
Abstract
Introduction
It is important to understand the experiences of elderly people with dementia and their family caregivers. Moreover, the maintenance of family caregivers’ satisfaction with co-occupation is important to ensure that they intend to continue providing care. This study developed and validated the Measure of Supporting Co-occupation, which assesses co-occupation involving elderly people with dementia and their family caregivers.
Method
This study used a cross-sectional design and questionnaire survey. Participants were recruited from 21 institutions. Descriptive statistics were calculated for the following domains: ‘evocation of the story of co-occupation’, ‘intention to continue co-occupation’ and ‘preferred co-occupation’. The construct validity and reliability of the ‘intention to continue co-occupation’ domain were examined using exploratory factor analysis, confirmatory factor analysis and Cronbach’s alpha. The criterion-related validity of the ‘intention to continue co-occupation’ was examined by means of correlations with other scales.
Results
There were 115 pairs of participants. Good criterion-related validity and internal consistency were confirmed for the ‘intention to continue co-occupation’ domain. However, confirmatory factor analysis showed insufficient model fitness.
Conclusion
The ‘intention to continue co-occupation’ domain is not ready for clinical application due to insufficient model fitness, it is necessary to revise the Measure of Supporting Co-occupation.
Introduction
Most elderly people with mild to moderate cognitive impairment are cared for by family members at home. These family members are forced to incur a heavy burden by assuming a role that is very similar to that of caregivers in institutions (Knapp and Prince, 2007). Behavioural and psychological symptoms of dementia (BPSD) vary between individuals and affect family caregivers’ burden and feelings of helplessness (Onishi et al., 2005). Thus it is important to understand the experiences of elderly people with dementia and their family caregivers.
In a previous study, we identified the need for support, such as support for identifying preferred co-occupations, and demonstrated the importance of supporting self-care for elderly people with dementia (Ono et al., 2014). ‘Co-occupation’ refers to the shared engagement of two or more people in an occupation or activity, and is regarded as an important target for occupational therapy (Zemke and Clark, 1996). However, only a few instruments are available to evaluate co-occupation. This study developed and validated the Measure of Supporting Co-occupation (MSC) to assess co-occupation among elderly people with dementia and their family caregivers.
Literature review
The family caregivers were predominantly women, who are required to assume and maintain a main role in family life and take responsibility for household duties, such as those involving household chores and work, in addition to providing care (Grafström et al., 1992). Furthermore, relatives of people with dementia who live at home experience psychological stress, and their affective and social lives are often limited when compared to those whose elderly relatives do not have dementia (Grafström et al., 1992). Mullin et al. highlighted the importance of relationships between elderly people with dementia and family caregivers and the need for identity in the implementation of long-term care (Mullin et al., 2013). Yamamoto and Wallhagen reported that three distinct factors explain why Japanese caregivers continue to provide caregiving: value of care; maintainers of value; and reinforcers of care continuation (Yamamoto and Wallhagen, 1997). Strain and Blandford reported that family caregivers who express affection for elderly people with dementia are less likely to cease caregiving activities (Strain and Blandford, 2002). In addition, caregivers’ satisfaction with the activities they perform with elderly people with dementia influences the continuation of care considerably (Keller et al., 2015). However, family caregivers of elderly people with dementia lead lives that are intertwined with the progress of dementia symptoms and must adapt to changing daily occupational situations (Persson and Zingmark, 2006). Kajiwara and Yokoyama (2007) reported that care satisfaction was associated with the continuation of care by family caregivers at home, and identified a need for assistance to enhance satisfaction with care. Burgener and Dickerson-Putman (1999) suggested the importance of interventions designed to improve the patient–caregiver relationship and reduce caregiver stress.
Co-occupation involves aspects of shared physicality, emotionality and intentionality (Pickens and Pizur-Barnekow, 2009). One of the characteristics of co-occupation was shared participation in an activity, and is highly interactive (Zemke and Clark, 1996). In a previous study, we reported that although most family caregivers perceived co-occupations to be troublesome, they still wanted to continue them (Ono et al., 2014). Troublesome co-occupations included ‘feeding’, ‘dressing’ and ‘diaper changing’. By contrast, about half of the subjects identified preferred co-occupations such as ‘travel’, ‘walking’ and ‘shopping’, ‘exercise’ and ‘meal preparation’, which were also included. However, approximately half of the family caregivers of elderly people with dementia reported having no preferences regarding co-occupation (Ono et al., 2014). Therefore, we identified the caregivers’ need for support, such as support for the affirmative recognition of preferred co-occupations, and demonstrated the importance of supporting self-care for elderly people with dementia. It would also be useful to develop an occupational therapy intervention for co-occupation that can be continued in caregivers’ home lives, as it could help improve the daily lives of elderly people with dementia and their family caregivers.
Occupational therapy encourages participation in meaningful activities with necessary modifications to the environment (World Federation of Occupational Therapists, 2012). There were many reports on the interventions that focused on the daily lives of elderly people with dementia and their family caregivers (Gitlin et al., 2001; Graff et al., 2008, 2003, 2007). In one study, an environmental programme that focused on adjusting the home environment and modifying the care strategy improved family caregivers’ self-efficacy and decreased BPSD in elderly people with dementia (Gitlin et al., 2001). The guidelines of Graff and colleagues for community-based occupational therapy focused on the adjustment of physical and human environments among elderly people with dementia and their family caregivers. These guidelines focused on improving elderly people’s performance in certain daily activities identified by interviews, and were found to improve the health status, quality of life (QoL) and daily performance in elderly people with dementia; they also improved the health status, QoL and sense of competence of family caregivers (Graff et al., 2003, 2007). In addition, community-based occupational therapy was cost-effective, especially in terms of informal caregiving (Graff et al., 2008). All these reports focused on interventions related to co-occupation between elderly people with dementia and their family caregiver.
The complexities of co-occupation (CoCO) scale was developed to evaluate co-occupation (Beckinger et al., 2016). The CoCO scale was expected to be a valuable tool for measuring and understanding co-occupation as experienced by clients in a range of contexts, including mental health practice and dementia care. However, it is necessary to develop instruments that evaluate the intention to continue co-occupation among family caregivers of elderly people with dementia, as it could help identify co-occupations that must be improved.
Aim
This study aimed to develop and validate the MSC, to assess co-occupation involving elderly people with dementia and their family caregivers. The development of a measure to assess co-occupation could clarify its use as part of community-based occupational therapy and fulfil the needs of family caregivers.
Method
Ethical issues
Ethical approval for the study was granted by the ethical committee at the institution with which the first author was affiliated. The study was conducted in accordance with the Declaration of Helsinki. The elderly people with dementia and their family caregivers provided written informed consent prior to participation in the study. To obtain consent from the elderly people with dementia, we used as simple an explanation as possible. In cases in which elderly people with dementia could not provide written informed consent for reasons that demonstrated confusion, proxy consent was sought, and the elderly people with dementia were asked to provide oral assent to participate in the study that followed.
Participants and procedure
Participants who fulfilled the following inclusion criteria were included in the study: (a) cohabitation between family members and elderly people with dementia; (b) consideration of the family member as the primary caregiver; (c) cognitive impairment scores of 14–23 for elderly people with dementia, based on the Mini-Mental State Examination (MMSE); and (d) absence of cognitive dysfunction and the ability to answer questionnaires reliably in family members.
Participants were recruited from 21 institutions (four outpatient rehabilitation centres, nine day care centres with rehabilitation services, five home-visit nursing stations, two home-visit rehabilitation centres, and one day service centre for the elderly) in Japan between June and November 2014.
This study used a cross-sectional design and questionnaire survey. The study coordinator recruited the participants, assessed elderly people for dementia by interviews, and requested that family caregivers complete the survey. Family caregivers who agreed to participate completed self-report questionnaires.
Item development
Domain 1 served to evoke the story of co-occupation in elderly people with dementia (‘evocation of the story of co-occupation’). This domain was created to make it easier to complete the following domains by reconfirming the relationship between family caregivers and elderly people with dementia, as well as their co-occupations so far.
Domain 2 assessed important factors representing intention to continue co-occupation in elderly people with dementia and their family caregivers (‘intention to continue co-occupation’). This domain contains 12 items: ‘importance of co-occupation’; ‘fatigue in co-occupation’; ‘effect of BPSD on co-occupation’; ‘participation in communication’; ‘care-related knowledge’; ‘duration of caregiving’; ‘satisfaction with co-occupation’; ‘environment in which co-occupation occurs’; ‘hope of participating in co-occupation’; ‘acceptance of co-occupation’; ‘desire for future co-occupation’; and ‘motivation for new co-occupation’ based on the characteristics of co-occupation identified in other studies (Burgener and Dickerson-Putman, 1999; Davis and Curtin, 2011; Kramer, 1997; Onishi et al., 2005; Ono et al., 2014; Sequeira, 2013; Steadman et al., 2007). Responses for these 12 items were provided using a four-point scale ranging from 1 (very unlikely) to 4 (very likely).
Domain 3 identified preferred new co-occupation or co-occupation that required
improvement (‘preferred co-occupation’). The importance of, performance in, and
satisfaction with, each co-occupation activity were measured using a scale of 1
(not at all) to 10 (very much). Of the items pertaining to preferred new
co-occupation interactions, performance and satisfaction were predicted (Figure 1). The Measure of Supporting Co-occupation
(MSC).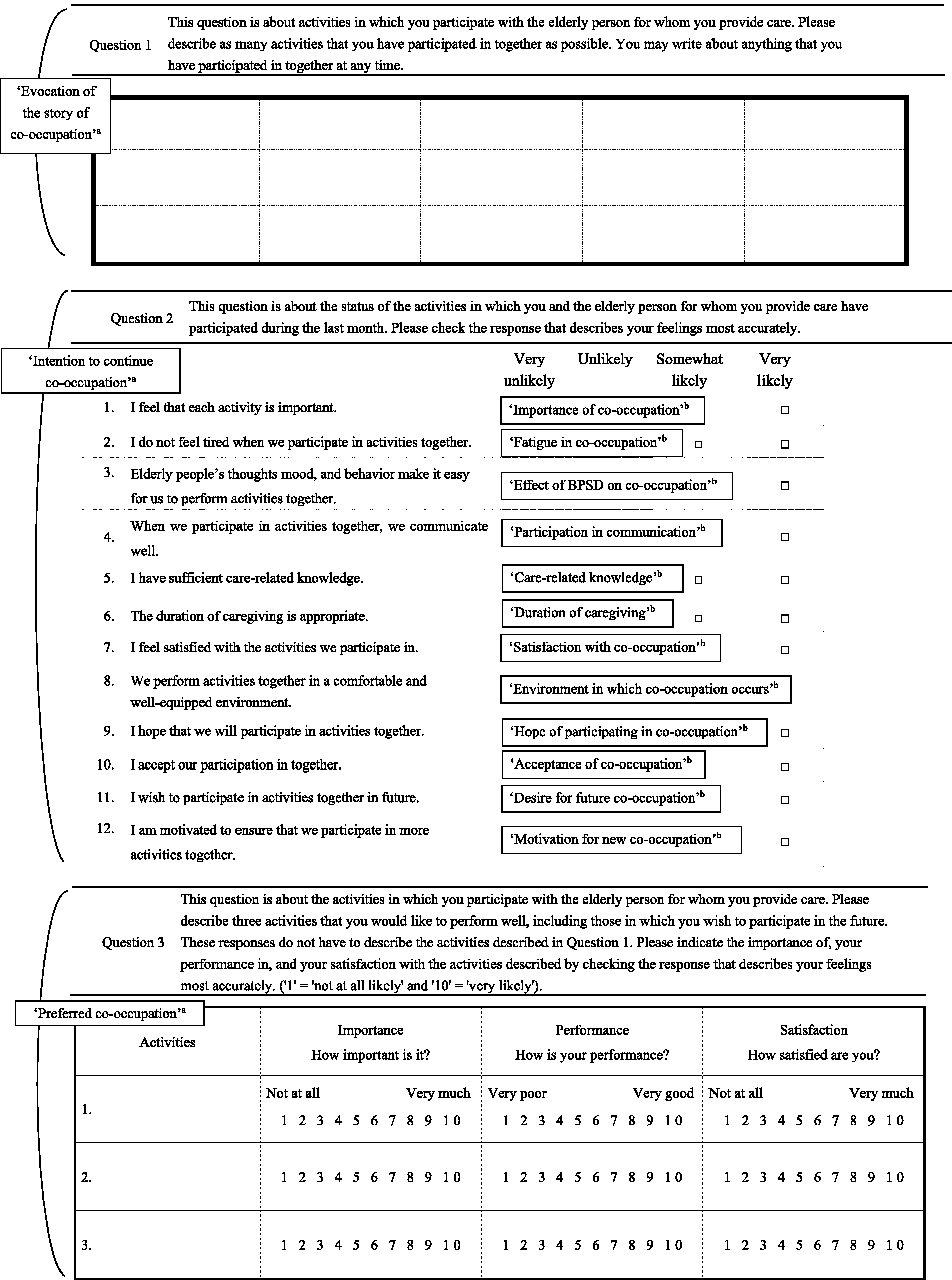
The study coordinator administered the MSC to family caregivers after providing the following explanation: ‘I will now ask you about various activities that you and the elderly person perform jointly in daily life. This activity includes all activities involving the participation of two people such as personal self-care, productivity, leisure, and rest.’
Family caregiver information
Basic information about family caregivers
Information about family caregivers’ sex, age, relationships with elderly people with dementia and caregiving period (in years) was obtained.
Japanese version of the EuroQoL-5 dimension
The EuroQoL-5 dimension (EQ-5D) was used to evaluate family caregivers’ health-related quality of life (HRQoL) (Tsuchiya et al., 2002). The descriptive system of the EQ-5D consists of five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Responses for each dimension are provided using three response choices (1 = no problem, 2 = moderate problem, 3 = severe problem). A summary index with a maximum score of 1 is derived from the five dimensions, using a score conversion table. The EQ-5D is a widely used generic instrument for the measurement of HRQoL. Among Alzheimer’s patients, the EQ-5D has been confirmed to have strong convergent validity and reliability (intraclass correlation coefficients ≥0.70; Naglie et al., 2006).
Self-completed occupational performance index
The Self-Completed Occupational Performance index (SOPI) was used to assess family caregivers’ occupational performance (Imai and Saito, 2010). The SOPI is based on the Canadian Occupational Performance Measure (COPM) and is used to evaluate social participation containing occupational performance (Imai and Saito, 2010). The SOPI consists of nine items including ‘occupational control’, ‘occupational balance’ and ‘satisfaction with performance’, in three domains: leisure, productivity, and self-care. Responses to each domain are provided using a five-point scale. A total SOPI score (maximum 100) is derived from these three dimensions. The reliability of the SOPI has been confirmed (Cronbach’s alpha = 0.93). Furthermore, the construct validity was confirmed as excellent based on correlation coefficients between the SOPI and Medical Outcomes Study (MOS) 36-Item Short Form Health Survey (SF-36), Version 2 (Imai and Saito, 2010).
Elderly people with dementia information
Basic information for elderly people with dementia
Information about sex, age, primary nursing care requirement authorisation and causative disease was collected for elderly people with dementia.
Mini-Mental State Examination (MMSE)
The MMSE was used to evaluate cognitive function in elderly people with dementia. The MMSE has been validated for dementia screening and has a score range of 0–30 (Folstein et al., 1975).
Dementia QoL instrument
The dementia quality of life instrument (DQoL) was used to evaluate subjective QoL in elderly people with dementia (Brod et al., 1999). The DQoL consists of 29 items divided between the following five domains: self-esteem, positive affect/humour, negative affect, feeling of belonging and sense of aesthetics. The total possible score for each domain is 5. The internal consistency reliability (Cronbach’s alpha) for the five domains of the DQoL ranges from 0.66 to 0.86. The construct validity of the DQoL was confirmed based on a moderate significant correlation coefficient between the geriatric depression scale and the DQoL subscales (Suzuki et al., 2005). The DQoL was administered by way of an interview; the questions were explained slowly so as to avoid confusing the elderly people with dementia.
Analysis
Content and face validity of the MSC
With respect to the content validity of the MSC, the relevance and appropriateness of each domain were reviewed and discussed by the experts. The experts (n = 4) were three occupational therapists, including one who was familiar with the development of psychometric instruments and one nurse who worked in mental health. They confirmed whether the contents of each domain of the MSC are able to assess each construct and those of each item in the ‘intention to continue co-occupation’ domain are able to assess each construct. Furthermore, it confirmed whether the contents of the ‘intention to continue co-occupation’ domain are adequately covered by the identified items. The content validity was assured with the agreement of all the experts. With regard to the face validity of the MSC, the MSC was administered to three family caregivers of elderly people with dementia who were not included in the study, and it was confirmed that the content of items and domains could be sufficiently understood.
Descriptive statistics for the MSC
Medians and interquartile ranges were calculated for the number of co-occupations reported for the ‘evocation of the story of co-occupation’ domain, item scores for the ‘intention to continue co-occupation’ domain and the number of co-occupations and importance of, performance in, and satisfaction with the co-occupation in the ‘preferred co-occupation’ domain.
Construct validity of the ‘intention to continue co-occupation’ domain
We performed exploratory factor analysis (EFA) for ordinal categorical data, using the weighted least squares method for the 12 items in the ‘intention to continue co-occupation’ domain, to extract the factor structure. EFA is used to identify a set of latent constructs underlying a battery of measured variables (Fabrigar et al., 1999). Factor loadings were based on EFA with oblique (promax) rotation. The number of factors was calculated following assessment of eigenvalues greater than 1 and the production of a scree plot (Floyd and Widamon, 1995). Items with factor loadings of 0.40 or greater for one factor were selected. Moreover, items with low communalities were removed.
Confirmatory factor analysis (CFA) was performed for ordinal categorical data with robust estimation (weighted least squares method), to confirm the factor structure. When there is sufficient theoretical and empirical basis for researchers to specify the most plausible model, CFA is considered a better approach than EFA (Fabrigar et al., 1999). We assessed model fitness using the Tucker–Lewis index (TLI), comparative fit index (CFI) and root mean square error of approximation (RMSEA), according to the following criteria: TLI > 0.95, CFI > 0.95 and RMSEA < 0.08 (Hu and Bentler, 1999).
Criterion-related validity of the ‘intention to continue co-occupation’ domain
We performed correlation analysis to explore the relationships between the factors explored by EFA for the ‘intention to continue co-occupation’ domain and variables from other scales. Spearman’s rank correlation coefficients indicated significant relationships between ‘intention to continue co-occupation’, the EQ-5D and SOPI in family caregivers. Pairwise interclass correlation coefficients indicated significant relationships between the ‘intention to continue co-occupation’ domain, MMSE and DQoL in elderly people with dementia. The strength of the Spearman’s rank correlation coefficients and pairwise interclass correlation coefficients was interpreted as follows: |r| ≥ 0.8, very strong relationship; 0.6 ≤ |r|<0.8, strong relationship; 0.4 ≤ |r| < 0.6, moderate relationship; 0.2 ≤ |r| < 0.4, mild relationship; |r| < 0.2, very weak relationship (Campbell and Swinscow, 2009).
Reliability of the ‘intention to continue co-occupation’ domain
Cronbach’s alpha was calculated to determine the internal consistency reliability for the ‘intention to continue co-occupation’ domain and each factor.
Relationships between the ‘evocation of the story of co-occupation’, ‘intention to continue co-occupation’ and ‘preferred co-occupation’ domains
Spearman’s rank correlation coefficients indicated relationships between the number of co-occupations in the ‘evocation of the story of co-occupation’ domain; the total score and factor scores in the ‘intention to continue co-occupation’ domain; and the number of co-occupations and importance of, performance in, and satisfaction with, these interactions in the ‘preferred co-occupation’ domain. The Spearman’s rank correlation coefficient strength was interpreted using the same criteria as above.
Statistical significance was set at P < 0.05 for two-tailed tests in all statistical analyses. We used R3.1.2 for Windows for EFA, M-plus version 7 for CFA and HAD version 13.00 for pairwise interclass correlation coefficients. We used SPSS 21.0J for Windows for other analyses.
Results
Participants
Findings were obtained from 115 pairs of participants from 21 cooperative institutions. Of the family caregivers, 26 (22.6%) were men and 89 (77.4%) were women, and their average age was 65.3 ± 11.1 years. The average caregiving duration was 3.9 ± 3.1 years. Of the elderly people with dementia, 49 (42.6%) were men and 66 (57.4%) were women, and their average age was 83.4 ± 6.9 years. The average MMSE score was 19.9 ± 3.2.
Content and face validity of the MSC
With respect to the content validity, the experts discussed whether the items used in each domain in the MSC are able to assess each construct and adequately covered important aspects. All experts agreed that the contents of domains of the MSC assessed each construct, and the 12 items were found to cover all the important aspects of the ‘intention to continue co-occupation’. As for the face validity, in advance, the experts discussed whether the wording of the items and domains were easy to understand for family caregivers of elderly people with dementia. Thereafter, the MSC was administered to three family caregivers of elderly people with dementia, and they pointed out that some wording used in the questionnaire was difficult to understand. As a result, they made suggestions for minor adjustments to the phrasing of these items, and the wording was revised accordingly by the experts. The MSC that was modified was confirmed by family caregivers of elderly people with dementia, and was considered to be easy to understand.
Descriptive statistics for the MSC
Scores for the Measure of Supporting Co-occupation (MSC), EQ-5D, the SOPI and the DQoL.
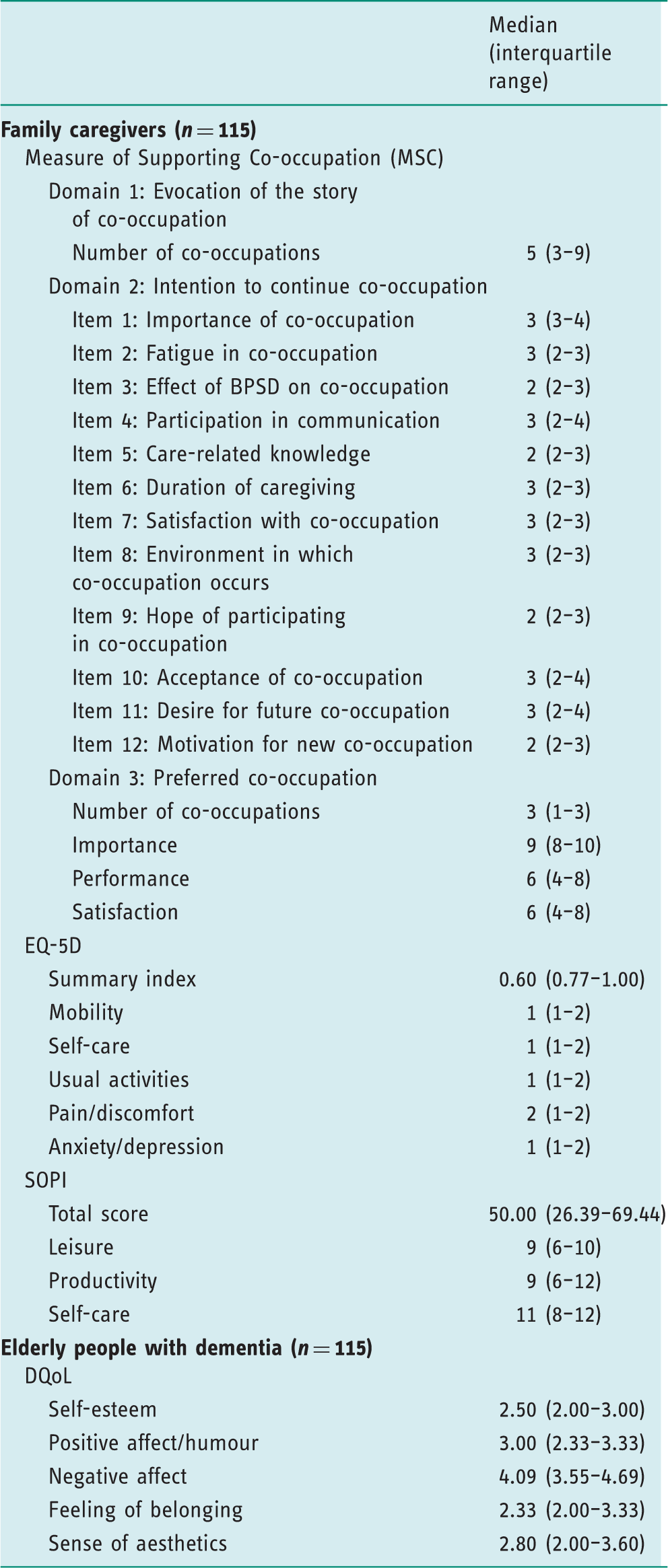
BPSD: behavioural and psychological symptoms of dementia; DQoL: dementia quality of life instrument; EQ-5D: EuroQoL-5 dimension; SOPI: Self-Completed Occupational Performance Index.
Construct validity of the ‘intention to continue co-occupation’ domain
Exploratory factor analysis of the ‘intention to continue co-occupation’ domain.
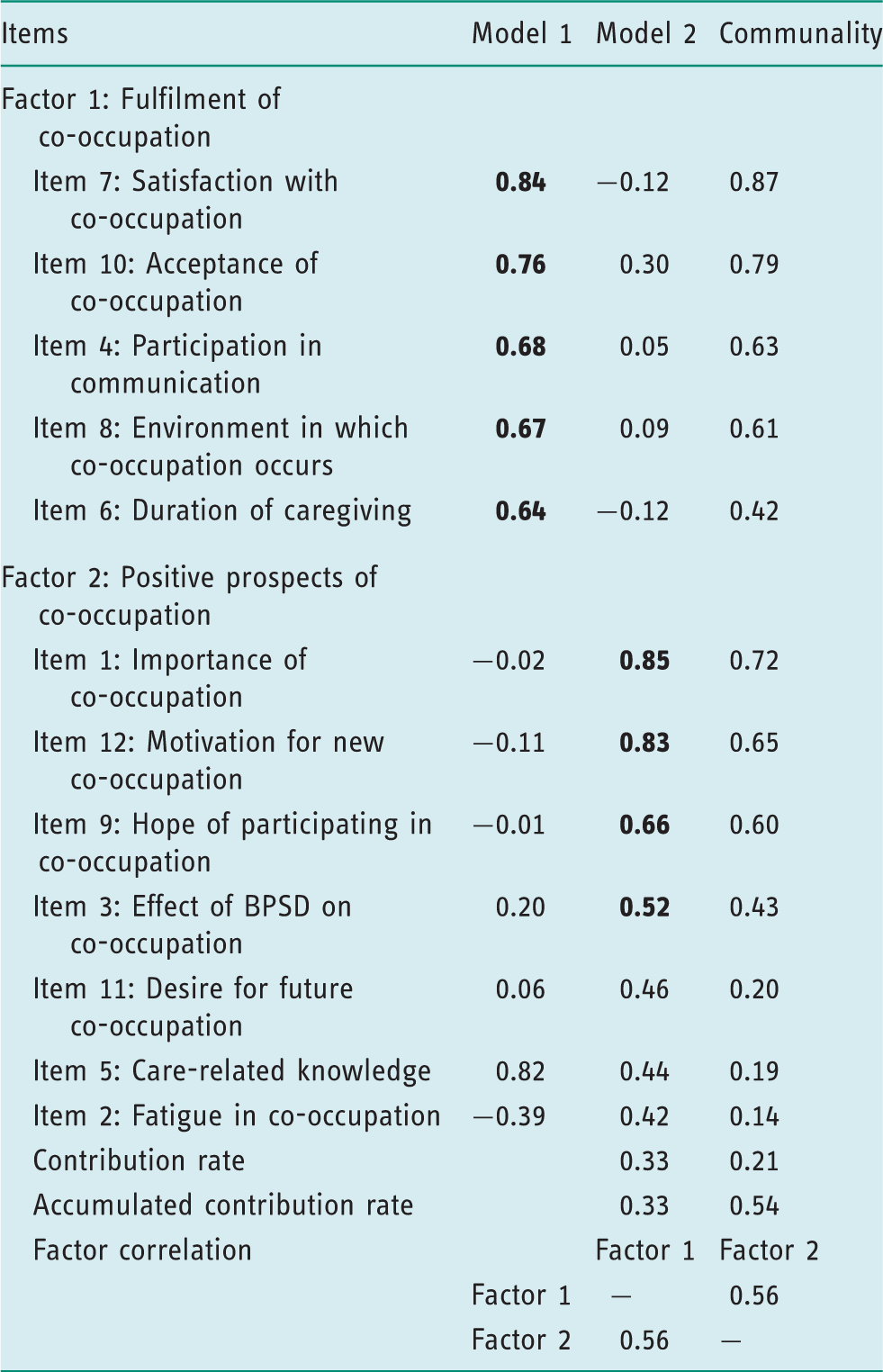
BPSD : behavioural and psychological symptoms of dementia.
The first and strongest factor consisted of five items with positive factor loadings ranging from 0.64 to 0.84: ‘satisfaction with co-occupation’, ‘acceptance of co-occupation’, ‘participation in communication’, ‘environment in which co-occupation occurs’ and ‘duration of caregiving’. The first factor was named ‘fulfilment of co-occupation’.
Factor 2 comprised four items with positive factor loadings (0.52–0.85): ‘importance of co-occupation’, ‘motivation for new co-occupation’, ‘hope of participating in co-occupation’ and ‘effect of BPSD on co-occupation’. Factor 2 was named ‘positive prospects for co-occupation’.
To determine the construct validity of ‘intention to continue co-occupation’, we
conducted CFA based on the results of the EFA. The model with the highest
goodness-of-fit was a second-order factor model that regarded ‘intention to
continue co-occupation’ as a higher-order factor, and two factors extracted by
the EFA as lower-order factors (Figure 2). All path coefficients were over 0.5, and model fitness
was as follows: TLI = 0.941, CFI = 0.955 and RMSEA = 0.120. The resulting
goodness-of-fit indices suggested insufficient fitness. Confirmatory factor analysis of the ‘intention
to continue co-occupation’ domain. Domains included in the
questionnaire and items in the ‘intention to continue co-occupation’
domain (d1 and d2 and e1–e9 error variables).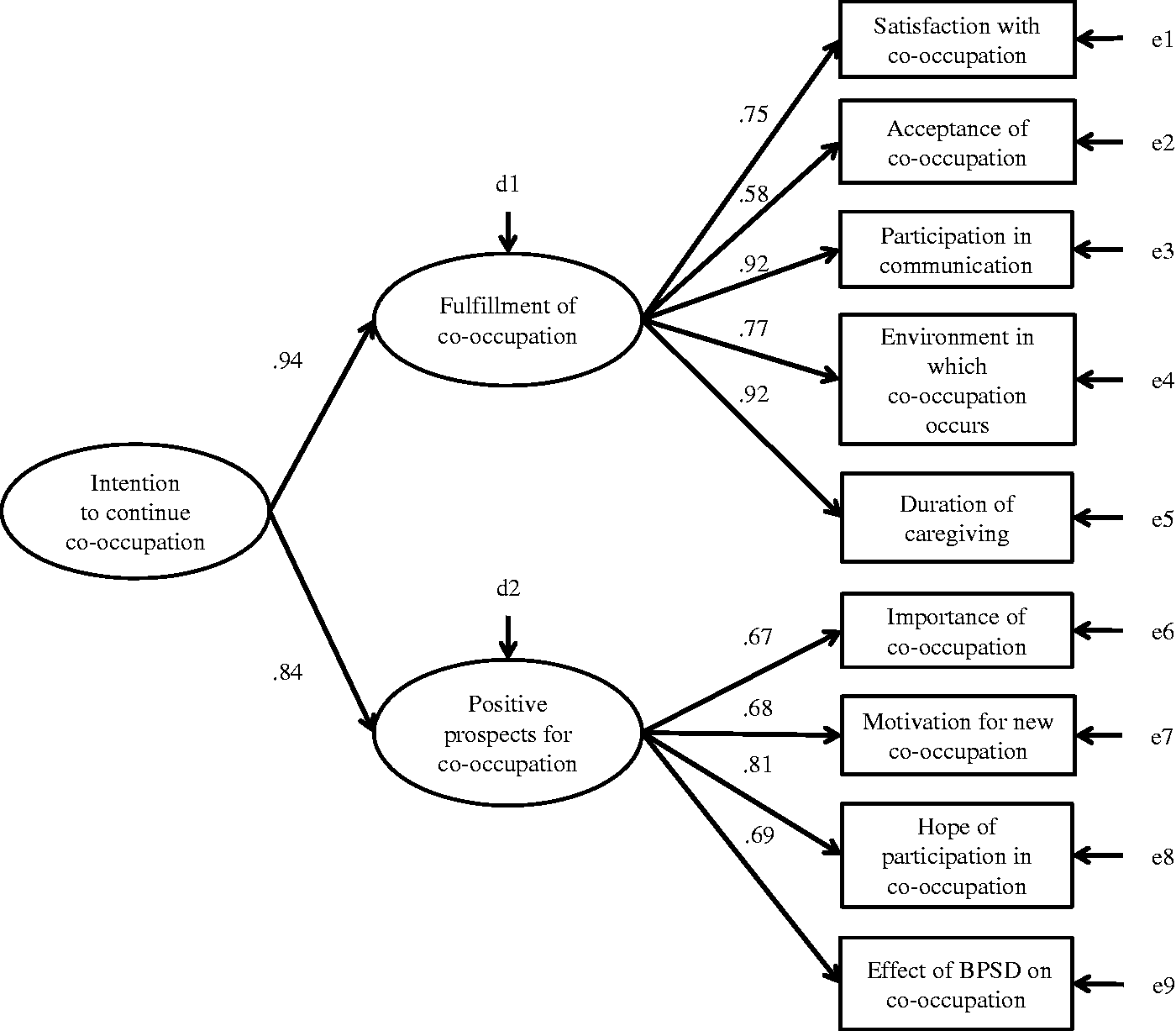
Criterion-related validity of the ‘intention to continue co-occupation’ domain
Correlation coefficients between ‘intention to continue co-occupation’ and the EQ-5D and SOPI.
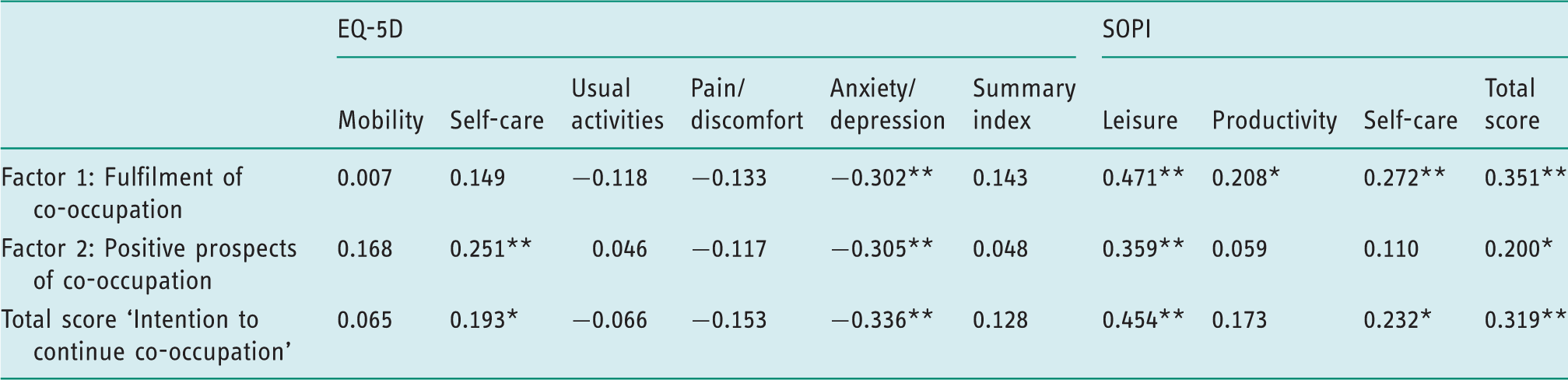
Spearman’s rank correlation coefficient.
P < 0.01; *P < 0.05.
EQ-5D: EuroQoL-5 dimension; SOPI: Self-Completed Occupational Performance Index.
No significant correlations were observed between the ‘intention to continue co-occupation’ domain and any of the MMSE factors or the DQoL.
Reliability of the ‘intention to continue co-occupation’ domain
Cronbach’s alpha for the ‘fulfilment of co-occupation’ and ‘positive prospects for co-occupation’ factors were 0.86 and 0.75.
Relationships between the ‘evocation of the story of co-occupation’, ‘intention to continue co-occupation’ and ‘preferred co-occupation’ domains
Significant positive correlations were observed between the number of co-occupations in the ‘evocation of the story of co-occupation’ and the number of co-occupations in the ‘preferred co-occupation’ domains (r = 0.43, P < 0.01). The total scores for the ‘intention to continue co-occupation’ domain and ‘positive prospects for co-occupation’ factor were significantly correlated with the number of co-occupations in the ‘preferred co-occupation’ domain (r = 0.33, P < 0.01; r = 0.32, P < 0.01). The total scores for the ‘intention to continue co-occupation’ domain and the ‘fulfilment of co-occupation’ and ‘positive prospects for co-occupation’ factors were significantly correlated with the satisfaction item in the ‘preferred co-occupation’ domain (r = 0.36, P < 0.01; r = 0.35, P < 0.01; r = 0.31, P < 0.01). The importance and performance items in the ‘preferred co-occupation’ domain were not significantly correlated with other domains.
Discussion
Validity and reliability of the ‘intention to continue co-occupation’ domain
The ‘intention to continue co-occupation’ domain demonstrated good criterion-related validity and internal consistency. However, the model for ‘intention to continue co-occupation’ showed insufficient fitness.
The construct validity and the results of the EFA indicated that the ‘intention to continue co-occupation’ domain consisted of two factors: ‘fulfilment of co-occupation’ and ‘positive prospects for co-occupation’. Kajiwara et al. reported that care satisfaction was associated with the continuation of care by family caregivers at home, and identified a need for assistance to enhance satisfaction with care (Kajiwara and Yokoyama, 2007). In addition, Mullin et al. highlighted the importance of relationships between elderly people with dementia and family caregivers and the need for identity in the implementation of long-term care (Mullin et al., 2013). In view of these finding, the two factors that were extracted in the current study were considered valid. However, the secondary factor model showed insufficient fitness, based on the results of CFA. The provision of support for family caregivers has previously been shown to diminish negative factors such as the burden of care. Furthermore, Persson and Zingmark (2006) reported that family caregivers of elderly people with dementia experience high levels of stress because they must adapt to daily changes in occupational situations. Therefore, family caregivers of elderly people with dementia might often be unable to engage in their own meaningful occupations, and may not be able to afford to manage their daily lives. Based on these results, it is necessary to reconsider whether the excluded items of ‘fatigue in co-occupation’, ‘care-related knowledge’ and ‘desire for future co-occupation’ are in fact associated with the ‘intention to continue co-occupation’ domain. Accordingly, the ‘intention to continue co-occupation’ domain could involve additional factors; therefore, future research should examine additional factors for this domain.
With regard to criterion-related validity, the ‘intention to continue co-occupation’ domain was associated with occupational performance (according to the SOPI) and the psychological aspects of QoL (according to the EQ-5D) of family caregivers. Because co-occupation involves the aspects of shared emotionality and intentionality, the ‘intention to continue co-occupation’ domain was considered to reflect psychological and social constructs in family caregivers, such as ‘anxiety/depression’ and ‘leisure’. This suggests that the ‘intention to continue co-occupation’ domain is considered relevant to achieving occupational balance in valuable activities for family caregivers. Therefore, reductions in ‘intention to continue co-occupation’ occur presumably because either care provision is too burdensome for one person or occupational balance declines in daily life.
With respect to the reliability of the ‘intention to continue co-occupation’ domain, as the Cronbach’s alpha for the factors exceeded 0.75, the domain demonstrated adequate reliability.
Psychometric characteristics of the MSC
The MSC demonstrated good content and face validity. In face validity, some of the wording used in the questionnaire was difficult to understand for family caregivers of elderly people with dementia. It was considered that the wording was somewhat jargonistic. Thereafter, through suggestion and revisions by the experts, the wording was replaced with similar representation and modified to be easily understood by family caregivers of elderly people with dementia.
The MSC consists of three domains: ‘evocation of the story of co-occupation’, ‘intention to continue co-occupation’ and ‘preferred co-occupation’. The results showed that the number of co-occupations in the ‘evocation of the story of co-occupation’ domain was moderately associated with the number of co-occupations in the ‘preferred co-occupation’ domain. This confirmed that the content of evoked co-occupations can not only elucidate the history of co-occupation but can also help in understanding the level of attachment between caregivers and elderly people with dementia. Attachment is known to be associated with the continuation of care (Strain and Blandford, 2002; Yamamoto and Wallhagen, 1997). In other words, even if family caregivers have a negative feeling about the current co-occupation, family caregivers with a strong attachment are less likely to give up on care. Therefore, we considered that the level of attachment has an effect on the association between the ‘preferred co-occupation’ domain, which refers to the occupations that family caregivers want to improve in the future, and the ‘evocation of the story of co-occupation’ domain. In contrast, the ‘evocation of the story of co-occupation’ domain was not associated with the ‘intention to continue co-occupation’ domain. As mentioned above, it is considered that even family caregivers with strong attachment to elderly people with dementia have negative feelings. Therefore, we considered that the items of ‘intention to continue co-occupation’ were not just associated with the relationship (for example, level of attachment) between elderly people with dementia and family caregivers. As noted before, Pickens and Pizur-Barnekow (2009) proposed that co-occupation involves aspects of shared physicality, emotionality and intentionality. The items of the ‘intention to continue co-occupation’ domain potentially reflected not only the relationship (for example, level of attachment) so far but also the shared emotions and intentions arising from the interaction between elderly people with dementia and family caregivers at present. The total score for the ‘intention to continue co-occupation’ was associated with the number of co-occupations in and satisfaction with the ‘preferred co-occupation’ domain. In other words, family caregivers with a strong intention to continue co-occupation might engage in more co-occupations that are satisfying to them, whereas family caregivers with a weak intention might have less motivation to engage in new co-occupations, and be dissatisfied with their co-occupations. This suggests a need to improve caregivers’ satisfaction with preferred co-occupations, which in turn might improve their intention to continue co-occupation.
These results suggest that, rather than relying on ‘intention to continue co-occupation’ alone, future interventions could use the whole MSC to examine co-occupation. In addition, the implementation of evaluations using the MSC could encourage family caregivers to review co-occupation and improve current understanding of the occupational narratives of family caregivers.
Limitations
The study was subject to several limitations. For example, the number of items in the ‘intention to continue co-occupation’ domain was low, which could have affected model fitness. The development of the MSC involved the selection of factors that were important in the ‘intention to continue co-occupation’ domain, based on a preliminary investigation and literature review. However, reducing the burden of care has been shown to be important for supporting the family. Therefore, excluded items, such as ‘fatigue in co-occupation’, ‘care-related knowledge’ and ‘desire for future co-occupation’ might need to be included. Furthermore, this is because many other studies have reported that these concepts are the elements of care continuation (Davis and Curtin, 2011; Onishi et al., 2005; Ono et al., 2014; Steadman et al., 2007). In future studies, it is necessary to investigate more items potentially related to the ‘intention to continue co-occupation’ domain, in order to facilitate the establishment of a stable model.
In addition, some participants could have misunderstood some of the items. For instance, ‘I hope to do activities together’ is an ambiguous expression and could have been confused with activities in daily life. Therefore, expressions that evoke memories of concrete situations should be used in future research. Moreover, modification of the wording of the MSC should be considered, as the implicit suggestion that co-occupation should be performed could have been embedded in some of the sentences in the MSC. Furthermore, use of a neutral voice and re-examination of face validity are required in future studies.
Moreover, the MSC demonstrated only internal consistency reliability; therefore, test–retest reliability should be assessed in future studies. Furthermore, the study participants were family caregivers of elderly people with dementia, and they were not classified according to personal attributes. The effects of the provision of care by spouses and offspring could differ; therefore, caregivers’ personal attributes should be considered in future studies.
Conclusion
This study involved the development and validation of the MSC as a means of assessing co-occupation in elderly people with dementia and their family caregivers. However, the ‘intention to continue co-occupation’ domain did not demonstrate adequate model fitness, but content and face validity, criterion-related validity and reliability were confirmed. The MSC could be used to obtain basic information regarding meaningful co-occupation in elderly people with dementia and their family caregivers. However, the ‘intention to continue co-occupation’ domain of MSC is not ready for clinical application due to insufficient model fitness. Future study is necessary to revise the MSC.
Key findings
The Measure of Supporting Co-occupation (MSC) was developed. The ‘intention to continue co-occupation’ model domain showed
insufficient fitness. Future research should examine additional factors of the ‘intention to
continue co-occupation’ domain.
What the study has added
The MSC can be used to obtain basic information on meaningful co-occupation in elderly people with dementia and their family caregivers dwelling in the community.
Footnotes
Acknowledgements
The authors wish to thank the participants, the occupational therapy practitioners who cooperated with the study and the teachers who provided guidance.
Research ethics
Ethical approval for the study was granted by the ethics committee of Kawasaki University of Medical Welfare (reference number: 444; 7 April 2014).
Consent
The elderly people with dementia and their family caregivers provided written informed consent. In cases in which elderly people with dementia could not provide written informed consent for reasons that demonstrated confusion, proxy consent was sought and the elderly people with dementia were asked to provide oral assent to participate in the study that followed.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.