explored anxiety provoked by declining skills and the pressure of maintaining social involvement. The single participant design means these findings have limited transferability. Given the high prevalence of anxiety in Parkinson’s, and limited research, an understanding of the experience of anxiety amongst PWPs is required. Deane et al. (2014) concur; in collaboration with the charity Parkinson’s UK, they identified anxiety as the second highest unmet research need in Parkinson’s. None of the papers reported clearly stated an included PPI component in their design.
This suggests that a future exploratory study using in-depth phenomenological face-to-face interviews to explore the lived experience of anxiety among people with Parkinson’s is required to respond to this research gap. Some methodological issues appear self-evident, for example purposive sampling used with a maximum variation strategy to capture a wide range of participant experiences (Emerson, 2015). However, to design such a study well, a PPI consultation phase was required using a qualitative approach to provide a richer understanding of PWPs’ views about how the study should be conducted.
Method
Aim
The aim of this PPI consultation was to explore PWPs’ opinions regarding the need for anxiety research, and any methodological considerations they felt would be important for future research studies. This work provides the foundation for occupational therapists to develop more robust research into constructing a future complex intervention to support PWPs experiencing anxiety.
Design
The methodology for this PPI consultation was founded upon a constructivist epistemological framework, which views an individual’s reality as a construct of the human mind formed from interacting with experience in the real world (Elkind, 2004). A pragmatic inquiry framework, along with an inductive approach, was used to focus the PPI participants to look for actionable findings. Pragmatism itself is conceptually consistent with the philosophical underpinnings of occupational therapy (Ikiugu and Schultz, 2006). This further serves to make this a suitable research framework to be implemented by occupational therapists. The findings of this PPI consultation will be used to inform the development of future occupational therapy research. Semi-structured telephone and Skype interviews were conducted in this PPI consultation to facilitate the description of retrospective experiences and opinions towards the future research. The interviews were conducted in February and March 2016.
Sample
Parkinson’s UK provide their own ‘Research Support Network’, which helps researchers recruit participants with the charity’s support. PWPs that are interested in engaging with PPI consultations receive training for the specific purpose of engaging with researchers. Contact was made with the charity’s PPI coordinator via an online form, and a subsequent recruitment email was developed with the PPI coordinator to email out to volunteers. This email included a brief description of the proposed study and the purpose of the PPI consultation. The information sent out was explicit in stating that this PPI consultation focused on anxiety and an anxiety study. Also offered were choices for how the PPI consultation interview could be conducted, considering that communication problems are a common difficulty for PWPs (Barone et al., 2009). Choices offered included telephone interviews, Skype interviews, email, or any other suggestions the volunteer had. If participants consented to engage in the consultation by responding to the email, the main author contacted them to arrange a mutually convenient time for the interview.
Papers reporting similar consultations had sample sizes ranging from seven to 17 participants (Daveson et al., 2015; Kleme et al., 2014). Considering the wide range of sample sizes presented in the literature, a sample of 10 was deemed large enough to provide a potential saturation point for this PPI consultation whereby enough rich data could be extracted (Creswell, 2003). Participants were recruited using convenience sampling. The first 10 PWPs to respond were included in the consultation. These participants had received training for PWPs interested in being involved in research consultations.
Ethical considerations
Ethical approval was provided by Plymouth University’s health student ethics sub-committee, ref number (16/17)-244. Participants gave written consent via email, which included a clear statement that the work would be published.
Data collection
The PPI consultation was completed in line with the process laid out in the NIHR handbook (NIHR, 2014). Seven participants chose to undertake a telephone interview and two participants chose to engage in a Skype interview using a webcam. One participant stopped responding to emails. The PWPs suggested no other interview methods. The first author, who is an occupational therapist, conducted all interviews.
A short, six-question interview schedule was used for all PPI consultation interviews (Figure 1). The Parkinson’s UK PPI coordinator reviewed the interview schedule prior to use. Taking advice from the PPI coordinator, minor changes to the wording of questions were made. The first question was a general question to open up the interview and relax the interviewee, with the second question being used to focus the interview. This was in line with the guidance presented in the NIHR handbook (2014). Audio recordings were made during all interviews, with participants’ consent, and were destroyed following transcription. Field notes were taken during all interviews to ensure richness of data. The shortest interview lasted nine minutes and the longest interview lasted 35 minutes, with a mean average interview duration of 18 minutes.
Interview guide and prompt sheet.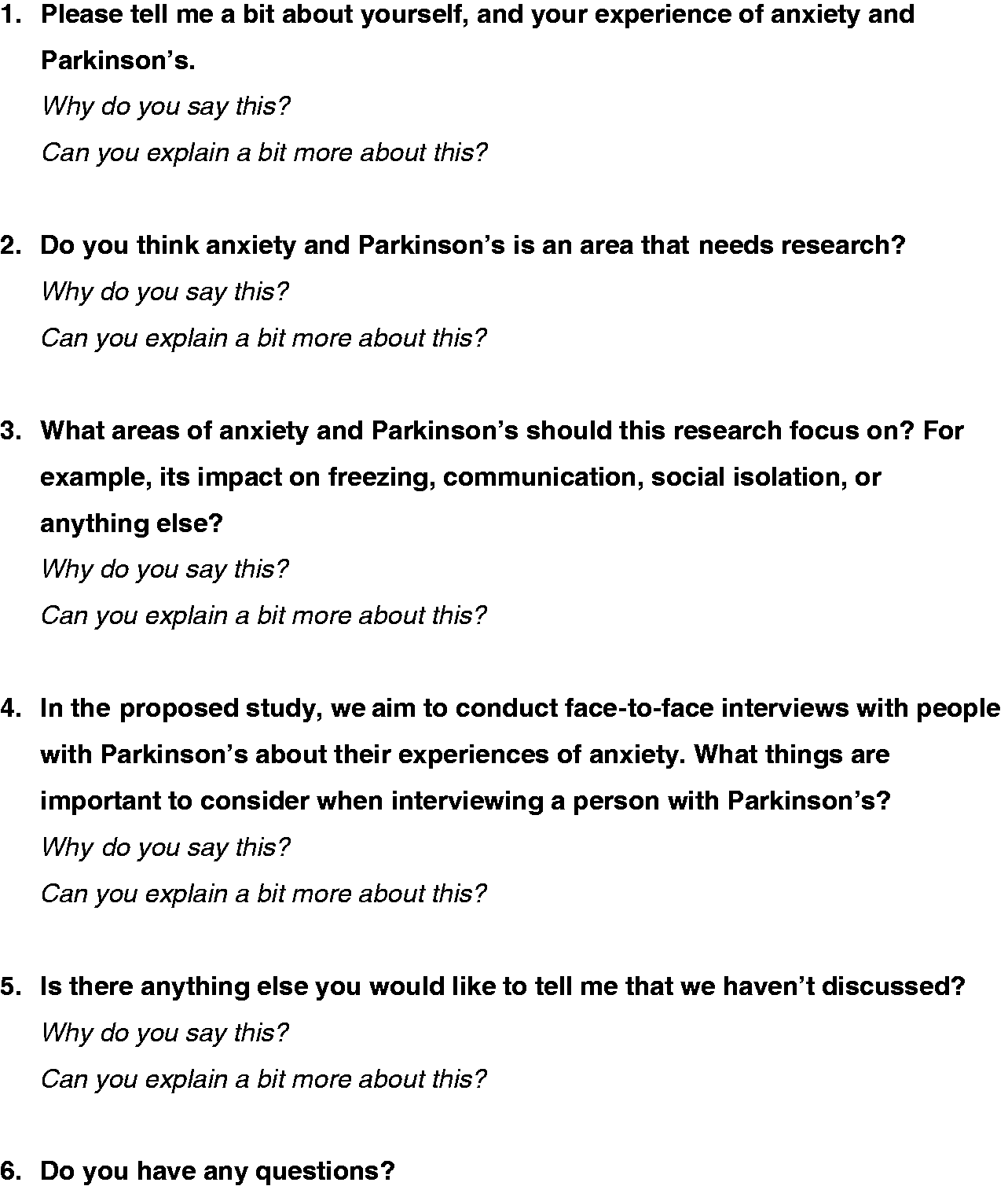
Data analysis
Data was analysed using thematic analysis to identify, analyse, and report patterns emerging from the data (Braun and Clarke, 2006). An inductive approach was adopted to allow frequent, dominant, and significant themes to emerge from the raw data without the restrictions of a predefined framework. The transcribed interviews were then uploaded to the computer-assisted qualitative software NVivo (version 10). This was used to facilitate coding and to take advantage of its ability to manage, organise, and track data. Next, three researchers (CL, DC, and DWE) read the interview transcripts to immerse themselves within the data. They then independently formulated initial codes (sub-themes) across the data. The researchers then examined their defined codes together until agreement was reached. Several codes were renamed or merged to provide a deeper understanding of the participants’ meaning and experiences. The third step was collating and reviewing the codes to identify potential themes. The final step was the search for vivid quotations to illustrate the themes that related back to the PPI consultation’s aim. The rigour and credibility of the data analysis was assured by two senior researchers (JL, KB). The senior researchers provided constructive feedback until consensus was achieved on the text fragments, sub-themes, and themes. These themes are illustrated with quotes that have been anonymised with pseudonyms to protect confidentiality, and presented with corresponding transcript (T) and line numbers for transparency.
Rigour
The criteria proposed by Lincoln and Guba (1985) were used to promote rigour and credibility in the PPI consultation’s findings. Once interviews were transcribed verbatim, member checking was employed to ensure the validity of the accounts. Three of the nine interviewees consented to checking their respective interview transcripts; they confirmed their accuracy. Peer-review triangulation was used to ensure increased credibility in the coding process. This was achieved using two independent reviewers, of different professional backgrounds, who did not work directly with PWPs to code a sample of transcripts (four of nine transcripts). Member checking was also employed following thematic analysis. Three of the original participants assessed the adequacy of the data analysis and confirmed its validity. Findings were triangulated with Sunvisson (2006) and Wressle et al. (2007) to ensure that the developed themes were rich, robust, and valid.
A reflexive field journal was used to confirm that the researchers’ assumptions had as minimal an influence on the findings as possible. On two occasions, participants asked the author unexpected and challenging questions regarding the author’s opinions on familial genetic testing for Parkinson’s. Whilst adequate answers were given redirecting the participants to their GPs and a short debrief with the Parkinson’s UK PPI coordinator occurred, it has highlighted the need for comprehensive planning for such unexpected questions. Being reflexive, it is surmised that the participants might have been introducing a new topic that was more important to them, and perhaps more of a priority for research than anxiety. This is a subject that warrants further exploration as a potential area of research.
Findings
Following the initial email appeal, 10 volunteers expressed interest (six male, four female). The mean age of all participants was 65 (age range 33–79). One male participant initially responded to a follow-up email, and then stopped answering emails with no reason given. It was assumed he had declined to participate in the consultation, and no further contact was attempted. The final number of participants was nine (five male, four female).
Clustering of sub-categories into three main themes.

Experiences of anxiety in Parkinson’s
All participants expressed anxiety as a negative experience associated with Parkinson’s that has a detrimental impact on quality of life, which should be the focus of future research. Three participants in the opening question described certain roles, for example jobs, as ‘stress’ and ‘stressful’, but none ever directly described themselves as stressed or used the term in any other way. Anxiety was often described as ‘crippling’, and one of the most disabling aspects of Parkinson’s. For example: … my own experience of anxiety is that it can be a crippling illness. I used to have panic attacks and the fear of getting one was almost worse than actually having a panic attack. I think anxiety can be a real scourge for people with Parkinson’s who suffer from it. (Irene, T9, line 94) It’s there in the background all of the time, and I was always fearful of it reoccurring, it was a very painful experience having anxiety to the extent that I did. It was, it was just awful. (Harry, T8, line 38)
Coping with anxiety in Parkinson’s
A variety of coping strategies were identified. Four participants identified internal resilience as an important coping strategy or mechanism, and that this was something that was either developed prior to being diagnosed with Parkinson’s or after: … possibly that I have had a career which is not a conventional career in terms of progression through the same field of work over a large number of years. I have totally changed course from time to time and in, at those change points there has been some apprehension about what is going to be happening next. And it’s possible that I have learnt to cope with those situations over time, even before I had Parkinson’s. Therefore, when I now look at myself and the last three years there must be some coping mechanism somewhere which means that I don’t quite feel anxiety the way that I’ve noticed some people seriously suffer from who have Parkinson’s. (Eric, T5, line 20) … when I got diagnosed first I mentally put myself into a little electric buggy which my mother had had when she had rheumatoid arthritis, and I mentally drove around in this buggy for about three days, then a good friend of mine said heh, my aunt’s had Parkinson’s for 18 years and she plays badminton three times a week and get over yourself. I burst out laughing and realised what I’d been doing. I ditched the buggy. (Abigail, T1, line 344)
Considerations for future research
Every participant stated that anxiety in Parkinson’s needs further research and that they felt that future research in the area was relevant: ‘Oh absolutely, because the PWPs that I hang out with and talk to, for us this is a big area and a very debilitating area’ (Abigail, T1, line 72).
The impact of anxiety on social interaction and communication were felt to be key areas that participants believed that research should focus on. Participants reported that social situations that they previously had no issue with or even excelled at, now either caused or were affected by anxiety, causing emotional distress and loss of quality of life. Furthermore, this often led to the loss of occupational roles for participants. This was closely related to communication in that people often felt becoming more anxious affected their voice, which in turn made them more anxious and continued the cycle: ‘In my case, my voice changes. It gets weaker. I think uh, people tend to um, worry about what people think of them. And then that makes my voice worse’ (Gordon, T7, line 244).
Participants highlighted a number of considerations for researchers interviewing a PWP, which also have additional implications for occupational therapists and other healthcare professionals. For example, of primary importance was to consider ‘the impact of the interview’ (Charlie, T3, line 102) and ‘get to know the person’ (Daniel, T4, line 124). Suggested solutions for these were to provide multiple choices for where, when, and how the interview is performed, and having a pre-interview telephone call to make sure the person is having a good day. Logistical considerations were consistent across all participants, for example ensuring there are adequate breaks, considering the time of day, timing the interview with respect to on/off phases, allowing additional time for slowed thinking and communication, and easy access to drinks and medication. Several participants highlighted the importance of establishing a safe environment. It was important to frame the researcher–participant relationship as collaborative and mutually beneficial to achieve research aims: I feel very strongly that I am the expert in my own body, and in my own life, and I get cross when medical professionals and whatever feel, try to tell me what I am or should be feeling. So, creating an atmosphere of partnerships and mutual benefit. (Abigail, T1, line 221)
Discussion and implications
This PPI consultation showed that PWPs interviewed considered the proposed study to be important, needed, and relevant, which corresponds with the findings of Deane et al. (2014). Some of the themes uncovered in this consultation have been noted in relation to coping with anxiety in Parkinson’s before. Sunvisson (2006) identifies the conscious structuring of daily habitual routines and activities to reduce anxiety. Furthermore, Wressle et al. (2007) identified activity restriction and decreased socialisation as contributors to increased anxiety and fear. Considerations for future research specifically regarding experiences of anxiety in Parkinson’s have not previously been discussed in the literature.
The participants stated that anxiety was invasive and had a detrimental impact on their quality of life, as confirmed in other studies (Lindesay et al., 2012). The specific sub-themes regarding the fear of the future and unpredictability were indicated in the works of Sunvisson (2006) and Wressle et al. (2007), although these studies were not focused on anxiety in Parkinson’s. However, as these themes have also appeared in papers discussing anxiety in general populations (Cisler et al., 2009), it suggests that future research should focus on determining more precisely how anxiety is experienced for PWPs than those without the condition. This intelligence could inform the design of discrete, effective anxiety interventions and approaches for people with Parkinson’s (Deane et al., 2014) and presents an opportunity for occupational therapists to become pioneers in the development of such treatments.
Coping strategies were an area that all participants felt required more research. Whilst some studies have explored coping with anxiety for people without Parkinson’s (Krohne and Hock, 2011), literature regarding coping mechanisms for anxiety in PWPs has been limited to outcome measurement or experiences regarding deep brain stimulation that only affect a small number of individuals (Hurt et al., 2011). Researchers have only just started to focus on Parkinson’s-specific anxiety interventions (Bloem et al., 2015), and in particular mindfulness techniques are emerging as potential anxiety treatments for PWPs (Pickut et al., 2015). However, it has been acknowledged that mindfulness is not a solution for everyone (Holmes, 2009). The views of participants in this consultation suggest that future research should explore coping strategies in more depth to highlight alternative avenues of research.
The concept of establishing a safe and sensitive research environment was important to participants, to enable them to feel both physically and psychologically supported. This will be valuable to not only maximise validity, but also minimise any risk of bias or potential harm in the proposed study (Morris et al., 2009). An important consideration raised in the consultation was the need for a ‘culturally safe research environment’. This will be important for interview schedule planning: to protect participants from potential indirect harm, and experiences of feeling demeaned, or under-represented by a dominant research methodology, epistemology, or even socio-cultural lens (Elmir et al., 2011). Furthermore, participants identified wanting a ‘mutually beneficial’ rapport with researchers in this consultation. Guillemin and Heggen (2009) argue that establishing this type of rapport early is necessary for generating rich data and ensuring respect is sustained between researchers and participants. In addition, Varga-Dobai (2012) details how a strong researcher–participant rapport can provide mutual benefits in self-learning and reflection. Alongside the concrete logistical suggestions put forth by participants, this suggests that establishing a safe research environment and strong researcher–participant rapport early on should be key practice in future research. As the suggestions of collaborative working and rapport-building are key concepts of occupational therapy, this places the profession in an ideal position to lead such research.
Limitations
Despite successful recruitment through the Parkinson’s UK PPI network, it must be acknowledged that by limiting to one recruitment method this has narrowed the potential sample and potentially introduced bias. That is, only those individuals with access to a computer, an Internet connection, and an email account were able to participate. Furthermore, the participants accessed through the Parkinson’s UK network have all received training in PPI, therefore whether they can truly be considered ‘lay people’ is debatable (Mockford et al., 2012).
It may be argued that only subjecting a small sample of the transcripts to peer-review triangulation reduced the credibility of the findings. However, there was close agreement between reviewers, which increases confidence in the findings. The fact that not all participants chose to be involved with member checking may impact on the robustness of these findings (Morse, 2015). However, those who did respond agreed with the analysis, suggesting it represented their views. It is acknowledged that there is controversy surrounding the validity of multiple-source triangulation; the assumption that weaknesses in one method will be compensated for in another are unlikely (Morse, 2015).
Finally, a particular challenge of this consultation is the nature of PPI itself. Both Staniszewska et al. (2008) and Mockford et al. (2012) highlight that there is little evidence supporting the effectiveness of PPI. Furthermore, in their systematic reviews both Mockford et al. (2012) and Brett et al. (2014) highlight the little impact that PPI has in terms of real world benefits to date. Our PPI was specifically performed to inform a research proposal. The participants were PWPs acting as consultants and not research participants (NIHR, 2014), but they were able to provide valuable contributions to improve the research protocol.
Conclusion
Despite the evidence suggesting PPI has little impact on real world healthcare or research, this consultation work has provided valuable insights into important issues related to anxiety in Parkinson’s. The findings should inform the design of future studies. Working in collaboration with Parkinson’s UK proved to be a valuable resource for recruitment. The methods used for interviewing participants (telephone and Skype interviews) worked well, but from the feedback received in this consultation it would be beneficial for occupational therapy researchers to provide more choice or novel ways in which participants can engage. With this in mind, it is important for researchers to also plan to access support for participants should unexpected and challenging questions arise. Finally, the philosophy of occupational therapy complements the identified recommendations in such a way that occupational therapists are ideally placed to take research into anxiety in Parkinson’s forwards.
Key findings
This consultation round with people with Parkinson’s strengthens the argument that anxiety needs more research. People with Parkinson’s identify anxiety as a ubiquitous, detrimental presence in their lives which they cope with in a variety of ways. Establishing a safe and supportive research environment for participants with Parkinson’s is important for occupational therapists to consider when designing and conducting research.
What the study has added
Anxiety is experienced by people with Parkinson’s and it should be a consideration when developing interventions with, and the design of research about, people with this condition.
Footnotes
Acknowledgements
The authors would like to thank the participants for sharing their experiences and their time, Daffyd Wilson-Evans for his contribution to the triangulation process, and Isabelle Abbey-Vital at Parkinson’s UK for her support with the PPI consultation process.
Research ethics
Ethical approval was obtained from Plymouth University’s health student ethics sub-committee, reference number (16/17)-244, 2016. Participants gave written informed consent via email, which included a clear statement that the work would be published.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
This research received no specific grant support from any funding agency in the public, commercial, or not-for-profit sectors.