
Abstract
Introduction
Psychosocial contributors to fall risk for people with multiple sclerosis are often overlooked in falls prevention practice. This study explored several fall-related, psychosocial variables and their association with falls self-efficacy in a sample of people with multiple sclerosis reporting a fall.
Method
A cross-sectional, structured telephone survey was employed. The survey explored socio-demographics, multiple sclerosis characteristics, and fall-related psychosocial variables. Multiple linear regression was employed to investigate associations with Falls Efficacy Scale – International scores.
Results
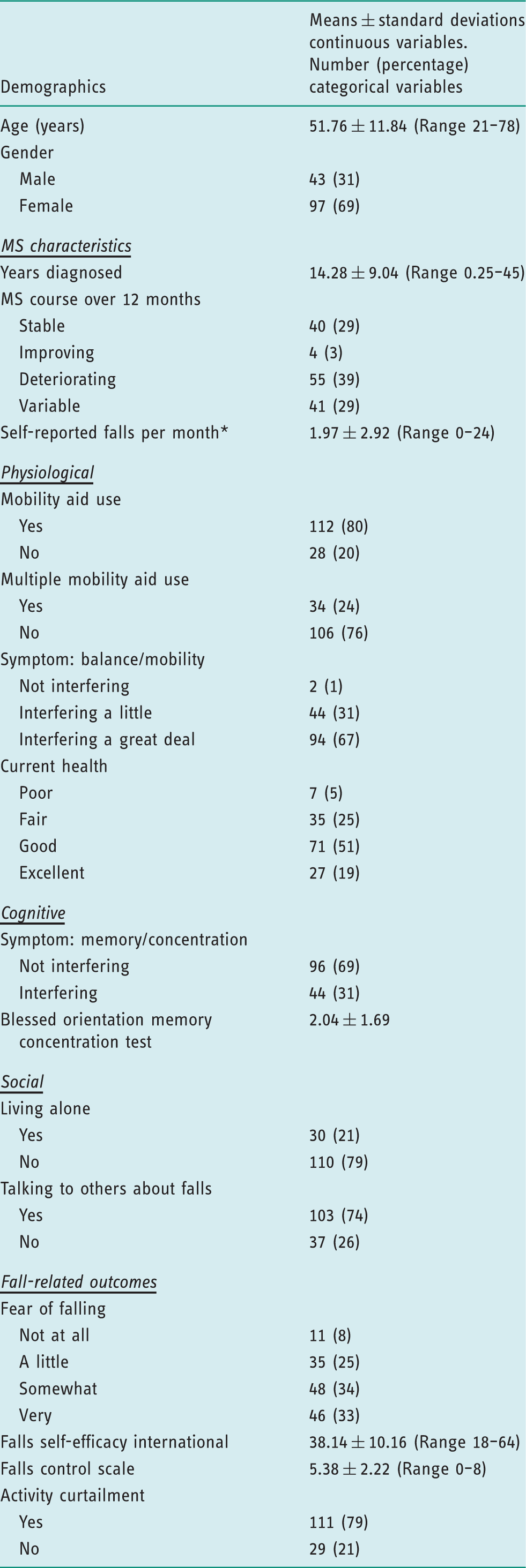
The mean Falls Efficacy Scale – International score for 140 participants was 38.14(SD = 10.16), and the mean Falls Control Scale score was 5.38(SD = 2.22). Fear of falling was expressed by 129 (92%) participants, with 111 (79%) reporting associated activity curtailment. A regression model including six predictors explained 47% of the variance in the Falls Efficacy Scale – International scores. Results of the multiple linear regression showed that fear of falling, associated activity curtailment, balance interference, falls control, and health status were associated with falls self-efficacy.
Conclusion
Fear of falling and associated activity curtailment, low falls self-efficacy, and compromised falls control are common among people with multiple sclerosis who have fallen. These fall-related psychosocial variables are distinct and each warrants attention during assessment. Findings suggest that falls self-efficacy among people with multiple sclerosis who have fallen is a complex construct associated with physical and psychosocial factors.
Introduction
Multiple sclerosis (MS) is a chronic, inflammatory-mediated disease resulting in demyelination of the central nervous system, and is often progressive in nature (Trapp and Nave, 2008). Currently it is estimated that the global prevalence of MS is 33 per 100,000, with a total of 2.3 million people with MS (pwMS) worldwide, rendering MS as one of the most common neurological disorders in the developed world, with a notably high incidence in young adults (Koch-Henriksen and Sørensen, 2010). The pathological and symptomatic presentation of the disease are markedly heterogeneous with motor, sensory, psychological, and cognitive deficits regularly seen in varying proportions (Compston and Coles, 2002).
Due to the diversity of systems affected by MS, occupational therapists and health professionals alike must address a diverse range of impairments and factors that threaten the functional status and participation ability of pwMS (Steultjens et al., 2003). Within this diversity of rehabilitation practice, falls prevention for pwMS is an area of rehabilitation that has received little attention in the past and is an area described as being very much in its infancy at present (Sosnoff and Sung, 2015).
Falls are now recognized as a considerable consequence of MS, with recent literature suggesting that 56% of pwMS will experience a fall in any 3-month period (Nilsagard et al., 2015). Like MS symptomatology, risk factors for falls in this population are diverse, and their impact on functioning is likely to be cumulative in nature (Gunn et al., 2013). Among pwMS, 44% to 58% of falls will result in injuries (Cameron et al., 2013). Compared to physical outcomes, fall-related psychosocial outcomes, such as fear of falling, falls self-efficacy, and falls control, often receive far less attention during fall prevention efforts for pwMS. This is evident in the lack of consistent consideration of psychosocial factors in fall prevention trials involving pwMS (Sosnoff and Sung, 2015). Systematic reviews examining evidence for the effectiveness of interventions within the scope of occupational therapy practice for pwMS suggest that pwMS benefit from individualized, goal-directed interventions that address functional performance and promote participation, such as multidisciplinary rehabilitation programmes, health promotion programmes, and fatigue management courses (Yu and Mathiowetz, 2014). The omission of consideration of fall-related psychosocial outcomes may reflect the fact that MS fall prevention intervention research is still in an early phase of development. Nonetheless, fall-related, psychosocial outcomes warrant the attention of interdisciplinary health care professionals, including occupational therapists, due to concerns regarding a client’s subjective experience of engagement in occupation (AOTA, 2014) alongside their prevalence and impact on pwMS being increasingly well documented (Mazumder et al., 2015; Peterson et al., 2007).
Fear of falling, defined as a lasting concern about falling that leads to an individual avoiding activities that he/she remains capable of performing (Tinetti and Powell, 1993), is a multidimensional construct possessing physiological, cognitive and behavioural components (Hadjistavropoulos et al., 2011). Researchers investigating the prevalence of fear of falling involving pwMS have operationalized the construct in different ways, using terms such as ‘worried or afraid’ (Finlayson et al., 2009; Peterson et al., 2008) or ‘concerned’ (Matsuda et al., 2012; Peterson et al., 2007).
Activity curtailment due to fear of falling has received widespread attention in the geriatric literature. Although activity curtailment can be protective when it prevents a person from engaging in activities that exceed functional abilities, gerontological research has demonstrated that excessive activity curtailment due to fear of falling that leads an individual to avoid activities that he or she is safely capable of performing can have a detrimental effect on physical functioning and independence (Delbaere et al., 2004). For this reason, it is alarming that findings from a large cross-sectional study involving pwMS revealed that 83% of the study participants reported fear of falling and associated activity curtailment (Peterson et al., 2007). Such restriction of activity bears considerable additional weight for MS populations given the breadth of evidence highlighting the deterioration of symptoms resulting from inactivity (Motl et al., 2008).
Perceived sense of control over falling and falls self-efficacy have been shown to act as significant mediating factors on fear of falling and activity curtailment during falls prevention interventions for older adults (Zijlstra et al., 2011). Perceived sense of control over falling is a construct originally presented by Tennstedt et al. (1998). Finlayson et al. (2009) subsequently used the Falls Control Scale as an outcome in a pilot study of a fall risk management programme specifically designed for pwMS. The concept of falls self-efficacy was created by Tinetti et al. (1990), who developed the original Falls Efficacy Scale (FES), and is based on the theoretical work of Bandura (1977). Bandura defined self-efficacy as belief in one’s ability to succeed in specific situations or accomplish a task. Self-efficacy is important because it determines how people feel, think, motivate themselves, and behave (Bandura et al., 1994). Self-efficacy also influences how much effort people will expend and how long they will persist in the face of obstacles and aversive experiences (Bandura, 1977; Bandura et al., 1994). The Falls Efficacy Scale – International (FES-I), which was introduced in 1990, was developed to address the limitations of the FES, and is now considered a criterion standard for assessment in older adults (Yardley et al., 2005; Zijlstra et al., 2007). Although the term ‘falls efficacy’ has been retained in the title to acknowledge the historical development of the scale, the FES-I actually assesses ‘concern’ about falling, a term that is closely related to fear, but is less intense and emotional (Yardley et al., 2005). The instrument assesses the intensity of concern about falling when performing a range of physical and social activities that vary in the degree of physical challenge they present. Importantly, when introduced, the FES was intended as a measure of fear of falling; however, evidence stemming from studies involving older adults now suggests that falls self-efficacy and fear of falling are separate constructs (Hadjistavropoulos et al., 2011; McKee et al., 2002). Among pwMS, falls self-efficacy has been shown to be associated with future recurrent falls independent of past recurrent falls in people with MS (Mazumder et al., 2015).
Within the occupational therapy literature, falls self-efficacy has been studied in the context of the Model of Human Occupation (MOHO) (Peterson et al., 1999, 2010). Peterson et al. (1999) provided justification for considering falls self-efficacy as a component of personal causation by demonstrating the relationship between falls self-efficacy and several measures of occupational functioning. When considered an aspect of personal causation, falls self-efficacy can be understood as part of a larger pattern of thoughts and feelings that cluster around choices for and experience and interpretation of participating in occupations (Peterson et al., 1999). A qualitative study undertaken to explore and describe the lived experience of falls self-efficacy among six pwMS yielded an overall theme of managing fall risk as a means of supporting activity, and revealed the multidimensional nature of falls self-efficacy (Peterson et al., 2010). The findings also emphasized that the study participants’ involvement in valued occupations was clearly influenced by their feelings and thoughts about their personal causation (that is, their sense of capacity and effectiveness).
Recognizing the critical role that fall-related, psychosocial variables have in influencing fall risk and the unique significance of falls self-efficacy to both the MOHO and the wider interdisciplinary fall prevention community, this study was undertaken to (a) explore fall-related psychosocial variables in a sample of pwMS with a recent fall history and (b) investigate a range of fall-related variables and their association with the criterion standard of falls self-efficacy.
Method
Design
This study was cross-sectional in nature, employing a structured telephone survey for data collection.
The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist for cross-sectional studies was utilized throughout the reporting of this study (Von Elm et al., 2014).
Ethical approval
This study was reviewed and approved by the Education and Health Sciences Research Ethics Committee at the University of Limerick, Ireland (Approval reference: 2014_05_08_EHS).
Recruitment
Participants were recruited primarily through the Multiple Sclerosis of Ireland Society registry, with regional offices acting as gatekeepers distributing text and/or email alerts to members within their locality. Practising physiotherapists in acute and community settings and social media were further used to disseminate information relating to the study. Eligibility criteria for this study were a self-reported diagnosis of MS, aged 18 years or older, the ability to ambulate 10 metres with or without a walking aid, and having self-reported at least one fall in the last 3 months.
Instrument
The survey utilized in this study was developed by two of the authors and based on a survey used in previous studies of pwMS (Finlayson et al., 2006; Peterson et al., 2007). Amendments were made to the instrument following reflection on its utility in these initial studies and to add standardized outcome measures. The survey contained four sections: socio-demographics; MS characteristics; fall-related psychosocial variables; and falls prevention intervention development. For the purpose of this study, only data relating to socio-demographics, MS characteristics, and fall-related psychosocial variables were used. Extracted variables were based on previous studies relating to fear of falling in pwMS (Finlayson et al., 2006; Peterson et al., 2007). Information on age and gender was collected, in addition to MS-related characteristics such as time since diagnosis and MS course during previous 12 months (‘stable’, ‘improving’, ‘deteriorating’, or ‘variable’) (Finlayson et al., 2006).
Data on physiological variables were collected, including self-reported interference of balance/mobility via the question ‘How much do problems with balance or mobility interfere with your daily activities?’ (‘not a problem’, ‘interfering a little’, ‘interfering a great deal’) (Finlayson et al., 2006). Fall history was established by asking: ‘In any given month, how often do you fall to the ground, including both inside and outside?’; use of mobility aids (‘no aids’, ‘one aid’, ‘multiple aids’); self-reported falls in the past month; and current health status (‘poor’, ‘fair’, ‘good’, ‘excellent’) (Peterson et al., 2007). The Blessed Orientation Memory Concentration test (BOMC) was used to assess cognition, with higher scores indicating possible cognitive impairment. Self-reported interference of memory or concentration was collected through the question ‘How much do problems with concentration or forgetfulness interfere with your daily activities?’ Response options offered were ‘not a problem’, ‘interferes a little’, or ‘interferes’ (Finlayson et al., 2006). Social variables collected included asking if the participants lived alone at present (‘yes’, ‘no’) (Peterson et al., 2007) and if they spoke to others about their falls, including family members, friends, and healthcare practitioners (‘yes’, ‘no’).
Information relating to fall-related, psychosocial variables was collected through four measures. The 16-item Falls Efficacy Scale International (FES-I), which has been shown to be a valid and reliable measure in pwMS, was administered (van Vliet et al., 2013). Scores range from 16 to 64, with higher scores indicating lower falls-efficacy. Fear of falling was assessed through a Likert response to the question ‘How worried are you that you might fall?’ (‘not at all’, ‘a little’, ‘somewhat’, ‘very’). Fear of falling and its associated activity curtailment was assessed through a dichotomous question that was informed by the work of Peterson et al. (2007): ‘In general are there things you would like to do but do not do because you are worried you might fall?’ (‘yes’, ‘no’). The Falls Control Scale, developed by Tennstedt et al. (1998), was administered to assess perceived control. Items include: ‘I can reduce my risk of falling’; ‘there are things I can do to keep myself from falling’; ‘I can overcome my fear of falling’; and ‘falling is something I can control’. Scores range from zero to eight, with higher scores indicating higher perceived control over falling. Finlayson et al. (2009) used a five-point scale where 1 indicated ‘strongly disagree’ and 5 indicated ‘strongly agree’ and found the Falls Control Scale to have poor reliability in MS populations (Cronbach’s alpha = 0.48). Therefore, in this study, a three-item response option of ‘agree’, ‘unsure’, and ‘disagree’ was used in order to simplify the response options and examine the impact of that change on Falls Control Scale reliability for pwMS.
Procedure
Interested participants were provided with contact details for the research team and expressed interest through either phone or email. A member of the research team contacted interested participants to provide information relating to the study and afforded participants the opportunity to ask any questions or express concerns they had. Hard copies of a consent form and an information leaflet were then mailed to interested participants. The consent form was returned, via a provided stamped addressed envelope, to the research team if the participant wished to partake in the study. A follow-up phone call was made following receipt of the signed consent form to schedule an appropriate time to complete the survey. Prior to completion of the survey, participants were again provided the opportunity to ask questions and reminded that completion was voluntary and that they were free to cease at any point without reason or penalty. The survey took approximately 30 minutes to complete and the order in which questions were asked was standardized across all participants.
Data analysis
Data were coded, entered, screened, cleaned, and analysed through SPSS version 22 (IBM corporation, New York, USA) by the authors. Prior to analyses, variables were assessed for normality. The primary variable, FES-I score, showed a normal distribution, while the majority of remaining variables had a non-normal distribution, therefore non-parametric statistical tests were employed as appropriate.
Descriptive statistics were employed to describe the characteristics of the study population. For the purposes of this analysis, the FES-I was considered as the dependent (outcome) variable and the remaining 15 were considered as independent variables. The decision to anchor the FES-I as the dependent outcome reflects its well-established reliability and utility with the literature, providing a validated anchor to enable an exploratory analysis to be undertaken. To ensure multicollinearity was not present, Pearson’s correlation coefficients were assessed for all continuous independent variables and a cut off of r = 0.7 or above was set as the criterion for exclusion.
Exploration of the FES-I scores was undertaken using Spearman’s Rho to investigate relationships with the continuous variables of age, time since diagnosis, number of self-reported falls, and BOMC scores. Mann Whitney U tests assessed differences in FES-I scores among the dichotomous variables. One-way ANOVAs with Bonferroni post-hoc analyses were employed to investigate differences in FES-I scores across categorical variables.
Univariate associations between the independent variables and the FES-I were assessed through the use of simple linear regression. For inclusion in the multivariable regression model, explanatory variables had to have a threshold p-value of ≤ 0.15 in the univariate analysis (Hosmer and Lemeshow, 2000). Dichotomous categorical variables were entered directly into the model. Categorical variables were transformed using dummy-coding as directed by Field (2013), where each level of the variable was compared to all other responses (reference standard baseline group). The regression parameters are presented as the difference in FES-I score between that level of the variable and the reference standard baseline group. The F-statistic, statistical significance values, and R2 for each model are presented for interpretation. The beta value (β) and related 95% confidence intervals, indicating the degree which the FES-I scores vary with each independent variable when all other independent variables are held constant, and the statistical significance values for each significant association are further reported. In terms of developing a stable regression equation, an independent variable to sample size ratio of 3:40 was employed. This ratio is broadly in keeping with the 15 participants per predictor proposed by Tabachnick et al. (2001).
Results
Respondents
A total of 178 individuals expressed interest in taking part in the study. Fourteen individuals did not meet the eligibility criteria for the study: one person did not have a definite MS diagnosis; one person was unable to ambulate 10 metres; and 12 people had not experienced a fall in the previous 3 months. Twenty-one individuals declined to participate following distribution of consent forms/information leaflets, and three individuals could not be contacted to complete the survey after returning consent forms. Accordingly, 140 participants completed the survey.
Characteristics of participants
Descriptive Statistics (N = 140).
Exploration of FES-I scores
There was a weak but significant correlation between FES-I score and number of self-reported falls (r = 0.283, p = 0.001) and falls control (r = –0.338, p < 0.001). There was no correlation between age (r = 0.03, p = 0.723), time since diagnosis (r = –0.132, p = 0.121) or BOMC test scores (r = –0.007, p = 0.937).
Falls Self-efficacy International (FES-I) scores across dichotomous variables.
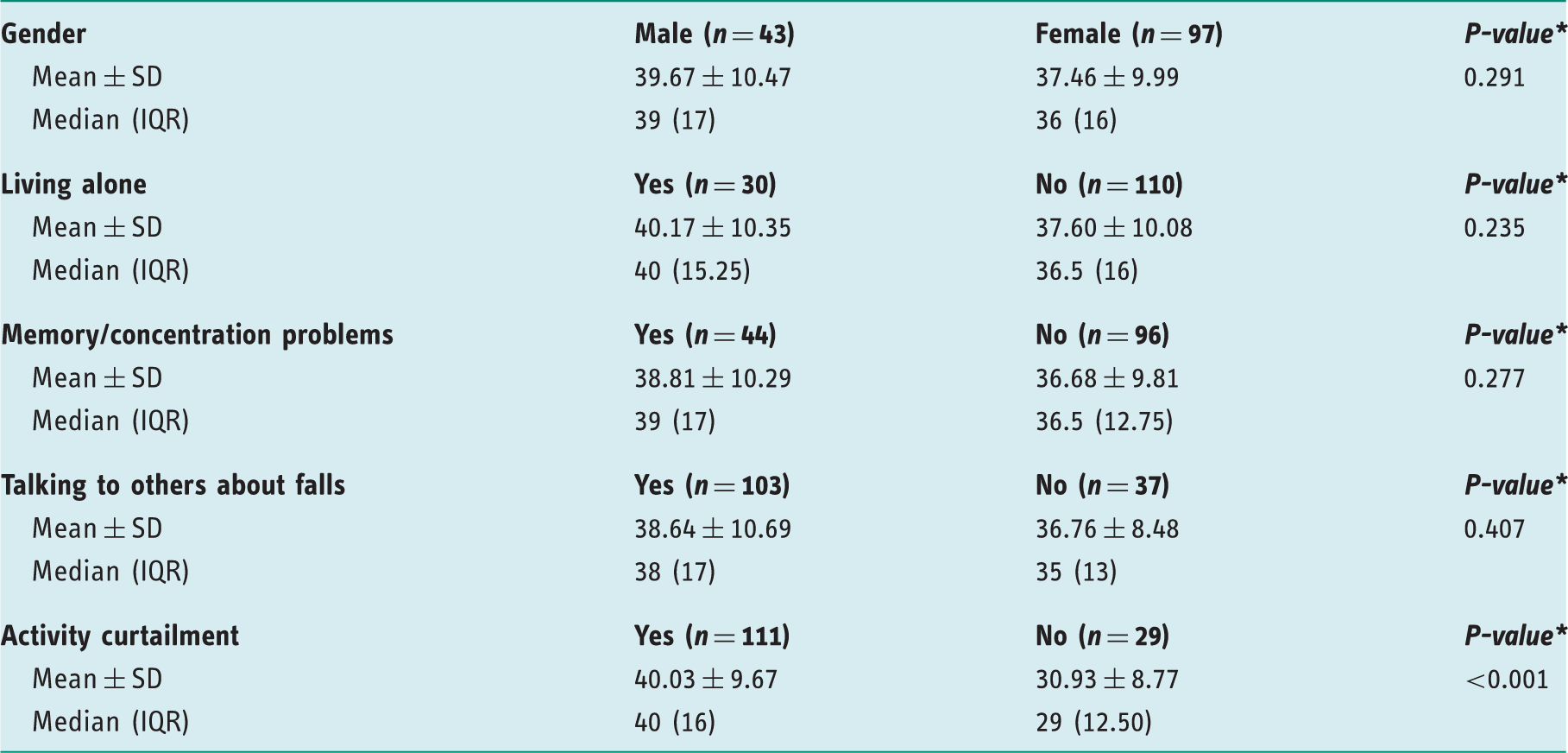
Mann–Whitney U Test
Falls Self- efficacy International (FES-I) scores across categorical variables.
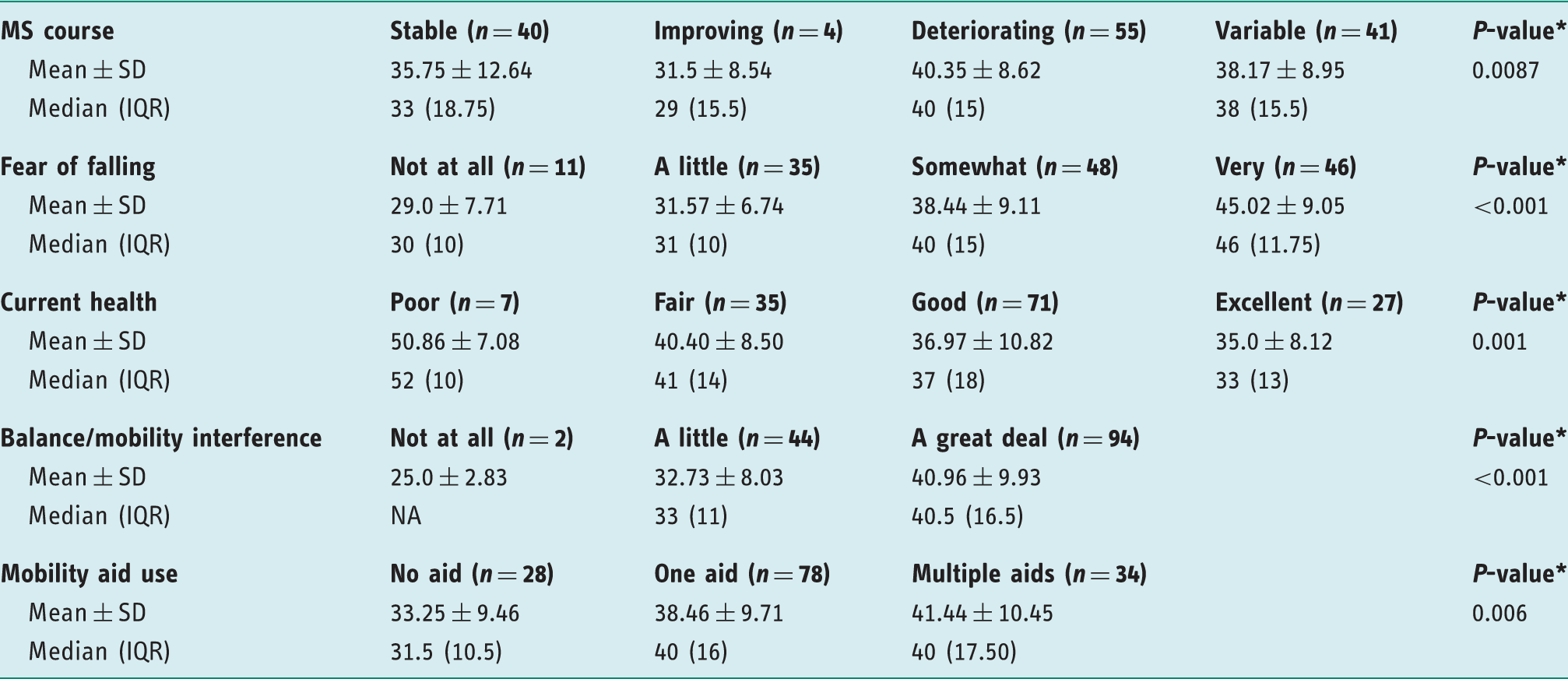
Results based on ANOVA tests
Univariate associations with falls self-efficacy
No variables met the criterion for multicollinearity and so all were eligible for inclusion in the further analyses. The 15 previously described variables were assessed for association with FES-I scores through the use of simple linear regression. Twelve variables met this entry criterion: a deteriorating MS course (β = 4.595, p = 0.029); self-reported falls (β = 0.081, p = 0.033); single aid use (β = 5.212, p = 0.018); multiple aid use (β = 8.191, p = 0.001); ‘fair’ health status (β = –10.45, p = 0.010); ‘good’ health status (β = –13.885, p < 0.001); ‘excellent’ health status (β = –15.857, p < 0.001); ‘somewhat’ worried about falling (β = 9.437, p = 0.001); ‘very’ worried about falling (β = 16.022, p < 0.001); ‘a great deal’ of balance interference (β = 15.957, p = 0.018); activity curtailment associated with a fear of falling (β = 9.096, p < 0.001); and falls control (β = –1.601, p < 0.001).
Multivariate association with falls self-efficacy
Multiple linear regression for Falls Self-efficacy International (FES-I) scores.
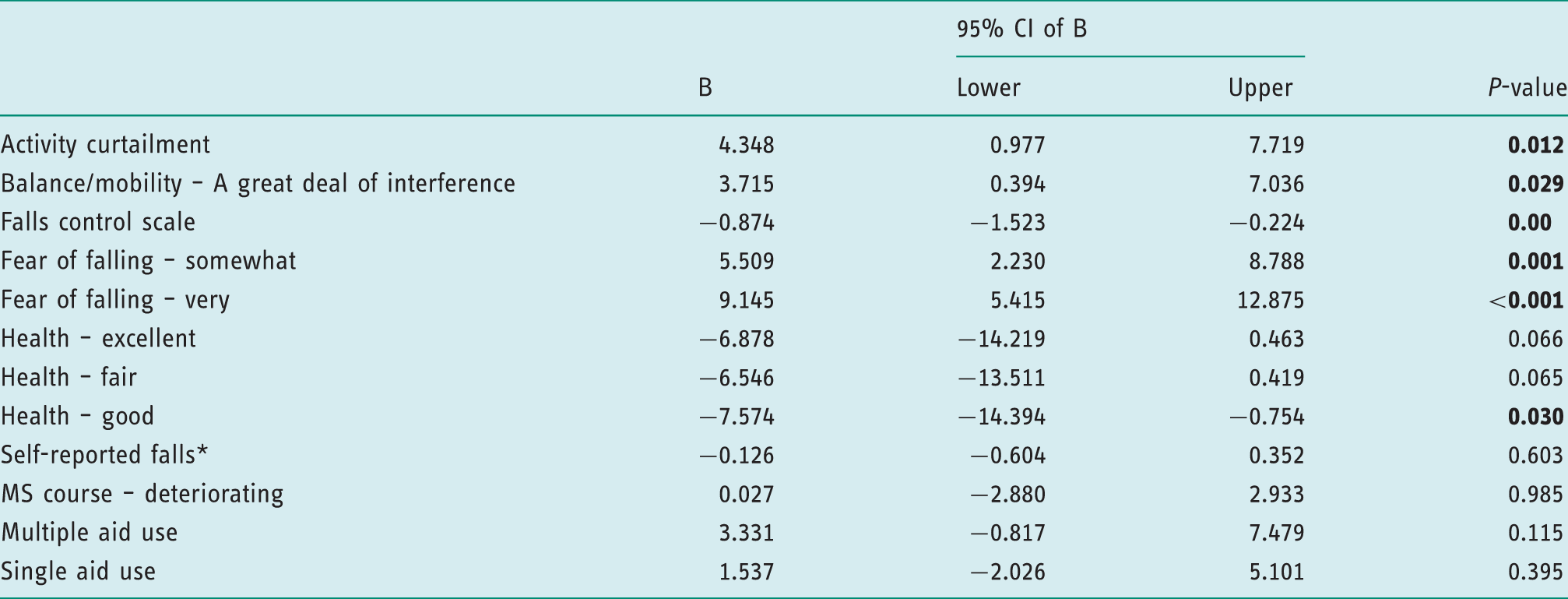
One participant was identified as an outlier and was excluded from analyses.
Discussion and implications
This was the first study to explore fall-related, psychosocial variables in a sample of pwMS who have fallen, and to investigate a range of fall-related variables and their association with the criterion standard of falls self-efficacy. The findings of this study indicate that fear of falling, associated activity curtailment, low falls self-efficacy, and compromised falls control are common in this population. Furthermore, each of these fall-related psychosocial variables are distinct and each warrants individualized attention during the occupational therapy evaluation process.
The degree of falls self-efficacy in the present study population, measured through the FES-I, is similar to those from a cross-sectional study of pwMS performed by van Vliet et al. (2013). Delbaere et al. (2010) created categories of ‘low’, ‘moderate’, or ‘high’ levels of falls self-efficacy based on FES-I scores drawn from an older adult population. Applying this interpretation indicated that on average, this sample of pwMS presented with considerably low levels of falls self-efficacy. Considered in light of the strong influence that self-efficacy has on motivation for participating in life occupations, as described by Bandura et al. (1994) and the MOHO (Kielhofner, 2008), and findings from qualitative research that point to the importance of falls self-efficacy to engagement in valued activities among pwMS (Peterson et al., 2010), this finding provides important evidence that attention to falls self-efficacy in occupational therapy practice and research involving pwMS is well justified.
This study adjusted the response options of the Falls Control Scale in an effort to improve the instrument’s performance in pwMS. We attained a reasonable increase in reliability scores in comparison to a previous study (Finlayson et al., 2009); however, the Cronbach’s alpha remains below the acceptable value of usability of 0.7. Hence, despite being a valuable measure in older adults (Tennstedt et al., 1998), the Falls Control Scale may not be appropriate for use in MS populations. One of the items in the Falls Control Scale is ‘Falling is something I can control’. This is at odds with the findings of a qualitative study involving pwMS, in which participants saw their risk for falling as always present and expected some falls to be inevitable (Peterson et al., 2010). Therefore, refinement of the Falls Control Scale to better match the perspectives of pwMS is indicated. Qualitative studies examining views that pwMS have regarding their ability to control falls and exploring the best wording to use for an item related to controlling falls would be beneficial.
The prevalence of fear of falling reported in this study is considerably higher than those previously reported in MS cohorts, which ranged from 60–67% (Finlayson et al., 2006; Matsuda et al., 2012; Peterson et al., 2007). A similar trend is seen in relation to activity curtailment associated with fear of falling, with previous studies reporting a prevalence of 68% (Peterson et al., 2007) and 71% (Matsuda et al., 2012). One explanation for these elevated findings is that the present study investigated only pwMS who had recently experienced a fall. However, further explanation may lie in discrepancies surrounding how these two constructs are assessed. The diversity of verbs used to capture the fear of falling construct (for example fear’, ‘worry’, ‘concern’), alongside the disparities which exist with regards to the response options used, such as the use of dichotomous versus multilevel options, will innately affect a participant’s response (Legters, 2002). A standardized means of assessment for both fear of falling and associated activity curtailment is crucial when considering future studies of MS populations.
In this multivariate analysis, our study found that both fear of falling and associated activity curtailment were independently associated with falls self-efficacy. This finding supports the positions of McKee et al. (2002) and Hadjistavropoulos et al. (2011), who advocate that despite potentially being related, these constructs remain distinct and should be treated as such in terms of measurement and interpretation of effect. This finding has important implications for both clinical and research practice in occupational therapy. Specifically, fear of falling, associated activity curtailment, and falls self-efficacy should be measured using tools that are known to be reliable for pwMS. It is important to note that occupational therapy interventions designed to help pwMS better manage fall risk often focus on closing the gap between task demands and personal capacity through the use of education and behavioural modification to reduce fall risk where an individual’s perception of ability is skewed, resulting in engagement in activities beyond their capacity. As a result of engaging in such interventions, an individual living with MS may develop a more realistic appraisal of his or her limited abilities, and their falls self-efficacy score may simultaneously increase, indicating less confidence in avoiding falls during day-to-day activities. Thus, if declines in falls self-efficacy are observed, it is vitally important for occupational therapists to explore the extent to which such declines are therapeutically beneficial, given that theoretically an avoidance of activity is a negative outcome; however, clinically this may reflect a reduction in behaviours related to fall risk (Hadjistavropoulos et al., 2011). Qualitative data can provide important insights that support interpretation of FES-I scores. Interpretation of falls self-efficacy scores, especially if seen over time, must also be assessed with full consideration of changes in MS symptoms, given that MS is typically a progressive disease.
Our findings suggest that fear of falling, associated activity curtailment, and falls self-efficacy are discrete outcomes and their prevalence among pwMS builds the case for targeting these outcomes through occupational therapy interventions. As targeted outcomes, they must be assessed before and after interventions to determine if significant and clinically important changes have occurred. Future research needs to identify what the minimal clinically important differences are for these outcomes in an MS population. Interventions informed by occupational therapy expertise and designed to address fall-related, psychosocial outcomes have been well-established in older adult populations. These interventions, which are typically complex in nature, provide important evidence that fall-related psychosocial outcomes are modifiable (Tennstedt et al., 1998; Zijlstra et al., 2009) and reduce falls (Clemson et al., 2004; Zijlstra et al., 2009). To date, only one evaluated intervention specifically designed for pwMS and targeting fall-related psychosocial outcomes exists. Finlayson et al. (2009) developed, delivered, and evaluated the ‘Safe at Home BAASE’ intervention. The intervention, which was delivered by occupational therapists, led to improvements in fear of falling, falls self-efficacy, and falls control among participants. The authors emphasized the necessity of promoting self-management practices, which is noteworthy given the increased attention that is being given to the role of occupational therapy in supporting self-management interventions (Leland et al., 2017). Further research employing robust trial methodologies is required to investigate the optimum strategies to build falls self-efficacy and address other fall-related psychosocial variables among pwMS. Findings from the present study suggest that interventions designed to build falls self-efficacy among pwMS who have fallen may be most effective if they address balance interference, health status, and other psychosocial fall-related outcomes, specifically fear of falling, associated activity curtailment, and falls control.
This study should be interpreted with consideration of its limitations. First, given the cross-sectional nature of our study, causality of variables associated with falls self-efficacy cannot be assumed. Second, the generalizability of the findings needs to be considered also as only individuals registered with the Multiple Sclerosis Society of Ireland and who had recently fallen were invited to participate. Furthermore, the self-report methodology employed necessitates caution when interpreting this data, particularly in terms of fall rates. Nevertheless, this study provides valuable insight into fall-related, psychosocial variables in pwMS who have fallen. Our study provokes important considerations for both the clinical and research domains in terms of present and future practice.
Conclusion
The findings of this cross-sectional study indicate that fear of falling, associated activity curtailment, low falls self-efficacy, and low perceptions of control relating to falls are prevalent among pwMS who have fallen. Furthermore, these psychosocial variables appear distinct in nature and notably warrant individualized attention during both assessment of and intervention for falls prevention. Future research is needed to develop standardized tools to measure fear of falling, associated activity curtailment, and falls control among pwMS, and to develop interventions that utilize occupational therapy expertise to support management of fall-related, psychosocial sequelae in this population.
Key findings
Fear of falling, associated activity curtailment, low falls self-efficacy, and compromised falls control are common among pwMS who have fallen. These constructs are distinct and should be treated as such during assessment. Falls self-efficacy among pwMS is associated with both physical and psychosocial factors.
What the study has added
This study provides evidence that fear of falling, associated activity curtailment, falls control, and falls self-efficacy are common and separate constructs which warrant individual attention during assessment and intervention for fall prevention.
Footnotes
Acknowledgements
The authors wish to thank Eve Geraghty, Julie Lucey, and Karen McGrath for their assistance in collecting data for this study.
Research ethics
This study was reviewed and approved by the Education and Health Sciences Research Ethics Committee at the University of Limerick, Ireland (Approval reference: 2014_05_08_EHS). All participants provided written informed consent.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Laura Comber is a PhD candidate funded by the Multiple Sclerosis Society of Ireland through the Ireland Fund.